
HIV Drug Resistance Mutations Detection by Next-Generation Sequencing during Antiretroviral Therapy Interruption in China


Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Study Population
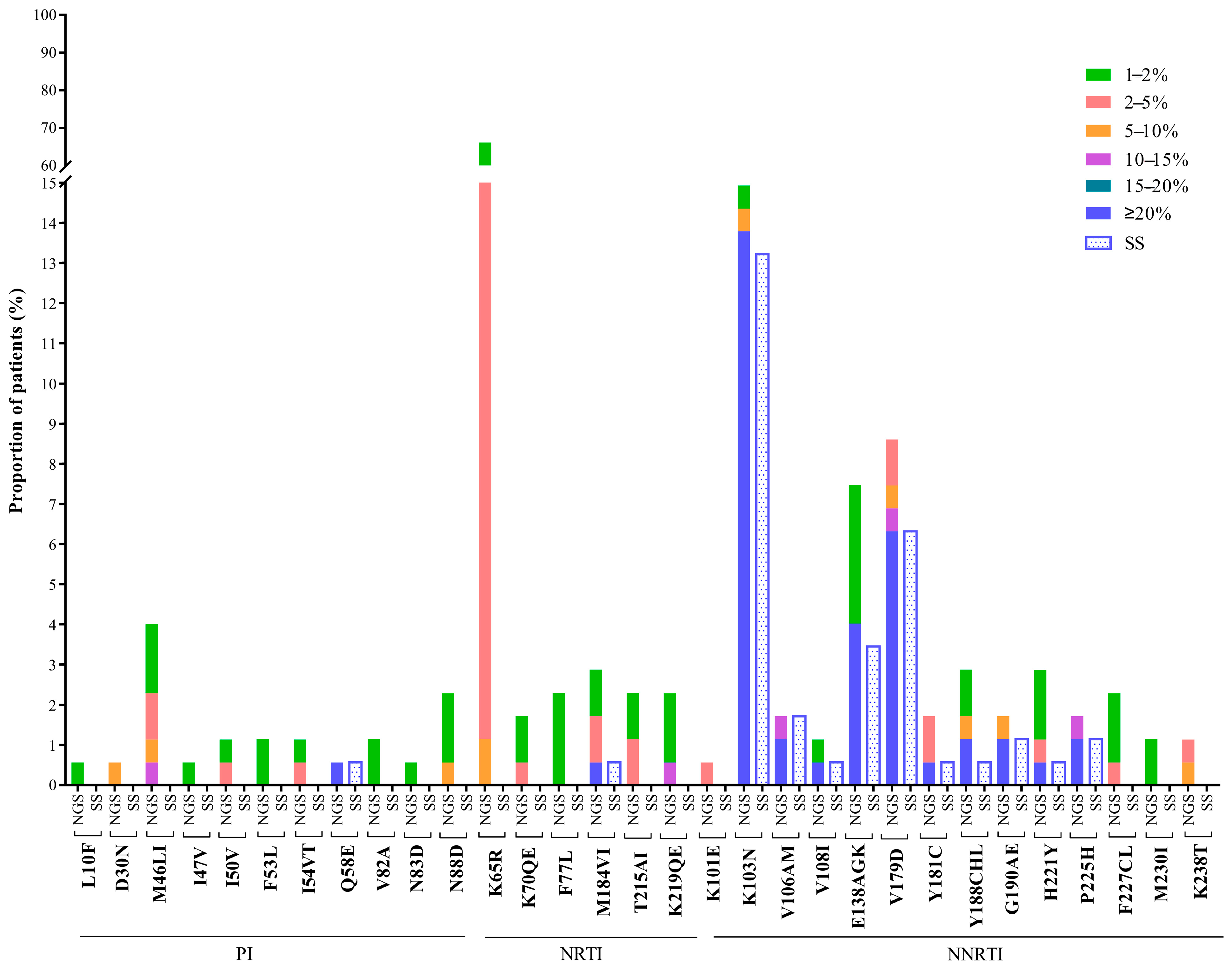
2.2. Detected HIV Drug Resistance Mutations
2.3. HIV Drug Resistance Interpretations
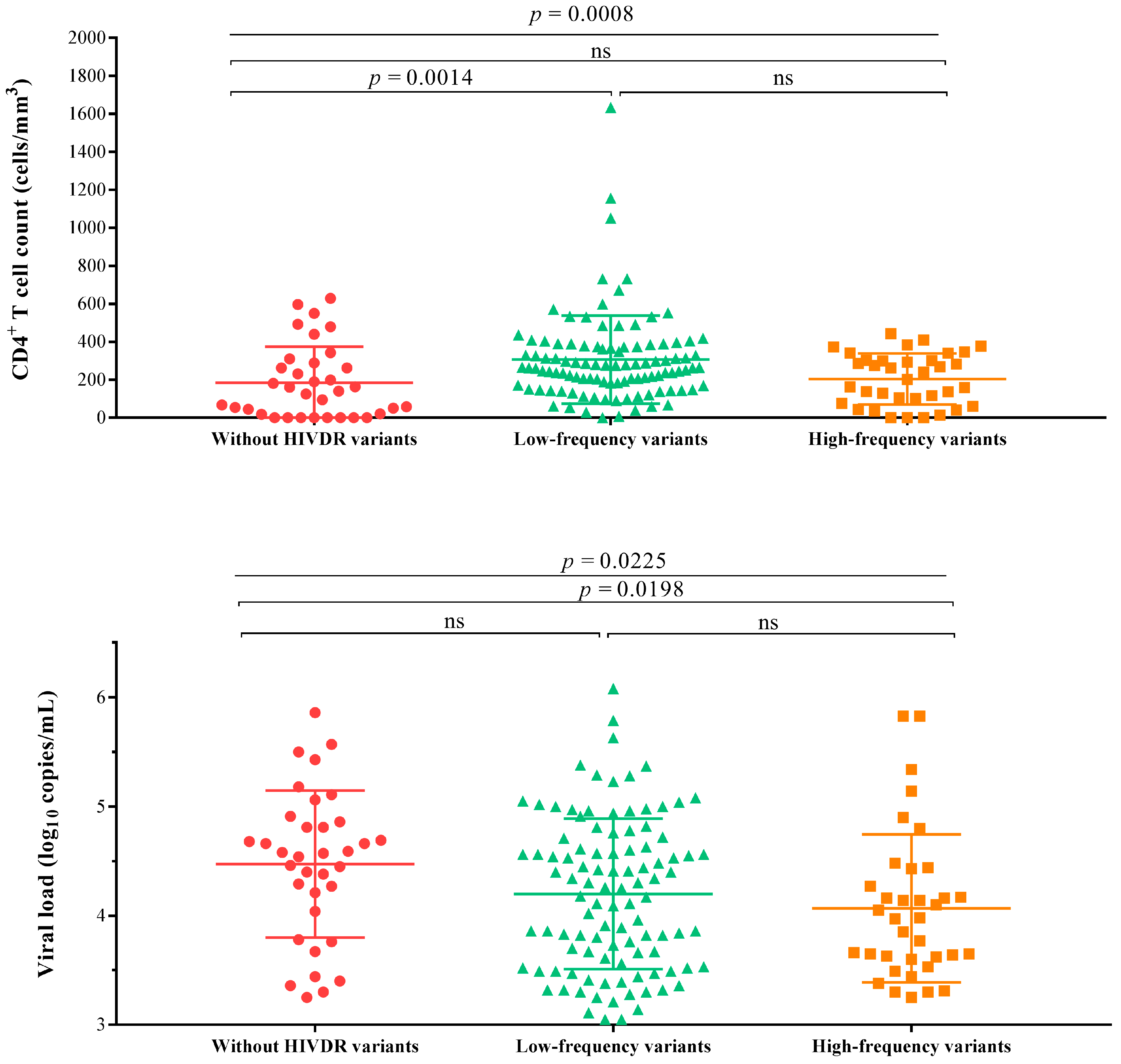
2.4. Relationship between CD4+ T Cell Count, Viral Load and HIVDR Mutation Frequency
