Epidemiology of Injuries in Ultimate (Frisbee): A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Assessment of Study Quality
2.6. Data Extraction and Synthesis
3. Results
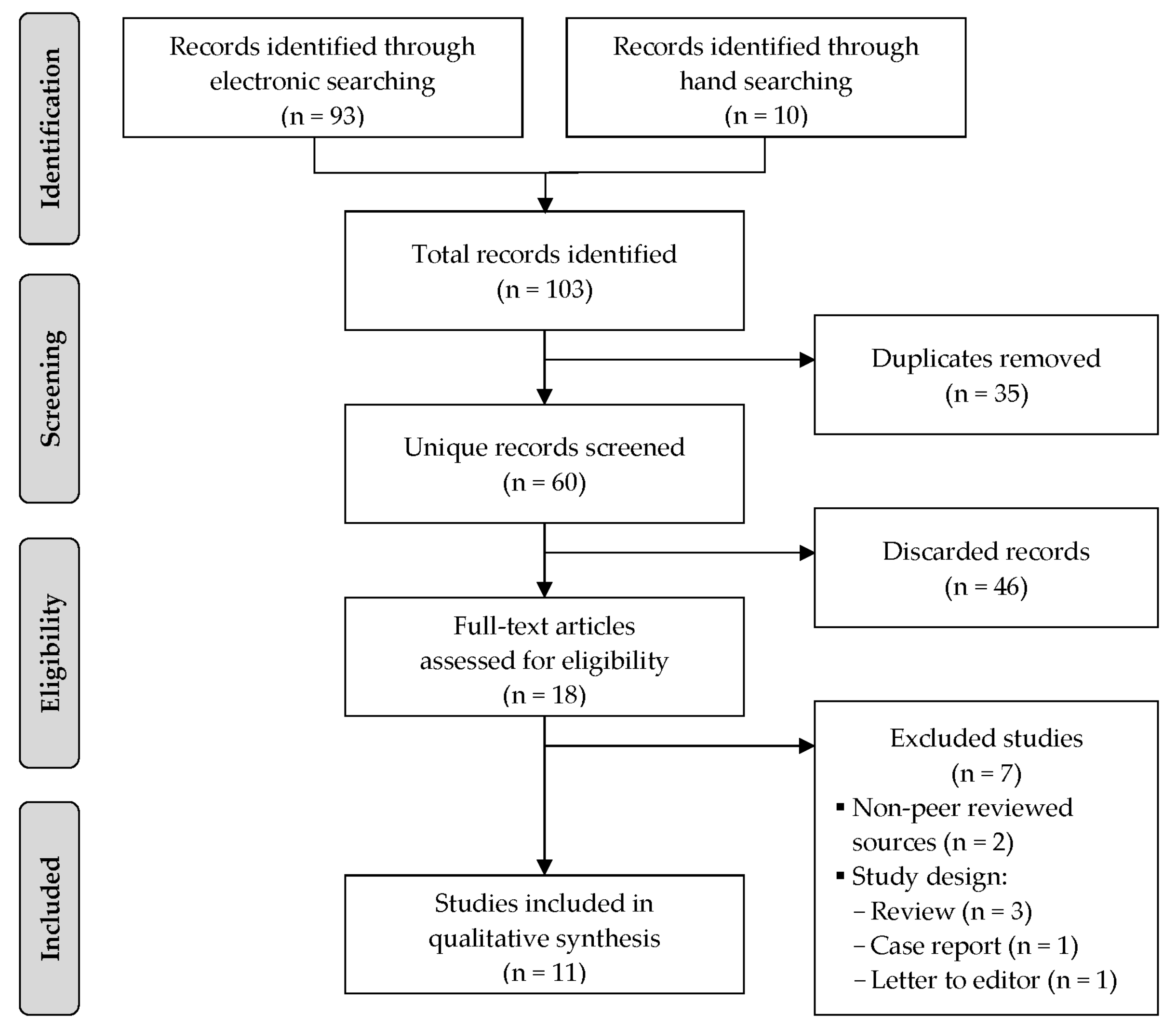
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Injury Incidence and Prevalence
3.4. Injury Pattern
3.5. Risk Factors for Injury
4. Discussion
4.1. Injury Incidence and Prevalence
4.2. Injury Pattern
4.3. Risk Factors
4.4. Strengths and Limitations
4.5. Recommendations for Future Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Flying Disc Federation. Disciplines. WFDF: Colorado Springs, CO, USA. 2020. Available online: http://www.wfdf.org/disciplines/ (accessed on 2 November 2020).
