
Risk Factors for Cytomegalovirus Infection and Its Impact on Survival after Living Donor Liver Transplantation in South Korea: A Nested Case-Control Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
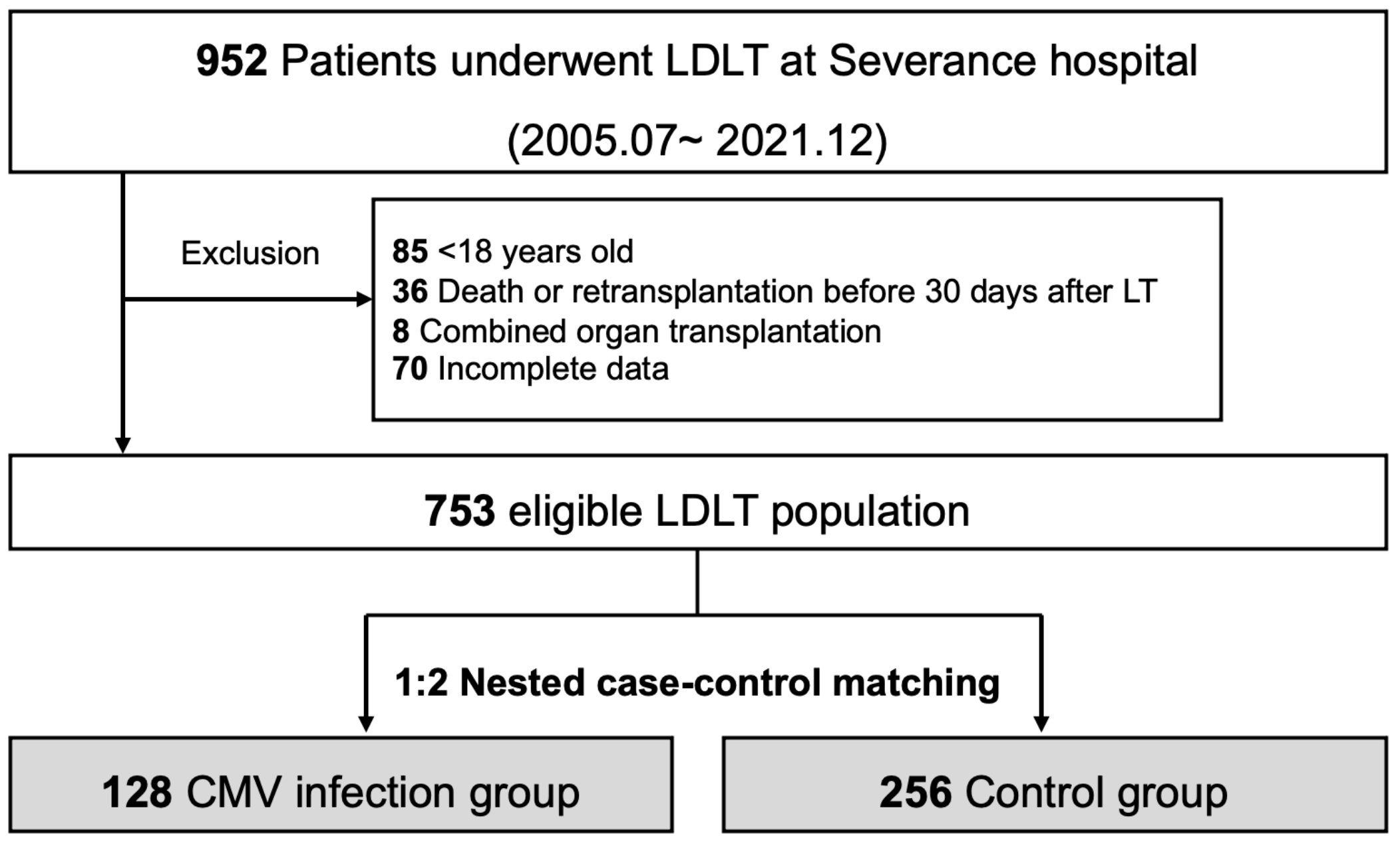
2.1. Study Material
2.2. Screening and Management of CMV Infection
2.3. Nested Case-Control Study
2.4. Statistical Methods
3. Results
3.1. Incidence of CMV Infection in Entire Patients
3.2. Baseline Characteristics of Matched Case-Control Patients
3.3. Pretransplant Blood Tests and Immunosuppression
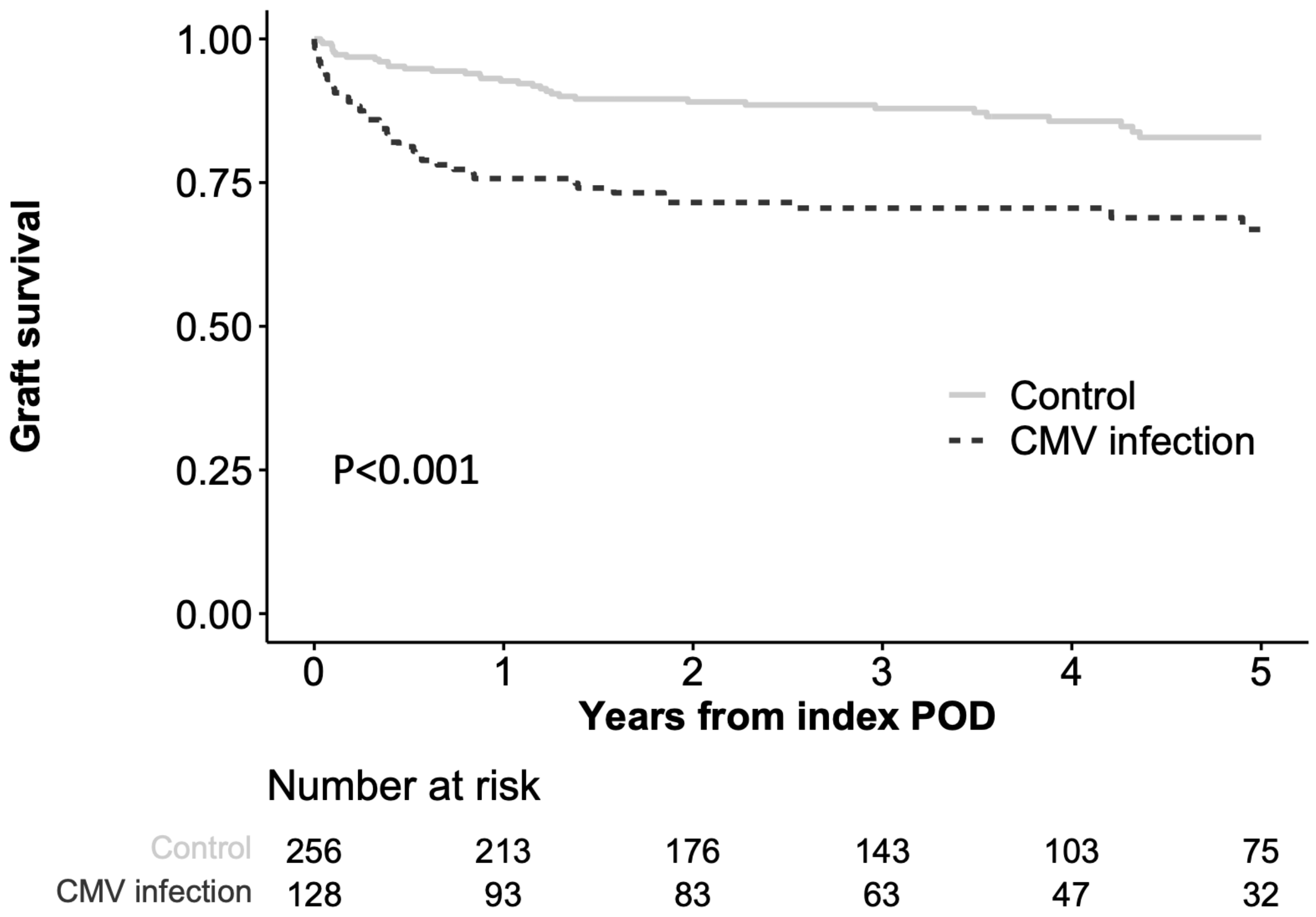
3.4. CMV Infection, CMV Disease and Graft Survival
3.5. Risk Factors for CMV Infection after LDLT
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| CMV | Cytomegalovirus |
| CI | Confidence interval |
| DDLT | Deceased donor liver transplantation |
| HCC | Hepatocellular carcinoma |
| HR | Hazard ratio |
| IQR | Interquartile range |
| LT | Liver transplantation |
| LDLT | Living donor liver transplantation |
| MELD | Model for end-stage liver disease |
| OR | Odds ratio |
| PCR | Polymerase chain reaction |
References
- Kotton, C.N. CMV: Prevention, Diagnosis and Therapy. Am. J. Transplant. 2013, 13 (Suppl. 3), 24–40; quiz 40. [Google Scholar] [CrossRef]
- Atabani, S.F.; Smith, C.; Atkinson, C.; Aldridge, R.W.; Rodriguez-Perálvarez, M.; Rolando, N.; Harber, M.; Jones, G.; O’Riordan, A.; Burroughs, A.K.; et al. Cytomegalovirus replication kinetics in solid organ transplant recipients managed by preemptive therapy. Am. J. Transplant. 2012, 12, 2457–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gane, E.; Saliba, F.; Valdecasas, G.J.; O’Grady, J.; Pescovitz, M.D.; Lyman, S.; Robinson, C.A. Randomised trial of efficacy and safety of oral ganciclovir in the prevention of cytomegalovirus disease in liver-transplant recipients. The Oral Ganciclovir International Transplantation Study Group [corrected]. Lancet 1997, 350, 1729–1733. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kim, S.J.; Joh, J.W.; Kwon, C.H.; Song, S.; Shin, M.; Moon, J.I.; Kim, G.S.; Hong, S.H.; Lee, S.K. Is cytomegalovirus infection dangerous in cytomegalovirus-seropositive recipients after liver transplantation? Liver Transplant. 