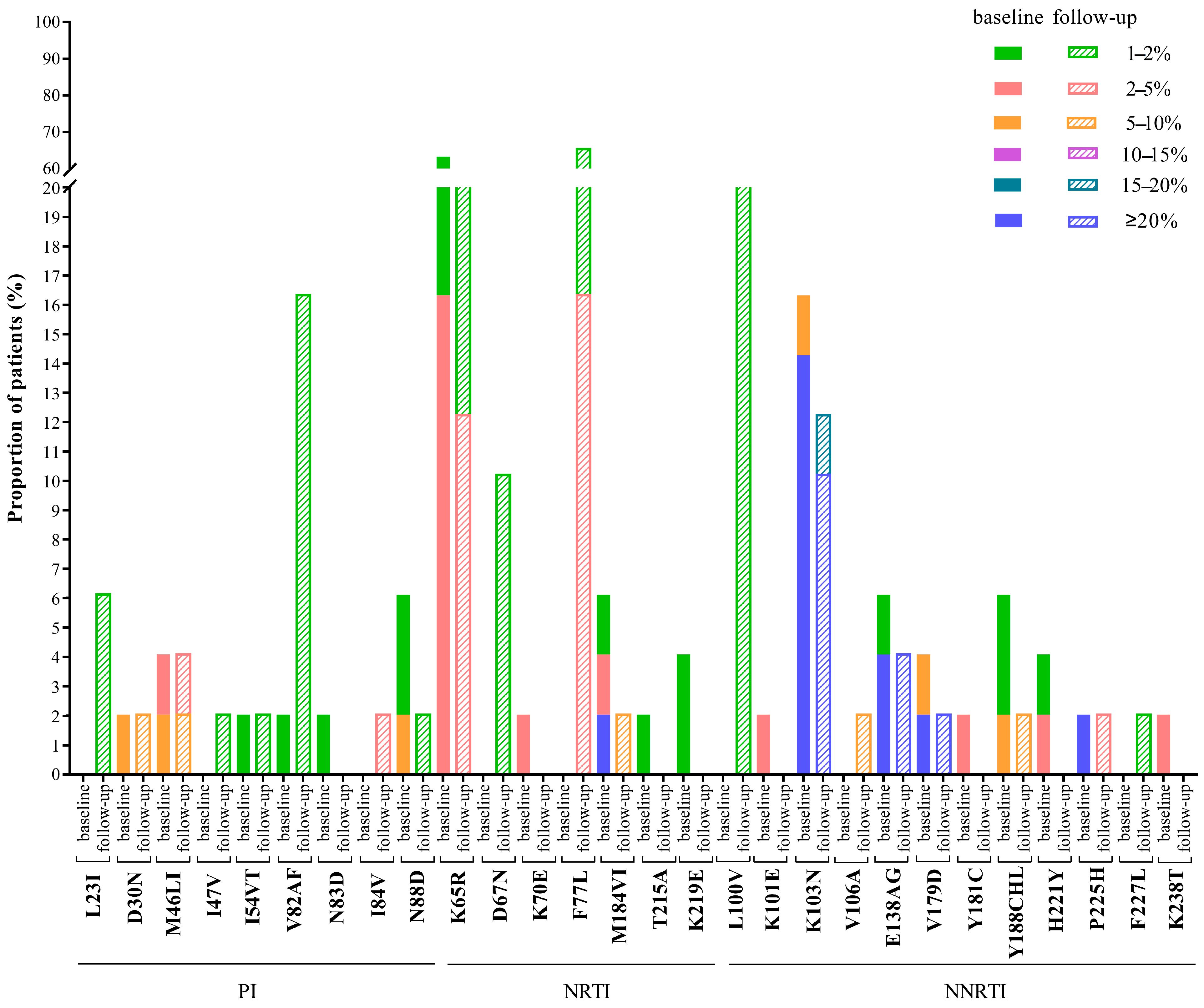
2.5. Changes of HIVDR Mutations at Follow-Up
3. Discussion
4. Materials and Methods
4.1. Study Design and Study Participants
4.2. HIV RNA Extraction and Sample Amplification
4.3. Sanger Sequencing and Drug Resistance Analysis
4.4. Next-Generation Sequencing and Drug Resistance Analysis
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poorolajal, J.; Hooshmand, E.; Mahjub, H.; Esmailnasab, N.; Jenabi, E. Survival rate of AIDS disease and mortality in HIV-infected patients: A meta-analysis. Public Health 2016, 139, 3–12. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. Latest Global and Regional Statistics on the Status of the AIDS Epidemic. 2020. Available online: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf (accessed on 27 September 2020).