- World Flying Disc Federation. Rules of Ultimate. WFDF: Colorado Springs, CO, USA. 2020. Available online: http://rules.wfdf.org/ (accessed on 2 November 2020).
- Marfleet, P. Ultimate injuries: A survey. Br. J. Sports Med. 1991, 25, 235. [Google Scholar] [CrossRef] [Green Version]
- World Flying Disc Federation. 2018 Annual Census; World Flying Disc Federation: Colorado Springs, CO, USA, 2018. [Google Scholar]
- USA Ultimate. USA Ultimate 2016 Annual Report; USA Ultimate: Colorado Springs, CO, USA, 2016. [Google Scholar]
- Krustrup, P.; Mohr, M. Physical Demands in Competitive Ultimate Frisbee. J. Strength Cond. Res. 2015, 29, 3386–3391. [Google Scholar] [CrossRef]
- Kee, C.K.; Agrawal, S.; Hallinan, J.T.P.D.; Singbal, S.B. Luxatio erecta in a Frisbee player: Magnetic resonance imaging findings of a rare injury. Am. J. Phys. Med. Rehabil. 2020, 99, e28–e29. [Google Scholar] [CrossRef] [PubMed]
- Suero, E.M.; Omar, M.; Citak, M.; Daluiski, A.; Pearle, A.D. Proximal hamstring avulsion injury in an ultimate frisbee player: Case report and literature review. J. Orthop. Trauma Rehabil. 2018, 25, 34–36. [Google Scholar] [CrossRef] [Green Version]
- Fong, D.T.; Hong, Y.; Chan, L.-K.; Yung, P.S.-H.; Chan, K.-M. A Systematic Review on Ankle Injury and Ankle Sprain in Sports. Sports Med. 2007, 37, 73–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mechelen, W.V.; Hlobil, H.; Kemper, H.C. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med. 1992, 14, 82–99. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Krosshaug, T. Understanding injury mechanisms: A key component of preventing injuries in sport. Br. J. Sports Med. 2005, 39, 324–329. [Google Scholar] [CrossRef]
- Meeuwisse, W.H.; Tyreman, H.; Hagel, B.; Emery, C. A dynamic model of etiology in sport injury: The recursive nature of risk and causation. Clin. J. Sport Med. 2007, 17, 215–219. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Elm, E.V.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P.T. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falck, R.S.; Davis, J.C.; Liu-Ambrose, T. What is the association between sedentary behaviour and cognitive function? A systematic review. Br. J. Sports Med. 2017, 51, 800–811. [Google Scholar] [CrossRef] [Green Version]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 711–718. [Google Scholar]
- Rothman, K.; Greenland, S.; Lash, T. Modern Epidemiology, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sore for every spot (frisbee elbow). Prevention 1980, 32, 82–83.
