“Paralympic Brain”. Compensation and Reorganization of a Damaged Human Brain with Intensive Physical Training


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant
2.2. Experiments
2.2.1. Experiment 1
- 1.
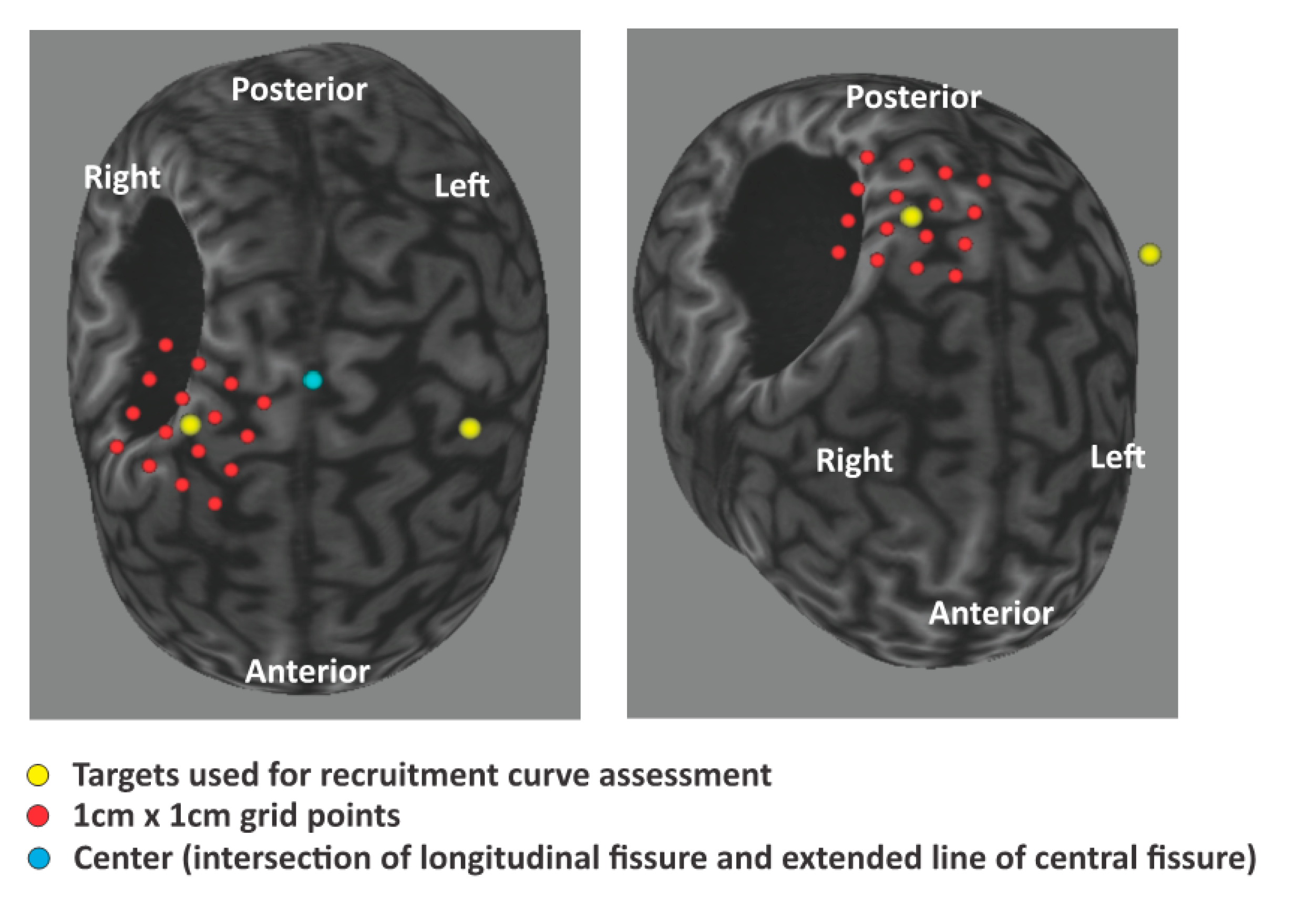
- Transcranial magnetic stimulation
- 2.