- Touloumi, G.; Pantazis, N.; Antoniou, A.; Stirnadel, H.A.; Walker, S.A.; Porter, K. Highly Active Antiretroviral Therapy Interruption. JAIDS J. Acquir. Immune Defic. Syndr. 2006, 42, 554–561. [Google Scholar] [CrossRef]
- Olsen, C.H.; Mocroft, A.; Kirk, O.; Vella, S.; Blaxhult, A.; Clumeck, N.; Fisher, M.; Katlama, C.; Phillips, A.; Lundgren, J.; et al. Interruption of combination antiretroviral therapy and risk of clinical disease progression to AIDS or death. HIV Med. 2007, 8, 96–104. [Google Scholar] [CrossRef]
- Kavasery, R.; Galai, N.; Astemborski, J.; Lucas, G.M.; Celentano, D.D.; Kirk, G.D.; Mehta, S.H. Nonstructured Treatment Interruptions Among Injection Drug Users in Baltimore, MD. JAIDS J. Acquir. Immune Defic. Syndr. 2009, 50, 360–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, H.; Napravnik, S.; Eron, J.; Cole, S.; Ma, Y.; Wohl, D.; Dou, Z.; Zhang, Y.; Liu, Z.; Zhao, D.; et al. Attrition among Human Immunodeficiency Virus (HIV)- Infected Patients Initiating Antiretroviral Therapy in China, 2003–2010. PLoS ONE 2012, 7, e39414. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Uria, G.; Naik, P.K.; Pakam, R.; Midde, M. Factors associated with attrition, mortality, and loss to follow up after antiretroviral therapy initiation: Data from an HIV cohort study in India. Glob. Health Action 2013, 6, 21682. [Google Scholar] [CrossRef]
- Ananworanich, J.; Gayet-Ageron, A.; Le Braz, M.; Prasithsirikul, W.; Chetchotisakd, P.; Kiertiburanakul, S.; Munsakul, W.; Raksakulkarn, P.; Tansuphasawasdikul, S.; Sirivichayakul, S.; et al. CD4-guided scheduled treatment interruptions compared with continuous therapy for patients infected with HIV-1: Results of the Staccato randomised trial. Lancet 2006, 368, 459–465. [Google Scholar] [CrossRef]
- Hogg, R.S.; Heath, K.; Bangsberg, D.; Yip, B.; Press, N.; O’Shaughnessy, M.V.; Montaner, J.S.G. Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. AIDS 2002, 16, 1051–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira-Vaz, J.; Duque, V.; Trindade, L.; Saraiva-Da-Cunha, J.; Meliço-Silvestre, A. Detection of the protease codon 35 amino acid insertion in sequences from treatment-naïve HIV-1 subtype C infected individuals in the Central Region of Portugal. J. Clin. Virol. 2009, 46, 169–172. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on HIV Drug Resistance 2017–2021. Available online: https://www.who.int/hiv/pub/drugresistance/hivdr-action-plan-2017-2021/en/ (accessed on 15 September 2020).
- Devereux, H.L.; Youle, M.; Johnson, M.A.; Loveday, C. Rapid decline in detectability of HIV-1 drug resistance mutations after stopping therapy. Aids 1999, 13, F123–F127. [Google Scholar] [CrossRef]
- Lawrence, J.; Mayers, D.L.; Hullsiek, K.H.; Collins, G.; Abrams, D.I.; Reisler, R.B.; Crane, L.R.; Schmetter, B.S.; Dionne, T.J.; Saldanha, J.M.; et al. Structured Treatment Interruption in Patients with Multidrug-Resistant Human Immunodeficiency Virus. N. Engl. J. Med. 2003, 349, 837–846. [Google Scholar] [CrossRef]
- Taylor, S.; Jayasuriya, A.; Fisher, M.; Allan, S.; Wilkins, E.; Gilleran, G.; Heald, L.; Fidler, S.; Owen, A.; Back, D.; et al. Lopinavir/ritonavir single agent therapy as a universal combination antiretroviral therapy stopping strategy: Results from the STOP 1 and STOP 2 studies. J. Antimicrob. Chemother. 2011, 67, 675–680. [Google Scholar] [CrossRef] [Green Version]
