The Effect of Caffeine Ingestion and Carbohydrate Mouth Rinse on High-Intensity Running Performance


Abstract
:1. Introduction
2. Materials and Methods
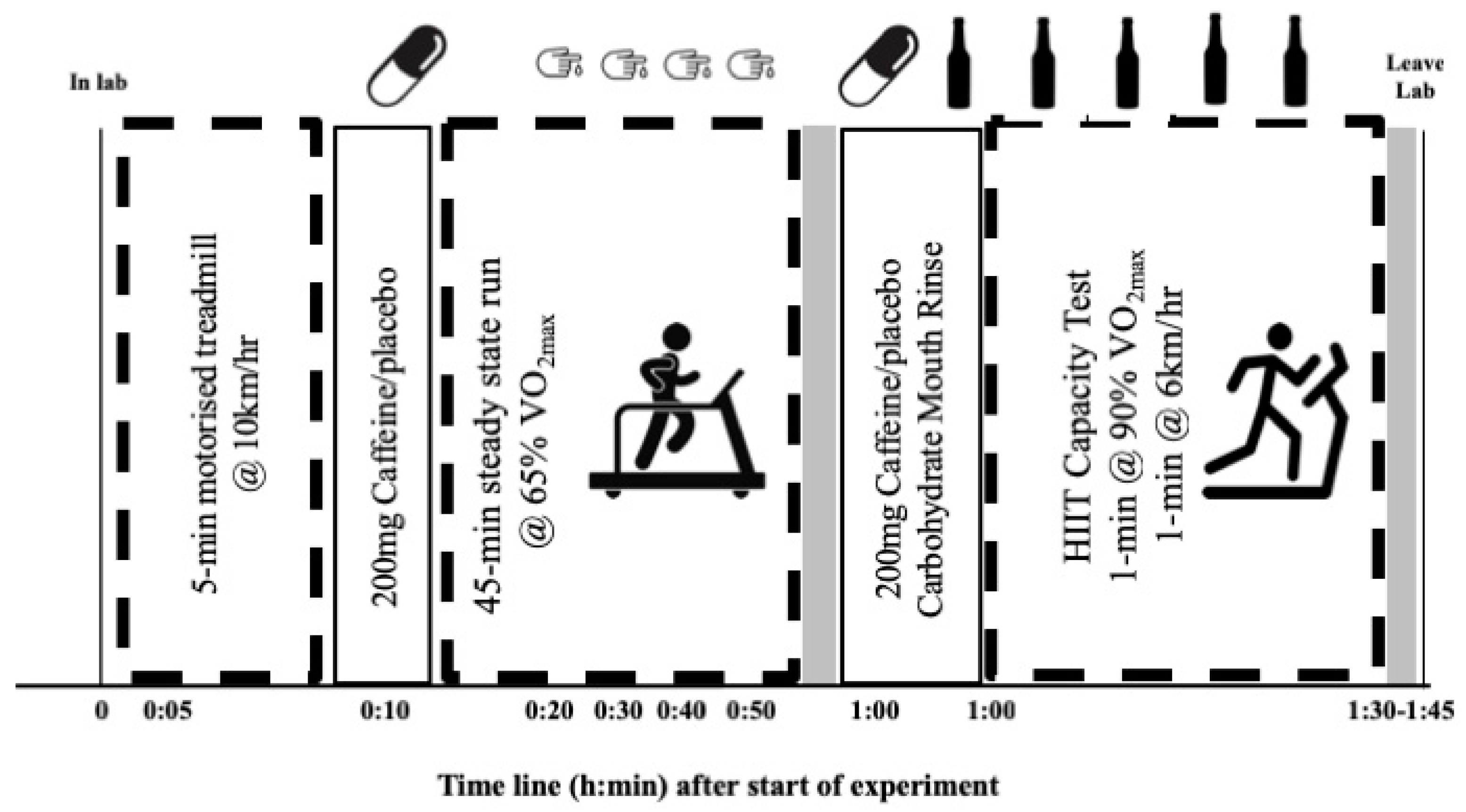
2.1. Experimental Design
2.2. Participants
2.3. Assessment of Anthropometrics and Maximal Oxygen Uptake
2.4. Steady-State Exercise and HIIT Running Protocol
2.5. Dietary Control and Blinding
2.6. Statistical Analysis
3. Results
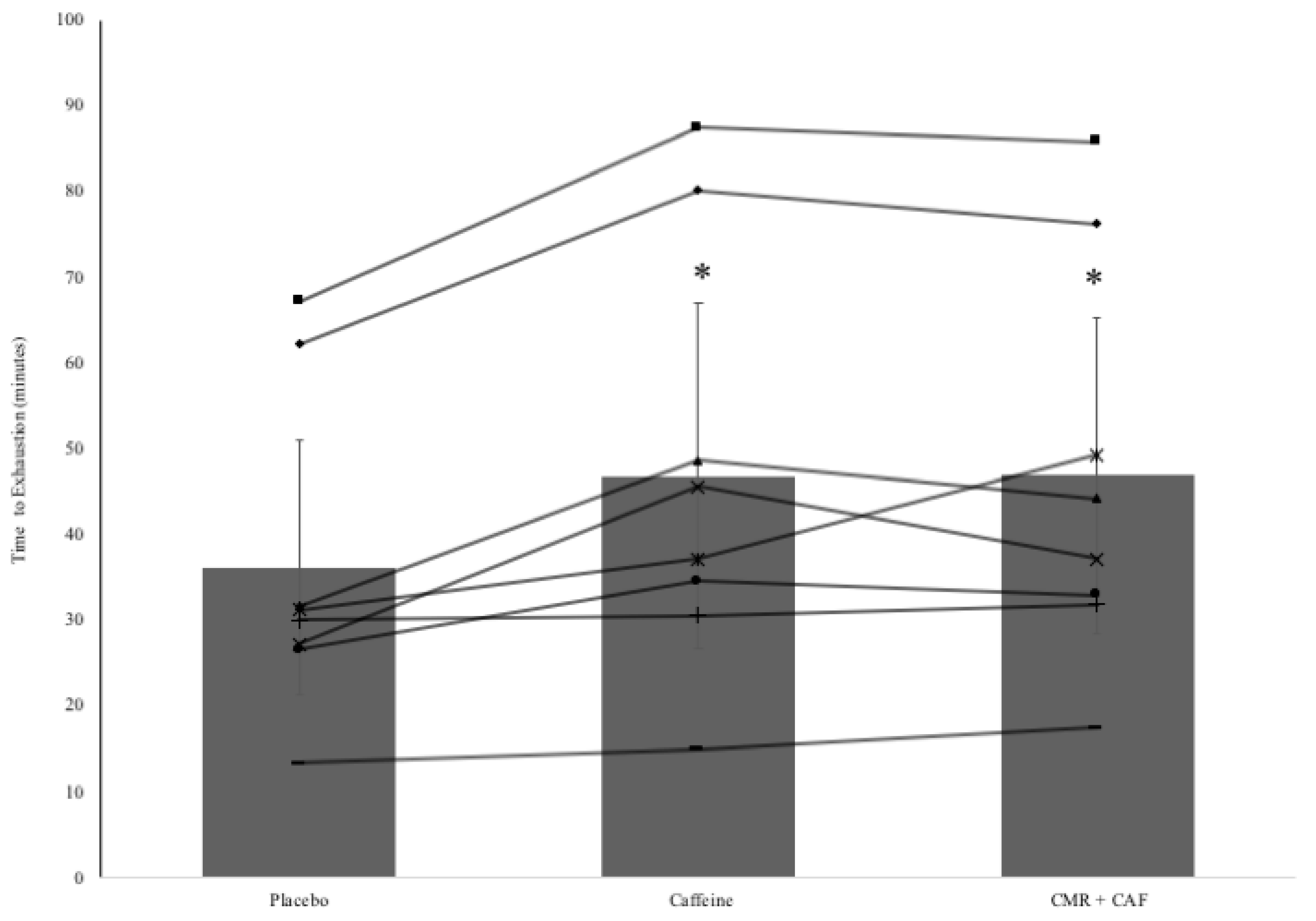
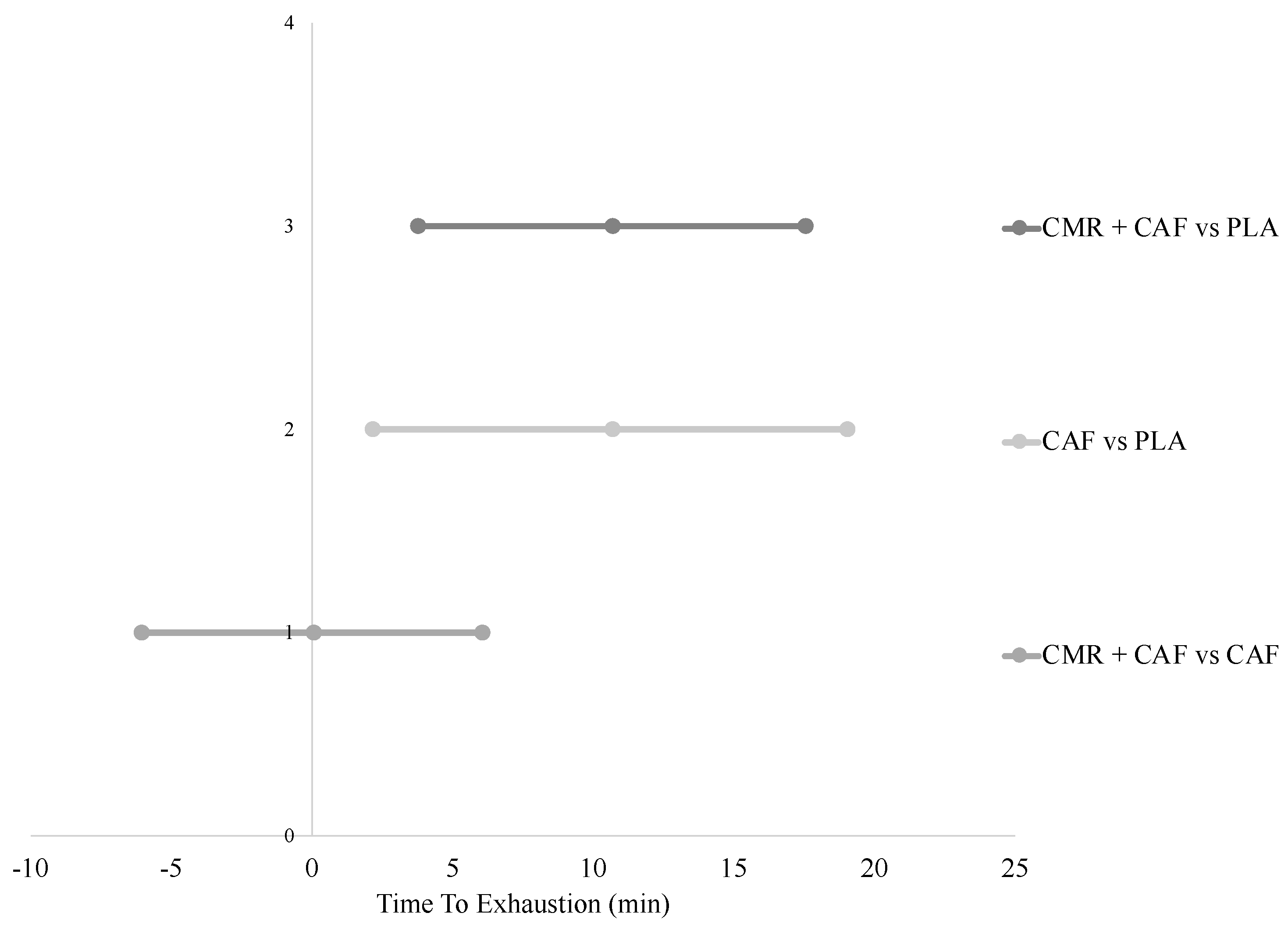
3.1. Exercise Capacity during HIIT
3.2. Physiological Responses during Steady State and HIIT
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chambers, E.S.; Bridge, M.W.; Jones, D.A. Carbohydrate sensing in the human mouth: Effects on exercise performance and brain activity. J. Physiol. 2009, 587, 1779–1794. [Google Scholar] [CrossRef]
- Carter, J.M.; Jeukendrup, A.E.; Jones, D.A. The effect of carbohydrate mouth rinse on 1-h cycle time trial performance. Med. Sci. Sports Exerc. 2004, 36, 2107–2111. [Google Scholar] [CrossRef]
- Whitham, M.; McKinney, J. Effect of a carbohydrate mouthwash on running time-trial performance. J. Sports Sci. 2007, 25, 1385–1392. [Google Scholar] [CrossRef]
- Beelen, M.; Berghuis, J.; Bonaparte, B.; Ballak, S.B.; Jeukendrup, A.E.; van Loon, L.J.C. Carbohydrate mouth rinsing in the fed state: Lack of enhancement of time-trial performance. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 400–409. [Google Scholar] [CrossRef]
- Fares, E.-J.M.; Kayser, B. Carbohydrate mouth rinse effects on exercise capacity in pre- and postprandial States. J. Nutr. Metab. 2011, 2011, 385962. [Google Scholar] [CrossRef]