- Fox, C.; Florczyk, D.; Wu, J. Injury patterns in club collegiate ultimate frisbee. Clin. J. Sport Med. 2018, 28, 190. [Google Scholar]
- Harper, S. Ultimate frisbee. Sports Physio 2007, 1, 16–18. [Google Scholar]
- Melchionda, A.M.; Linburg, R.M. Volar Plate Injuries. Phys. Sportsmed. 1982, 10, 77–84. [Google Scholar] [CrossRef]
- Mueller, L.P.; Rudig, L.; Kreitner, K.F.; Degreif, J. Hypothenar hammer syndrome in sports. Knee Surg Sports Traumatol. Arthrosc. 1996, 4, 167–170. [Google Scholar] [CrossRef]
- Akinbola, M.; Logerstedt, D.; Hunter-Giordano, A.; Snyder-Mackler, L. Ultimate frisbee injuries in a collegiate setting. Int. J. Sports Phys. Ther. 2015, 10, 75–84. [Google Scholar]
- Kołodziej, G.; Jandziś, S.; Kołodziej, K.; Skubal, A.; Cyran-Grzebyk, B. Most frequent in juries and their causes in Ultimate Frisbee players. Eur. J. Clin. Exp. Med. 2018, 15, 315–321. [Google Scholar] [CrossRef]
- Lazar, D.J.; Lichtenstein, J.D.; Tybor, D.J. Concussion Prevalence in Competitive Ultimate Frisbee Players. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McElveen, M.; North, T., Jr.; Rossow, A.; Cattell, M. Injury Rates in Intramural Sports. Recreat. Sports J. 2014, 38, 98–103. [Google Scholar] [CrossRef]
- Reynolds, K.H.; Halsmer, S.E. Injuries from ultimate frisbee. WMJ 2006, 105, 46–49. [Google Scholar] [PubMed]
- Swedler, D.I.; Nuwer, J.M.; Nazarov, A.; Huo, S.C.; Malevanchik, L. Incidence and descriptive epidemiology of injuries to college ultimate players. J. Athl. Train. 2015, 50, 419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, L.E.; Gregory, A.; Kuhn, J.E.; Markle, R. The ultimate frisbee injury study: The 2007 Ultimate Players Association College Championships. Clin. J. Sport Med. 2010, 20, 300–305. [Google Scholar] [CrossRef]
- Hess, M.C.; Swedler, D.I.; Collins, C.S.; Ponce, B.A.; Brabston, E.W. Descriptive Epidemiology of Injuries in Professional Ultimate Frisbee Athletes. J. Athl. Train. 2020, 55, 195–204. [Google Scholar] [CrossRef]
- Brezinski, T.; Martin, J.; Ambegaonkar, J.P. Prospective Injury Epidemiology in Competitive Collegiate Club Sports, Quidditch, and Ultimate Frisbee. Athl. Train. Sports Health Care 2020. [Google Scholar] [CrossRef]
- Kerr, Z.; Caswell, S.; Lincoln, A.; Djoko, A.; Dompier, T. The epidemiology of boys’ youth lacrosse injuries in the 2015 season. Inj. Epidemiol. 2016, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Hootman, J.M.; Dick, R.W.; Agel, J. Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J. Athl. Train. 2007, 42, 311–319. [Google Scholar]
- Panagodage Perera, N.K.; Joseph, C.; Kemp, J.L.; Finch, C.F. Epidemiology of Injuries in Women Playing Competitive Team Bat-or-Stick Sports: A Systematic Review and a Meta-Analysis. Sports Med. 2018, 48, 617–640. [Google Scholar] [CrossRef] [PubMed]
- Lynall, R.C.; Gardner, E.C.; Paolucci, J.; Currie, D.W.; Knowles, S.B.; Pierpoint, L.A.; Wasserman, E.B.; Dompier, T.P.; Comstock, R.D.; Marshall, S.W.; et al. The First Decade of Web-Based Sports Injury Surveillance: Descriptive Epidemiology of Injuries in US High School Girls’ Field Hockey (2008–2009 Through 2013–2014) and National Collegiate Athletic Association Women’s Field Hockey (2004–2005 Through 2013–2014). J. Athl. Train. 2018, 53, 938–949. [Google Scholar] [PubMed] [Green Version]