- Casadellà, M.; Paredes, R. Deep sequencing for HIV-1 clinical management. Virus Res. 2017, 239, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Arias, A.; López, P.; Sánchez, R.; Yamamura, Y.; Rivera-Amill, V. Sanger and Next Generation Sequencing Approaches to Evaluate HIV-1 Virus in Blood Compartments. Int. J. Environ. Res. Public Health 2018, 15, 1697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, E.P.S.; Simen, B.B.; Turenchalk, G.S.; Braverman, M.S.; Abbate, I.; Aerssens, J.; Bouchez, O.; Gabriel, C.; Izopet, J.; Meixenberger, K.; et al. A Follow-Up of the Multicenter Collaborative Study on HIV-1 Drug Resistance and Tropism Testing Using 454 Ultra Deep Pyrosequencing. PLoS ONE 2016, 11, e0146687. [Google Scholar] [CrossRef]
- Nouchi, A.; Nguyen, T.; Valantin, M.A.; Simon, A.; Sayon, S.; Agher, R.; Calvez, V.; Katlama, C.; Marcelin, A.G.; Soulie, C. Dynamics of drug resistance-associated mutations in HIV-1 DNA reverse tran-scriptase sequence during effective ART. J. Antimicrob. Chemother. 2018, 73, 2141–2146. [Google Scholar] [CrossRef]
- Kozal, M.J.; Chiarella, J.; John, E.P.S.; Moreno, E.A.; Simen, B.B.; Arnold, T.E.; Lataillade, M. Prevalence of low-level HIV-1 variants with reverse transcriptase mutation K65R and the effect of antiretroviral drug exposure on variant levels. Antivir. Ther. 2011, 16, 925–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metzner, K.J.; Giulieri, S.G.; Knoepfel, S.A.; Rauch, P.; Burgisser, P.; Yerly, S.; Gunthard, H.F.; Cavassini, M. Minority Quasispecies of Drug-Resistant HIV-1 That Lead to Early Therapy Failure in Treatment-Naive and -Adherent Patients. Clin. Infect. Dis. 2009, 48, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Mbunkah, A.H.; Bertagnolio, S.; Hamers, R.L.; Hunt, G.; Inzaule, S.; De Wit, T.F.R.; Paredes, R.; Parkin, N.T.; Jordan, M.R.; Metzner, K.J.; et al. Low-Abundance Drug-Resistant HIV-1 Variants in Antiretroviral Drug-Naive Individuals: A Systematic Review of Detection Methods, Prevalence, and Clinical Impact. J. Infect. Dis. 2019, 221, 1584–1597. [Google Scholar] [CrossRef]
- Inzaule, S.C.; Hamers, R.L.; Noguera-Julian, M.; Casadellà, M.; Parera, M.; Kityo, C.; Steegen, K.; Naniche, D.; Clotet, B.; De Wit, T.F.R.; et al. Clinically relevant thresholds for ultrasensitive HIV drug resistance testing: A multi-country nested case-control study. Lancet HIV 2018, 5, e638–e646. [Google Scholar] [CrossRef]
- Kang, R.-H.; Liang, S.-J.; Ma, Y.-L.; Liang, S.; Xiao, L.; Zhang, X.-H.; Lu, H.-Y.; Xu, X.-Q.; Luo, S.-B.; Sun, X.-G.; et al. Pretreatment HIV drug resistance in adults initiating antiretroviral therapy in China, 2017. Infect. Dis. Poverty 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Zuo, Z.; Liang, S.; Sun, X.; Bussell, S.; Yan, J.; Kan, W.; Leng, X.; Liao, L.; Ruan, Y.; Shao, Y.; et al. Drug Resistance and Virological Failure among HIV-Infected Patients after a Decade of Antiretroviral Treatment Expansion in Eight Provinces of China. PLoS ONE 2016, 11, e0166661. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Sun, X.; Su, S.; Lv, C.; Zhang, X.; Lin, L.; Wang, R.; Fu, J.; Kang, D. HIV drug resistance in HIV positive individuals under antiretroviral treatment in Shandong Province, China. PLoS ONE 2017, 12, e0181997. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; He, C.; Hsi, J.H.; Xu, X.; Liu, Y.; He, J.; Ling, H.; Ding, P.; Tong, Y.; Zou, X.; et al. Virological Outcomes and Drug Resistance in Chinese Patients after 12 Months of 3TC-Based First-Line Antiretroviral Treatment, 2011–2012. PLoS ONE 2014, 9, e88305. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.; Wang, X.; Liao, L.; Ma, Y.; Su, B.; Fu, J.; He, J.; Chen, L.; Pan, X.; Dong, Y.; et al. Incidence and Associated Factors of HIV Drug Resistance in Chinese HIV-Infected Patients Receiving Antiretroviral Treatment. PLoS ONE 2013, 8, e62408. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. HIV Drug Resistance Report 2019. Available online: https://www.who.int/hiv/pub/drugresistance/hivdr-report-2019/en/ (accessed on 28 August 2020).
