


Prolonged Inflammation and Infectious Changes in the Corneal Epithelium Are Associated with Persistent Epithelial Defect (PED)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
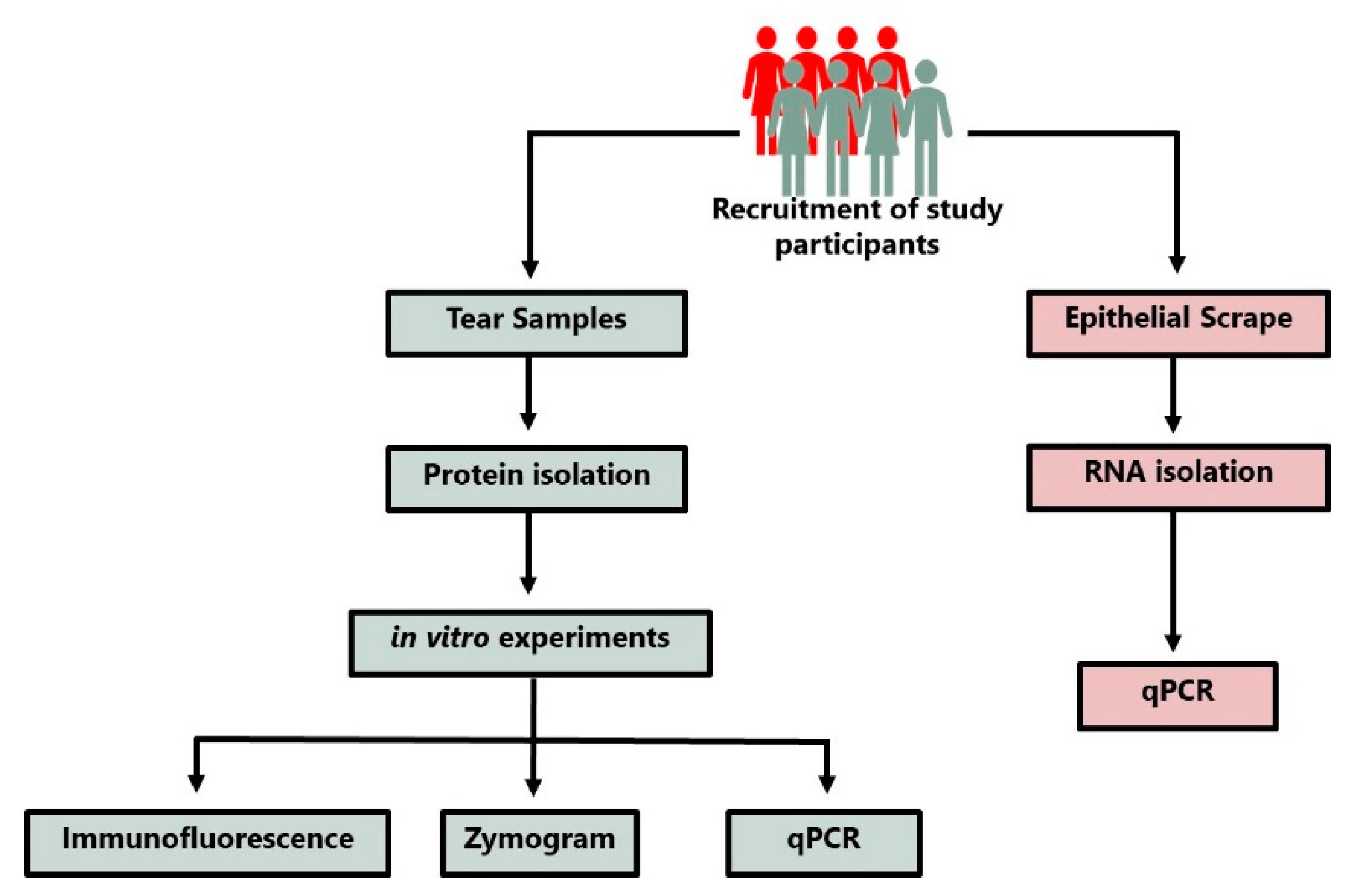
2.1. Study Design
2.2. Cell Culture and Maintenance
2.3. Extraction of Tears Protein and HCLE Treatment
2.4. Gelatin Zymography
2.5. Immunofluorescence
2.6. Data Analysis
2.7. Correlation Plot
3. Results
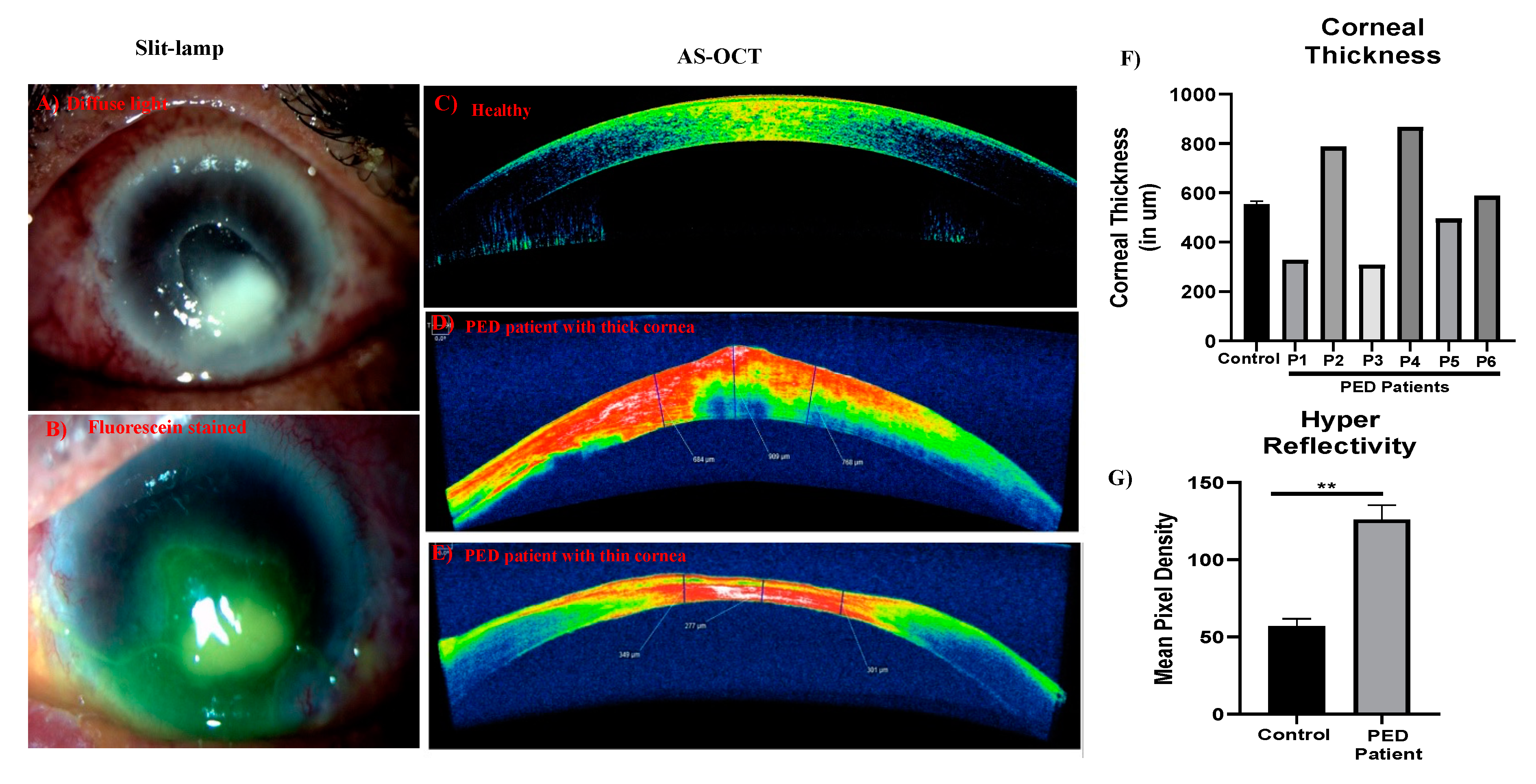
3.1. Ophthalmic and Clinical Evaluations
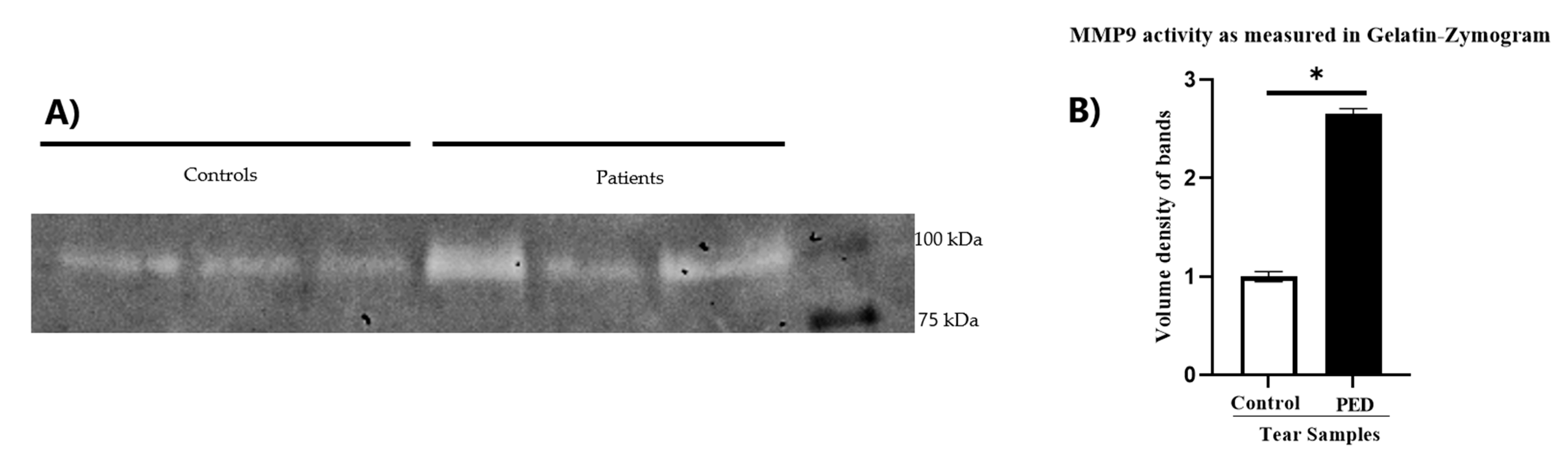
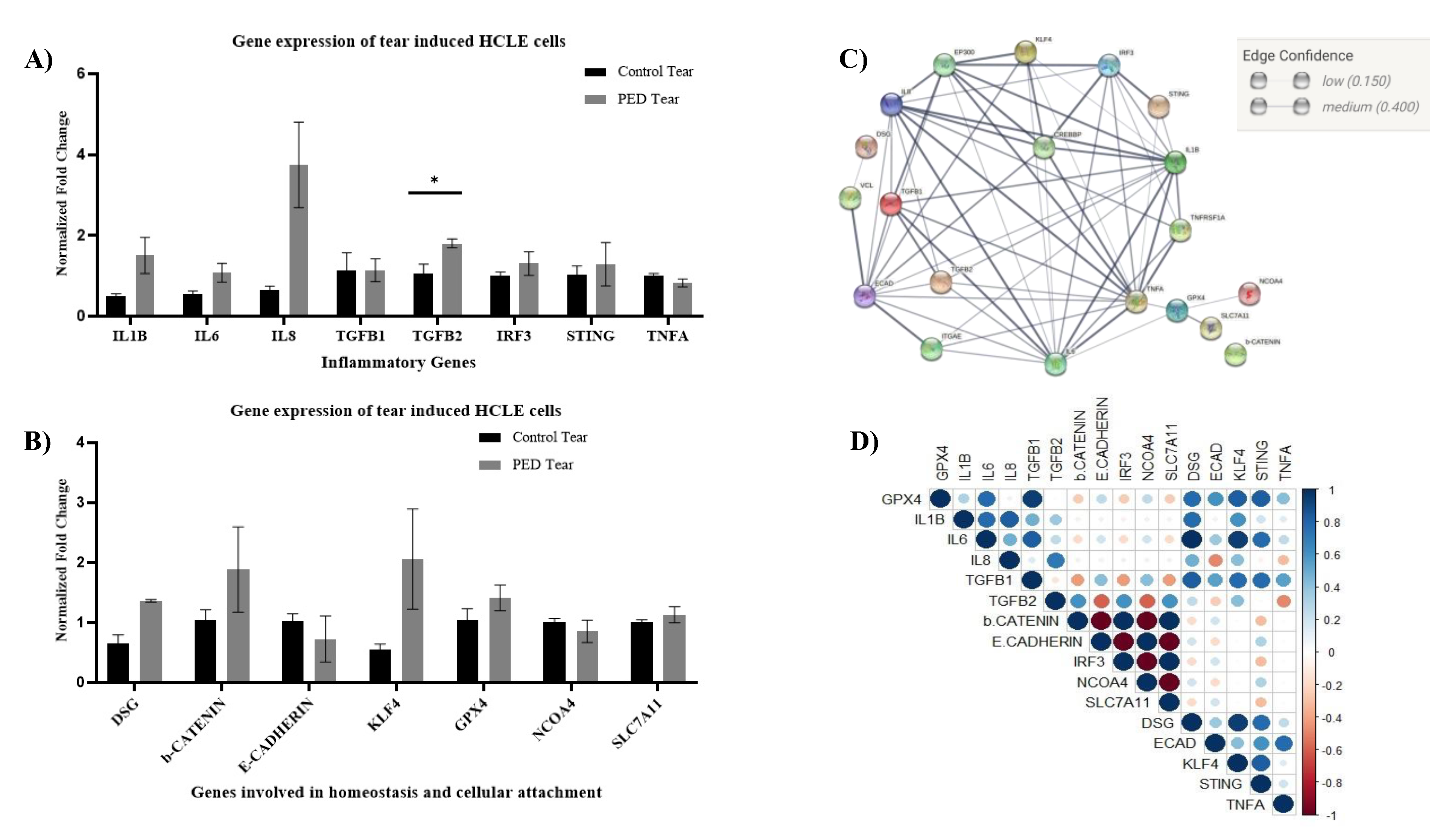
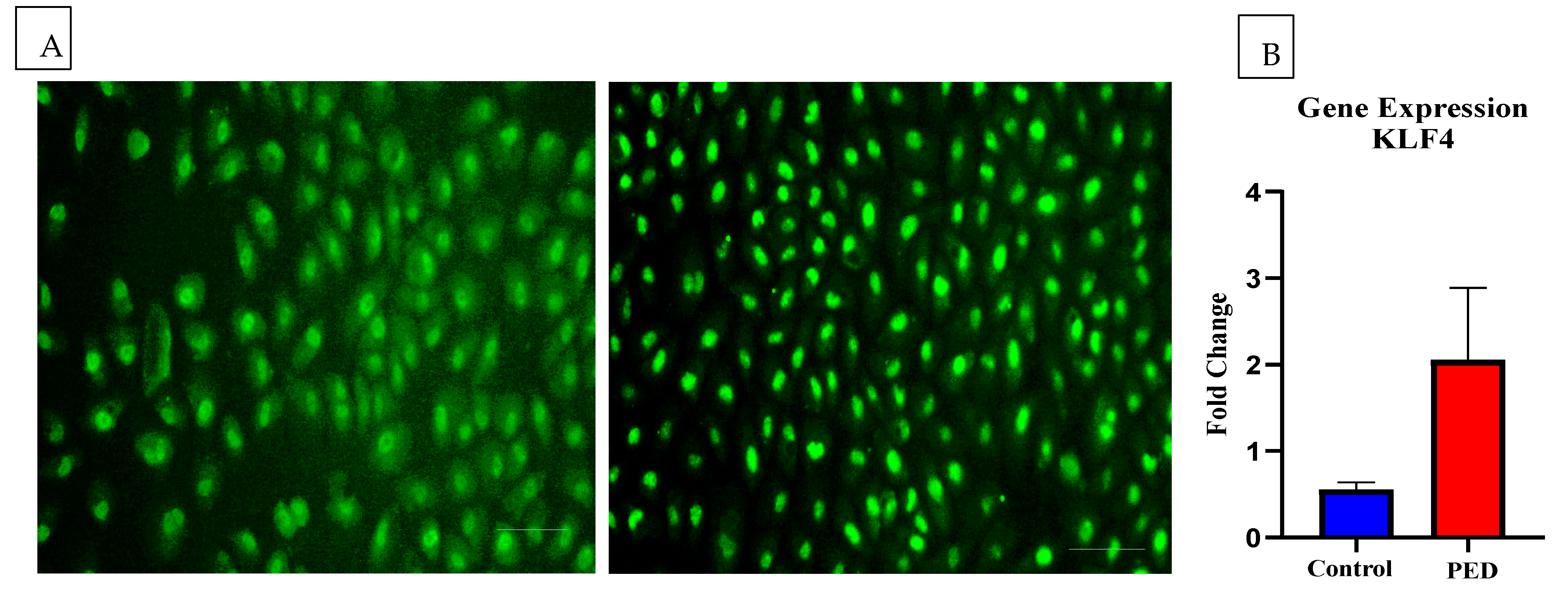
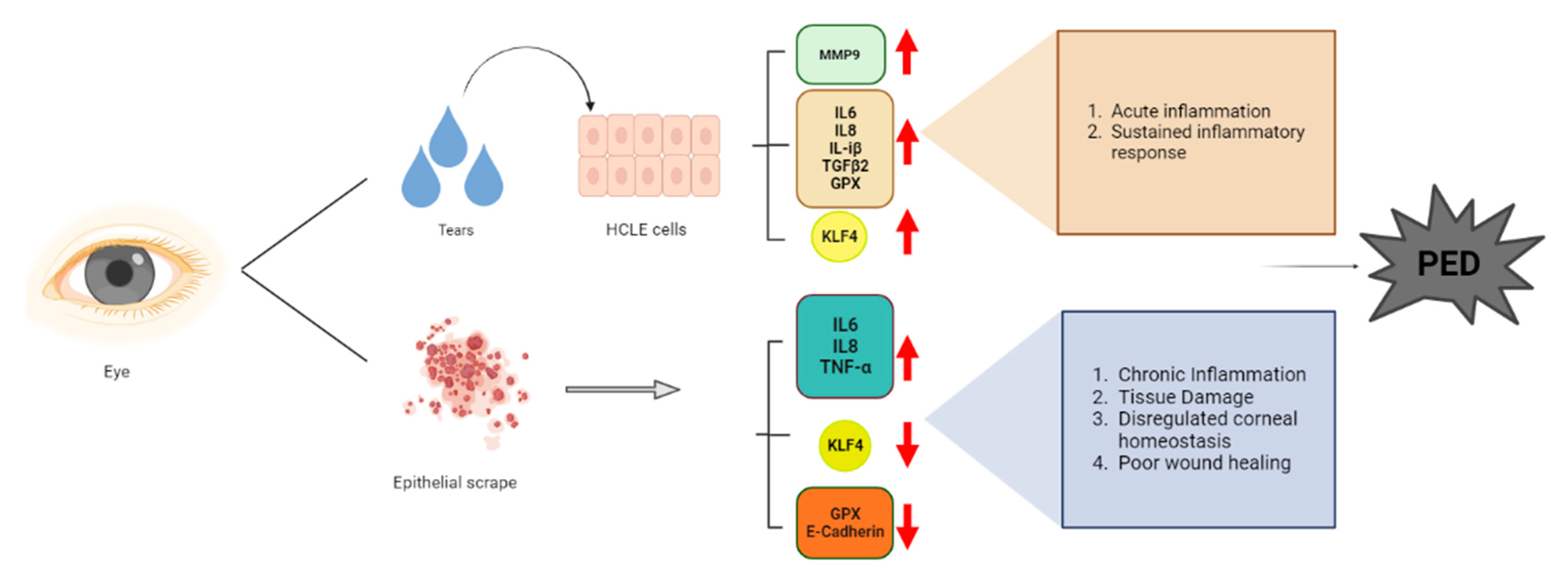
3.2. PED Tears Create an Acute Inflammatory Milieu That Possibly Compromises the CE Homeostasis
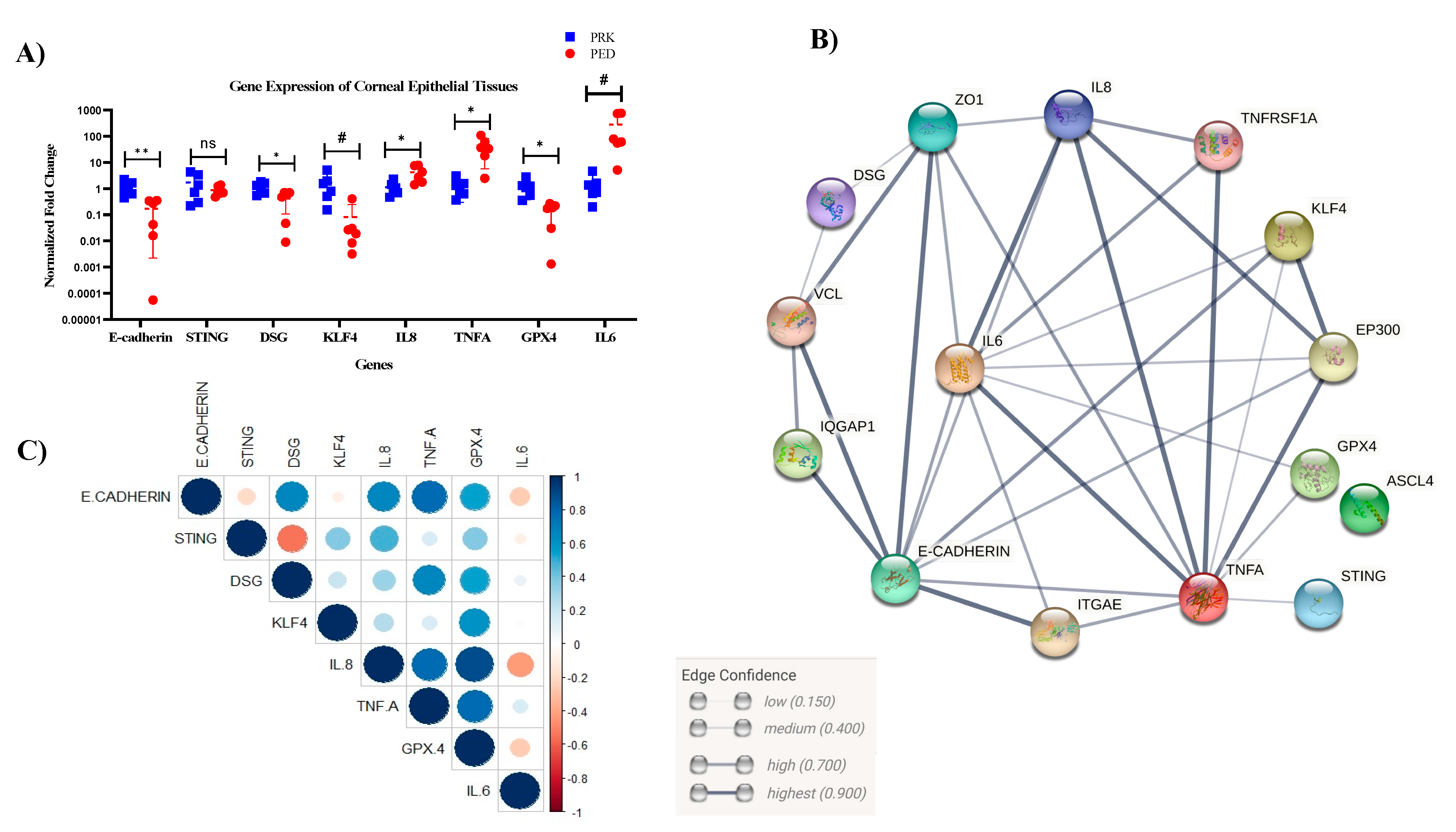
3.3. Epithelial Scrapes of Patients Indicate a Chronic Stage of Inflammation Associated with Compromised CE Homeostasis
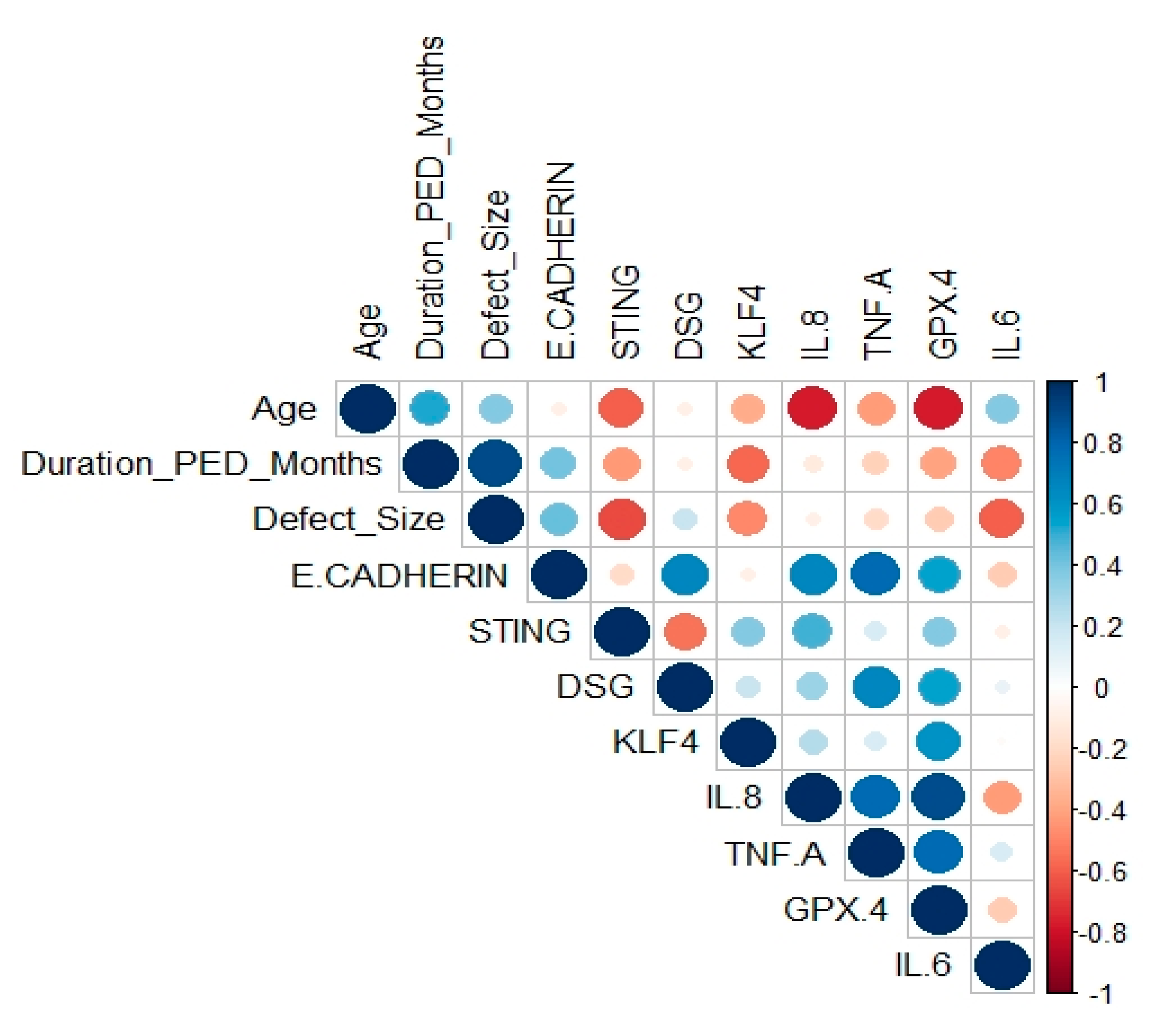
3.4. Correlation of In Vivo Results with Clinical Factors
4. Discussion
Discussion of Correlation Plot
