Short-Term Cardiac Autonomic Recovery after a Repeated Sprint Test in Young Soccer Players

 , ,
, , 

{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. HRV Analysis
2.3. Repeated Sprint Ability Test
2.4. Statistical Analysis
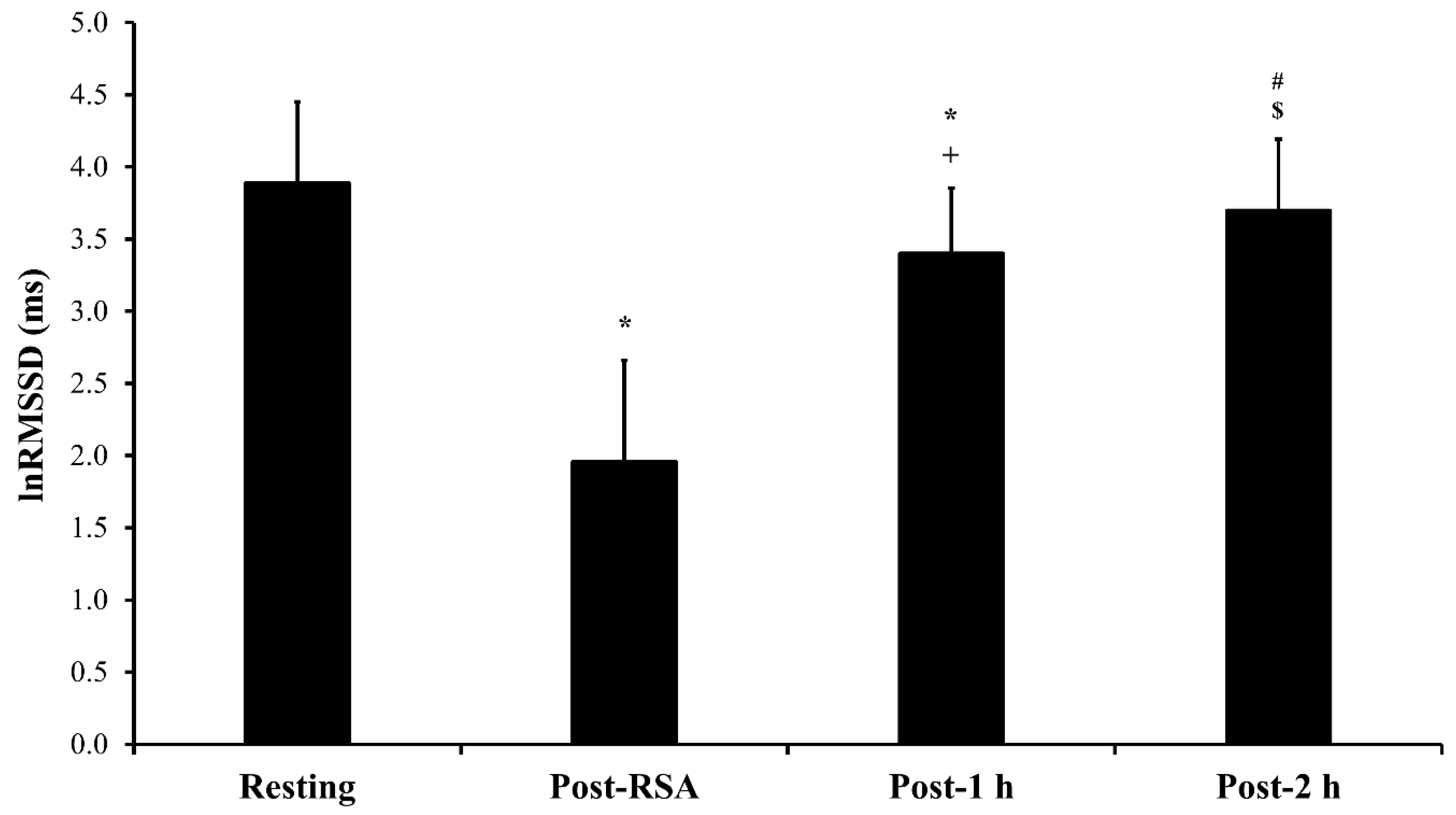
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Bishop, D.; Girard, O.; Mendez-Villanueva, A. Repeated-sprint ability—Part II. Sports Med. 2011, 41, 741–756. [Google Scholar] [CrossRef]
- Loturco, I.; Abad, C.C.C.; Jeleilate, D.; Falcão, D.; Fachina, R.; Kitamura, K.; Kobal, R.; Pereira, L.A.; Nakamura, F.Y. Differences in fitness characteristics between Brazilian World Championship and South-American Championship National basketball teams. J. Sports Med. Phys. Fitness 2015, 56, 1428–1429. [Google Scholar]
- Girard, O.; Mendez-Villanueva, A.; Bishop, D. Repeated-sprint ability—Part I. Sports Med. 2011, 41, 673–694. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Moiz, J.A.; Shareef, M.Y.; Husain, M.E. Physical performance and markers of muscle damage following sports specific sprints in male collegiate soccer players: Repeated bout effect. J. Sports Med. Phys. Fitness 2015, 56, 765–774. [Google Scholar] [PubMed]
- Buchheit, M.; Laursen, P.B.; Ahmaidi, S. Parasympathetic reactivation after repeated sprint exercise. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H133–H141. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, F.Y.; Soares-Caldeira, L.F.; Laursen, P.B.; Polito, M.D.; Leme, L.C.; Buchheit, M. Cardiac autonomic responses to repeated shuttle sprints. Int. J. Sports Med. 2009, 30, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.S.; Liao, C.J.; Lu, W.A.; Kuo, C.D. Sympathetic enhancement in futsal players but not in football players after repeated sprint ability test. BMJ Open Sport Exerc. Med. 2015, 1, e000049. [Google Scholar] [CrossRef]
- Mascarin, R.B.; De Andrade, V.L.; Barbieri, R.A.; Loures, J.P.; Kalva-Filho, C.A.; Papoti, M. Dynamics of Recovery of Physiological Parameters After a Small-Sided Game in Women Soccer Players. Front. Physiol. 2018, 9, 887. [Google Scholar] [CrossRef] [PubMed]
- Vernillo, G.; Agnello, L.; Barbuti, A.; Di Meco, S.; Lombardi, G.; Merati, G.; La Torre, A. Postexercise autonomic function after repeated-sprints training. Eur. J. Appl. Physiol. 2015, 115, 2445–2455. [Google Scholar] [CrossRef]
- Flatt, A.A.; Esco, M.R.; Allen, J.R.; Robinson, J.B.; Earley, R.L.; Fedewa, M.V.; Bragg, A.; Keith, C.M.; Wingo, J.E. Heart rate variability and training load among national collegiate athletic association division 1 college football players throughout spring camp. J. Strength Cond. Res. 2018, 32, 3127–3134. [Google Scholar] [CrossRef]
- Schneider, C.; Hanakam, F.; Wiewelhove, T.; Döweling, A.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Heart rate monitoring in team sports—A conceptual framework for contextualizing heart rate measures for training and recovery prescription. Front. Physiol. 2018, 9, 639. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Papelier, Y.; Laursen, P.B.; Ahmaidi, S. Noninvasive assessment of cardiac parasympathetic function: Postexercise heart rate recovery or heart rate variability? Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H8–H10. [Google Scholar] [CrossRef] [PubMed]