2011, 17, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Kotton, C.N.; Kumar, D.; Caliendo, A.M.; Huprikar, S.; Chou, S.; Danziger-Isakov, L.; Humar, A.; The Transplantation Society International CMV Consensus Group. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation 2018, 102, 900–931. [Google Scholar] [CrossRef] [Green Version]
- Bhugra, A.; Khodare, A.; Agarwal, R.; Pamecha, V.; Gupta, E. Role of cytomegalovirus specific cell-mediated immunity in the monitoring of cytomegalovirus infection among living donor liver transplantation adult recipients: A single-center experience. Transpl. Infect. Dis. 2023, 25, e14011. [Google Scholar] [CrossRef]
- Wadhawan, M.; Gupta, S.; Goyal, N.; Vasudevan, K.R.; Makki, K.; Dawar, R.; Sardana, R.; Lal, N.; Kumar, A. Cytomegalovirus infection: Its incidence and management in cytomegalovirus-seropositive living related liver transplant recipients: A single-center experience. Liver Transpl. 2012, 18, 1448–1455. [Google Scholar] [CrossRef]
- Yadav, S.K.; Saigal, S.; Choudhary, N.S.; Saha, S.; Sah, J.K.; Saraf, N.; Kumar, N.; Goja, S.; Rastogi, A.; Bhangui, P.; et al. Cytomegalovirus infection in living donor liver transplant recipients significantly impacts the early post-transplant outcome: A single center experience. Transpl. Infect. Dis. 2018, 20, e12905. [Google Scholar] [CrossRef]
- Ljungman, P.; Boeckh, M.; Hirsch, H.H.; Josephson, F.; Lundgren, J.; Nichols, G.; Pikis, A.; Razonable, R.R.; Miller, V.; Griffiths, P.D. Definitions of cytomegalovirus infection and disease in transplant patients for use in clinical trials. Clin. Infect. Dis. 2016, 64, 87–91. [Google Scholar]
- Kim, J.M.; Kim, D.G.; Kim, J.; Lee, K.; Lee, K.W.; Ryu, J.H.; Kim, B.W.; Choi, D.L.; You, Y.K.; Kim, D.S.; et al. Outcomes after liver transplantation in Korea: Incidence and risk factors from Korean transplantation registry. Clin. Mol. Hepatol. 2021, 27, 451–462. [Google Scholar] [CrossRef]