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, T.; Friedman, D.S.; Bradley, C.; Massof, R. Estimates of Incidence and Prevalence of Visual Impairment, Low Vision, and Blindness in the United States. JAMA Ophthalmol. 2018, 136, 12–19. [Google Scholar] [CrossRef]
- Burton, M.J. Prevention, Treatment and Rehabilitation. Community Eye Health 2009, 22, 33–35. [Google Scholar]
- Sridhar, M.S. Anatomy of Cornea and Ocular Surface. Indian J. Ophthalmol. 2018, 66, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Bohm, K.; Rosenblatt, M.; Kang, K. Epigenetic Regulation of Anterior Segment Diseases and Potential Therapeutics. Ocul. Surf. 2020, 18, 383–395. [Google Scholar] [CrossRef]
- Verma, S.; Singh, A.; Varshney, A.; Chandru, R.A.; Acharya, M.; Rajput, J.; Sangwan, V.S.; Tiwari, A.K.; Bhowmick, T.; Tiwari, A. Infectious Keratitis: An Update on Role of Epigenetics. Front. Immunol. 2021, 12, 765890. [Google Scholar] [CrossRef]
- Maurizi, E.; Adamo, D.; Magrelli, F.M.; Galaverni, G.; Attico, E.; Merra, A.; Maffezzoni, M.B.R.; Losi, L.; Genna, V.G.; Sceberras, V.; et al. Regenerative Medicine of Epithelia: Lessons From the Past and Future Goals. Front. Bioeng. Biotechnol. 2021, 9, 652214. [Google Scholar] [CrossRef]
