The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players




Abstract
:1. Introduction
2. Materials and Methods
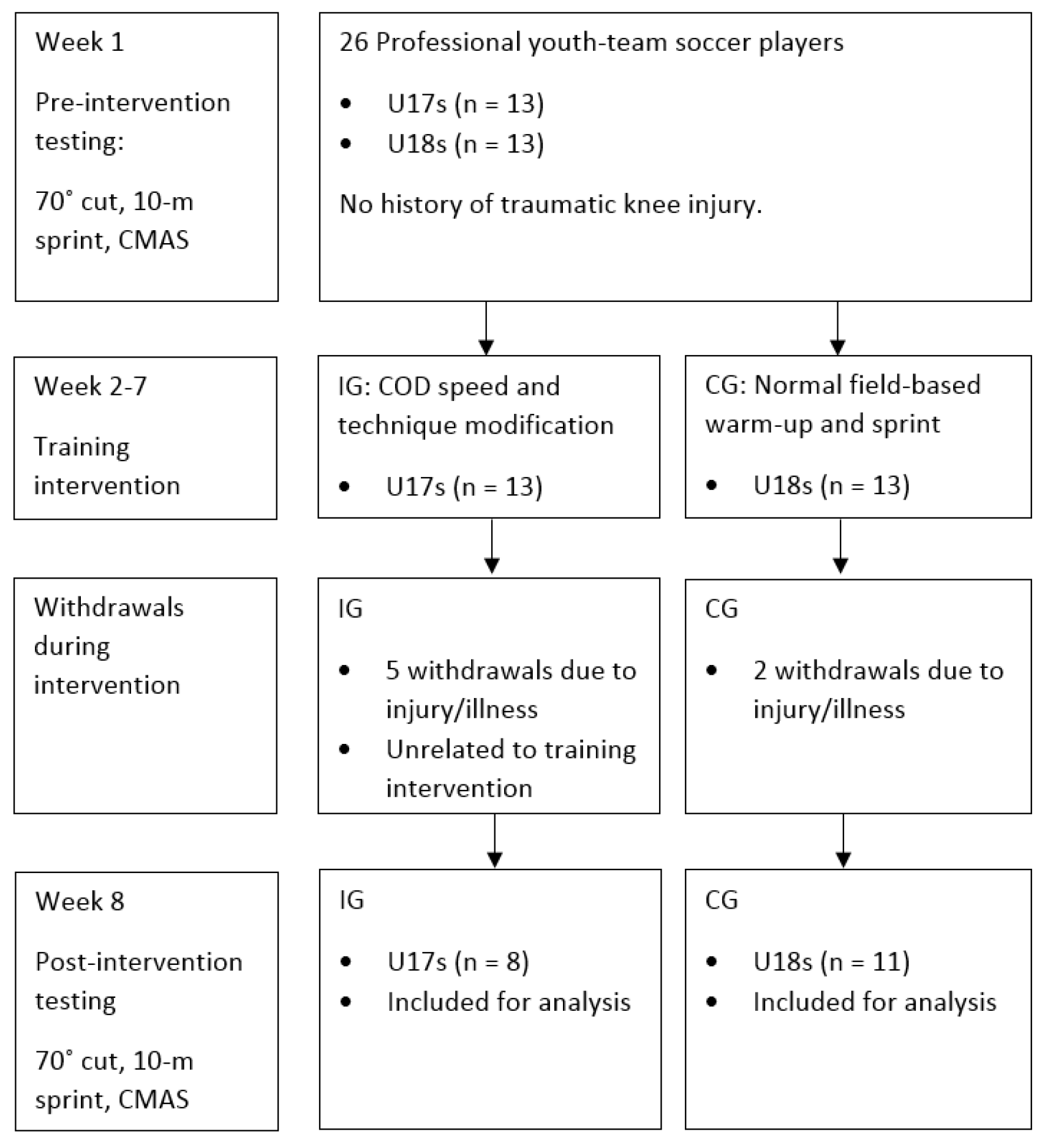
2.1. Research Design
2.2. Participants
2.3. Procedures and Field Tests
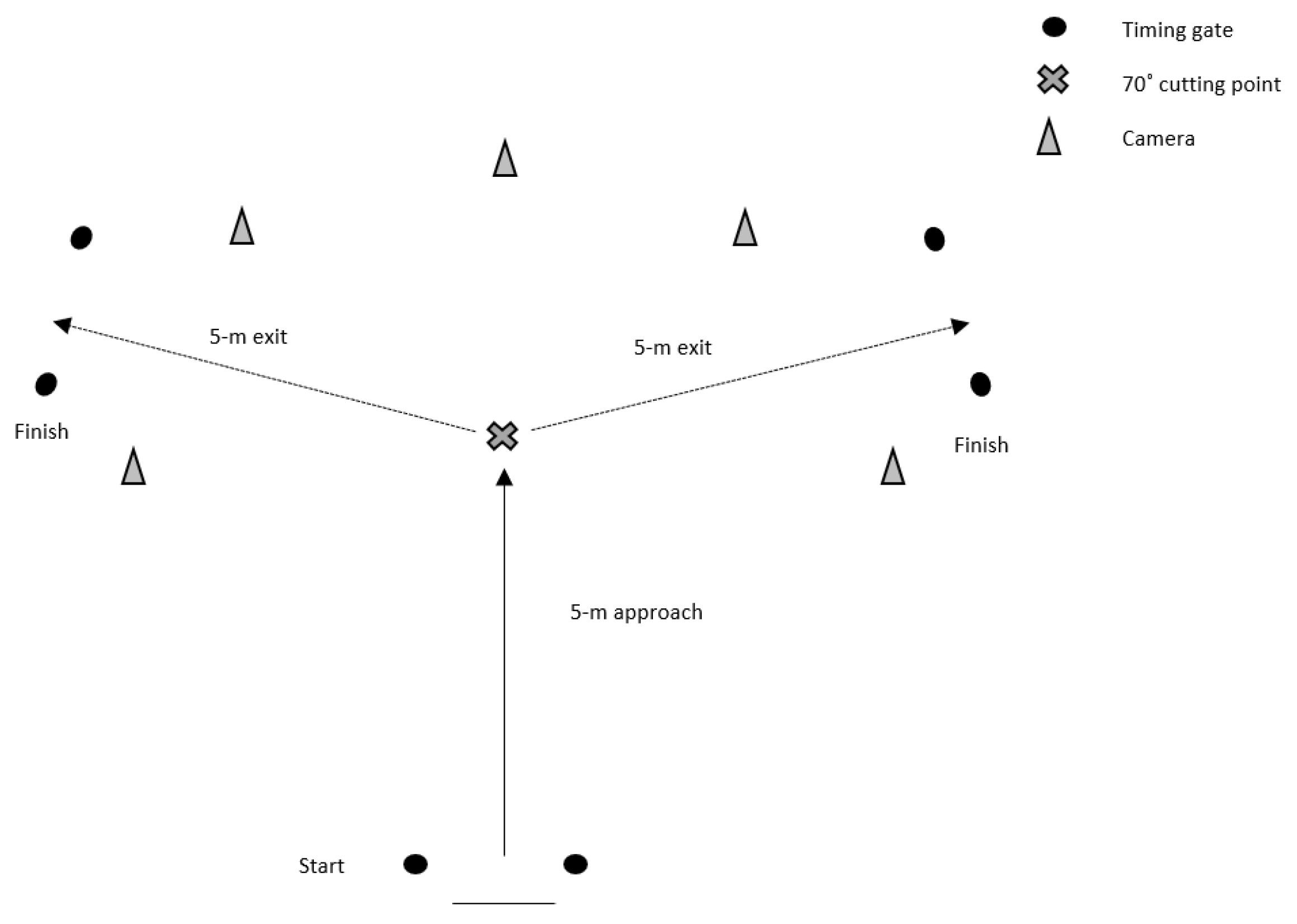
2.3.1. 70° Cutting Task
2.3.2. The 10 m Sprint
2.3.3. COD Deficit
2.3.4. CMAS Screening
2.3.5. Six-Week COD Speed and Technique Modification Training Intervention
2.4. Statistical Analyses
3. Results
3.1. Reliability
- Excellent intra- (ICC = 0.972, SEM = 0.32, SDD = 0.88) and inter-rater reliability (ICC = 0.917, SEM = 0.38, SDD = 1.05) was observed for CMAS total score.
- Excellent intra- (≥92.3%, k ≥ 0.866) and inter-rater (≥89.5% k ≥ 0.872) percentage-agreements and kappa coefficients were demonstrated for all CMAS variables (Table 2), with the exception of penultimate foot contact (PFC) braking (k = 0.755) and initial knee valgus position (k = 0.789) which demonstrated good kappa coefficients.
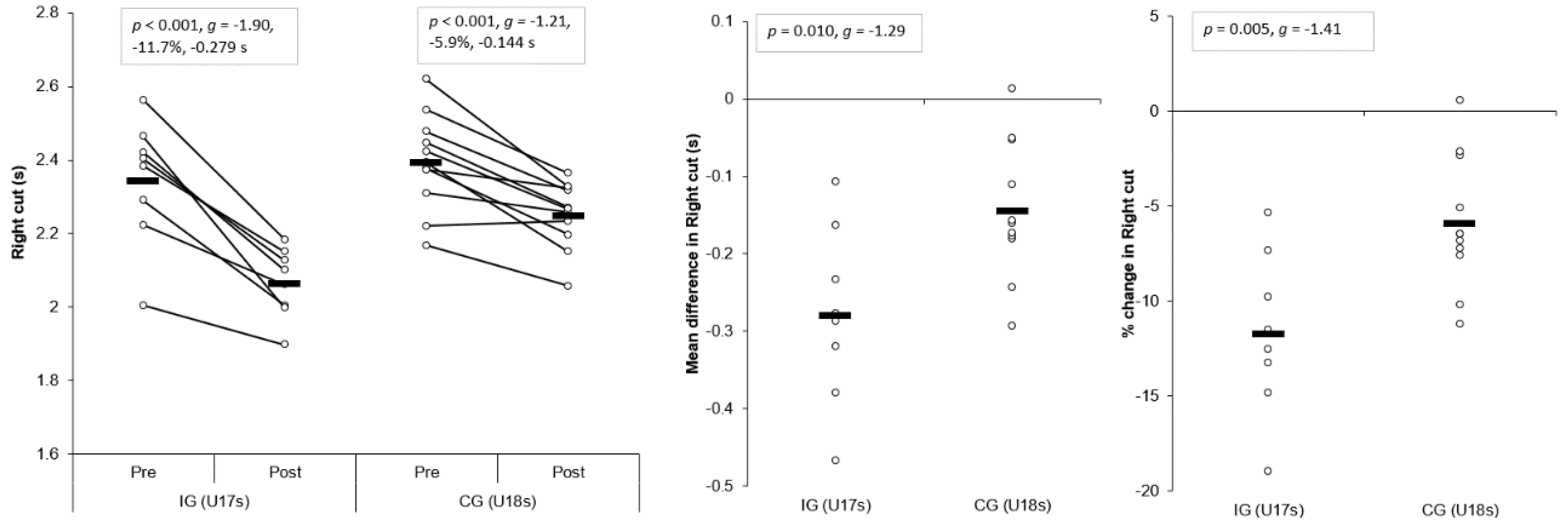
3.1.1. Right Cut
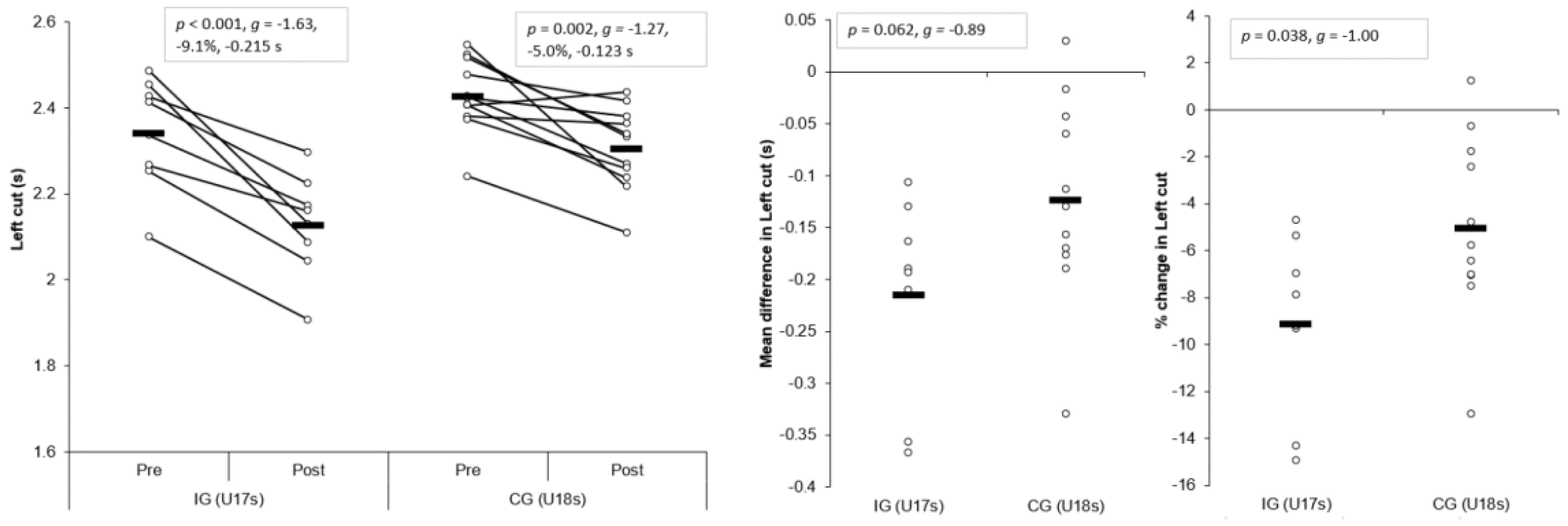
3.1.2. Left Cut
3.1.3. Right COD Deficit (CODD)
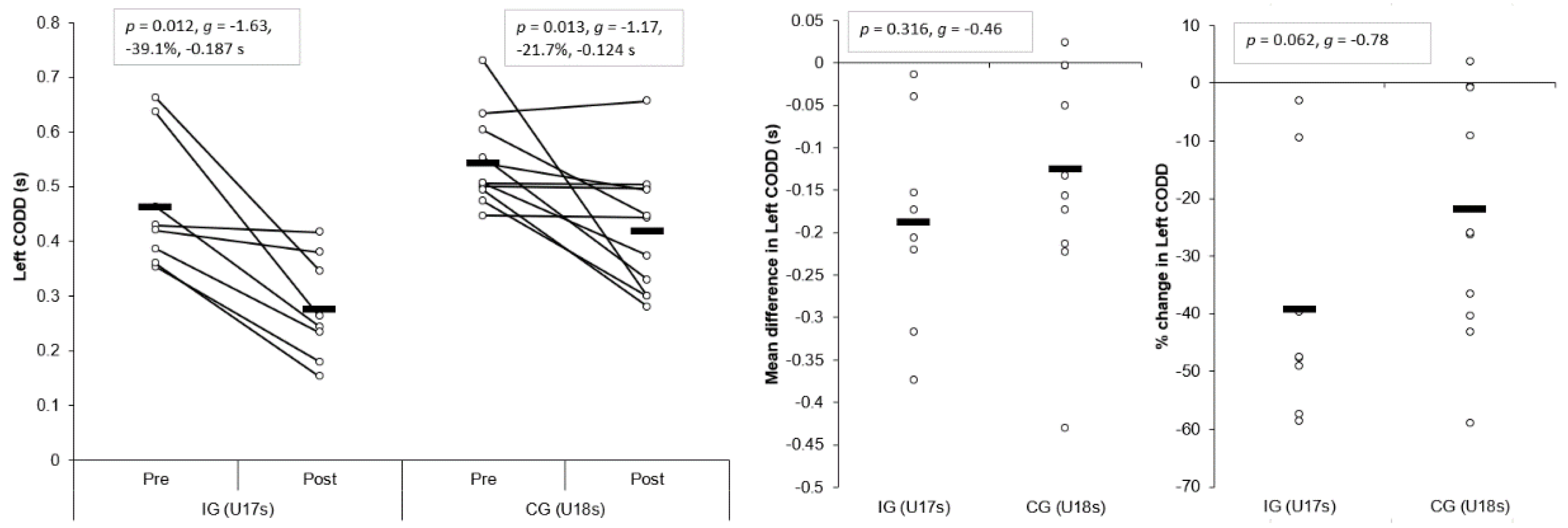
3.1.4. Left CODD
3.1.5. The 10 m Sprint
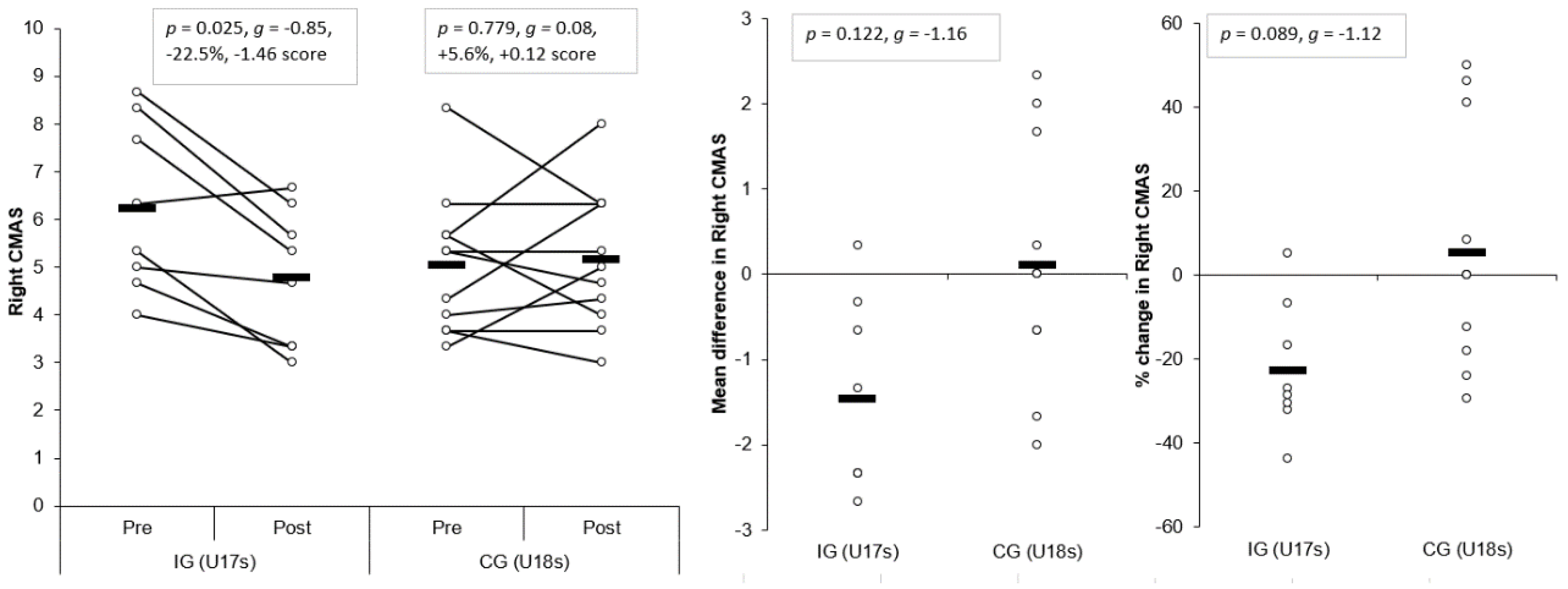
3.1.6. CMAS Right
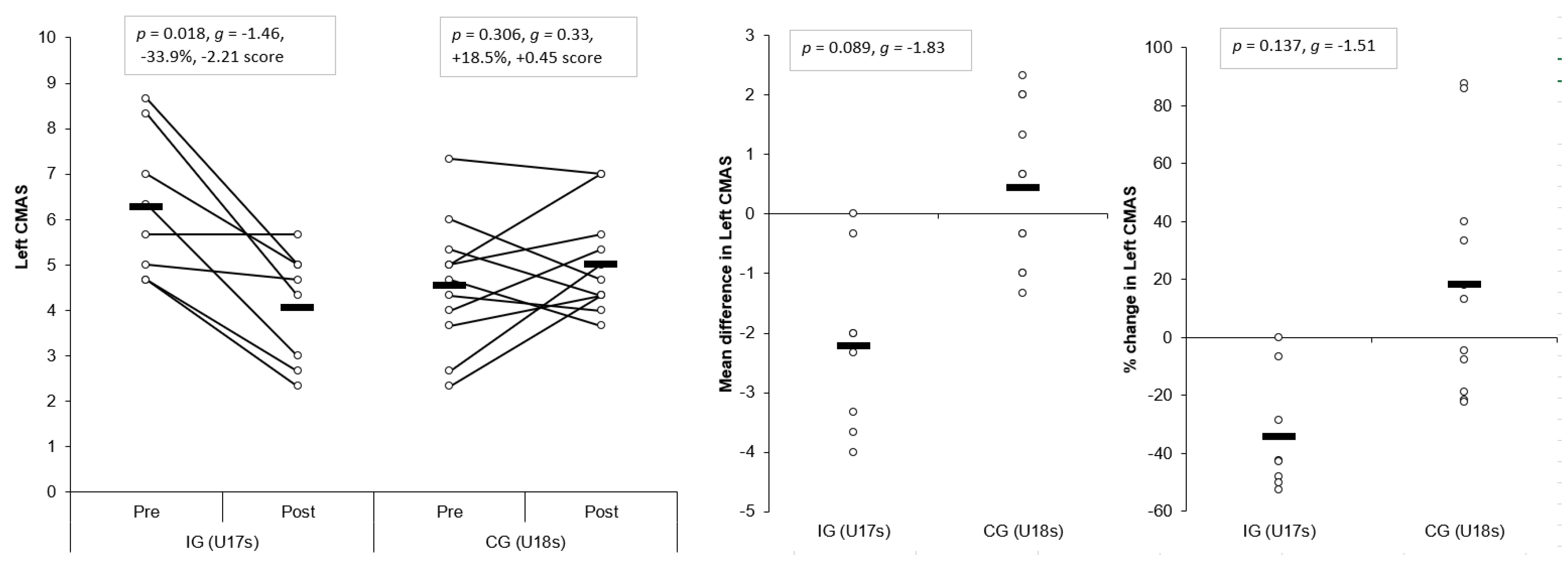
3.1.7. CMAS Left
3.2. Task Specific Changes in Cutting Movement Quality: CMAS Deficit Changes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bloomfield, J.; Polman, R.; Donoghue, P. Physical demands of different positions in fa premier league soccer. J. Sport Sci. Med. 2007, 6, 63–70. [Google Scholar]
- Robinson, G.; O’Donoghue, P.; Nielson, P. Path changes and injury risk in english fa premier league soccer. Int. J. Perform. Anal. Sport 2011, 11, 40–56. [Google Scholar] [CrossRef]
- Faude, O.; Koch, T.; Meyer, T. Straight sprinting is the most frequent action in goal situations in professional football. J. Sports Sci. 2012, 30, 625–631. [Google Scholar] [CrossRef]
