
Role of Partial Splenectomy in Hematologic Childhood Disorders

 , ,
, , 
Abstract
:1. Introduction
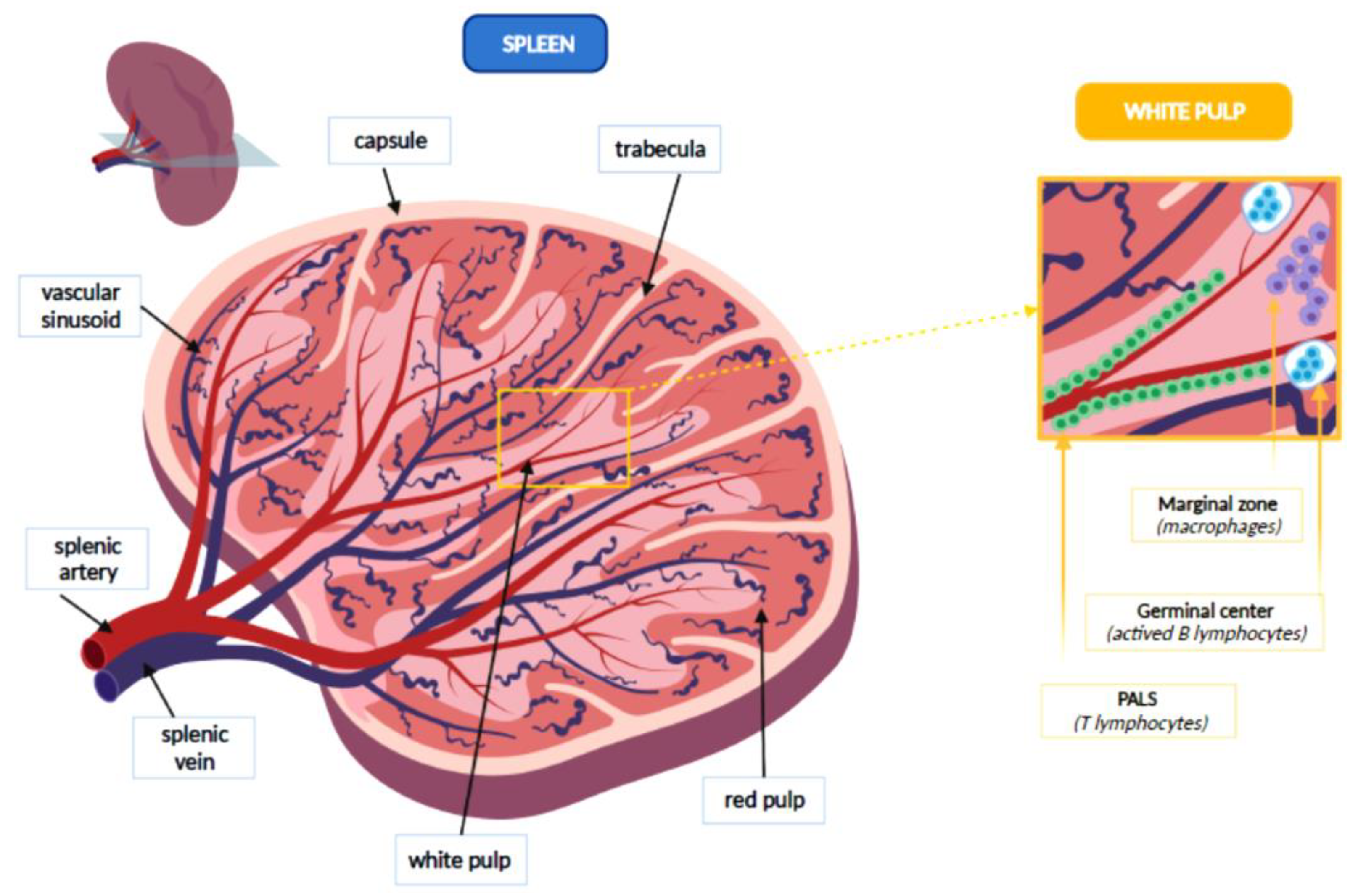
2. Anatomy and Functions of the Spleen
3. Splenectomy
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Di Buono, G.; Maienza, E.; Buscemi, S.; Gulotta, L.; Romano, G.; Agrusa, A. Laparoscopic near-total splenectomy. Report of a case. Int. J. Surg. Case. Rep. 2020, 77, S44–S47. [Google Scholar] [CrossRef]
- Diesen, D.L.; Zimmerman, S.A.; Thornburg, C.D.; Ware, R.E.; Skinner, M.; Oldham, K.T.; Rice, H.E. Partial splenectomy for children with congenital hemolytic anemia and massive splenomegaly. J. Pediatr. Surg. 2008, 43, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Bickenbach, K.A.; Gonen, M.; Labow, D.M.; Strong, V.; Heaney, M.L.; Zelenetz, A.D.; Coit, D.G. Indications for and efficacy of splenectomy for haematological disorders. Br. J. Surg. 2013, 100, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Belli, A.K.; Dönmez, C.; Özcan, Ö.; Dere, Ö.; Dirgen Çaylak, S.; Dinç Elibol, F.; Yazkan, C.; Yılmaz, N.; Nazlı, O. Adherence to vaccination recommendations after traumatic splenic injury. Ulus. Travma. Acil. Cerrahi. Derg. 2018, 24, 337–342. [Google Scholar] [CrossRef]
- Williams, L.; Warwick, R.; Dyson, M.; Bannister, L.H. Gray’s Anatomy, 37th ed.; Edinburgh: Churchill, Livingstone, 1989; p. 1598. [Google Scholar]
- Tahir, F.; Ahmed, J.; Malik, F. Post-splenectomy Sepsis: A Review of the Literature. Cureus 2020, 12, e6898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, G.M. Preventing infections in children and adults with asplenia. Hematol. Am. Soc. Hematol. Educ. Program 2020, 2020, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, S.; Arnold, D.M.; McCrae, K.R. Splenectomy for immune thrombocytopenia: Down but not out. Blood 2018, 131, 1172–1182. [Google Scholar] [CrossRef] [Green Version]
- Rab, M.A.E.; Meerveld-Eggink, A.; van Velzen-Blad, H.; van Loon, D.; Rijkers, G.T.; de Weerdt, O. Persistent changes in circulating white blood cell populations after splenectomy. Int. J. Hematol. 2018, 107, 157–165. [Google Scholar] [CrossRef]
- Leone, G.; Pizzigallo, E. Bacterial Infections Following Splenectomy for Malignant and Nonmalignant Hematologic Diseases. Mediterr. J. Hematol. Infect. Dis. 2015, 7, e2015057. [Google Scholar] [CrossRef]
- Chong, J.; Jones, P.; Spelman, D.; Leder, K.; Cheng, A.C. Overwhelming post-splenectomy sepsis in patients with asplenia and hyposplenia: A retrospective cohort study. Epidemiol. Infect. 2017, 145, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Dionne, B.; Dehority, W.; Brett, M.; Howdieshell, T.R. The Asplenic Patient: Post-Insult Immunocompetence, Infection, and Vaccination. Surg. Infect. 2017, 18, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Salvadori, M.I.; Price, V.E.; Canadian Paediatric Society, Infectious Diseases and immunization Committee. Preventing and treating infections in children with asplenia or hyposplenia. Paediatr. Child Health 2014, 19, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Madenci, A.L.; Armstrong, L.B.; Kwon, N.K.; Jiang, W.; Wolf, L.L.; Koehlmoos, T.P.; Ricca, R.L.; Weldon, C.B.; Haider, A.H.; Weil, B.R. Incidence and risk factors for sepsis after childhood splenectomy. J. Pediatr. Surg. 2019, 54, 1445–1448. [Google Scholar] [CrossRef]