- Flatt, A.A.; Howells, D. Effects of varying training load on heart rate variability and running performance among an Olympic rugby sevens team. J. Sci. Med. Sport 2019, 22, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Bisschoff, C.A.; Coetzee, B.; Esco, M.R. Heart rate variability and recovery as predictors of elite, African, male badminton players’ performance levels. Int. J. Perform. Anal. Sport 2018, 18, 1–16. [Google Scholar] [CrossRef]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; Tulppo, M.P. Endurance training guided individually by daily heart rate variability measurements. Eur. J. Appl. Physiol. 2007, 101, 743–751. [Google Scholar] [CrossRef]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; Nissilä, J.; Virtanen, P.; Karjalainen, J.; Tulppo, M.P. Daily exercise prescription on the basis of HR variability among men and women. Med. Sci. Sports Exerc. 2010, 42, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Vesterinen, V.; Nummela, A.; Heikura, I.; Laine, T.; Hynynen, E.; Botella, J.; Häkkinen, K. Individual endurance training prescription with heart rate variability. Med. Sci. Sports Exerc. 2016, 48, 1347–1354. [Google Scholar] [CrossRef]
- Da Silva, D.F.; Ferraro, Z.M.; Adamo, K.B.; Machado, F.A. Endurance Running Training Individually Guided by HRV in Untrained Women. J. Strength Cond. Res. 2019, 33, 736–746. [Google Scholar] [CrossRef]
- Javaloyes, A.; Sarabia, J.M.; Lamberts, R.P.; Moya-Ramon, M. Training Prescription Guided by Heart-Rate Variability in Cycling. Int. J. Sports Physiol. Perform. 2019, 14, 23–32. [Google Scholar] [CrossRef]
- Bangsbo, J. The physiology of soccer—With special reference to intense intermittent exercise. Acta Physiol. Scand. 1994, 619, 1–155. [Google Scholar]
- Seiler, S.; Haugen, O.; Kuffel, E. Autonomic recovery after exercise in trained athletes: Intensity and duration effects. Med. Sci. Sports Exerc. 2007, 39, 1366–1373. [Google Scholar] [CrossRef] [PubMed]
- Stanley, J.; Peake, J.M.; Buchheit, M. Cardiac parasympathetic reactivation following exercise: Implications for training prescription. Sport Med. 2013, 43, 1259–1277. [Google Scholar] [CrossRef] [PubMed]
- Rampinini, E.; Bishop, D.; Marcora, S.M.; Ferrari Bravo, D.; Sassi, R.; Impellizzeri, F.M. Validity of simple field tests as indicators of match-related physical performance in top-level professional soccer players. Int. J. Sports Med. 2007, 28, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Batterham, A.M.; Hopkins, W.G. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef]
- Ferrari Bravo, D.; Impellizzeri, F.M.; Rampinini, E.; Castagna, C.; Bishop, D.; Wisloff, U. Sprint vs. interval training in football. Int. J. Sports Med. 2008, 29, 668–674. [Google Scholar] [CrossRef]
- Buchheit, M.; Voss, S.C.; Nybo, L.; Mohr, M.; Racinais, S. Physiological and performance adaptations to an in-season soccer camp in the heat: Associations with heart rate and heart rate variability. Scand. J. Med. Sci. Sports 2011, 21, e477–e485. [Google Scholar] [CrossRef]
