Physiological Responses of Continuous and Intermittent Swimming at Critical Speed and Maximum Lactate Steady State in Children and Adolescent Swimmers


 ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Calculation of CS
2.3. Continuous Swimming Tests—Determination of MLSS
2.4. Intermittent Swimming at CS
2.5. Statistical Analysis
3. Results
3.1. Performance, Peak Heart Rate and Peak Oxygen Uptake in 200 and 400-m Tests
3.2. Speed and Physiological Responses during Continuous Swimming at CS and sMLSS
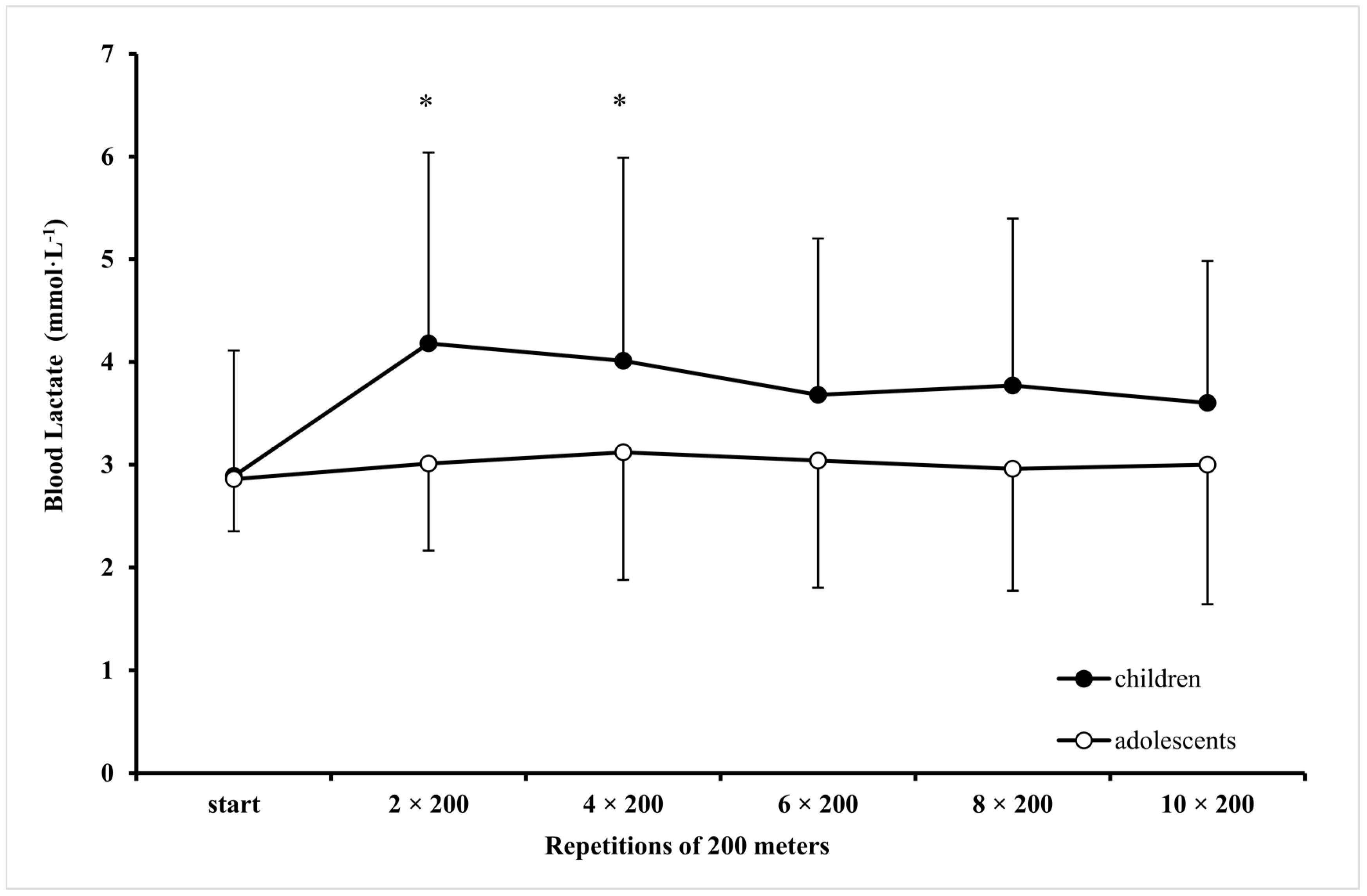
3.3. Physiological Responses during Intermittent Swimming at CS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Toubekis, A.G.; Tokmakidis, S.P. Metabolic responses at various intensities relative to critical swimming velocity. J. Strength Cond. Res. 2013, 27, 1731–1741. [Google Scholar] [CrossRef] [PubMed]
- Dekerle, J.; Pelayo, P. Assessing aerobic endurance in swimming. In World Book of Swimming from Science to Performance; Seifert, L., Chollet, D., Mujika, I., Eds.; Nova Science Publishers: New York, NY, USA, 2011; pp. 277–296. [Google Scholar]
- Wakayoshi, K.; Yoshida, T.; Kasai, T.; Moritani, T.; Mutoh, Y.; Miyashita, M. Validity of critical velocity as swimming fatigue threshold in the competitive swimmer. Ann. Physiol. Anthropol. 1992, 11, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Toussaint, H.M.; Wakayoshi, K.; Hollandre, P.; Ogita, F. Simulated front crawl swimming performance related to critical speed and critical power. Med. Sci. Sports Exerc. 1998, 30, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Wakayoshi, K.; Yoshida, T.; Udo, M.; Harada, T.; Moritani, T.; Mutoh, Y.; Miyashita, M. Does critical swimming velocity represent exercise intensity at maximal lactate steady state? Eur. J. Appl. Physiol. Occup. Physiol. 1993, 66, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.; Vilas-boas, J.P. Critical Velocity as a Criterion for Estimating Aerobic Training Pace in Juvenile Swimmers. In Biomechanics and Medicine in Swimming VIII; Keskinen, K.L., Komi, P.V., Hollander, A.P., Eds.; Gummerus Printing: Jyväskylä, Finland, 1999; pp. 233–244. [Google Scholar]
- Dekerle, J.; Brickley, G.; Alberty, M.; Pelayo, P. Characterising the slope of the distance-time relationship in swimming. J. Sci. Med. Sport 2010, 13, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Zacca, R.; Fernandes, R.J.P.; Pyne, D.B.; Castro, F.A.S. Swimming training assessment: The critical velocity and the 400-m test for age-group swimmers. J. Strength Cond. Res. 2016, 30, 1365–1372. [Google Scholar] [CrossRef]
- Maglischo, E. Swimming Fastest; Human Kinetics: Champaign, IL, USA, 2003. [Google Scholar]
- Toubekis, A.; Tsami, A.; Smilios, I.; Douda, H.; Tokmakidis, S. Training-induced changes on blood lactate profile and critical velocity in young swimmers. J. Strength Cond. Res. 2011, 25, 1563–1570. [Google Scholar] [CrossRef]
- Ratel, S.; Duche, P.; Williams, C.A. Muscle fatigue during high-intensity exercise in children. Sport Med. 2006, 36, 1031–1065. [Google Scholar] [CrossRef]
