
18F-FDG-PET/MR in Alveolar Echinococcosis: Multiparametric Imaging in a Real-World Setting

 ,
,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
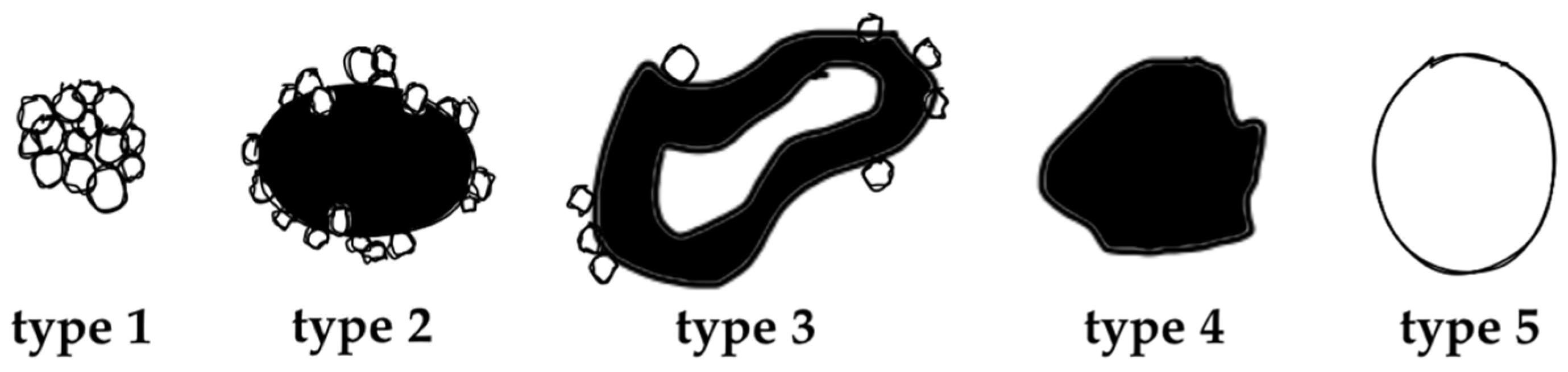
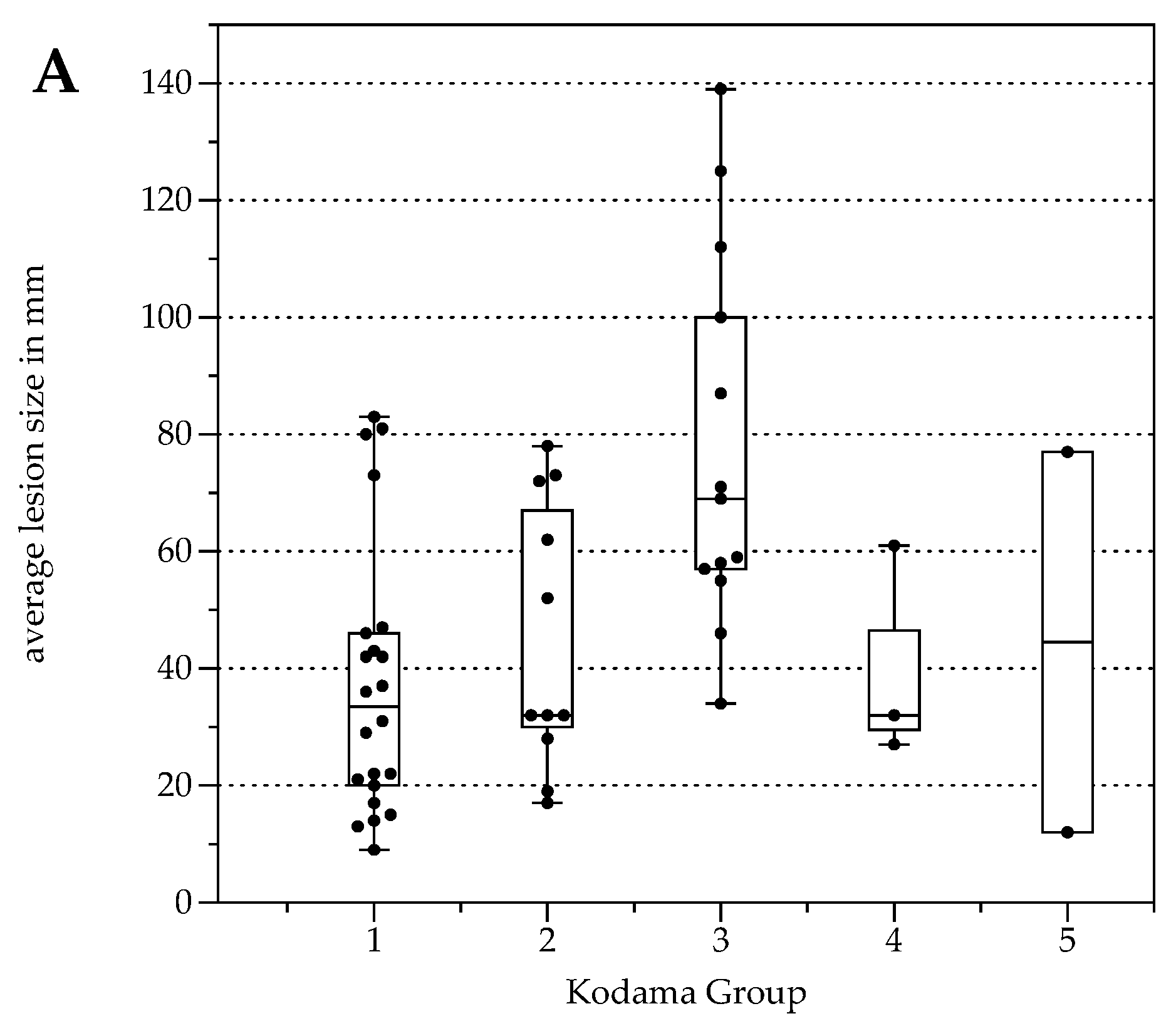
2.2. Kodama’s MRI Classification
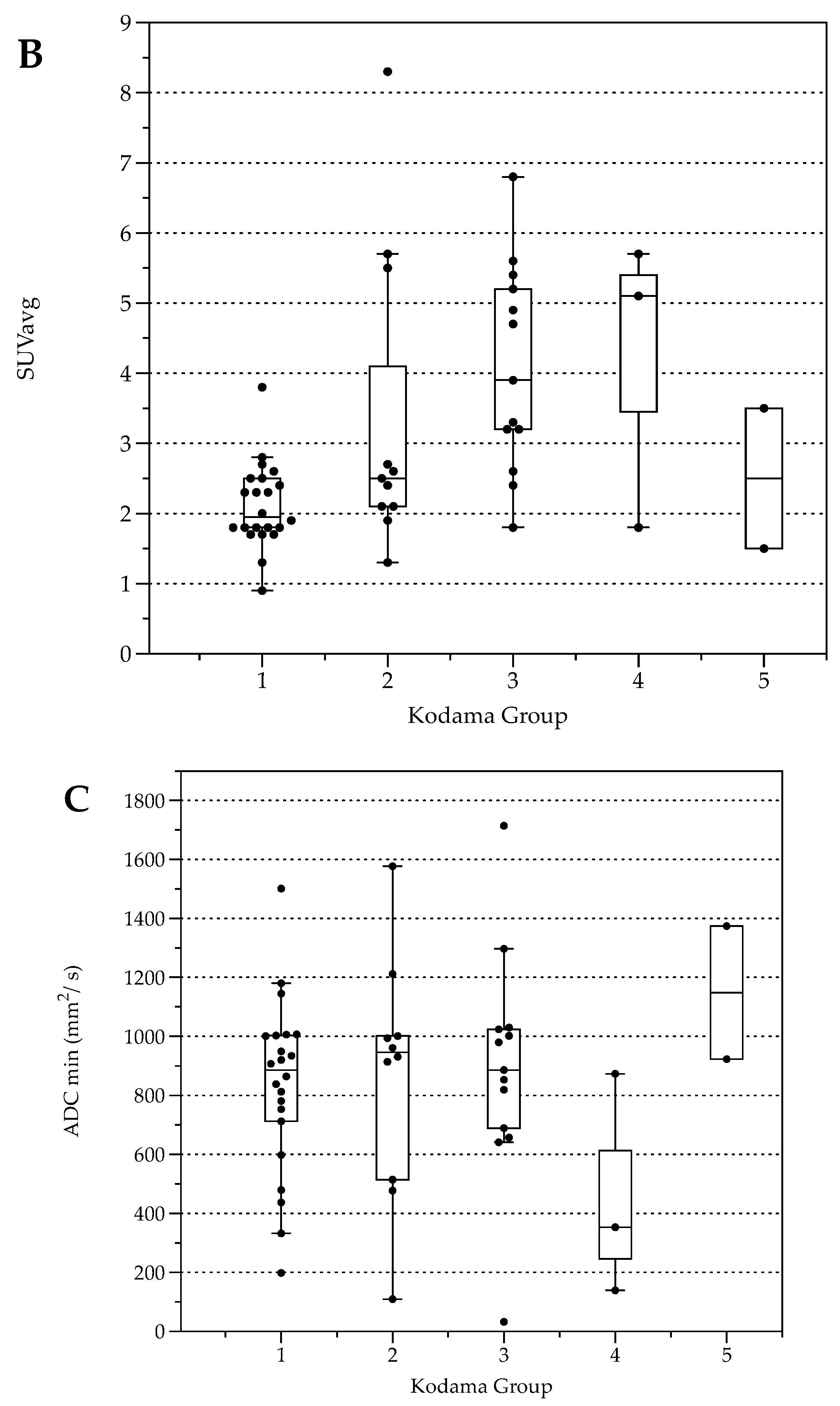
2.3. Lesion Characterization by FDG Uptake and Diffusion Restriction
2.4. FDG-PET Radiation Dose
3. Discussion
4. Material and Methods
4.1. Study Population
4.2. Imaging Study
4.3. Image Analysis
4.4. Serological Testing
4.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romig, T.; Deplazes, P.; Jenkins, D.; Giraudoux, P.; Massolo, A.; Craig, P.S.; Wassermann, M.; Takahashi, K.; de la Rue, M. Ecology and Life Cycle Patterns of Echinococcus Species. Adv. Parasitol. 2017, 95, 213–314. [Google Scholar] [PubMed]
- Eckert, J.; Deplazes, P. Biological, Epidemiological, and Clinical Aspects of Echinococcosis, a Zoonosis of Increasing Concern. Clin. Microbiol. Rev. 2004, 17, 107–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, P.S.; Budke, C.M.; Schantz, P.M.; Li, T.; Qiu, J.; Yang, Y.; Zeyhle, E.; Rogan, M.T.; Ito, A. Human Echinococcosis: A Neglected Disease? Trop. Med. Health 2007, 35, 283–292. [Google Scholar] [CrossRef] [Green Version]
- Kern, P. Clinical Features and Treatment of Alveolar Echinococcosis. Curr. Opin. Infect. Dis. 2010, 23, 505–512. [Google Scholar] [CrossRef]
- Miguet, J.P.; Bresson-Hadni, S. Alveolar Echinococcosis of the Liver. J. Hepatol. 1989, 8, 373–379. [Google Scholar] [CrossRef]
- Ammann, R.W.; Ilitsch, N.; Marincek, B.; Freiburghaus, A.U. Effect of Chemotherapy on the Larval Mass and the Long-Term Course of Alveolar Echinococcosis. Swiss Echinococcosis Study Group. Hepatology 1994, 19, 735–742. [Google Scholar] [CrossRef]
- Reuter, S.; Jensen, B.; Buttenschoen, K.; Kratzer, W.; Kern, P. Benzimidazoles in the Treatment of Alveolar Echinococcosis: A Comparative Study and Review of the Literature. J. Antimicrob. Chemother. 2000, 46, 451–456. [Google Scholar] [CrossRef] [Green Version]