- Vaidyanathan, U.; Hopping, G.C.; Liu, H.Y.; Somani, A.N.; Ronquillo, Y.C.; Hoopes, P.C.; Moshirfar, M. Persistent Corneal Epithelial Defects: A Review Article. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 163–176. [Google Scholar]
- Bandeira, F.; Goh, T.-W.; Setiawan, M.; Yam, G.H.-F.; Mehta, J.S. Cellular Therapy of Corneal Epithelial Defect by Adipose Mesenchymal Stem Cell-Derived Epithelial Progenitors. Stem Cell Res. 2020, 11, 14. [Google Scholar] [CrossRef]
- Wilson, S.E.; Medeiros, C.S.; Santhiago, M.R. Pathophysiology of Corneal Scarring in Persistent Epithelial Defects after PRK and Other Corneal Injuries. J. Refract. Surg. 2018, 34, 59–64. [Google Scholar] [CrossRef]
- Katzman, L.R.; Jeng, B.H. Management Strategies for Persistent Epithelial Defects of the Cornea. Saudi J. Ophthalmol. 2014, 28, 168–172. [Google Scholar] [CrossRef]
- Tiffany, J.M. Tears in Health and Disease. Eye 2003, 17, 923–926. [Google Scholar] [CrossRef] [PubMed]
- Hagan, S.; Martin, E.; Enríquez-de-Salamanca, A. Tear Fluid Biomarkers in Ocular and Systemic Disease: Potential Use for Predictive, Preventive and Personalised Medicine. EPMA J. 