- Lewis, S.M.; Williams, A.; Eisenbarth, S.C. Structure and function of the immune system in the spleen. Sci. Immunol. 2019, 4, eaau6085. [Google Scholar] [CrossRef]
- de Porto, A.P.; Lammers, A.J.; Bennink, R.J.; ten Berge, I.J.; Speelman, P.; Hoekstra, J.B. Assessment of splenic function. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1465–1473. [Google Scholar] [CrossRef] [Green Version]
- Buzelé, R.; Barbier, L.; Sauvanet, A.; Fantin, B. Medical complications following splenectomy. J. Visc. Surg. 2016, 153, 277–286. [Google Scholar] [CrossRef]
- Kruetzmann, S.; Rosado, M.M.; Weber, H.; Germing, U.; Tournilhac, O.; Peter, H.H.; Berner, R.; Peters, A.; Boehm, T.; Plebani, A.; et al. Human immunoglobulin M memory B cells controlling Streptococcus pneumoniae infections are generated in the spleen. J. Exp. Med. 2003, 197, 939–945. [Google Scholar] [CrossRef]
- Davies, J.M.; Lewis, M.P.; Wimperis, J.; Rafi, I.; Ladhani, S.; Bolton-Maggs, P.H. British Committee for Standards in Haematology. Review of guidelines for the prevention and treatment of infection in patients with an absent or dysfunctional spleen: Prepared on behalf of the British Committee for Standards in Haematology by a working party of the Haemato-Oncology task force. Br. J. Haematol. 2011, 155, 308–317. [Google Scholar] [CrossRef]
- El-Alfy, M.S.; El-Sayed, M.H. Overwhelming postsplenectomy infection: Is quality of patient knowledge enough for prevention? Hematol. J. 2004, 5, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Casciani, F.; Trudeau, M.T.; Vollmer, C.M., Jr. Perioperative Immunization for Splenectomy and the Surgeon’s Responsibility: A Review. JAMA Surg. 2020, 155, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Battista, A.; Coccia, P.; Attinà, G.; Riccardi, R. How to manage vaccinations in children with cancer. Pediatr. Blood. Cancer 2011, 57, 1104–1108. [Google Scholar] [CrossRef]
- Luu, S.; Spelman, D.; Woolley, I.J. Post-splenectomy sepsis: Preventative strategies, challenges, and solutions. Infect. Drug. Resist. 2019, 12, 2839–2851. [Google Scholar] [CrossRef] [Green Version]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using Open SAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Attinà, G.; Chiaretti, A. Additional hypotheses about why COVID-19 is milder in children than adults. Acta Paediatr. 2020, 109, 1690. [Google Scholar] [CrossRef]
- Cullingford, G.L.; Watkins, D.N.; Watts, A.D.; Mallon, D.F. Severe late postsplenectomy infection. Br. J. Surg. 1991, 78, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Rothman, J.A.; Stevens, J.L.; Gray, F.L.; Kalfa, T.A. How I approach hereditary hemolytic anemia and splenectomy. Pediatr. Blood Cancer 2020, 67, e28337. [Google Scholar] [CrossRef] [PubMed]
- Boam, T.; Sellars, P.; Isherwood, J.; Hollobone, C.; Pollard, C.; Lloyd, D.M.; Dennison, A.R.; Garcea, G. Adherence to vaccination guidelines post splenectomy: A five year follow up study. J. Infect. Public Health 2017, 10, 803–808. [Google Scholar] [CrossRef]