- Lane, S.C.; Bird, S.R.; Burke, L.M.; Hawley, J.A. Effect of a carbohydrate mouth rinse on simulated cycling time-trial performance commenced in a fed or fasted state. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Métab. 2013, 38, 134–139. [Google Scholar] [CrossRef]
- Haase, L.; Cerf-Ducastel, B.; Murphy, C. Cortical activation in response to pure taste stimuli during the physiological states of hunger and satiety. Neuroimage 2009, 44, 1008–1021. [Google Scholar] [CrossRef] [Green Version]
- Kasper, A.M.; Cocking, S.; Cockayne, M.; Barnard, M.; Tench, J.; Parker, L.; McAndrew, J.; Langan-Evans, C.; Close, G.L.; Morton, J.P. Carbohydrate mouth rinse and caffeine improves high-intensity interval running capacity when carbohydrate restricted. Eur. J. Sport Sci. 2016, 16, 560–568. [Google Scholar] [CrossRef]
- Devenney, S.; Mangan, S.; Shortall, M.; Collins, K. Effects of carbohydrate mouth rinse and caffeine on high intensity interval running in a fed state. Appl. Physiol. Nutr. Metab. 2017, 43, 517–521. [Google Scholar] [CrossRef]
- Fredholm, B.B.; Bättig, K.; Holmén, J.; Nehlig, A.; Zvartau, E.E. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol. Rev. 1999, 51, 83–133. [Google Scholar]
- Doherty, M.; Smith, P.M. Effects of caffeine ingestion on exercise testing: A meta-analysis. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 626–646. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; Ridder, D.H. International Standards for Anthropometric Assessment; International Society for Advancement of Kinanthropometry: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Jones, A.M.; Doust, J.H. A 1% treadmill grade most accurately reflects the energetic cost of outdoor running. J. Sports Sci. 1996, 14, 321–327. [Google Scholar] [CrossRef]