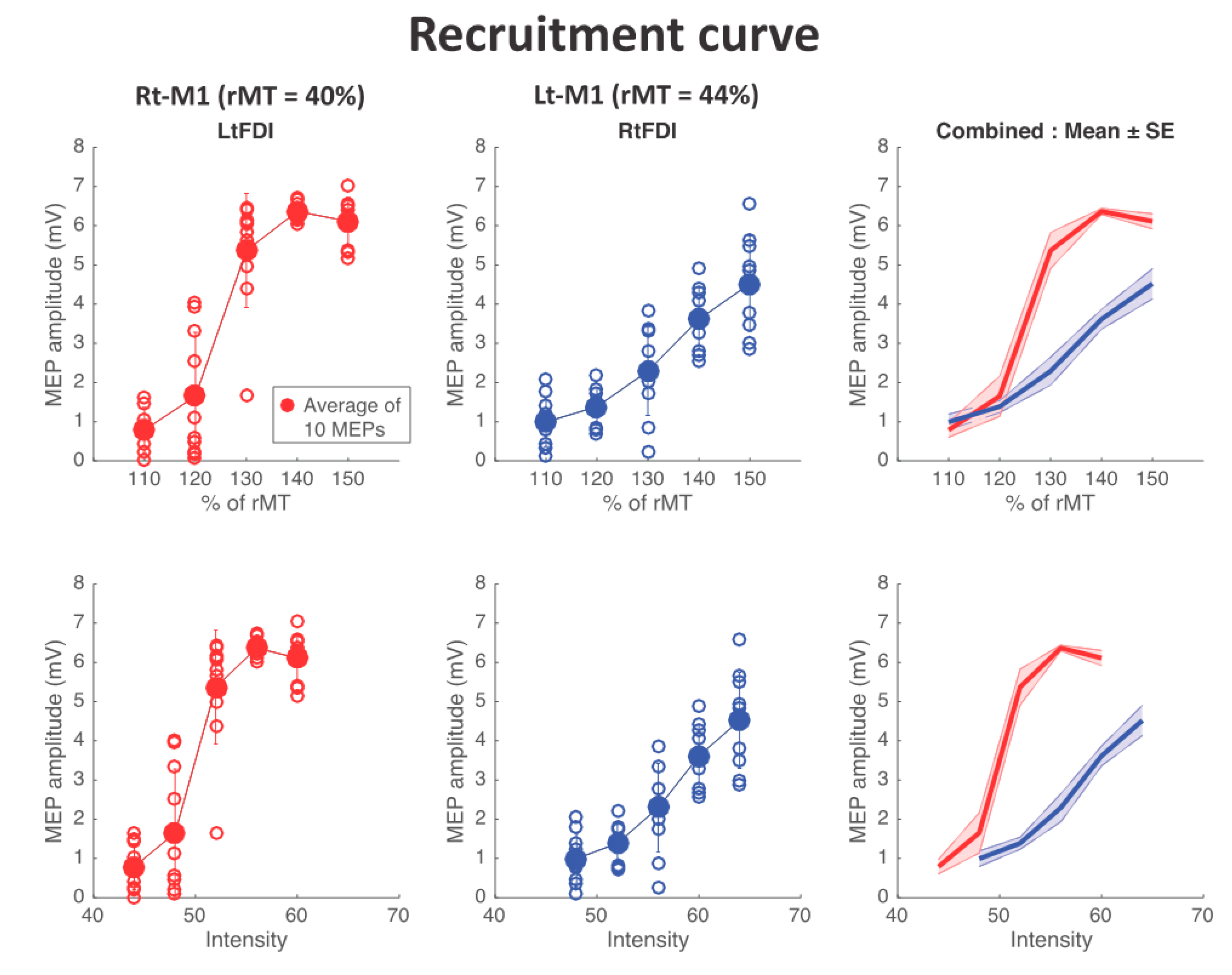
- MEP recruitment curve (stimulus response curve)
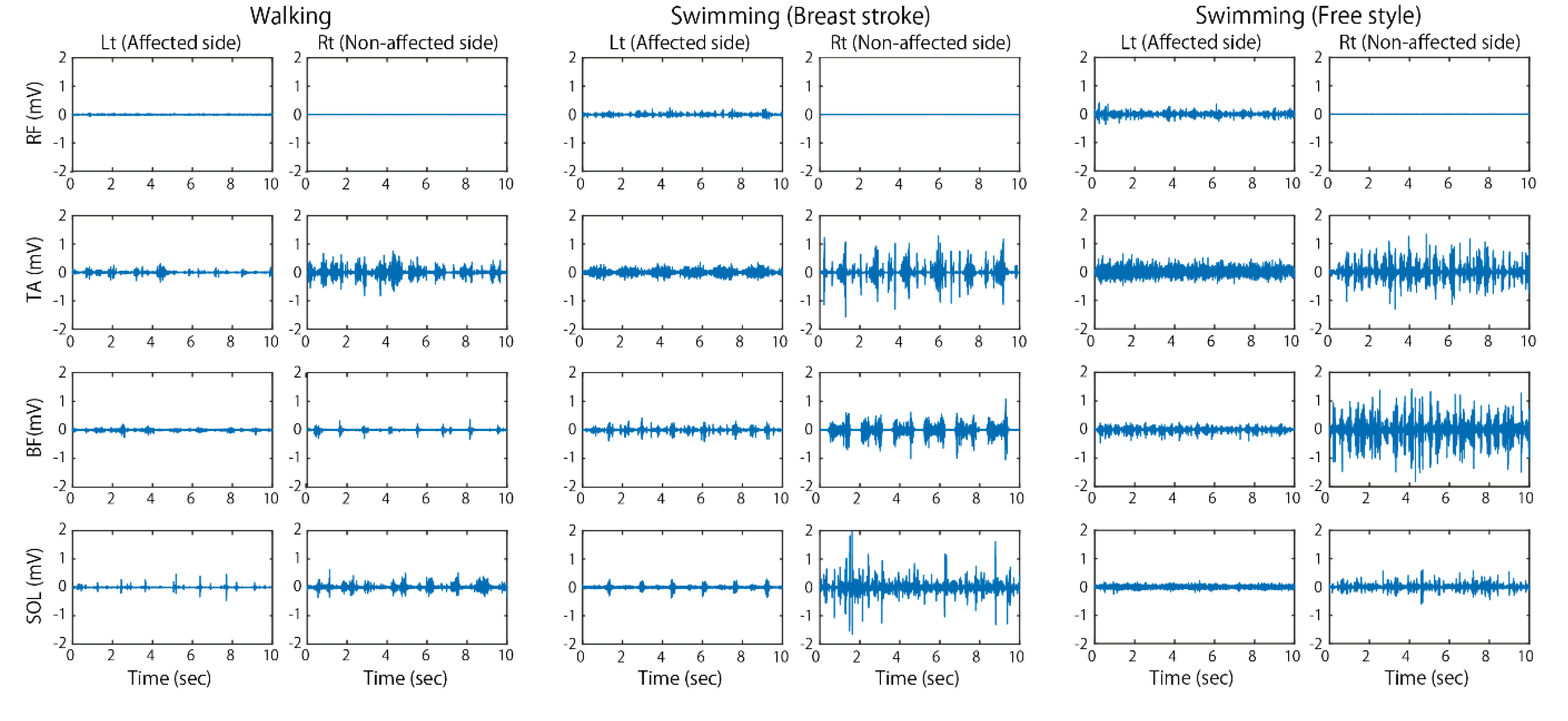
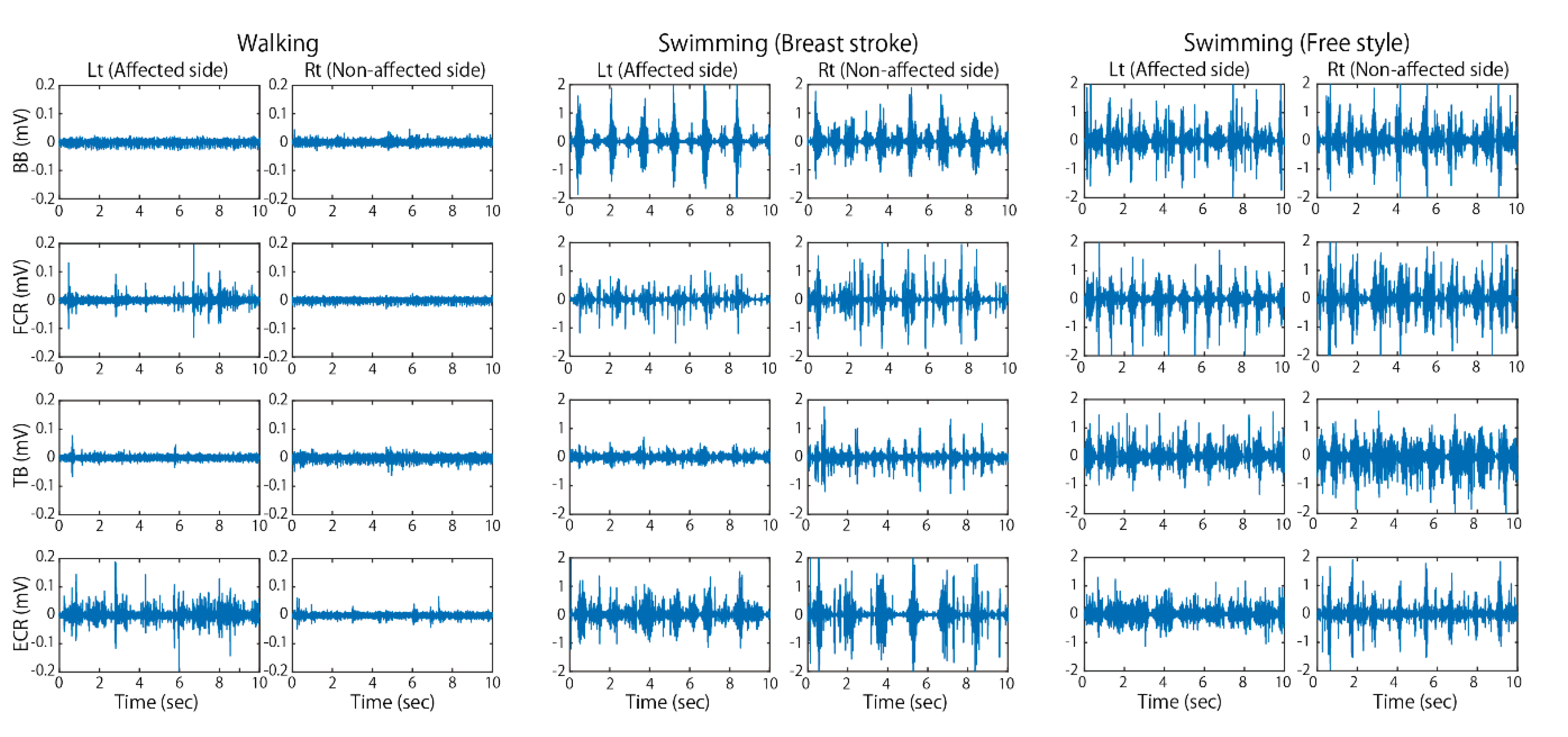
2.2.2. Experiment 2: Recording of Electromyographic (EMG) Activities during Swimming
- 3.
- Statistics
3. Results
3.1. TMS and MEP Recruitment Curves
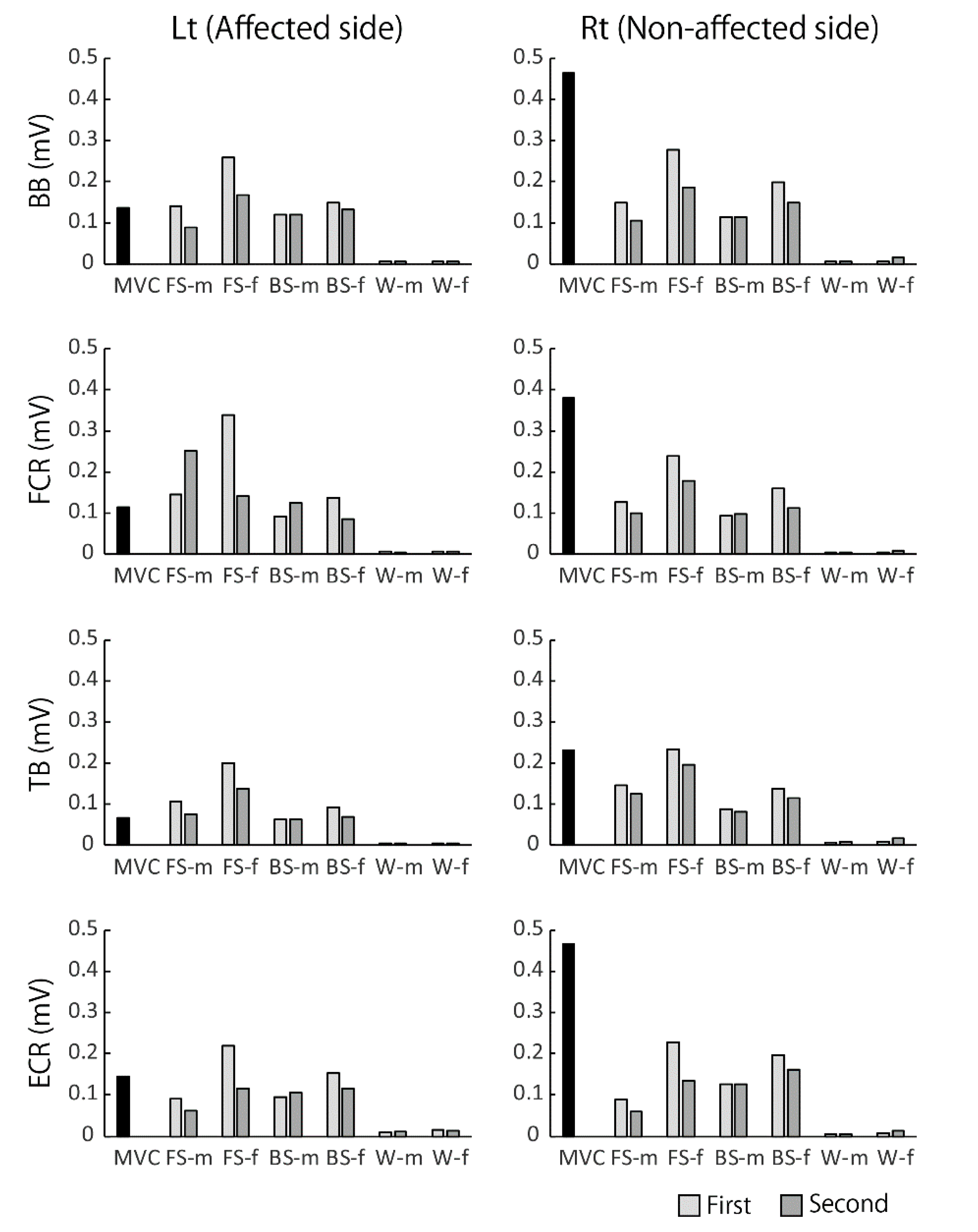
3.2. EMG Activities during Walking and Swimming
4. Discussion
4.1. Reorganization of Motor Cortical Area
4.2. The Well-Coordinated Muscular Activities in Water
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nudo, R.J.; Plautz, E.J.; Frost, S.B. Role of adaptive plasticity in recovery of function after damage to motor cortex. Muscle Nerve 2001, 24, 1000–1019. [Google Scholar] [CrossRef] [PubMed]
- Raineteau, O.; Schwab, M.E. Plasticity of motor systems after incomplete spinal cord injury. Nat. Rev. Neurosci. 2001, 2, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.B.; Cohen, L.G. The olympic brain. Does corticospinal plasticity play a role in acquisition of skills required for high-performance sports? J. Physiol. 2008, 586, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Lu, M.; Song, Z.; Wang, J. Long-term intensive training induced brain structural changes in world class gymnasts. Brain Struct. Funct. 2015, 220, 625–644. [Google Scholar] [CrossRef]