- Filipatou, E.; Toubekis, A.; Douda, H.; Pilianidis, T.; Tokmakidis, S. Lactate and heart rate responses during swimming at 95% and 100% of the critical velocity in children and young swimmers. Port J. Sport Sci. 2006, 6, 132–134. [Google Scholar]
- Boisseau, N.; Delamarche, P. Metabolic and hormonal responses to exercise in children and adolescents. Sport Med. 2000, 30, 405–422. [Google Scholar] [CrossRef]
- Toubekis, A.G.; Vasilaki, A.; Douda, H.; Gourgoulis, V.; Tokmakidis, S. Physiological responses during interval training at relative to critical velocity intensity in young swimmers. J. Sci. Med. Sport 2011, 14, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.V.; Júnior, O.A.; Marques, A.C.; Colantonio, E.; Cyrino, E.S.; De Mello, M.T. Effect of 12 weeks of training on critical velocity and maximal lactate steady state in swimmers. Eur. J. Sport Sci. 2011, 11, 165–170. [Google Scholar] [CrossRef]
- Dekerle, J.; Sidney, M.; Hespel, J.M.; Pelayo, P. Validity and reliability of critical speed, critical stroke rate, and anaerobic capacity in relation to front crawl swimming performances. Int. J. Sports Med. 2002, 23, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, L.F.P.; Lima, M.C.S.; Gobatto, C.A. Changes in physiological and stroking parameters during interval swims at the slope of the d-t relationship. J. Sci. Med. Sport 2010, 13, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Greco, C.C.; Denadai, B.S. Relationship between critical speed and endurance capacity in young swimmers: Effects of gender and age. Pediatr. Exerc. Sci. 2005, 17, 353–363. [Google Scholar] [CrossRef]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sport Exerc. 2002, 34, 689–694. [Google Scholar] [Green Version]
- Jürimäe, J.; Haljaste, K.; Cicchella, A.; Latt, E.; Purge, P.; Leppik, A.; Jürimäe, T. Analysis of swimming performance from physical, physiological, and biomechanical parameters in young swimmers. Pediatr. Exerc. Sci. 2007, 19, 70–81. [Google Scholar] [CrossRef]
- Beneke, R. Anaerobic threshold, individual anaerobic threshold, and maximal lactate steady state in rowing. Med. Sci. Sports Exerc. 1995, 27, 863–867. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Pelarigo, J.G.; Denadai, B.S.; Greco, C.C. Stroke phases responses around maximal lactate steady state in front crawl. J. Sci. Med. Sport 2011, 14, 168.e1–168.e5. [Google Scholar] [CrossRef]
- Dekerle, J.; Pelayo, P.; Clipet, B.; Depretz, S.; Lefevre, T.; Sidney, M. Critical swimming speed does not represent the speed at maximal lactate steady state. Int. J. Sports Med. 2005, 26, 524–530. [Google Scholar] [CrossRef]
- Barker, A.; Welsman, J.; Fulford, J.; Welford, D.; Armstrong, N. Quadriceps muscle energetics during incremental exercise in children and adults. Med. Sci. Sports Exerc. 2010, 42, 1303–1313. [Google Scholar] [CrossRef] [PubMed]
- Toussaint, H.M.; Roos, P.E.; Kolmogorov, S. The determination of drag in front crawl swimming. J. Biomech. 2004, 37, 1655–1663. [Google Scholar] [CrossRef] [PubMed]