- Moscona, R.; Ram, D.; Wax, M.; Bucris, E.; Levy, I.; Mendelson, E.; Mor, O. Comparison between next-generation and Sanger-based sequencing for the detection of transmitted drug-resistance mutations among recently infected HIV-1 patients in Israel, 2000–2014. J. Int. AIDS Soc. 2017, 20, 21846. [Google Scholar] [CrossRef]
- Taylor, T.; Lee, E.R.; Nykoluk, M.; Enns, E.; Liang, B.; Capina, R.; Gauthier, M.-K.; Van Domselaar, G.; Sandstrom, P.; Brooks, J.; et al. A MiSeq-HyDRA platform for enhanced HIV drug resistance genotyping and surveillance. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzou, P.L.; Ariyaratne, P.; Varghese, V.; Lee, C.; Rakhmanaliev, E.; Villy, C.; Yee, M.; Tan, K.; Michel, G.; Pinsky, B.A.; et al. Comparison of anIn VitroDiagnostic Next-Generation Sequencing Assay with Sanger Sequencing for HIV-1 Genotypic Resistance Testing. J. Clin. Microbiol. 2018, 56, e00105-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stelzl, E.; Pröll, J.; Bizon, B.; Niklas, N.; Danzer, M.; Hackl, C.; Stabentheiner, S.; Gabriel, C.; Kessler, H.H. Human immunodeficiency virus type 1 drug resistance testing: Evaluation of a new ultra-deep sequencing-based protocol and comparison with the TRUGENE HIV-1 Genotyping Kit. J. Virol. Methods 2011, 178, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.-Y.; Kao, S.-W.; Liu, Z.-H.; Wu, T.-S.; Tsai, C.-L.; Lin, H.-H.; Wong, W.-W.; Chang, Y.-Y.; Chen, S.-S.; Ku, S.W.-W. Shall I trust the report? Variable performance of Sanger sequencing revealed by deep sequencing on HIV drug resistance mutation detection. Int. J. Infect. Dis. 2020, 93, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Ávila-Ríos, S.; Parkin, N.; Swanstrom, R.; Paredes, R.; Shafer, R.; Ji, H.; Kantor, R. Next-Generation Sequencing for HIV Drug Resistance Testing: Laboratory, Clinical, and Implementation Considerations. Viruses 2020, 12, 617. [Google Scholar] [CrossRef]
- Trabaud, M.-A.; Icard, V.; Ramière, C.; Tardy, J.-C.; Scholtes, C.; André, P. Comparison of HIV-1 drug-resistance genotyping by ultra-deep sequencing and sanger sequencing using clinical samples. J. Med. Virol. 2017, 89, 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Fogel, J.M.; Bonsall, D.; Cummings, V.; Bowden, R.; Golubchik, T.; De Cesare, M.; Wilson, E.A.; Gamble, T.; Del Rio, C.; Batey, D.S.; et al. Performance of a high-throughput next-generation sequencing method for analysis of HIV drug resistance and viral load. J. Antimicrob. Chemother. 2020, 75, 3510–3516. [Google Scholar] [CrossRef] [PubMed]
- Dessilly, G.; Goeminne, L.; Vandenbroucke, A.-T.; Dufrasne, F.E.; Martin, A.; Kabamba-Mukabi, B. First evaluation of the Next-Generation Sequencing platform for the detection of HIV-1 drug resistance mutations in Belgium. PLoS ONE 2018, 13, e0209561. [Google Scholar] [CrossRef]
- Liu, T.F.; Shafer, R.W. Web Resources for HIV Type 1 Genotypic-Resistance Test Interpretation. Clin. Infect. Dis. 2006, 42, 1608–1618. [Google Scholar] [CrossRef] [Green Version]