- Pearce, A.J.; Thickbroom, G.W.; Byrnes, M.L.; Mastaglia, F.L. Functional reorganisation of the corticomotor projection to the hand in skilled racquet players. Exp. Brain Res. 2000, 130, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Maclean, N.; Pound, P.; Wolfe, C.; Rudd, A. Qualitative analysis of stroke patients’ motivation. BMJ 2000, 321, 1051–1054. [Google Scholar] [CrossRef] [Green Version]
- Cramer, S.C.; Sur, M.; Dobkin, B.H.; O’Brien, C.O.; Sanger, T.D.; Trojanowski, J.Q.; Rumsey, J.M.; Hicks, R.; Cameron, J.; Chen, D.; et al. Harnessing neuroplasticity for clinical applications. Brain 2011, 134, 1591–1609. [Google Scholar] [CrossRef]
- Dobkin, B.H.; Plummer-D’Amato, P.; Elashoff, R.; Lee, J.; SIRROWS Group. International randomized clinical trial, stroke inpatient rehabilitation with reinforcement of walking speed (SIRROWS), improves outcomes. Neurorehabil. Neural Repair 2010, 24, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Mizuguchi, N.; Nakagawa, K.; Tazawa, Y.; Kanosue, K.; Nakazawa, K. Functional plasticity of the ipsilateral primary sensorimotor cortex in an elite long jumper with below-knee amputation. Neuroimage Clin. 2019, 23, 101847. [Google Scholar] [CrossRef]