- Akubat, I.; Barrett, S.; Abt, G. Integrating the Internal and External Training Loads in Soccer. Int. J. Sports Physiol. Perform. 2014, 9, 457–462. [Google Scholar] [CrossRef]
- Billat, V.L.; Morton, R.H.; Blondel, N.; Berthoin, S.; Bocquet, V.; Koralsztein, J.P.; Barstow, T.J. Oxygen kinetics and modelling of time to exhaustion whilst running at various velocities at maximal oxygen uptake. Eur. J. Appl. Physiol. 2000, 82, 178–187. [Google Scholar] [CrossRef]
- Conway, K.J.; Orr, R.; Stannard, S.R. Effect of a divided caffeine dose on endurance cycling performance, postexercise urinary caffeine concentration, and plasma paraxanthine. J. Appl. Physiol. 2003, 94, 1557–1562. [Google Scholar] [CrossRef] [Green Version]
- Naderi, A.; Earnest, C.P.; Lowery, R.P.; Wilson, J.M.; Willems, M.E.T. Co-ingestion of Nutritional Ergogenic Aids and High-Intensity Exercise Performance. Sport Med. 2016, 46, 1407–1418. [Google Scholar] [CrossRef]
- Mero, A.A.; Hirvonen, P.; Saarela, J.; Hulmi, J.J.; Hoffman, J.R.; Stout, J.R. Effect of sodium bicarbonate and beta-alanine supplementation on maximal sprint swimming. J. Int. Soc. Sports Nutr. 2013, 10, 52. [Google Scholar] [CrossRef]
- Christensen, P.M.; Petersen, M.H.; Friis, S.N.; Bangsbo, J. Caffeine, but not bicarbonate, improves 6 min maximal performance in elite rowers. Appl. Physiol. Nutr. Metab. 2014, 39, 1058–1063. [Google Scholar] [CrossRef]
- Kilding, A.E.; Overton, C.; Gleave, J. Effects of caffeine, sodium bicarbonate, and their combined ingestion on high-intensity cycling performance. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 175–183. [Google Scholar] [CrossRef]
- Felippe, L.C.; Lopes-Silva, J.P.; Bertuzzi, R.; McGinley, C.; Lima-Silva, A.E. Separate and Combined Effects of Caffeine and Sodium-Bicarbonate Intake on Judo Performance. Int. J. Sports Physiol. Perform. 2016, 11, 221–226. [Google Scholar] [CrossRef]