- Marquardt, R.J.; Buletko, A.B.; Russman, A.N. Neurologic Injuries in Noncontact Sports. Neurol. Clin. 2017, 35, 573–587. [Google Scholar] [CrossRef] [PubMed]
- Hinton, R.Y.; Lincoln, A.E.; Almquist, J.L.; Douoguih, W.A.; Sharma, K.M. Epidemiology of Lacrosse Injuries in High School-Aged Girls and Boys: A 3-Year Prospective Study. Am. J. Sports Med. 2005, 33, 1305–1314. [Google Scholar] [CrossRef]
- Gessel, L.M.; Fields, S.K.; Collins, C.L.; Dick, R.W.; Comstock, R.D. Concussions among United States high school and collegiate athletes. J. Athl. Train. 2007, 42, 495–503. [Google Scholar]
- Veliz, P.; McCabe, S.E.; Eckner, J.T.; Schulenberg, J.E. Prevalence of Concussion Among US Adolescents and Correlated Factors. JAMA 2017, 318, 1180–1182. [Google Scholar] [CrossRef]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar]
- Haarbauer-Krupa, J.; Arbogast, K.B.; Metzger, K.B.; Greenspan, A.I.; Kessler, R.; Curry, A.E.; Bell, J.M.; DePadilla, L.; Pfeiffer, M.R.; Zonfrillo, M.R.; et al. Variations in Mechanisms of Injury for Children with Concussion. J. Pediatr. 2018, 197, 241–248.e1. [Google Scholar] [CrossRef]
- Zuckerman, S.L.; Kerr, Z.Y.; Yengo-Kahn, A.; Wasserman, E.; Covassin, T.; Solomon, G.S. Epidemiology of Sports-Related Concussion in NCAA Athletes From 2009–2010 to 2013–2014: Incidence, Recurrence, and Mechanisms. Am. J. Sports Med. 2015, 43, 2654–2662. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football (Soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Noya Salces, J.; Gómez-Carmona, P.M.; Gracia-Marco, L.; Moliner-Urdiales, D.; Sillero-Quintana, M. Epidemiology of injuries in First Division Spanish football. J. Sports Sci. 2014, 32, 1263–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Copeland, S. Throwing injuries of the shoulder. Br. J. Sports Med. 1993, 27, 221–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanley, E.; Rauh, M.J.; Michener, L.A.; Ellenbecker, T.S.; Garrison, J.C.; Thigpen, C.A. Shoulder range of motion measures as risk factors for shoulder and elbow injuries in high school softball and baseball players. Am. J. Sports Med. 2011, 39, 1997–2006. [Google Scholar] [CrossRef] [PubMed]
- Raya-González, J.; Clemente, F.M.; Beato, M.; Castillo, D. Injury Profile of Male and Female Senior and Youth Handball Players: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3925. [Google Scholar] [CrossRef] [PubMed]
- Andersson, S.H.; Bahr, R.; Clarsen, B.; Myklebust, G. Preventing overuse shoulder injuries among throwing athletes: A cluster-randomised controlled trial in 660 elite handball players. Br. J. Sports Med. 2017, 51, 1073–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber Foss, K.D.; Le Cara, E.; McCambridge, T.; Hinton, R.; Kushner, A.; Myer, G.D. Epidemiology of injuries in men’s lacrosse: Injury prevention implications for competition level, type of play, and player position. Phys. Sportsmed. 2017, 45, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.T.; Jones, R.E.; Runstrom, M.; Hardy, J. Disc Golf, a Growing Sport: Description and Epidemiology of Injuries. Orthop. J. Sports Med. 2015, 3, 2325967115589076. [Google Scholar] [CrossRef] [Green Version]