- Jones, P.; Bampouras, T.M.; Marrin, K. An investigation into the physical determinants of change of direction speed. J. Sports Med. Phys. Fit. 2009, 49, 97–104. [Google Scholar]
- Nimphius, S. Training change of direction and agility. In Advanced Strength and Conditioning; Turner, A., Comfort, P., Eds.; Routledge: Abdingdon, UK, 2018; pp. 291–308. [Google Scholar]
- Chaouachi, A.; Chtara, M.; Hammami, R.; Chtara, H.; Turki, O.; Castagna, C. Multidirectional sprints and small-sided games training effect on agility and change of direction abilities in youth soccer. J. Strength Cond. Res. 2014, 28, 3121–3127. [Google Scholar] [CrossRef]
- Chaalali, A.; Rouissi, M.; Chtara, M.; Owen, A.; Bragazzi, N.; Moalla, W.; Chaouachi, A.; Amri, M.; Chamari, K. Agility training in young elite soccer players: Promising results compared to change of direction drills. Biol. Sport 2016, 33, 345. [Google Scholar] [CrossRef]
- Chtara, M.; Rouissi, M.; Haddad, M.; Chtara, H.; Chaalali, A.; Owen, A.; Chamari, K. Specific physical trainability in elite young soccer players: Efficiency over 6 weeks’ in-season training. Biol. Sport 2017, 34, 137–148. [Google Scholar] [CrossRef]
- Garcia-Ramos, A.; Haff, G.G.; Feriche, B.N.; Jaric, S. Effects of different conditioning programmes on the performance of high-velocity soccer-related tasks: Systematic review and meta-analysis of controlled trials. Int. J. Sports Sci. Coach. 2017, 13, 129–151. [Google Scholar] [CrossRef]
- Grassi, A.; Smiley, S.P.; Roberti di Sarsina, T.; Signorelli, C.; Marcheggiani Muccioli, G.M.; Bondi, A.; Romagnoli, M.; Agostini, A.; Zaffagnini, S. Mechanisms and situations of anterior cruciate ligament injuries in professional male soccer players: A youtube-based video analysis. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 697–981. [Google Scholar] [CrossRef]
- Walden, M.; Krosshaug, T.; Bjorneboe, J.; Andersen, T.E.; Faul, O.; Hagglund, M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: A systematic video analysis of 39 cases. Br. J. Sports Med. 2015, 49, 1452–1460. [Google Scholar] [CrossRef]