- Nakagawa, K.; Takemi, M.; Nakanishi, T.; Sasaki, A.; Nakazawa, K. Cortical reorganization of lower-limb motor representations in an elite archery athlete with congenital amputation of both arms. Neuroimage Clin. 2020, 25, 102144. [Google Scholar] [CrossRef]
- Kamlin, C.; Moulton, E.; Leder, S.; Houot, M.; Meunier, S.; Rosso, C.; Lamy, J.C. Redundancy among parameters describing the input-output relation of motor evoked potentials in healthy subjects and stroke patients. Front. Neurol. 2019, 10, 535. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.M.; Bleyenheuft, Y.; Steenbergen, B. Pathophysiology of impaired hand function in children with unilateral cerebral palsy. Dev. Med. Child. Neurol. 2013, 55 (Suppl. 4), 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karni, A.; Meyer, G.; Jezzard, P.; Adams, M.M.; Turner, R.; Ungerleider, L.G. Functional MRIevidence for adult motorcortex plasticity during motor skilllearning. Nature 1995, 377, 155–158. [Google Scholar] [PubMed]
- Pascual-Leone, A.; Nguyet, D.; Cohen, L.G.; Brasil-Neto, J.P.; Cammarota, A.; Hallett, M. Modulation of muscle responses evoked by transcranial magnetic stimulation during the acquisition of new fine motor skills. J. Neurophysiol. 1995, 74, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Taubert, M.; Mehnert, J.; Pleger, B.; Villringer, A. Rapid and specific gray matter changes in M1 induced by balance training. Neuroimage 2016, 133, 399–407. [Google Scholar] [CrossRef]