2016, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Gipson, I.K.; Spurr-Michaud, S.; Argüeso, P.; Tisdale, A.; Ng, T.F.; Russo, C.L. Mucin Gene Expression in Immortalized Human Corneal-Limbal and Conjunctival Epithelial Cell Lines. Investig. Ophthalmol. Vis. Sci. 2003, 44, 2496–2506. [Google Scholar] [CrossRef]
- Szklarczyk, D.; Gable, A.L.; Lyon, D.; Junge, A.; Wyder, S.; Huerta-Cepas, J.; Simonovic, M.; Doncheva, N.T.; Morris, J.H.; Bork, P.; et al. STRING V11: Protein–Protein Association Networks with Increased Coverage, Supporting Functional Discovery in Genome-Wide Experimental Datasets. Nucleic Acids Res. 2019, 47, D607–D613. [Google Scholar] [CrossRef]
- Yabluchanskiy, A.; Ma, Y.; Iyer, R.P.; Hall, M.E.; Lindsey, M.L. Matrix Metalloproteinase-9: Many Shades of Function in Cardiovascular Disease. Physiology 2013, 28, 391–403. [Google Scholar] [CrossRef]
- GILL, S.; PARKS, W. Metalloproteinases and Their Inhibitors: Regulators of Wound Healing. Int. J. Biochem. Cell Biol. 2008, 40, 1334–1347. [Google Scholar] [CrossRef]