- Brophy, R.H.; Stepan, J.G.; Silvers, H.J.; Mandelbaum, B.R. Defending puts the anterior cruciate ligament at risk during soccer: A gender-based analysis. Sports Health 2015, 7, 244–249. [Google Scholar] [CrossRef]
- Dempsey, A.R.; Lloyd, D.G.; Elliott, B.C.; Steele, J.R.; Munro, B.J. Changing sidestep cutting technique reduces knee valgus loading. Am. J. Sport Med. 2009, 37, 2194–2200. [Google Scholar] [CrossRef]
- Fox, A. Change-of-direction biomechanics: Is what’s best for anterior cruciate ligament injury prevention also best for performance? Sports Med. 2018, 48, 1799–1807. [Google Scholar] [CrossRef]
- Markolf, K.L.; Burchfield, D.M.; Shapiro, M.M.; Shepard, M.F.; Finerman, G.A.M.; Slauterbeck, J.L. Combined knee loading states that generate high anterior cruciate ligament forces. J. Orthop. Res. 1995, 13, 930–935. [Google Scholar] [CrossRef]
- Lloyd, D.G. Rationale for training programs to reduce anterior cruciate ligament injuries in australian football. J. Orthop. Sport Phys. 2001, 31, 645–654. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; Di Stasi, S.L.; Foss, K.D.B.; Micheli, L.J.; Hewett, T.E. High knee abduction moments are common risk factors for patellofemoral pain (pfp) and anterior cruciate ligament (acl) injury in girls: Is pfp itself a predictor for subsequent acl injury? Br. J. Sports Med. 2015, 49, 118–122. [Google Scholar] [CrossRef]
- O’Kane, J.W.; Neradilek, M.; Polissar, N.; Sabado, L.; Tencer, A.; Schiff, M.A. Risk factors for lower extremity overuse injuries in female youth soccer players. Orthop. J. Sports Med. 2017, 5, 2325967117733963. [Google Scholar] [CrossRef]
- Waldén, M.; Hägglund, M.; Magnusson, H.; Ekstrand, J. Acl injuries in men’s professional football: A 15-year prospective study on time trends and return-to-play rates reveals only 65% of players still play at the top level 3 years after acl rupture. Br. J. Sports Med. 2016, 50, 744–750. [Google Scholar] [CrossRef]