- Brunetti, E.; Kern, P.; Vuitton, D.A. Writing Panel for the WHO-IWGE Expert Consensus for the Diagnosis and Treatment of Cystic and Alveolar Echinococcosis in Humans. Acta Trop. 2010, 114, 1–16. [Google Scholar] [CrossRef]
- Tamarozzi, F.; Silva, R.; Fittipaldo, V.A.; Buonfrate, D.; Gottstein, B.; Siles-Lucas, M. Serology for the Diagnosis of Human Hepatic Cystic Echinococcosis and Its Relation with Cyst Staging: A Systematic Review of the Literature with Meta-Analysis. PLoS Negl. Trop. Dis. 2021, 15, e0009370. [Google Scholar] [CrossRef]
- Hotz, J.F.; Peters, L.; Kapp-Schwörer, S.; Theis, F.; Eberhardt, N.; Essig, A.; Grüner, B.; Hagemann, J.B. Evaluation of Serological Markers in Alveolar Echinococcosis Emphasizing the Correlation of PET-CTI Tracer Uptake with RecEm18 and Echinococcus-Specific IgG. Pathogens 2022, 11, 239. [Google Scholar] [CrossRef]
- Sulima, M.; Szostakowska, B.; Nahorski, W.; Sikorska, K.; Wołyniec, W.; Wąż, P. The Usefulness of Commercially Available Serological Tests in the Diagnosis and Monitoring of Treatment in Patients with Alveolar Echinococcosis. Clin. Exp. Hepatol. 2019, 5, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Nüssle, K.; Kolokythas, O.; Haug, U.; Rieber, A.; Kern, P.; Kratzer, W. Alveolar Liver Echinococcosis: A Comparative Study of Three Imaging Techniques. Infection 2001, 29, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Kratzer, W.; Gruener, B.; Kaltenbach, T.E.M.; Ansari-Bitzenberger, S.; Kern, P.; Fuchs, M.; Mason, R.A.; Barth, T.F.E.; Haenle, M.M.; Hillenbrand, A.; et al. Proposal of an Ultrasonographic Classification for Hepatic Alveolar Echinococcosis: Echinococcosis Multilocularis Ulm Classification-Ultrasound. World J. Gastroenterol. 2015, 21, 12392–12402. [Google Scholar] [CrossRef] [PubMed]