- Liu, G.; Fan, Y. Feasibility and Safety of Laparoscopic Partial Splenectomy: A Systematic Review. World J. Surg. 2019, 43, 1505–1518. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, P.; Yang, K.; Wu, S.; Bai, Y.; Zhu, X.; Chen, X.; Li, L.; Cao, Y.; Zhang, M. Association between splenectomy and chronic thromboembolic pulmonary hypertension: A systematic review and meta-analysis. BMJ Open 2021, 11, e038385. [Google Scholar] [CrossRef]
- Stoehr, G.A.; Stauffer, U.G.; Eber, S.W. Near-total splenectomy: A new technique for the management of hereditary spherocytosis. Ann. Surg. 2005, 241, 40–47. [Google Scholar] [CrossRef]
- Catalano, M.; Rizzo, D.; Coccia, P.; Maurizi, P.; Nanni, L.; Ruggiero, A. Can partial splenectomy preserve humoral immunity in pediatric patients? Risks and benefits of partialsplenectomy. Signa. Vitae. 2018, 14, 17–19. [Google Scholar]
- Koren, A.; Haasz, R.; Tiatler, A.; Katzuni, E. Serum immunoglobulin levels in children after splenectomy. A prospective study. Am. J. Dis. Child. 1984, 138, 53–55. [Google Scholar] [CrossRef]
- Sheikha, A.K.; Salih, Z.T.; Kasnazan, K.H.; Khoshnaw, M.K.; Al-Maliki, T.; Al-Azraqi, T.A.; Zafer, M.H. Prevention of overwhelming postsplenectomy infection in thalassemia patients by partial rather than total splenectomy. Can. J. Surg. 2007, 50, 382–386. [Google Scholar] [PubMed]
- Buesing, K.L.; Tracy, E.T.; Kiernan, C.; Pastor, A.C.; Cassidy, L.D.; Scott, J.P.; Ware, R.E.; Davidoff, A.M.; Rescorla, F.J.; Langer, J.C.; et al. Partial splenectomy for hereditary spherocytosis: A multi-institutional review. J. Pediatr. Surg. 2011, 46, 178–183. [Google Scholar] [CrossRef]
- Guizzetti, L. Total versus partial splenectomy in pediatric hereditary spherocytosis: A systematic review and meta-analysis. Pediatr. Blood Cancer 2016, 63, 1713–1722. [Google Scholar] [CrossRef]
- Rice, H.E.; Oldham, K.T.; Hillery, C.A.; Skinner, M.A.; O’Hara, S.M.; Ware, R.E. Clinical and hematologic benefits of partial splenectomy for congenital hemolytic anemias in children. Ann. Surg. 2003, 237, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Englum, B.R.; Rothman, J.; Leonard, S.; Reiter, A.; Thornburg, C.; Brindle, M.; Wright, N.; Heeney, M.M.; Smithers, C.J.; Brown, R.L.; et al. Splenectomy in Congenital Hemolytic Anemia Consortium. Hematologic outcomes after total splenectomy and partial splenectomy for congenital hemolytic anemia. J. Pediatr. Surg. 2016, 51, 122–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafezi, N.; Carpenter, K.L.; Colgate, C.L.; Gray, B.W.; Rescorla, F.J. Partial splenectomy in children: Long-term preoperative outcomes. J. Pediatr. Surg 2021, 63, 1713–1722. [Google Scholar]
- Timeus, F.; Crescenzio, N.; Longoni, D.; Doria, A.; Foglia, L.; Pagliano, S.; Vallero, S.; Decimi, V.; Svahn, J.; Palumbo, G.; et al. Paroxysmal nocturnal hemoglobinuria clones in children with acquired aplastic anemia: A multicentre study. PLoS ONE 2014, 9, e101948. [Google Scholar] [CrossRef]