- Hewett, T. Preventive biomechanics: A paradigm shift with a translational approach to biomechanics. Am. J. Sports Med. 2017, 45, 2654–2664. [Google Scholar] [CrossRef]
- Padua, D.A.; DiStefano, L.J.; Hewett, T.E.; Garrett, W.E.; Marshall, S.W.; Golden, G.M.; Shultz, S.J.; Sigward, S.M. National athletic trainers’ association position statement: Prevention of anterior cruciate ligament injury. J. Athl. Train. 2018, 53, 5–19. [Google Scholar] [CrossRef]
- Dos’Santos, T.; McBurnie, A.; Thomas, C.; Comfort, P.; Jones, P. Biomechanical comparison of cutting techniques: A review and practical applications. Strength Cond. J. 2019, 41, 40–54. [Google Scholar] [CrossRef]
- Marshall, B.M.; Franklyn-Miller, A.D.; King, E.A.; Moran, K.A.; Strike, S.; Falvey, A. Biomechanical factors associated with time to complete a change of direction cutting maneuver. J. Strength Cond. Res. 2014, 28, 2845–2851. [Google Scholar] [CrossRef]
- Havens, K.; Sigward, S.M. Cutting mechanics: Relation to performance and anterior cruciate ligament injury risk. Med. Sci. Sports Exerc. 2015, 47, 818–824. [Google Scholar] [CrossRef]
- Jones, P.A.; Barber, O.R.; Smith, L.C. Changing Pivoting Technique Reduces Knee Valgus Moments. Free Communication. J. Sports Sci. 2015, 33, S62. [Google Scholar]
- Celebrini, R.G.; Eng, J.J.; Miller, W.C.; Ekegren, C.L.; Johnston, J.D.; MacIntyre, D.L. The effect of a novel movement strategy in decreasing acl risk factors in female adolescent soccer players. J. Strength Cond. Res. 2012, 26, 3406–3417. [Google Scholar] [CrossRef]
- Dos’Santos, T.; Thomas, C.; Comfort, P.; Jones, P.A. The effect of angle and velocity on change of direction biomechanics: An angle-velocity trade-off. Sports Med. 2018, 48, 2235–2253. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; Croix, M.B.D.S.; Myer, G.D.; Lloyd, R.S. Neuromuscular risk factors for knee and ankle ligament injuries in male youth soccer players. Sports Med. 2016, 46, 1059–1066. [Google Scholar] [CrossRef]