- Greco, C.C.; de Oliveira, M.F.M.; Caputo, F.; Denadai, B.S.; Dekerle, J. How narrow is the spectrum of submaximal speeds in swimming? J. Strength Cond. Res. 2013, 27, 1450–1454. [Google Scholar] [CrossRef] [PubMed]
- Baron, B.; Noakes, T.D.; Dekerle, J.; Moullan, F.; Robin, S.; Matran, R.; Pelayo, P. Why does exercise terminate at the maximal lactate steady state intensity? Br. J. Sports Med. 2008, 42, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Turley, K.; Wilmore, J. Cardiovascular responses to treadmill and cycle ergometer exercise in children and adults. J. Appl. Physiol. 1997, 83, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Keskinen, O.; Keskinen, K.; Mero, A. Effect of pool length on blood lactate, heart rate, and velocity in swimming. Int. J. Sports Med. 2007, 28, 407–413. [Google Scholar] [CrossRef]
- Beneke, R.; Hütler, M.; Von Duvillard, S.P.; Sellens, M.; Leithäuser, R.M. Effect of test interruptions on blood lactate during constant workload testing. Med. Sci. Sports Exerc. 2003, 35, 1626–1630. [Google Scholar] [CrossRef]
- Olbrecht, J.; Madsen, O.; Mader, A.; Liesen, H.; Hollmann, W. Relationship between swimming velocity and lactic concentration during continuous and intermittent training exercises. Int. J. Sports Med. 1985, 6, 74–77. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Children | Adolescents | ||||
|---|---|---|---|---|---|---|
| CS | sMLSS | ES | CS | sMLSS | ES | |
| Speed (m·s−1) | 1.092 ± 0.071 ‡ (1.136–1.048) | 1.083 ± 0.065 ‡ (1.123–1.042) | 0.14 small | 1.315 ± 0.068 (1.357–1.237) | 1.297 ± 0.056 (1.332–1.263) | 0.29 medium |
| End-HR (b·min−1) | 188 ± 13 ‡ (180–196) | 187 ± 8 ‡ (182–191) | 0.18 small | 179 ± 9 (174–185) | 175 ± 12 (168–182) | 0.44 medium |
| End O2(mL·kg−1·min−1) | 43.3 ± 5.4 (39.9–46.6) | 40.7 ± 7.4 (36.1–45.3) | 0.40 medium | 46.3 ± 6.6 (42.2–50.4) | 44.6 ± 6.9 (40.4–48.9) | 0.25 medium |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikitakis, I.S.; Paradisis, G.P.; Bogdanis, G.C.; Toubekis, A.G. Physiological Responses of Continuous and Intermittent Swimming at Critical Speed and Maximum Lactate Steady State in Children and Adolescent Swimmers. Sports 2019, 7, 25. https://doi.org/10.3390/sports7010025
Nikitakis IS, Paradisis GP, Bogdanis GC, Toubekis AG. Physiological Responses of Continuous and Intermittent Swimming at Critical Speed and Maximum Lactate Steady State in Children and Adolescent Swimmers. Sports. 2019; 7(1):25. https://doi.org/10.3390/sports7010025
Chicago/Turabian StyleNikitakis, Ioannis S., Giorgos P. Paradisis, Gregory C. Bogdanis, and Argyris G. Toubekis. 2019. "Physiological Responses of Continuous and Intermittent Swimming at Critical Speed and Maximum Lactate Steady State in Children and Adolescent Swimmers" Sports 7, no. 1: 25. https://doi.org/10.3390/sports7010025
APA StyleNikitakis, I. S., Paradisis, G. P., Bogdanis, G. C., & Toubekis, A. G. (2019). Physiological Responses of Continuous and Intermittent Swimming at Critical Speed and Maximum Lactate Steady State in Children and Adolescent Swimmers. Sports, 7(1), 25. https://doi.org/10.3390/sports7010025