- Samstein, B.; Smith, A.R.; Freise, C.E.; Zimmerman, M.A.; Baker, T.; Olthoff, K.M.; Fisher, R.A.; Merion, R.M. Complications and Their Resolution in Recipients of Deceased and Living Donor Liver Transplants: Findings from the A2ALL Cohort Study. Am. J. Transplant. 2016, 16, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Onor, I.O.; Todd, S.B.; Meredith, E.; Perez, S.D.; Mehta, A.K.; Marshall Lyon, G.; Knechtle, S.J.; Hanish, S.I. Evaluation of clinical outcomes of prophylactic versus preemptive cytomegalovirus strategy in liver transplant recipients. Transpl. Int. 2013, 26, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Owers, D.S.; Webster, A.C.; Strippoli, G.F.; Kable, K.; Hodson, E.M. Pre-emptive treatment for cytomegalovirus viraemia to prevent cytomegalovirus disease in solid organ transplant recipients. Cochrane Database Syst. Rev. 2013, 2013, CD005133. [Google Scholar] [CrossRef]
- Florescu, D.F.; Qiu, F.; Schmidt, C.M.; Kalil, A.C. A direct and indirect comparison meta-analysis on the efficacy of cytomegalovirus preventive strategies in solid organ transplant. Clin. Infect. Dis. 2014, 58, 785–803. [Google Scholar] [CrossRef] [Green Version]
- Mumtaz, K.; Faisal, N.; Husain, S.; Morillo, A.; Renner, E.; Shah, P. Universal prophylaxis or preemptive strategy for cytomegalovirus disease after liver transplantation: A systematic review and meta-analysis. Am. J. Transplant. 2015, 15, 472–481. [Google Scholar] [CrossRef]
- Tookey, P.A.; Ades, A.E.; Peckham, C.S. Cytomegalovirus prevalence in pregnant women: The influence of parity. Arch. Dis. Child. 1992, 67, 779–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pembrey, L.; Raynor, P.; Griffiths, P.; Chaytor, S.; Wright, J.; Hall, A.J. Seroprevalence of cytomegalovirus, Epstein Barr virus and varicella zoster virus among pregnant women in Bradford: A cohort study. PLoS ONE 2013, 8, e81881. [Google Scholar] [CrossRef] [Green Version]
- Busch, C.J.; Siegler, B.H.; Werle, H.; Lichtenstern, C.; Bruckner, T.; Heininger, A.; Mehrabi, A.; Weiss, K.H.; Weigand, M.A.; Hochreiter, M. Risk factors for early viral infections after liver transplantation. Langenbeck’s Arch. Surg. 2018, 403, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kwon, C.H.D.; Joh, J.-W.; Kang, E.-S.; Park, J.B.; Lee, J.H.; Kim, S.J.; Paik, S.W.; Lee, S.-K.; Kim, D.W. ABO-incompatible living donor liver transplantation is suitable in patients without ABO-matched donor. J. Hepatol. 2013, 59, 1215–1222. [Google Scholar] [CrossRef]