- Sinclair, J.; Bottoms, L.; Flynn, C.; Bradley, E.; Alexander, G.; McCullagh, S.; Finn, T.; Hurst, H.T. The effect of different durations of carbohydrate mouth rinse on cycling performance. Eur. J. Sport Sci. 2014, 14, 259–264. [Google Scholar] [CrossRef]
- Rollo, I.; Williams, C.; Nevill, M. Influence of ingesting versus mouth rinsing a carbohydrate solution during a 1-h run. Med. Sci. Sports Exerc. 2011, 43, 468–475. [Google Scholar] [CrossRef]
- de Souza Gonçalves, L.; de Salles Painelli, V.; Yamaguchi, G.; de Oliveira, L.F.; Saunders, B.; da Silva, R.P.; Maciel, E.; Artioli, G.G.; Roschel, H.; Gualano, B. Dispelling the myth that habitual caffeine consumption influences the performance response to acute caffeine supplementation. Am. J. Physiol.-Heart Circ. Physiol. 2017. [Google Scholar] [CrossRef]
- Pickering, C.; Kiely, J. What Should We Do About Habitual Caffeine Use in Athletes? Sports Med. 2018. [Google Scholar] [CrossRef]
- Dark, H.E.; Kamimori, G.H.; LaValle, C.R.; Eonta, S.E. Effects of high habitual caffeine use on performance during one night of sleep deprivation: Do high users need larger doses to maintain vigilance? J. Caffeine Res. 2015, 5, 155–166. [Google Scholar] [CrossRef]
- Evans, M.; Tierney, P.; Gray, N.; Hawe, G.; Macken, M.; Egan, B. Acute Ingestion of Caffeinated Chewing Gum Improves Repeated Sprint Performance of Team Sport Athletes with Low Habitual Caffeine Consumption. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 221–227. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Measure | 5 | 10 | 20 | 30 | 40 | 45 | Exh | |
|---|---|---|---|---|---|---|---|---|