- Louw, Q.A.; Manilall, J.; Grimmer, K.A. Epidemiology of knee injuries among adolescents: As ystematic review. Br. J. Sports Med. 2008, 42, 2–10. [Google Scholar] [CrossRef]
- Sadigursky, D.; Braid, J.A.; DeLira, D.N.L.; Machado, B.A.B.; Carneiro, R.J.F.; Colavolpe, P.O. The FIFA 11+ injury prevention program for soccer players: A systematic review. BMC Sports Sci. Med. Rehabil. 2017, 9, 18. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Finch, F.C.; Wajswelner, L.H.; Bennell, L.K. Predictors of Lower Extremity Injuries at the Community Level of Australian Football. Clin. J. Sport Med. 2004, 14, 56–63. [Google Scholar] [CrossRef]
- Andreoli, C.V.; Chiaramonti, B.C.; Biruel, E.; Pochini, A.C.; Ejnisman, B.; Cohen, M. Epidemiology of sports injuries in basketball: Integrative systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000468. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | Setting | Study Design | Study Period | Sample Size | Participants | Injury Definition | Number of Injuries | Outcome Measure | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Marfleet 1991 [3] | United Kingdom, Germany, Belgium, Denmark, Norway | World championships (Competition) | Prospective cohort | 1986 to 1990 (5 years) | N = 1000 | Sex: Men’s and women’s (proportions NR) Age: Master’s, open’s, and junior (proportions NR) Experience: NR | NR | n = 485 | NR | Moderate |
| Reynolds and Halsmer 2006 [29] | United States | Regional tournament (Competition) | Cross-sectional | 2002 | N = 135 | Sex: 41% females, 59% males Age: 18–46 years Experience: 7.5 years | NR | NR | Lifetime prevalence: 100% | Good |
| Yen et al. 2010 [31] | United States | College championship (Competition) | Prospective cohort | 2007 (3 days) | N = 705 | Sex: 50% women’s teams, 50% men’s teams Age: NR Experience: NR | Injury time-out: any injury that required a player to miss part of the game or practice. | n = 107 | Injury incidence rate: 68.0 per 1000 AEs (females), 110.0 per 1000 AEs (males) | Good |
| McElveen et al. 2014 [28] | United States | College league (Competition) | Prospective cohort | 2011 to 2013 (2 years) | N = 553 | Sex: NR Age: NR Experience: NR | Medical attention injury: any injury that occurred during participation in an intramural game and resulted in care by the intramural staff or more advanced care. | n = 6 | Injury incidence proportion: 1.0 per 100 athletes (competition) | Poor |
| Akinbola et al. 2015 [25] | United States | University club sports (Competition and training) | Prospective cohort | 2000 to 2012 (12 years) | N = 97 | Sex: NR Age: NR Experience: NR | Medical attention injury: any injury for which an athlete sought medical attention at the Sports Clinic. | n = 143 | 12-year period prevalence: 100% | Moderate |
| Swedler et al. 2015 [30] | United States | College series (Competition and training) | Prospective cohort | 2012 (4 months) | NR | Sex: 50% women’s teams, 50% men’s teams Age: NR Experience: NR | Injury time-out: any injury that required a player to miss part of the game or practice. | n = 1317 | Injury incidence rate: 14.5 per 1000 AEs (competition), 10.1 per 1000 AEs (training) | Good |