- Jones, P.A.; Donelon, T.; Dos’ Santos, T. A preliminary investigation into a qualitative assessment tool to identify athletes with high knee abduction moments during cutting: Cutting movement assessment score (cmas). Prof. Strength Cond. 2017, 47, 37–42. [Google Scholar]
- Dos’Santos, T.; McBurnie, A.; Donelon, T.; Thomas, C.; Comfort, P.; Jones, P.A. A qualitative screening tool to identify athletes with “high-risk” movement mechanics during cutting: The cutting movement assessment score (cmas). Phys. Sport 2019, 38, 152–161. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.; Myer, G.D.; Lloyd, R.S. An audit of injuries in six english professional soccer academies. J. Sports Sci. 2018, 36, 1542–1548. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using g* power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Beck, T.W. The importance of a priori sample size estimation in strength and conditioning research. J. Strength Cond. Res. 2013, 27, 2323–2337. [Google Scholar] [CrossRef]
- Nimphius, S.; Callaghan, S.J.; Sptieri, T.; Lockie, R.G. Change of direction deficit: A more isolated measure of change of direction performance than total 505 time. J. Strength Cond. Res. 2016, 30, 3024–3032. [Google Scholar] [CrossRef]
- Nimphius, S.; Geib, G.; Spiteri, T.; Carlisle, D. “Change of direction deficit” measurement in division i american football players. J. Aust. Strength Cond. 2013, 21, 115–117. [Google Scholar]
- Nimphius, S.; Callaghan, S.J.; Bezodis, N.E.; Lockie, R.G. Change of direction and agility tests: Challenging our current measures of performance. Strength Cond. J. 2017, 40, 26–38. [Google Scholar] [CrossRef]
- Onate, J.; Cortes, N.; Welch, C.; Van Lunen, B. Expert versus novice interrater reliability and criterion validity of the landing error scoring system. J. Sport Rehabil. 2010, 19, 41–56. [Google Scholar] [CrossRef]
- Fort-Vanmeerhaeghe, A.; Montalvo, A.M.; Lloyd, R.S.; Read, P.; Myer, G.D. Intra-and inter-rater reliability of the modified tuck jump assessment. J. Sport Sci. Med. 2017, 16, 117–124. [Google Scholar]
