
Enhancing Insights into Australia’s Gonococcal Surveillance Programme through Stochastic Modelling


Abstract
:1. Introduction
2. Materials and Methods
2.1. Core Methodology for Scenario Tree Building
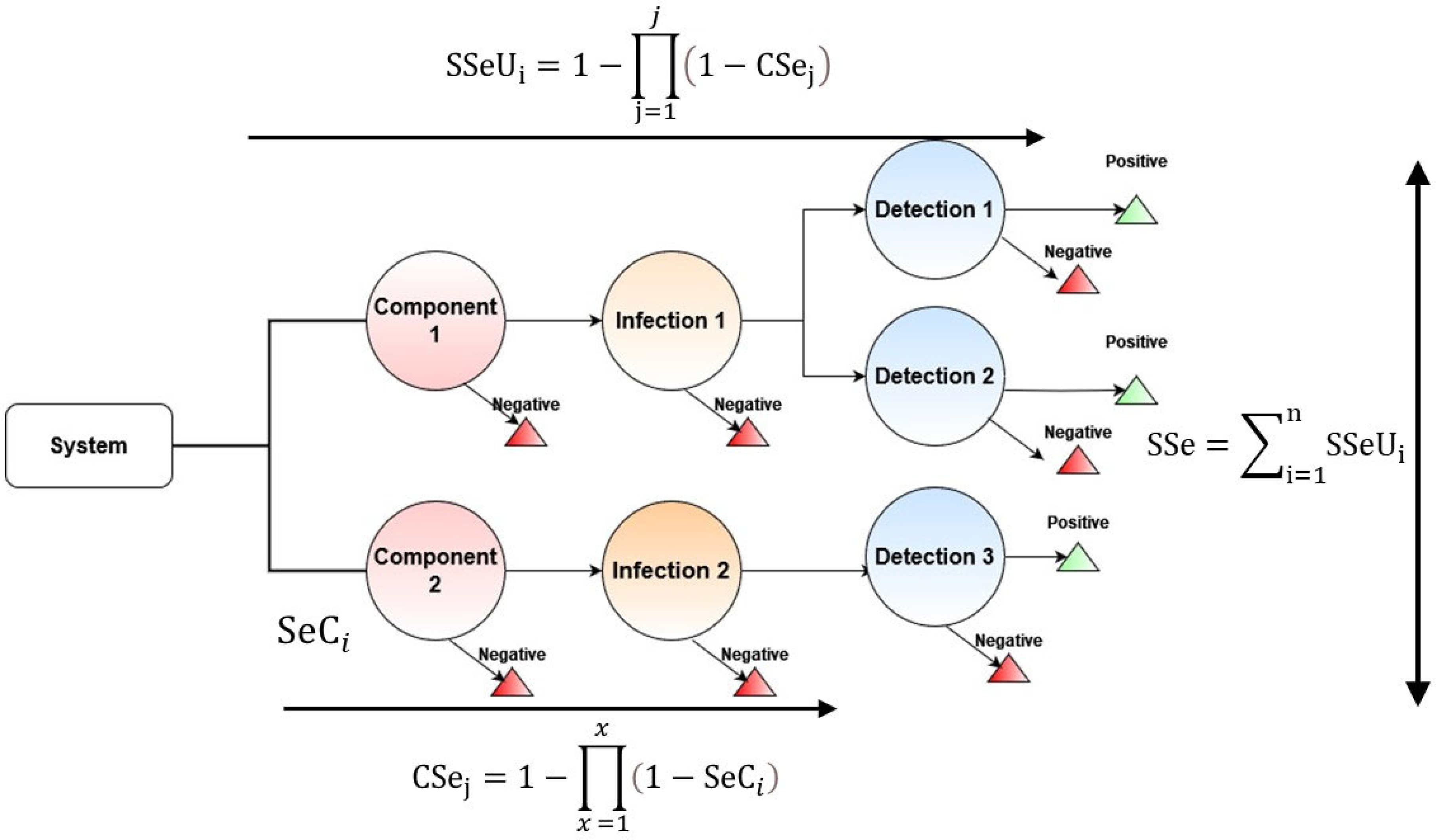
2.1.1. Modified Scenario Tree Modelling Methodology and Structure
2.1.2. Collection of Data for Parameters