- Burbach, G.J.; Naik, S.M.; Harten, J.B.; Liu, L.; Dithmar, S.; Grossniklaus, H.; Ward, S.L.; Armstrong, C.A.; Caughman, S.W.; Ansel, J.C. Interleukin-18 expression and modulation in human corneal epithelial cells. Curr. Eye Res. 2001, 23, 64–68. [Google Scholar] [CrossRef]
- Fong, P.Y.; Shih, K.C.; Lam, P.Y.; Chan, T.C.Y.; Jhanji, V.; Tong, L. Role of Tear Film Biomarkers in the Diagnosis and Management of Dry Eye Disease. Taiwan J. Ophthalmol. 2019, 9, 150–159. [Google Scholar] [CrossRef]
- Janus, J.; Guzek, J.W. The Vasopressin Content in the Neurohypophysis under Conditions of Intracerebroventricular Beta-Adrenergic Blockade in Euhydrated and Dehydrated Rats. Acta Physiol. Pol. 1987, 38, 402–409. [Google Scholar]
- Jindatanmanusan, P.; Luanraksa, S.; Boonsiri, T.; Nimmanon, T.; Arnutti, P. Wound Fluid Matrix Metalloproteinase-9 as a Potential Predictive Marker for the Poor Healing Outcome in Diabetic Foot Ulcers. Pathol. Res. Int. 2018, 2018, 1631325. [Google Scholar] [CrossRef]
- Tiwari, A.; Swamynathan, S.; Alexander, N.; Gnalian, J.; Tian, S.; Kinchington, P.R.; Swamynathan, S.K. KLF4 Regulates Corneal Epithelial Cell Cycle Progression by Suppressing Canonical TGF-β Signaling and Upregulating CDK Inhibitors P16 and P27. Investig. Ophthalmol. Vis. Sci. 2019, 60, 731–740. [Google Scholar] [CrossRef]