- Clutter, D.S.; Jordan, M.R.; Bertagnolio, S.; Shafer, R.W. HIV-1 drug resistance and resistance testing. Infect. Genet. Evol. 2016, 46, 292–307. [Google Scholar] [CrossRef] [Green Version]
- Mocroft, A.; Phillips, A.N.; Gatell, J.; Ledergerber, B.; Fisher, M.; Clumeck, N.; Losso, M.; Lazzarin, A.; Fätkenheuer, G.; Lundgren, J.D. Normalisation of CD4 counts in patients with HIV-1 infection and maximum virological suppression who are taking combination antiretroviral therapy: An observational cohort study. Lancet 2007, 370, 407–413. [Google Scholar] [CrossRef]
- El-Sadr, W.; Lundgren, J.D.; Neaton, J.D.; Gordin, F.; Abrams, D.; Arduino, R.C.; Babiker, A.; Burman, W.J.; Clumeck, N.; Cohen, C.; et al. CD4+ Count–Guided Interruption of Antiretroviral Treatment. N. Engl. J. Med. 2006, 355, 2283–2296. [Google Scholar] [CrossRef] [Green Version]
- E Iarikov, D.; Irizarry-Acosta, M.; Martorell, C.; A Rauch, C.; Hoffman, R.P.; Skiest, D.J. Use of HIV Resistance Testing After Prolonged Treatment Interruption. JAIDS J. Acquir. Immune Defic. Syndr. 2010, 53, 333–337. [Google Scholar] [CrossRef]
- Hill, A.L.; Rosenbloom, D.I.S.; Nowak, M.A.; Siliciano, R.F. Insight into treatment of HIV infection from viral dynamics models. Immunol. Rev. 2018, 285, 9–25. [Google Scholar] [CrossRef]
- Paredes, R.; Sagar, M.; Marconi, V.C.; Hoh, R.; Martin, J.N.; Parkin, N.T.; Petropoulos, C.J.; Deeks, S.G.; Kuritzkes, D.R. In Vivo Fitness Cost of the M184V Mutation in Multidrug-Resistant Human Immunodeficiency Virus Type 1 in the Absence of Lamivudine. J. Virol. 2008, 83, 2038–2043. [Google Scholar] [CrossRef] [Green Version]
- Mohamed, S.; Ravet, S.; Camus, C.; Khiri, H.; Olive, D.; Halfon, P. Clinical and analytical relevance of NNRTIs minority mutations on viral failure in HIV-1 infected patients. J. Med. Virol. 2014, 86, 394–403. [Google Scholar] [CrossRef]
- Lei, L.; Zhong-Bao, Z.; Ling-Jie, L.; Shu-Jia, L.; Yan-Ling, M.; Guo-Hui, W.; Shu, L.; Sui-An, T.; Jian-Mei, H.; Yi-Ming, S.; et al. The drug resistance in HIV/AIDS patients who had stopped ART in 2016. China Trop. Med. 2018, 18, 1613–1618. [Google Scholar]
- Inzaule, S.; Yang, C.; Kasembeli, A.; Nafisa, L.; Okonji, J.; Oyaro, B.; Lando, R.; Mills, L.A.; Laserson, K.; Thomas, T.; et al. Field Evaluation of a Broadly Sensitive HIV-1 In-House Genotyping Assay for Use with both Plasma and Dried Blood Spot Specimens in a Resource-Limited Country. J. Clin. Microbiol. 2012, 51, 529–539. [Google Scholar] [CrossRef] [Green Version]
- Ravi, R.K.; Walton, K.; Khosroheidari, M. MiSeq: A Next Generation Sequencing Platform for Genomic Analysis. In Methods in Molecular Biology; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2018; Volume 1706, pp. 223–232. [Google Scholar]
- Nykoluk, M.; Taylor, T.; Enns, E.; Ji, H. HyDRA Web User Guide. 2016. Available online: https://hydra.canada.ca/pages/about?lang=en-CA (accessed on 20 August 2019).