- Egawa, H.; Teramukai, S.; Haga, H.; Tanabe, M.; Fukushima, M.; Shimazu, M. Present status of ABO-incompatible living donor liver transplantation in Japan. Hepatology 2008, 47, 143–152. [Google Scholar] [CrossRef]
- Song, G.-W.; Lee, S.-G.; Hwang, S.; Kim, K.-H.; Ahn, C.-S.; Moon, D.-B.; Ha, T.-Y.; Jung, D.-H.; Park, G.-C.; Kang, S.-H. Biliary stricture is the only concern in ABO-incompatible adult living donor liver transplantation in the rituximab era. J. Hepatol. 2014, 61, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Andrassy, J.; Hoffmann, V.S.; Rentsch, M.; Stangl, M.; Habicht, A.; Meiser, B.; Fischereder, M.; Jauch, K.-W.; Guba, M. Is cytomegalovirus prophylaxis dispensable in patients receiving an mTOR inhibitor–based immunosuppression? A systematic review and meta-analysis. Transplantation 2012, 94, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Tam, N.; Deng, R.; Chen, P.; Li, H.; Wu, L. Everolimus-based calcineurin-inhibitor sparing regimens for kidney transplant recipients: A systematic review and meta-analysis. Int. Urol. Nephrol. 2014, 46, 2035–2044. [Google Scholar] [CrossRef]
- Sheng, L.; Jun, S.; Jianfeng, L.; Lianghui, G. The effect of sirolimus-based immunosuppression vs. conventional prophylaxis therapy on cytomegalovirus infection after liver transplantation. Clin. Transplant. 2015, 29, 555–559. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | CMV Infection (n = 128) | Control (n = 256) | p |
|---|---|---|---|
| Age | 54 (49–61) | 55 (51–61) | 0.144 |
| Sex, female | 51 (39.8) | 57 (22.3) | <0.001 |
| BMI, kg/m2 | 23.6 (21.5–25.4) | 23.7 (22.2–25.9) | 0.126 |
| Year of LT | 1.000 | ||
| 2012–2015 | 33 (25.8) | 66 (25.8) | |
| 2016–2018 | 70 (54.7) | 140 (54.7) | |
| 2019–2021 | 25 (19.5) | 50 (19.5) | |
| Hypertension | 31 (24.2) | 51 (19.9) | 0.403 |
| Diabetes mellitus | 42 (32.8) | 82 (32.0) | 0.969 |
| Cardiovascular disease | 11 (8.6) | 14 (5.5) | 0.342 |
| Underlying liver disease | 0.005 | ||
| Viral | 63 (49.2) | 156 (60.9) | |
| Alcoholic | 29 (22.7) | 63 (24.6) | |
| Others | 36 (28.1) | 37 (14.5) | |
| HCC | 53 (41.4) | 165 (64.5) | <0.001 |