- Tiwari, A.; Swamynathan, S.; Jhanji, V.; Swamynathan, S.K. KLF4 Coordinates Corneal Epithelial Apical-Basal Polarity and Plane of Cell Division and Is Downregulated in Ocular Surface Squamous Neoplasia. Investig. Ophthalmol. Vis. Sci. 2020, 61, 15. [Google Scholar] [CrossRef]
- Choi, H.; Roh, J. Role of Klf4 in the Regulation of Apoptosis and Cell Cycle in Rat Granulosa Cells during the Periovulatory Period. Int. J. Mol. Sci. 2018, 20, 87. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.Z.; Stevenson, A.W.; Prêle, C.M.; Fear, M.W.; Wood, F.M. The Role of IL-6 in Skin Fibrosis and Cutaneous Wound Healing. Biomedicines 2020, 8, 101. [Google Scholar] [CrossRef]
- Wagner, J.A. Is IL-6 Both a Cytokine and a Neurotrophic Factor? J. Exp. Med. 1996, 183, 2417–2419. [Google Scholar] [CrossRef]
- Baker, M.; Noisakran, S.; Gebhardt, B.M.; Kriesel, J.D.; Carr, D.J. The Relationship between Interleukin-6 and Herpes Simplex Virus Type 1: Implications for Behavior and Immunopathology. Brain Behav. Immun. 1999, 13, 201–211. [Google Scholar] [CrossRef]