- DeWeese, B.H.; Nimphius, S. Program design technique for speed and agility training. In Essentials of Strength Training and Conditioning; Haff, G.G., Triplett, N.T., Eds.; Human Kinetics: Champaign, IL, USA, 2016; pp. 521–558. [Google Scholar]
- Haff, G.G.; Triplett, N.T. Essentials of Strength Training and Conditioning, 4th ed.; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Dos’Santos, T.; Thomas, C.; Comfort, P.; Jones, P. The role of the penultimate foot contact during change of direction: Implications on performance and risk of injury. Strength Cond. J. 2018. [Google Scholar] [CrossRef]
- Welling, W.; Benjaminse, A.; Gokeler, A.; Otten, B. Enhanced retention of drop vertical jump landing technique: A randomized controlled trial. Hum. Mov. Sci. 2016, 45, 84–95. [Google Scholar] [CrossRef]
- Porter, J.; Nolan, R.; Ostrowski, E.; Wulf, G. Directing attention externally enhances agility performance: A qualitative and quantitative analysis of the efficacy of using verbal instructions to focus attention. Front. Psychol. 2010, 1, 216. [Google Scholar] [CrossRef]
- Thomas, J.R.; Nelson, J.K.; Silverman, S.J. Research Methods in Physical Activity; Human Kinetics: Champaign, IL, USA, 2005. [Google Scholar]
- Kropmans, T.J.B.; Dijkstra, P.U.; Stegenga, B.; Stewart, R.; De Bont, L.G.M. Smallest detectable difference in outcome variables related to painful restriction of the temporomandibular joint. J. Dent. Res. 1999, 78, 784–789. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Baumgartner, T.A.; Chung, H. Confidence limits for intraclass reliability coefficients. Meas. Phys. Educ. Exerc. Sci. 2001, 5, 179–188. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Analysis for the Behavioral Sciences; Lawrance Erlbaum: Hillsdale, MI, USA, 1988. [Google Scholar]
- Hedges, L.; Olkin, I. Statistical Methods for Meta-Analysis; Acdemic Press: New York, NY, USA, 1985. [Google Scholar]
- Hopkins, W.G. A scale of magnitudes for effect statistics. New View Stat. 2002, 502, 411. Available online: http://sportsci.org/resource/stats/effectmag.html (accessed on 15 June 2019).