| Kolodziej et al. 2017 [26] | Poland | Local club sports (Competition and training) | Cross-sectional | 2016 | N = 110 | Sex: 33% females, 67% males Age: NR Experience: <1 year | NR | n = 408 | Lifetime prevalence: 100% | Good |
| Lazar et al. 2018 [27] | United States | National teams and leagues (Competition and training) | Cross-sectional | 2012 | N = 787 | Sex: 30% females, 70% males Age: NR Experience: 8.8 years | Concussion | n = 338 | Lifetime prevalence: 26% | Good |
| Arthur-Banning et al. 2018 [34] | United States | University club sports (Competition and training) | Retrospective cohort | NR (2 years) | NR | Sex: NR Age: NR Experience: NR | Time-loss injury: incident that required medical attention and resulted in restriction to participation for at least one day. | NR | Injury incidence rate: 1.3 per 1000 AEs (competition, males), 0.4 per 1000 AEs (training, males), 9.2 per 1000 AEs (competition, females) | Moderate |
| Hess et al. 2020 [32] | United States, Canada | National league (Competition and training) | Prospective cohort | 2017 | NR | Sex: 100% men’s teams Age: NR Experience: NR | Injury time-out: any physical harm that happened while the player was participating in competition or practice and caused the player to miss part of a competition or practice. | n = 299 | Injury incidence rate: 45.1 per 1000 AEs (competition), 20.0 per 1000 AEs (training) | Good |
| Brezinski et al. 2020 [33] | United States | University club sports (Competition) | Prospective cohort | 2018 (16 weeks) | N = 69 | Sex: 30% females, 70% males Age: NR Experience: NR | Time-loss injury: incident that required medical attention and resulted in restriction to participation for at least one day. | n = 18 | Injury incidence rate: 11.1 per 1000 AEs (females), 9.6 per 1000 AEs (males) | Good |
| Body Region/ Anatomical Area | Marfleet 1991 [3] | Yen et al. 2010 [31] | Akinbola et al. 2015 [25] | Swedler et al. 2015 [30] b | Kolodziej et al. 2017 [26] | Hess et al. 2020 [32] c | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Head and Neck | 32 | 6.7 | 15 | 15.0 | - | - | 139 | 10.9 | 63 | 15.4 | 10 | 3.5 |
| Head | 7 | 1.5 | - | - | - | - | 89 | 7.0 | 14 | 3.4 | - | - |
| Neck | 10 | 2.1 | - | - | - | - | 7 | 0.5 | - | - | - | - |
| Other | 15 | 3.1 | - | - | - | - | 43 | 3.4 | 49 | 12.0 | - | - |
| Upper Limb | 88 | 18.3 | 11 | 11.0 | 6 | 4.2 | 186 | 14.6 | 17 | 4.2 | 45 | 16.0 |
| Shoulder | 22 | 4.6 | - | - | 3 | 2.1 | 83 | 6.5 | 3 | 0.7 | 17 | 6.0 |
| Upper arm | 1 | 0.2 | - | - | - | - | - | - | - | - | - | - |
| Elbow | 23 | 4.8 | - | - | - | - | 17 | 1.3 | 5 | 1.2 | 11 | 3.9 |
| Forearm | 6 | 1.3 | - | - | - | - | - | - | - | - | - | - |
| Wrist and hand | 36 | 7.5 | - | - | 3 | 2.1 | 86 | 6.8 | 9 | 2.2 | 17 | 6.0 |
| Trunk | 37 | 7.7 | 12 | 12.0 | 11 | 7.7 | 68 | 5.3 | 108 | 53.4 | 16 | 5.7 |
| Chest | 9 | 1.9 | - | - | - | - | - | - | - | - | - | - |
| Thoracic spine | 28 | 5.8 | - | - | - | - | 68 | 5.3 | 64 | 15.7 | - | - |
| Lumbar spine | - | - | - | - | 11 | 7.7 | - | - | 44 | 10.8 | - | - |