- Paludan, S.R. Requirements for the Induction of Interleukin-6 by Herpes Simplex Virus-Infected Leukocytes. J. Virol. 2001, 75, 8008–8015. [Google Scholar] [CrossRef]
- Tiwari, A.; Loughner, C.L.; Swamynathan, S.; Swamynathan, S.K. KLF4 Plays an Essential Role in Corneal Epithelial Homeostasis by Promoting Epithelial Cell Fate and Suppressing Epithelial-Mesenchymal Transition. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2785–2795. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Age | Sex | Clinical Diagnosis | Penetrating Keratoplasty (PK) Status | Duration PED Months | Defect Size (mm2) |
|---|---|---|---|---|---|---|
| PED1 | 66 | M | HSV | POST-PK | 1 | 2 |
| PED2 | 44 | M | HSV | POST-PK | 2 | 6 |
| PED3 | 40 | M | HSV | POST PK | 1 | 12 |
| PED4 | 70 | M | HSV | NO | 10 | 49 |
| PED5 | 65 | M | PSEUDOMONAS | POST PK | 4 | 36 |
| PED6 | 78 | F | PSEUDOMONAS | NO | 3 | 35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dutta, T.; Sangwan, J.; Mondal, M.; Vohra, M.; Nidhi, V.; Gour, A.; Kapur, N.; Gupta, N.; Bhowmick, T.; Chandru, A.; et al. Prolonged Inflammation and Infectious Changes in the Corneal Epithelium Are Associated with Persistent Epithelial Defect (PED). Pathogens 2023, 12, 261. https://doi.org/10.3390/pathogens12020261