- Stroube, B.W.; Myer, G.D.; Brent, J.L.; Ford, K.R.; Heidt, R.S., Jr.; Hewett, T.E. Effects of task-specific augmented feedback on deficit modification during performance of the tuck-jump exercise. J. Sport Rehabil. 2013, 22, 7–18. [Google Scholar] [CrossRef]
- Withrow, T.J.; Huston, L.J.; Wojtys, E.M.; Ashton-Miller, J.A. The effect of an impulsive knee valgus moment on in vitro relative acl strain during a simulated jump landing. Clin. Biomech. 2006, 21, 977–983. [Google Scholar] [CrossRef]
- Waiteman, M.C.; Briani, R.V.; Pazzinatto, M.F.; Ferreira, A.S.; Ferrari, D.; de Oliveira Silva, D.; de Azevedo, F.M. Relationship between knee abduction moment with patellofemoral joint reaction force, stress and self-reported pain during stair descent in women with patellofemoral pain. Clin. Biomech. 2018, 59, 110–116. [Google Scholar] [CrossRef]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for noncontact anterior cruciate ligament injuries knee joint kinematics in 10 injury situations from female team handball and basketball. Am. J. Sport Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IG Pre-Intervention within-Session Reliability | ||||||||||
| Variable | ICC | LB | UB | CV% | LB | UB | SEM | SDD | SDD% | |
| Completion time | Right Cut (s) | 0.944 | 0.800 | 0.988 | 2.8 | 1.8 | 3.7 | 0.042 | 0.117 | 5.0 |
| Left Cut (s) | 0.865 | 0.537 | 0.971 | 2.8 | 1.4 | 4.2 | 0.054 | 0.150 | 6.4 | |
| CODD | Right CODD (s) | 0.889 | 0.622 | 0.976 | 15.1 | 8.3 | 21.9 | 0.043 | 0.120 | 25.9 |
| Left CODD (s) | 0.843 | 0.461 | 0.966 | 13.9 | 8.6 | 19.3 | 0.055 | 0.153 | 33.0 | |
| Sprint | 10-m sprint (s) | 0.861 | 0.561 | 0.969 | 2.1 | 0.9 | 3.4 | 0.034 | 0.093 | 5.0 |
| CMAS | CMAS Right | 0.934 | 0.776 | 0.986 | 11.4 | 5.2 | 17.6 | 0.49 | 1.36 | 21.7 |
| CMAS Left | 0.865 | 0.526 | 0.971 | 15.7 | 9.3 | 22.2 | 0.67 | 1.84 | 29.3 | |
| IG post-intervention within-session reliability | ||||||||||
| Completion time | Right Cut (s) | 0.934 | 0.786 | 0.985 | 2.0 | 1.6 | 2.4 | 0.026 | 0.071 | 3.5 |
| Left Cut (s) | 0.917 | 0.732 | 0.982 | 2.3 | 1.1 | 3.4 | 0.037 | 0.102 | 4.8 | |
| CODD | Right CODD (s) | 0.873 | 0.596 | 0.972 | 20.8 | 15.0 | 26.6 | 0.027 | 0.074 | 34.7 |
| Left CODD (s) | 0.870 | 0.580 | 0.972 | 17.0 | 10.5 | 23.4 | 0.038 | 0.106 | 38.4 | |
| Sprint | 10-m sprint (s) | 0.932 | 0.776 | 0.985 | 1.8 | 0.7 | 2.9 | 0.027 | 0.076 | 4.1 |
| CMAS | CMAS Right | 0.870 | 0.553 | 0.972 | 18.3 | 12.4 | 24.3 | 0.59 | 1.63 | 33.9 |
| CMAS Left | 0.817 | 0.373 | 0.961 | 22.2 | 16.0 | 28.3 | 0.63 | 1.74 | 42.6 | |
| CG pre-intervention within-session reliability | ||||||||||
| Completion time | Right Cut (s) | 0.878 | 0.671 | 0.964 | 3.0 | 2.1 | 3.9 | 0.051 | 0.141 | 5.9 |
| Left Cut (s) | 0.693 | 0.180 | 0.909 | 2.9 | 1.9 | 4.0 | 0.061 | 0.168 | 6.9 | |
| CODD | Right CODD (s) | 0.847 | 0.585 | 0.955 | 14.9 | 9.6 | 20.3 | 0.052 | 0.145 | 28.3 |
| Left CODD (s) | 0.661 | 0.096 | 0.899 | 13.2 | 8.7 | 17.7 | 0.062 | 0.172 | 31.5 | |
| Sprint | 10-m sprint (s) | 0.762 | 0.311 | 0.931 | 2.3 | 1.7 | 3.0 | 0.035 | 0.096 | 5.1 |
| CMAS | CMAS Right | 0.898 | 0.723 | 0.970 | 14.4 | 9.9 | 18.8 | 0.52 | 1.43 | 28.3 |
| CMAS Left | 0.877 | 0.668 | 0.964 | 18.5 | 9.8 | 27.3 | 0.56 | 1.55 | 33.9 | |
| CG post-intervention within-session reliability | ||||||||||
| Completion time | Right Cut (s) | 0.727 | 0.214 | 0.921 | 3.1 | 2.2 | 4.1 | 0.059 | 0.163 | 7.2 |
| Left Cut (s) | 0.903 | 0.738 | 0.972 | 2.0 | 1.3 | 2.7 | 0.033 | 0.092 | 4.0 | |
| CODD | Right CODD (s) | 0.721 | 0.197 | 0.920 | 18.8 | 14.1 | 23.6 | 0.059 | 0.163 | 44.7 |
| Left CODD (s) | 0.932 | 0.816 | 0.980 | 11.6 | 7.4 | 15.7 | 0.032 | 0.089 | 21.3 | |
| Sprint | 10-m sprint (s) | 0.830 | 0.546 | 0.950 | 2.4 | 1.4 | 3.3 | 0.036 | 0.099 | 5.3 |
| CMAS | CMAS Right | 0.854 | 0.609 | 0.957 | 19.2 | 14.1 | 24.2 | 0.63 | 1.76 | 33.9 |
| CMAS Left | 0.774 | 0.355 | 0.935 | 15.3 | 8.9 | 21.7 | 0.65 | 1.81 | 36.0 | |