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number (%) |
|---|---|
| Total | 174 |
| Age | |
| 18–30 | 20 (11.5) |
| 30–50 | 78 (44.8) |
| ≥50 | 76 (43.7) |
| Gender | |
| Male | 115 (66.1) |
| Female | 59 (33.9) |
| Education | |
| Illiterate and primary school | 114 (65.5) |
| Secondary school and above | 60 (34.5) |
| Marital status | |
| Married or living with partner | 117 (67.2) |
| Single | 32 (18.4) |
| Other | 25 (14.4) |
| Route of HIV infection | |
| Heterosexual | 107 (61.5) |
| Homosexual | 7 (4.0) |
| Injecting drug using | 48 (27.6) |
| Other | 12 (6.9) |
| Subtype | |
| CRF01_AE | 35 (20.1) |
| CRF07_BC | 61 (35.1) |
| CRF08_BC | 58 (33.3) |
| B′ | 16 (9.2) |
| Other a | 4 (2.3) |
| CD4+ T cell count at the time of investigation(per uL) | |
| <200 | 70 (40.2) |
| 200–350 | 62 (35.6) |
| ≥350 | 42 (24.2) |
| Antiretroviral regimen before discontinuation | |
| d4T+3TC+EFV/NVP | 1 (0.6) |
| AZT+3TC+EFV/NVP | 66 (37.9) |
| TDF+3TC+EFV/NVP | 83 (47.7) |
| AZT/TDF+3TC+LPV/r | 24 (13.8) |
| Duration of treatment before ART interruption(median, (IQR), months) | 16 (7–26) |
| Duration of ART interruption at survey (median, (IQR), months) | 12 (6–24) |
| SS | 20% NGS a | 15% NGS a | 10% NGS a | 5% NGS a | 2% NGS a | 1% NGS a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SS or NGS at Various Thresholds | N (%) | N (%) | p Value | N (%) | p Value | N (%) | p Value | N (%) | p Value | N (%) | p Value | N (%) | p Value |
| Any classes | 34 (19.5) | 36 (20.7) | 0.317 | 36 (20.7) | 0.317 | 37 (21.3) | 0.180 | 42 (24.1) | 0.011 | 79 (45.4) | <0.001 | 139 (79.9) | <0.001 |
| PI-related | 1 (0.6) | 1 (0.6) | 1.000 | 1 (0.6) | 1.000 | 2 (1.2) | 0.317 | 5 (2.9) | 0.046 | 9 (5.2) | 0.005 | 23 (13.2) | <0.001 |
| NRTI-related | 1 (0.6) | 1 (0.6) | 1.000 | 1 (0.6) | 1.000 | 1 (0.6) | 1.000 | 3 (1.7) | 0.157 | 43 (24.7) | <0.001 | 120 (69.0) | <0.001 |
| NNRTI-related | 33 (19.0) | 35 (20.1) | 0.317 | 35 (20.1) | 0.317 | 35 (20.1) | 0.317 | 36 (20.7) | 0.180 | 43 (24.7) | 0.004 | 51 (29.3) | <0.001 |
| EFV/NVP | 27 (15.5) | 28 (16.1) | 0.564 | 28 (16.1) | 0.564 | 29 (16.7) | 0.317 | 31 (17.8) | 0.103 | 37 (21.3) | 0.004 | 46 (26.4) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Liang, S.; Zhou, C.; Chen, M.; Liang, S.; Liu, C.; Zuo, Z.; Liu, L.; Feng, Y.; Song, C.; et al. HIV Drug Resistance Mutations Detection by Next-Generation Sequencing during Antiretroviral Therapy Interruption in China. Pathogens 2021, 10, 264. https://doi.org/10.3390/pathogens10030264
Li M, Liang S, Zhou C, Chen M, Liang S, Liu C, Zuo Z, Liu L, Feng Y, Song C, et al. HIV Drug Resistance Mutations Detection by Next-Generation Sequencing during Antiretroviral Therapy Interruption in China. Pathogens. 2021; 10(3):264. https://doi.org/10.3390/pathogens10030264
Chicago/Turabian StyleLi, Miaomiao, Shujia Liang, Chao Zhou, Min Chen, Shu Liang, Chunhua Liu, Zhongbao Zuo, Lei Liu, Yi Feng, Chang Song, and et al. 2021. "HIV Drug Resistance Mutations Detection by Next-Generation Sequencing during Antiretroviral Therapy Interruption in China" Pathogens 10, no. 3: 264. https://doi.org/10.3390/pathogens10030264
APA StyleLi, M., Liang, S., Zhou, C., Chen, M., Liang, S., Liu, C., Zuo, Z., Liu, L., Feng, Y., Song, C., Xing, H., Ruan, Y., Shao, Y., & Liao, L. (2021). HIV Drug Resistance Mutations Detection by Next-Generation Sequencing during Antiretroviral Therapy Interruption in China. Pathogens, 10(3), 264. https://doi.org/10.3390/pathogens10030264