Dutta T, Sangwan J, Mondal M, Vohra M, Nidhi V, Gour A, Kapur N, Gupta N, Bhowmick T, Chandru A, et al. Prolonged Inflammation and Infectious Changes in the Corneal Epithelium Are Associated with Persistent Epithelial Defect (PED). Pathogens. 2023; 12(2):261. https://doi.org/10.3390/pathogens12020261
Chicago/Turabian StyleDutta, Tanmoy, Jyoti Sangwan, Moumita Mondal, Mehak Vohra, Vatsala Nidhi, Abha Gour, Neha Kapur, Nidhi Gupta, Tuhin Bhowmick, Arun Chandru, and et al. 2023. "Prolonged Inflammation and Infectious Changes in the Corneal Epithelium Are Associated with Persistent Epithelial Defect (PED)" Pathogens 12, no. 2: 261. https://doi.org/10.3390/pathogens12020261
APA StyleDutta, T., Sangwan, J., Mondal, M., Vohra, M., Nidhi, V., Gour, A., Kapur, N., Gupta, N., Bhowmick, T., Chandru, A., Mathur, U., Sangwan, V. S., Acharya, M., & Tiwari, A. (2023). Prolonged Inflammation and Infectious Changes in the Corneal Epithelium Are Associated with Persistent Epithelial Defect (PED). Pathogens, 12(2), 261. https://doi.org/10.3390/pathogens12020261