| Pretransplant MELD | 15 (10–25) | 11 (8–15.0) | <0.001 |
| Pretransplant stay | <0.001 | ||
| Out-patient day | 66 (51.6) | 180 (70.6) | |
| In-hospital | 62 (48.4) | 76 (29.4) | |
| Refractory ascites | 10 (7.8) | 25 (9.8) | 0.661 |
| Severe encephalopathy | 26 (20.3) | 27 (10.5) | 0.014 |
| Re-transplantation | 1 (0.8) | 0 (0.0) | 0.723 |
| ABO incompatibility | 44 (34.4) | 57 (22.3) | 0.016 |
| Donor age | 33 (26–43) | 32 (25–41) | 0.476 |
| Donor sex, female | 43 (33.6) | 96 (37.5) | 0.523 |
| Donor BMI | 23.0 ± 2.6 | 22.9 ± 2.4 | 0.964 |
| Macrovesicular steatosis (≥10) | 30 (23.4) | 39 (15.2) | 0.067 |
| Operation time, min | 646 (565–730) | 652 (543–720) | 0.885 |
| Transfusion of RBC, pack | 4 (2–8) | 3 (1–6) | 0.013 |
| Re-operation before index POD | 16 (12.5) | 16 (6.2) | 0.058 |
| CMV antibody status | 0.539 | ||
| R+ | 128 (100) | 253 (98.8) | |
| R-D+ | 0 | 3 (1.2) | |
| Acute cellular rejection | 34 (26.6) | 67 (26.2) | 1.000 |
| Variables | CMV Infection (n = 128) | Control (n = 256) | p |
|---|---|---|---|
| White blood cell, 103/μL | 4.5 (2.9–6.4) | 3.4 (2.6–4.6) | <0.001 |
| Neutrophil, 103/μL | 3.1 (1.8–4.7) | 2.1 (1.5–3.2) | <0.001 |
| Lymphocyte, 103/μL | 0.6 (0.4–1.0) | 0.7 (0.5–1.0) | 0.077 |
| Hemoglobin, g/dL | 10.6 (8.9–12.0) | 10.9 (9.2–12.5) | 0.116 |
| Platelet, 103/μL | 69 (51–108) | 72 (52–108) | 0.825 |
| Albumin, g/dL | 3.2 ± 0.5 | 3.2 ± 0.6 | 0.449 |
| Glucose, mg/dL | 119 (92–158) | 105 (90–137) | 0.046 |
| Creatinine, mg/dL | 0.7 (0.6–1.1) | 0.7 (0.6–0.9) | 0.481 |
| Use of immunosuppressants a | |||
| TAC | 127 (99.2) | 252 (98.4) | 0.874 |
| Mycophenolate mofetil | 82 (64.1) | 165 (64.5) | 1.000 |
| mTOR inhibitor | 10 (7.8) | 25 (9.8) | 0.661 |
| Steroid | 122 (95.3) | 244 (95.3) | 1.000 |
| Mean TAC trough level, ng/dL b | 7.3 (5.5–8.7) | 7.2 (5.7–9.0) | 0.846 |
| Maximum TAC trough level, ng/dL b | 13.6 (9.2–17.6) | 11.9 (8.8–16.9) | 0.333 |
| Univariable a | Multivariable b | |||
|---|---|---|---|---|
| Variables | OR (95 CI) | p | OR (95 CI) | p |
| Age | 0.98 (0.95–1.00) | 0.084 | 0.98 (0.95, 1.01) | 0.175 |
| Sex, female | 2.31 (1.46–3.67) | 0.001 | 2.40 (1.35, 4.28) | 0.003 |
| Pretransplant MELD | 1.09 (1.06–1.12) | 0.001 | 1.06 (1.02, 1.11) | 0.004 |