- Krings, T.; Töpper, R.; Foltys, H.; Erberich, S.; Sparing, R.; Willmes, K.; Thron, A. Cortical activation patterns during complex motor tasks in piano players and control subjects. A functional magnetic resonance imaging study. Neurosci. Lett. 2000, 278, 189–193. [Google Scholar] [CrossRef]
- Naito, E.; Hirose, S. Efficient foot motor control by Neymar’s brain. Front. Hum. Neurosci. 2014, 8, 594. [Google Scholar] [CrossRef]
- Miwa, C.; Mano, T.; Saito, M.; Iwase, S.; Matsukawa, T.; Sugiyama, Y.; Koga, K. Ageing reduces sympatho-suppressive response to head-out water immersion in humans. Acta Physiol. Scand. 1996, 158, 15–20. [Google Scholar] [CrossRef]
- Kamibayashi, K.; Nakazawa, K.; Ogata, H.; Obata, H.; Akai, M.; Shinohara, M. Invariable H-reflex and sustained facilitation of stretch reflex with heightened sympathetic outflow. J. Electromyogr. Kinesiol. 2009, 19, 1053–1060. [Google Scholar] [CrossRef]
- Hjortskov, N.; Skotte, J.; Hye-Knudsen, C.; Fallentin, N. Sympathetic outflow enhances the stretch reflex response in the relaxed soleus muscle in humans. J. Appl. Physiol. 2005, 98, 1366–1370. [Google Scholar] [CrossRef] [Green Version]