- Rinninella, E.; Ruggiero, A.; Maurizi, P.; Triarico, S.; Cintoni, M.; Mele, M.C. Clinical tools to assess nutritional risk and malnutrition in hospitalized children and adolescents. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2690–2701. [Google Scholar]
- Romboli, A.; Annicchiarico, A.; Morini, A.; Castro Ruiz, C.; Pagliai, L.; Montali, F.; Costi, R. Laparoscopic Partial Splenectomy: A Critical Appraisal of an Emerging Technique. A Review of the First 457 Published Cases. J. Laparoendosc. Adv. Surg. Tech. A 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Morinis, J.; Dutta, S.; Blanchette, V.; Butchart, S.; Langer, J.C. Laparoscopic partial vs total splenectomy in children with hereditary spherocytosis. Pediatr. Surg. 2008, 43, 1649–1652. [Google Scholar] [CrossRef] [PubMed]
- Riera, M.; Buczacki, S.; Khan, Z.A. Splenic regeneration following splenectomy and impact on sepsis: A clinical review. J. R. Soc. Med. 2009, 102, 139–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| MEDICAL INDICATIONS |
| Congenital hemolytic anemia Hereditary spherocytosis Hereditary ellipsocitosis Pyruvate kinase deficiency Drepanocytosis |
| Acquired immunological disorders Autoimmune platelets Autoimmune hemolytic anemia |
| Hypersplenism Thalassemia Congestive splenomegaly Accumulation disorder (Gaucher disease, Niemann-Pick disease) |
| SURGICAL INDICATIONS |
| Traumatic rupture of the spleen |
| Intrinsic splenic diseases Cysts Hemangioma Lymphoma |
| Surgery in the left hemiabdomen |
| The risk of infection increases throughout life. |
| It is important to inform your caregiver of the state of asplenia. |
| Perform a medical evaluation before traveling especially to malaria-endemic areas. |
| Always have an antibiotic on hand. |
| Perform vaccinations against the main capsulated germs (Pneumococcus, Meningococcus and Hemophilus Influenzae type B, and annual anti-flu vaccination) |
| Be very careful about animal bites or insect bites. |
| The patient should be informed about symptoms that may indicate the onset of OPSI (high fever, myalgia, headache, vomiting, abdominal pain, chills). |
| Suggest registering in a register of patients with diabetes (if available). |
| Carry an identification plate with the indication of the condition of splenectomized. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attina’, G.; Triarico, S.; Romano, A.; Maurizi, P.; Mastrangelo, S.; Ruggiero, A. Role of Partial Splenectomy in Hematologic Childhood Disorders. Pathogens 2021, 10, 1436. https://doi.org/10.3390/pathogens10111436
Attina’ G, Triarico S, Romano A, Maurizi P, Mastrangelo S, Ruggiero A. Role of Partial Splenectomy in Hematologic Childhood Disorders. Pathogens. 2021; 10(11):1436. https://doi.org/10.3390/pathogens10111436
Chicago/Turabian StyleAttina’, Giorgio, Silvia Triarico, Alberto Romano, Palma Maurizi, Stefano Mastrangelo, and Antonio Ruggiero. 2021. "Role of Partial Splenectomy in Hematologic Childhood Disorders" Pathogens 10, no. 11: 1436. https://doi.org/10.3390/pathogens10111436
APA StyleAttina’, G., Triarico, S., Romano, A., Maurizi, P., Mastrangelo, S., & Ruggiero, A. (2021). Role of Partial Splenectomy in Hematologic Childhood Disorders. Pathogens, 10(11), 1436. https://doi.org/10.3390/pathogens10111436