- Graeter, T.; Kratzer, W.; Oeztuerk, S.; Haenle, M.M.; Mason, R.A.; Hillenbrand, A.; Kull, T.; Barth, T.F.; Kern, P.; Gruener, B. Proposal of a Computed Tomography Classification for Hepatic Alveolar Echinococcosis. World J. Gastroenterol. 2016, 22, 3621–3631. [Google Scholar] [CrossRef] [PubMed]
- Grimm, J.; Beck, A.; Nell, J.; Schmidberger, J.; Hillenbrand, A.; Beer, A.J.; Dezsényi, B.; Shi, R.; Beer, M.; Kern, P.; et al. Combining Computed Tomography and Histology Leads to an Evolutionary Concept of Hepatic Alveolar Echinococcosis. Pathogens 2020, 9, 634. [Google Scholar] [CrossRef]
- Kantarci, M.; Bayraktutan, U.; Karabulut, N.; Aydinli, B.; Ogul, H.; Yuce, I.; Calik, M.; Eren, S.; Atamanalp, S.S.; Oto, A. Alveolar Echinococcosis: Spectrum of Findings at Cross-Sectional Imaging. Radiographics 2012, 32, 2053–2070. [Google Scholar] [CrossRef]
- Yangdan, C.-R.; Wang, C.; Zhang, L.-Q.; Ren, B.; Fan, H.-N.; Lu, M.-D. Recent Advances in Ultrasound in the Diagnosis and Evaluation of the Activity of Hepatic Alveolar Echinococcosis. Parasitol. Res. 2021, 120, 3077–3082. [Google Scholar] [CrossRef]
- Schuhbaur, J.; Schweizer, M.; Philipp, J.; Schmidberger, J.; Schlingeloff, P.; Kratzer, W. Long-Term Follow-up of Liver Alveolar Echinococcosis Using Echinococcosis Multilocularis Ultrasound Classification. World J. Gastroenterol. 2021, 27, 6939–6950. [Google Scholar] [CrossRef]
- Kodama, Y.; Fujita, N.; Shimizu, T.; Endo, H.; Nambu, T.; Sato, N.; Todo, S.; Miyasaka, K. Alveolar Echinococcosis: MR Findings in the Liver. Radiology 2003, 228, 172–177. [Google Scholar] [CrossRef]
- Brumpt, É.; Liu, W.; Graeter, T.; Calame, P.; Rong, S.; Jiang, Y.; Li, W.; Bao, H.; Delabrousse, É. XUUB consortium Kodama-XUUB: An Informative Classification for Alveolar Echinococcosis Hepatic Lesions on Magnetic Resonance Imaging. Parasite 2021, 28, 66. [Google Scholar] [CrossRef]