| Variable/CMAS Tool Criteria | Intra-Rater Reliability | Inter-Rater Reliability | ||
|---|---|---|---|---|
| % Agreement | k | % Agreement | k | |
| Clear PFC braking | 92.3 | 0.755 | 94.7 | 0.894 |
| Wide lateral leg plant | 96.2 | 0.920 | 100.0 | 1.000 |
| Hip in an initial internally rotated position | 100.0 | 1.000 | 100.0 | 1.000 |
| Initial knee ‘valgus’ position | 96.2 | 0.866 | 89.5 | 0.789 |
| Inwardly rotated foot position | 96.2 | 0.922 | 100.0 | 1.000 |
| Frontal plane trunk position relative to intended direction | 96.2 | 0.935 | 94.7 | 0.906 |
| Trunk upright or leaning back throughout contact | 96.2 | 0.906 | 100.0 | 1.000 |
| Limited Knee Flexion during final contact | 96.2 | 0.923 | 94.7 | 0.872 |
| Excessive Knee ‘valgus’ motion during contact | 96.2 | 0.920 | 94.7 | 0.906 |
| Average | 96.2 | 0.905 | 96.5 | 0.930 |
| Variable | IG Pre | IG Post | Hedges’ g Effect Size | % Change | Mean Difference | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | g | LB | UB | Mean | SD | LB | UB | Mean | SD | LB | UB | |
| R Cut (s) | 2.344 | 0.172 | 2.065 | 0.095 | <0.001 | −1.90 | −3.08 | −0.72 | −11.7 | 4.3 | −16.2 | −7.7 | −0.279 | 0.115 | −0.375 | −0.182 |
| L Cut (s) | 2.342 | 0.130 | 2.128 | 0.119 | <0.001 | −1.63 | −2.76 | −0.50 | −9.1 | 3.8 | −12.5 | −5.8 | −0.215 | 0.097 | −0.296 | −0.133 |
| R CODD (s) | 0.466 | 0.121 | 0.214 | 0.068 | 0.001 | −2.43 | −3.72 | −1.14 | −51.5 | 17.4 | −72.8 | −35.3 | −0.252 | 0.129 | −0.360 | −0.144 |
| L CODD (s) | 0.464 | 0.121 | 0.277 | 0.095 | 0.012 | −1.63 | −2.76 | −0.50 | −39.1 | 21.2 | −54.3 | −26.3 | −0.187 | 0.123 | −0.290 | −0.084 |
| 10-m sprint (s) | 1.878 | 0.081 | 1.850 | 0.098 | 0.328 | −0.29 | −1.27 | 0.70 | −1.4 | 3.9 | −2.6 | −0.4 | −0.027 | 0.075 | −0.034 | 0.090 |
| R CMAS | 6.3 | 1.8 | 4.8 | 1.4 | 0.025 | −0.85 | −1.88 | 0.17 | −22.5 | 15.7 | −31.5 | −15.2 | −1.5 | 1.1 | −2.6 | −0.4 |
| L CMAS | 6.3 | 1.6 | 4.1 | 1.2 | 0.018 | −1.46 | −2.57 | −0.36 | −33.9 | 20.3 | −47.3 | −22.9 | −2.2 | 1.5 | −3.5 | −1.0 |
| Variable | CG Pre | CG Post | Hedges’ g Effect Size | % Change | Mean Difference | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | g | LB | UB | Mean | SD | LB | UB | Mean | SD | LB | UB | |
| R Cut (s) | 2.395 | 0.131 | 2.251 | 0.089 | <0.001 | −1.21 | −2.28 | −0.15 | −5.9 | 3.5 | −8.3 | −3.7 | −0.144 | 0.089 | −0.203 | −0.084 |
| L Cut (s) | 2.429 | 0.087 | 2.306 | 0.097 | 0.002 | −1.27 | −2.34 | −0.19 | −5.0 | 3.9 | −7.1 | −3.1 | −0.123 | 0.099 | −0.190 | −0.057 |
| R CODD (s) | 0.510 | 0.117 | 0.365 | 0.088 | <0.001 | −1.32 | −2.41 | −0.24 | −27.9 | 10.5 | −38.3 | −18.5 | −0.145 | 0.057 | −0.183 | −0.106 |
| L CODD (s) | 0.545 | 0.082 | 0.420 | 0.116 | 0.013 | −1.17 | −2.23 | −0.11 | −21.7 | 21.4 | −30.8 | −14.9 | −0.124 | 0.136 | −0.216 | −0.032 |
| 10-m sprint (s) | 1.885 | 0.058 | 1.885 | 0.075 | 0.957 | 0.01 | −0.97 | 0.99 | 0.1 | 3.3 | −0.9 | 1.0 | 0.001 | 0.061 | −0.041 | −0.040 |
| R CMAS | 5.1 | 1.5 | 5.2 | 1.5 | 0.779 | 0.08 | −0.90 | 1.06 | 5.6 | 28.2 | −11.1 | 22.3 | 0.1 | 1.4 | −0.9 | 1.1 |
| L CMAS | 4.6 | 1.4 | 5.0 | 1.1 | 0.306 | 0.33 | −0.65 | 1.32 | 18.5 | 39.8 | −5.0 | 42.0 | 0.5 | 1.3 | −0.5 | 1.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dos’Santos, T.; McBurnie, A.; Comfort, P.; Jones, P.A. The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players. Sports 2019, 7, 205. https://doi.org/10.3390/sports7090205
Dos’Santos T, McBurnie A, Comfort P, Jones PA. The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players. Sports. 2019; 7(9):205. https://doi.org/10.3390/sports7090205
Chicago/Turabian StyleDos’Santos, Thomas, Alistair McBurnie, Paul Comfort, and Paul A. Jones. 2019. "The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players" Sports 7, no. 9: 205. https://doi.org/10.3390/sports7090205
APA StyleDos’Santos, T., McBurnie, A., Comfort, P., & Jones, P. A. (2019). The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players. Sports, 7(9), 205. https://doi.org/10.3390/sports7090205