- Horslen, B.C.; Murnaghan, C.D.; Inglis, J.T.; Chua, R.; Carpenter, M.G. Effects of postural threat on spinal stretch reflexes: Evidence for increased muscle spindle sensitivity? J. Neurophysiol. 2013, 110, 899–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakazawa, K.; Obata, H.; Nozaki, D.; Uehara, S.; Celnik, P. “Paralympic Brain”. Compensation and Reorganization of a Damaged Human Brain with Intensive Physical Training. Sports 2020, 8, 46. https://doi.org/10.3390/sports8040046
Nakazawa K, Obata H, Nozaki D, Uehara S, Celnik P. “Paralympic Brain”. Compensation and Reorganization of a Damaged Human Brain with Intensive Physical Training. Sports. 2020; 8(4):46. https://doi.org/10.3390/sports8040046
Chicago/Turabian StyleNakazawa, Kimitaka, Hiroki Obata, Daichi Nozaki, Shintaro Uehara, and Pablo Celnik. 2020. "“Paralympic Brain”. Compensation and Reorganization of a Damaged Human Brain with Intensive Physical Training" Sports 8, no. 4: 46. https://doi.org/10.3390/sports8040046
APA StyleNakazawa, K., Obata, H., Nozaki, D., Uehara, S., & Celnik, P. (2020). “Paralympic Brain”. Compensation and Reorganization of a Damaged Human Brain with Intensive Physical Training. Sports, 8(4), 46. https://doi.org/10.3390/sports8040046