| Abdomen | 4 | 0.8 | - | - | - | - | - | - | 110 | 27.0 | - | - |
| Lower Limb | 323 | 67.3 | 62 | 62.0 | 126 | 88.1 | 881 | 69.2 | 110 | 27.0 | 210 | 74.5 |
| Hip and groin | 10 | 2.1 | - | - | 10 | 7.0 | 85 | 6.7 | 6 | 1.5 | 13 | 4.6 |
| Thigh | 103 | 21.5 | - | - | 15 | 10.5 | 152 | 11.9 | - | - | 50 | 17.7 |
| Knee | 73 | 15.2 | - | - | 50 | 35.0 | 209 | 16.4 | 37 | 9.1 | 41 | 14.5 |
| Lower leg | 48 | 10.0 | - | - | 21 | 14.7 | 93 | 7.3 | 49 | 12.0 | 35 | 12.4 |
| Ankle | 59 | 12.3 | - | - | 30 | 21.0 | 265 | 20.8 | 17 | 4.2 | 58 | 20.6 |
| Foot | 30 | 6.3 | - | - | - | - | 77 | 6.0 | 1 | 0.2 | 13 | 4.6 |
| Type of Tissue/Pathology | Marfleet. 1991 [3] b | Swedler et al. 2015 [30] c | Kolodziej et al. 2017 [26] d | Hess et al. 2020 [32] e | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Muscle/Tendon | 202 | 45.8 | 342 | 39.2 | 30 | 29.7 | 97 | 42.5 |
| Muscle injury | 179 | 40.6 | 319 | 36.5 | 30 | 29.7 | 86 | 37.7 |
| Tendon rupture | 23 | 5.2 | 23 | 2.6 | - | - | 11 | 4.8 |
| Nervous | 7 | 1.6 | 47 | 5.4 | - | - | 2 | 0.9 |
| Brain/Spinal cord injury | 6 | 1.4 | 47 | 5.4 | - | - | 2 | 0.9 |
| Peripheral nerve injury | 1 | 0.2 | - | - | - | - | - | - |
| Bone | 5 | 1.1 | 41 | 4.7 | - | - | 6 | 2.6 |
| Fracture | 5 | 1.1 | 41 | 4.7 | - | - | 6 | 2.6 |
| Cartilage/Synovium/Bursa | 23 | 5.2 | 7 | 0.8 | - | - | 4 | 1.8 |
| Synovitis/Capsulitis | 23 | 5.2 | - | - | - | - | 4 | 1.8 |
| Ligament/Joint Capsule | 38 | 8.6 | 246 | 28.2 | 71 | 70.3 | 62 | 27.2 |
| Joint sprain | 38 | 8.6 | 246 | 28.2 | 71 | 70.3 | 62 | 27.2 |
| Superficial Tissues/Skin | 166 | 37.6 | 190 | 21.8 | - | - | 57 | 25.0 |
| Contusion (superficial) | 110 | 24.9 | 140 | 16.0 | - | - | 46 | 20.2 |
| Laceration | 56 | 12.7 | 50 | 5.7 | - | - | 11 | 4.8 |
| Injury Mechanism | Yen et al. 2010 [31] | Swedler et al. 2015 [30] b | Hess et al. 2020 [32] c | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Non-Contact | 44 | 40.4 | 871 | 68.6 | 191 | 65.0 |
| Direct Contact | 65 | 59.6 | 399 | 31.4 | 103 | 35.0 |
| With another athlete | 43 | 39.4 | 387 | 30.5 | 101 | 34.4 |
| With an object | 22 | 20.2 | 12 | 0.9 | 2 | 0.7 |
| Mode of Onset | Swedler et al. 2015 [30] c | Hess et al. 2020 [32] | ||
|---|---|---|---|---|
| n | % | n | % | |
| Acute | 1027 | 79.7 | 275 | 92.0 |
| Sudden onset | 1027 | 79.7 | 275 | 92.0 |
| Repetitive | 262 | 20.3 | 24 | 8.0 |
| Sudden onset | - | - | - | - |
| Gradual onset | 262 | 20.3 | 24 | 8.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fajardo Pulido, D.; Lystad, R.P. Epidemiology of Injuries in Ultimate (Frisbee): A Systematic Review. Sports 2020, 8, 168. https://doi.org/10.3390/sports8120168
Fajardo Pulido D, Lystad RP. Epidemiology of Injuries in Ultimate (Frisbee): A Systematic Review. Sports. 2020; 8(12):168. https://doi.org/10.3390/sports8120168
Chicago/Turabian StyleFajardo Pulido, Diana, and Reidar P. Lystad. 2020. "Epidemiology of Injuries in Ultimate (Frisbee): A Systematic Review" Sports 8, no. 12: 168. https://doi.org/10.3390/sports8120168
APA StyleFajardo Pulido, D., & Lystad, R. P. (2020). Epidemiology of Injuries in Ultimate (Frisbee): A Systematic Review. Sports, 8(12), 168. https://doi.org/10.3390/sports8120168