- Ammann, R.W.; Stumpe, K.D.M.; Grimm, F.; Deplazes, P.; Huber, S.; Bertogg, K.; Fischer, D.R.; Müllhaupt, B. Outcome after Discontinuing Long-Term Benzimidazole Treatment in 11 Patients with Non-Resectable Alveolar Echinococcosis with Negative FDG-PET/CT and Anti-EmII/3–10 Serology. PLoS Negl. Trop. Dis. 2015, 9, e0003964. [Google Scholar] [CrossRef] [PubMed]
- Husmann, L.; Muehlematter, U.J.; Grimm, F.; Ledergerber, B.; Messerli, M.; Kudura, K.; Gruenig, H.; Muellhaupt, B.; Hasse, B.; Huellner, M.W. PET/CT Helps to Determine Treatment Duration in Patients with Resected as Well as Inoperable Alveolar Echinococcosis. Parasitol. Int. 2021, 83, 102356. [Google Scholar] [CrossRef] [PubMed]
- Aini, A.; Yimingjiang, M.; Yasen, A.; Ran, B.; Jiang, T.; Li, X.; Wang, J.; Abulizi, A.; Li, Z.; Shao, Y.; et al. Quantitative Evaluation of Range and Metabolic Activity of Hepatic Alveolar Echinococcosis Lesion Microenvironment Using PET/CT and Multi-Site Sampling Method. BMC Infect. Dis. 2021, 21, 702. [Google Scholar] [CrossRef] [PubMed]
- Becce, F.; Pomoni, A.; Uldry, E.; Halkic, N.; Yan, P.; Meuli, R.; Schmidt, S. Alveolar Echinococcosis of the Liver: Diffusion-Weighted MRI Findings and Potential Role in Lesion Characterisation. Eur. J. Radiol. 2014, 83, 625–631. [Google Scholar] [CrossRef] [Green Version]
- Reuter, S.; Schirrmeister, H.; Kratzer, W.; Dreweck, C.; Reske, S.N.; Kern, P. Pericystic Metabolic Activity in Alveolar Echinococcosis: Assessment and Follow-Up by Positron Emission Tomography. Clin. Infect. Dis. 1999, 29, 1157–1163. [Google Scholar] [CrossRef]
- Stumpe, K.D.M.; Renner-Schneiter, E.C.; Kuenzle, A.K.; Grimm, F.; Kadry, Z.; Clavien, P.-A.; Deplazes, P.; von Schulthess, G.K.; Muellhaupt, B.; Ammann, R.W.; et al. F-18-Fluorodeoxyglucose (FDG) Positron-Emission Tomography of Echinococcus Multilocularis Liver Lesions: Prospective Evaluation of Its Value for Diagnosis and Follow-up during Benzimidazole Therapy. Infection 2007, 35, 11–18. [Google Scholar] [CrossRef]