- Buchheit, M.; Millet, G.P.; Parisy, A.; Pourchez, S.; Laursen, P.B.; Ahmaidi, S. Supramaximal training and postexercise parasympathetic reactivation in adolescents. Med. Sci. Sports Exerc. 2008, 40, 362–371. [Google Scholar] [CrossRef]
- Niewiadomski, W.; Gasiorowska, A.; Krauss, B.; Mróz, A.; Cybulski, G. Suppression of heart rate variability after supramaximal exertion. Clin. Physiol. Funct. Imaging 2007, 27, 309–319. [Google Scholar] [CrossRef]
- Al Haddad, H.; Laursen, P.B.; Chollet, D.; Lemaitre, F.; Ahmaidi, S.; Buchheit, M. Effect of cold or thermoneutral water immersion on post-exercise heart rate recovery and heart rate variability indices. Auton. Neurosci. 2010, 156, 111–116. [Google Scholar] [CrossRef]
- Buchheit, M.; Peiffer, J.J.; Abbiss, C.R.; Laursen, P.B. Effect of cold water immersion on postexercise parasympathetic reactivation. Am. J. Physiol. Heart Circ. Physiol. 2009, 296, H421–H427. [Google Scholar] [CrossRef]
- De Oliveira Ottone, V.; de Castro Magalhães, F.; de Paula, F.; Avelar, N.C.; Aguiar, P.F.; da Matta Sampaio, P.F.; Duarte, T.C.; Costa, K.B.; Araújo, T.L.; Coimbra, C.C.; et al. The effect of different water immersion temperatures on post-exercise parasympathetic reactivation. PLoS ONE 2014, 9, e113730. [Google Scholar] [CrossRef]
- Buchheit, M.; Gindre, C. Cardiac parasympathetic regulation: Respective associations with cardiorespiratory fitness and training load. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H451–H458. [Google Scholar] [CrossRef]
- Cook, C.J.; Beaven, C.M. Individual perception of recovery is related to subsequent sprint performance. Br. J. Sports Med. 2013, 47, 705–709. [Google Scholar] [CrossRef]
- Fürholz, M.; Radtke, T.; Roten, L.; Tanner, H.; Wilhelm, I.; Schmid, J.P.; Saner, H.; Wilhelm, M. Training-related modulations of the autonomic nervous system in endurance athletes: Is female gender cardioprotective? Eur. J. Appl. Physiol. 2013, 113, 631–640. [Google Scholar] [CrossRef]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abad, C.C.C.; Pereira, L.A.; Zanetti, V.; Kobal, R.; Loturco, I.; Nakamura, F.Y. Short-Term Cardiac Autonomic Recovery after a Repeated Sprint Test in Young Soccer Players. Sports 2019, 7, 102. https://doi.org/10.3390/sports7050102
Abad CCC, Pereira LA, Zanetti V, Kobal R, Loturco I, Nakamura FY. Short-Term Cardiac Autonomic Recovery after a Repeated Sprint Test in Young Soccer Players. Sports. 2019; 7(5):102. https://doi.org/10.3390/sports7050102
Chicago/Turabian StyleAbad, Cesar Cavinato Cal, Lucas Adriano Pereira, Vinicius Zanetti, Ronaldo Kobal, Irineu Loturco, and Fabio Yuzo Nakamura. 2019. "Short-Term Cardiac Autonomic Recovery after a Repeated Sprint Test in Young Soccer Players" Sports 7, no. 5: 102. https://doi.org/10.3390/sports7050102
APA StyleAbad, C. C. C., Pereira, L. A., Zanetti, V., Kobal, R., Loturco, I., & Nakamura, F. Y. (2019). Short-Term Cardiac Autonomic Recovery after a Repeated Sprint Test in Young Soccer Players. Sports, 7(5), 102. https://doi.org/10.3390/sports7050102