| Heart Rate | Placebo | 153 ± 12 | 161 ± 10 | 167 ± 14 | 170 ± 15 | 170 ± 14 | 171 ± 15* | 190 ± 6* |
| CHO | 152 ± 10 | 160 ± 9 | 165 ± 15 | 167 ± 10 | 170 ± 11 | 172 ± 12* | 189 ± 6* | |
| CHO + Caff | 150 ± 10 | 158 ± 12 | 165 ± 11 | 170 ± 9 | 173 ± 12 | 174 ± 16* | 191 ± 17* | |
| Lactate | Placebo | 2.5 ± 1.4 | 2.3 ± 1.1 | 2.6 ± 1.2 | 2.6 ± 1.3 | 2.5 ± 1.4 | 2.4 ± 1.3 | 10.3 ± 2.8* |
| CHO | 1.9 ± 0.9 | 2.2 ± 1.1 | 2.0 ± 0.9 | 2.0 ± 1.0 | 2.0 ± 1.1 | 2.2 ± 1.0 | 10.4 ± 2.3* | |
| CHO + Caff | 1.9 ± 1.1 | 2.1 ± 0.7 | 2.3 ± 1.2 | 2.6 ± 1.2 | 3.0 ± 1.5 | 2.5 ± 1.4 | 10.8 ± 3.0* | |
| RPE | Placebo | 10 ± 2 | 10 ± 3 | 11 ± 2 | 13 ± 2 | 14 ± 3 | 14 ± 3* | 20 ± 1* |
| CHO | 8 ± 2 | 10 ± 2 | 12 ± 2 | 14 ± 3 | 14 ± 2 | 14 ± 3* | 20 ± 1* | |
| CHO + Caff | 9 ± 3 | 11 ± 2 | 11 ± 3 | 13 ± 1 | 13 ± 2 | 14 ± 2* | 20 ± 1* | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Germaine, M.; Collins, K.; Shortall, M. The Effect of Caffeine Ingestion and Carbohydrate Mouth Rinse on High-Intensity Running Performance. Sports 2019, 7, 63. https://doi.org/10.3390/sports7030063
Germaine M, Collins K, Shortall M. The Effect of Caffeine Ingestion and Carbohydrate Mouth Rinse on High-Intensity Running Performance. Sports. 2019; 7(3):63. https://doi.org/10.3390/sports7030063
Chicago/Turabian StyleGermaine, Mark, Kieran Collins, and Marcus Shortall. 2019. "The Effect of Caffeine Ingestion and Carbohydrate Mouth Rinse on High-Intensity Running Performance" Sports 7, no. 3: 63. https://doi.org/10.3390/sports7030063
APA StyleGermaine, M., Collins, K., & Shortall, M. (2019). The Effect of Caffeine Ingestion and Carbohydrate Mouth Rinse on High-Intensity Running Performance. Sports, 7(3), 63. https://doi.org/10.3390/sports7030063