- Reuter, S.; Buck, A.; Manfras, B.; Kratzer, W.; Seitz, H.M.; Darge, K.; Reske, S.N.; Kern, P. Structured Treatment Interruption in Patients with Alveolar Echinococcosis. Hepatology 2004, 39, 509–517. [Google Scholar] [CrossRef]
- Al-Nabhani, K.Z.; Syed, R.; Michopoulou, S.; Alkalbani, J.; Afaq, A.; Panagiotidis, E.; O’Meara, C.; Groves, A.; Ell, P.; Bomanji, J. Qualitative and Quantitative Comparison of PET/CT and PET/MR Imaging in Clinical Practice. J. Nucl. Med. 2014, 55, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Azizi, A.; Blagosklonov, O.; Lounis, A.; Berthet, L.; Vuitton, D.-A.; Bresson-Hadni, S.; Delabrousse, E. Alveolar Echinococcosis: Correlation between Hepatic MRI Findings and FDG-PET/CT Metabolic Activity. Abdom. Imaging 2015, 40, 56–63. [Google Scholar] [CrossRef]
- Lötsch, F.; Waneck, F.; Groger, M.; Auer, H.; Kaczirek, K.; Rausch, I.; Wadsak, W.; Hacker, M.; Lagler, H.; Ramharter, M.; et al. FDG—PET/MRI Imaging for the Management of Alveolar Echinococcosis: Initial Clinical Experience at a Reference Centre in Austria. Trop. Med. Int. Health 2019, 24, 663–670. [Google Scholar] [CrossRef]
- Huang, B.; Law, M.W.-M.; Khong, P.-L. Whole-Body PET/CT Scanning: Estimation of Radiation Dose and Cancer Risk. Radiology 2009, 251, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Graeter, T.; Eberhardt, N.; Shi, R.; Schmidberger, J.; Beer, A.J.; Beer, M.; Henne-Bruns, D.; Hillenbrand, A.; Barth, T.F.E.; Grimm, J.; et al. Hepatic Alveolar Echinococcosis: Correlation between Computed Tomography Morphology and Inflammatory Activity in Positron Emission Tomography. Sci. Rep. 2020, 10, 11808. [Google Scholar] [CrossRef] [PubMed]
- Grüner, B.; Kern, P.; Mayer, B.; Gräter, T.; Hillenbrand, A.; Barth, T.E.F.; Muche, R.; Henne-Bruns, D.; Kratzer, W.; Kern, P. Comprehensive Diagnosis and Treatment of Alveolar Echinococcosis: A Single-Center, Long-Term Observational Study of 312 Patients in Germany. GMS Infect. Dis. 2017, 5, Doc01. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | |
|---|---|
| Age at diagnosis (mean, range) | 46.6, 17–73 |
| IgE levels (mean, range) | 331.5, 7.7–5728.0 |
| IgG levels (mean, range) | 50.9, 0–252.0 |
| ELISA Em2+ (positive/negative) | 39/12 |
| No. | |
|---|---|
| Liver involvement, N0 M0 | |
| P1 | 2 |
| P2 | 5 |
| P3 | 11 |
| P4 | 12 |
| PX, N1 and M0 | 15 |
| PX, NX and M1 | 6 |
| Lesion Type | No. of Lesions | No. of Lesions with SUVavg > 2.5 | No. of Lesions with Diffusion Restriction < 0.8 × 10−3 mm2/s | Mean Lesion Size in Millimeter, Range |
|---|---|---|---|---|
| Type 1 | 22 (43%) | 6 | 6 | 37, 9–83 |
| Type 2 | 11 (22%) | 6 | 3 | 45, 19–27 |
| Type 3 | 13 (25%) | 11 | 1 | 139, 34–139 |
| Type 4 | 3 (6%) | 2 | 1 | 40, 27–61 |
| Type 5 | 2 (4%) | 1 | 0 | 44, 12–77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eberhardt, N.; Peters, L.; Kapp-Schwoerer, S.; Beer, M.; Beer, A.J.; Grüner, B.; Thaiss, W.M. 18F-FDG-PET/MR in Alveolar Echinococcosis: Multiparametric Imaging in a Real-World Setting. Pathogens 2022, 11, 348. https://doi.org/10.3390/pathogens11030348
Eberhardt N, Peters L, Kapp-Schwoerer S, Beer M, Beer AJ, Grüner B, Thaiss WM. 18F-FDG-PET/MR in Alveolar Echinococcosis: Multiparametric Imaging in a Real-World Setting. Pathogens. 2022; 11(3):348. https://doi.org/10.3390/pathogens11030348
Chicago/Turabian StyleEberhardt, Nina, Lynn Peters, Silke Kapp-Schwoerer, Meinrad Beer, Ambros J. Beer, Beate Grüner, and Wolfgang M. Thaiss. 2022. "18F-FDG-PET/MR in Alveolar Echinococcosis: Multiparametric Imaging in a Real-World Setting" Pathogens 11, no. 3: 348. https://doi.org/10.3390/pathogens11030348
APA StyleEberhardt, N., Peters, L., Kapp-Schwoerer, S., Beer, M., Beer, A. J., Grüner, B., & Thaiss, W. M. (2022). 18F-FDG-PET/MR in Alveolar Echinococcosis: Multiparametric Imaging in a Real-World Setting. Pathogens, 11(3), 348. https://doi.org/10.3390/pathogens11030348