| Pretransplant stay (vs. Out-patient day) | ||||
| In-hospital | 2.15 (1.38–3.36) | 0.001 | 1.83 (1.06, 3.17) | 0.030 |
| Severe encephalopathy | 2.16 (1.20–3.90) | 0.010 | 1.06 (0.47, 2.33) | 0.882 |
| ABO incompatibility | 1.83 (1.14–2.92) | 0.012 | 2.10 (1.21, 3.67) | 0.009 |
| Macrovesicular steatosis, ≥10% | 1.70 (1.00–2.90) | 0.050 | 2.01 (1.07, 3.77) | 0.030 |
| Transfusion of RBC, pack | 1.03 (1.00–1.07) | 0.043 | 1.01 (0.97, 1.05) | 0.672 |
| Re-operation before index POD | 2.14 (1.03–4.47) | 0.040 | 2.51 (1.06, 5.94) | 0.035 |
| Creatinine, mg/dL | 1.71 (1.16–2.78) | 0.017 | 1.45 (0.94, 2.51) | 0.141 |
| Glucose, mg/dL | 1.00 (1.00–1.01) | 0.077 | 1.00 (1.00, 1.01) | 0.130 |
| White blood cell, 103/μL | 1.18 (1.09–1.29) | 0.001 | 0.95 (0.72, 1.26) | 0.737 |
| Neutrophil, 103/μL | 1.24 (1.13–1.38) | 0.001 | 1.15 (0.84, 1.59) | 0.384 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yim, S.H.; Choi, M.C.; Kim, D.-G.; Min, E.-K.; Lee, J.G.; Joo, D.J.; Kim, M.S. Risk Factors for Cytomegalovirus Infection and Its Impact on Survival after Living Donor Liver Transplantation in South Korea: A Nested Case-Control Study. Pathogens 2023, 12, 521. https://doi.org/10.3390/pathogens12040521
Yim SH, Choi MC, Kim D-G, Min E-K, Lee JG, Joo DJ, Kim MS. Risk Factors for Cytomegalovirus Infection and Its Impact on Survival after Living Donor Liver Transplantation in South Korea: A Nested Case-Control Study. Pathogens. 2023; 12(4):521. https://doi.org/10.3390/pathogens12040521
Chicago/Turabian StyleYim, Seung Hyuk, Mun Chae Choi, Deok-Gie Kim, Eun-Ki Min, Jae Geun Lee, Dong Jin Joo, and Myoung Soo Kim. 2023. "Risk Factors for Cytomegalovirus Infection and Its Impact on Survival after Living Donor Liver Transplantation in South Korea: A Nested Case-Control Study" Pathogens 12, no. 4: 521. https://doi.org/10.3390/pathogens12040521
APA StyleYim, S. H., Choi, M. C., Kim, D. -G., Min, E. -K., Lee, J. G., Joo, D. J., & Kim, M. S. (2023). Risk Factors for Cytomegalovirus Infection and Its Impact on Survival after Living Donor Liver Transplantation in South Korea: A Nested Case-Control Study. Pathogens, 12(4), 521. https://doi.org/10.3390/pathogens12040521