2.2. Parameterisation of Inputs for the Scenario Tree Model
2.3. Implementation of the Scenario Tree Model
2.3.1. Core Assumptions of the Model
2.3.2. Model Outputs
2.3.3. Simulation of the Model
2.4. Modifications to Core Scenario Tree Modelling Methodology
2.5. Sensitivity Analysis of the Scenario Tree Model
3. Results
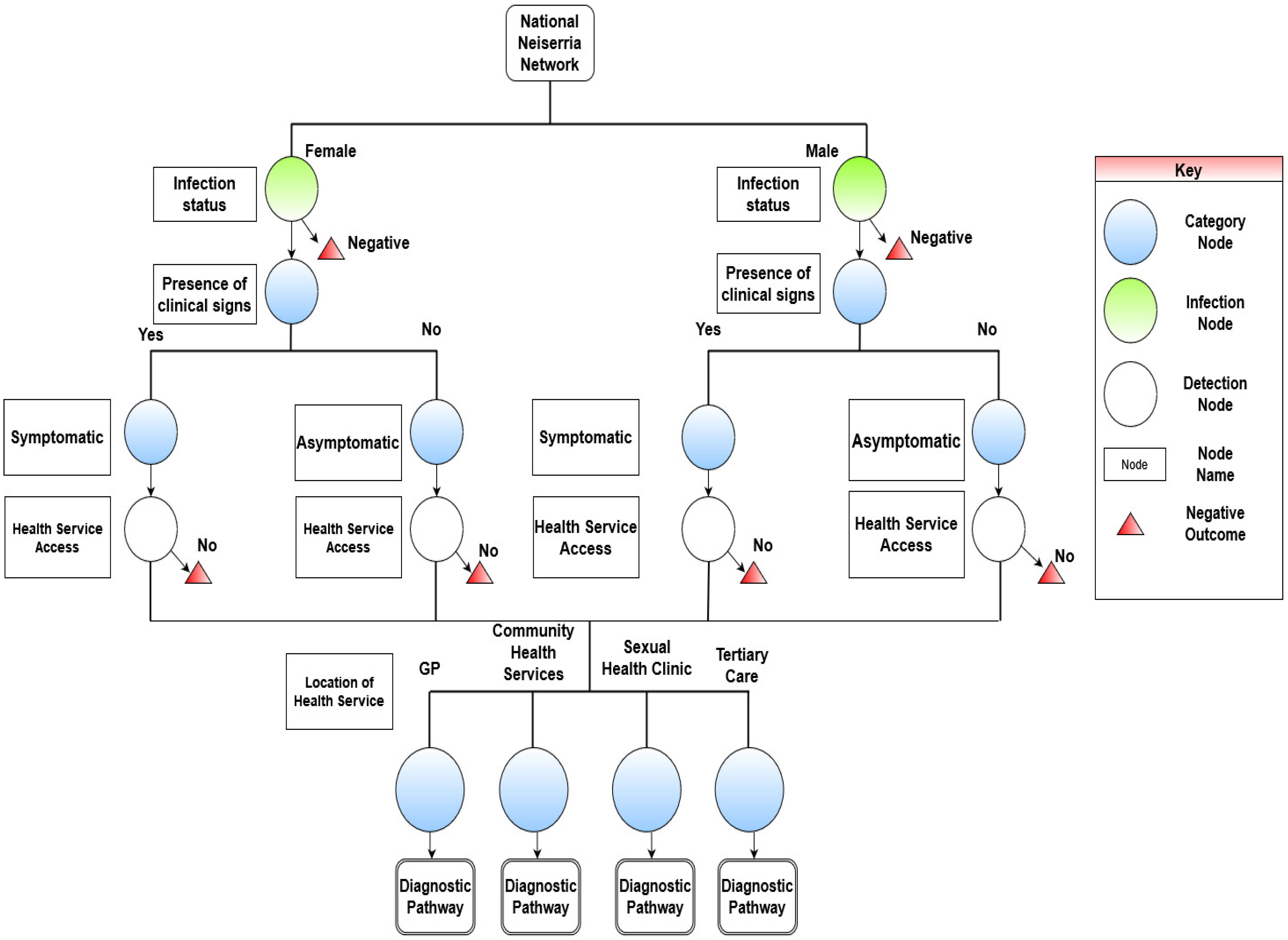
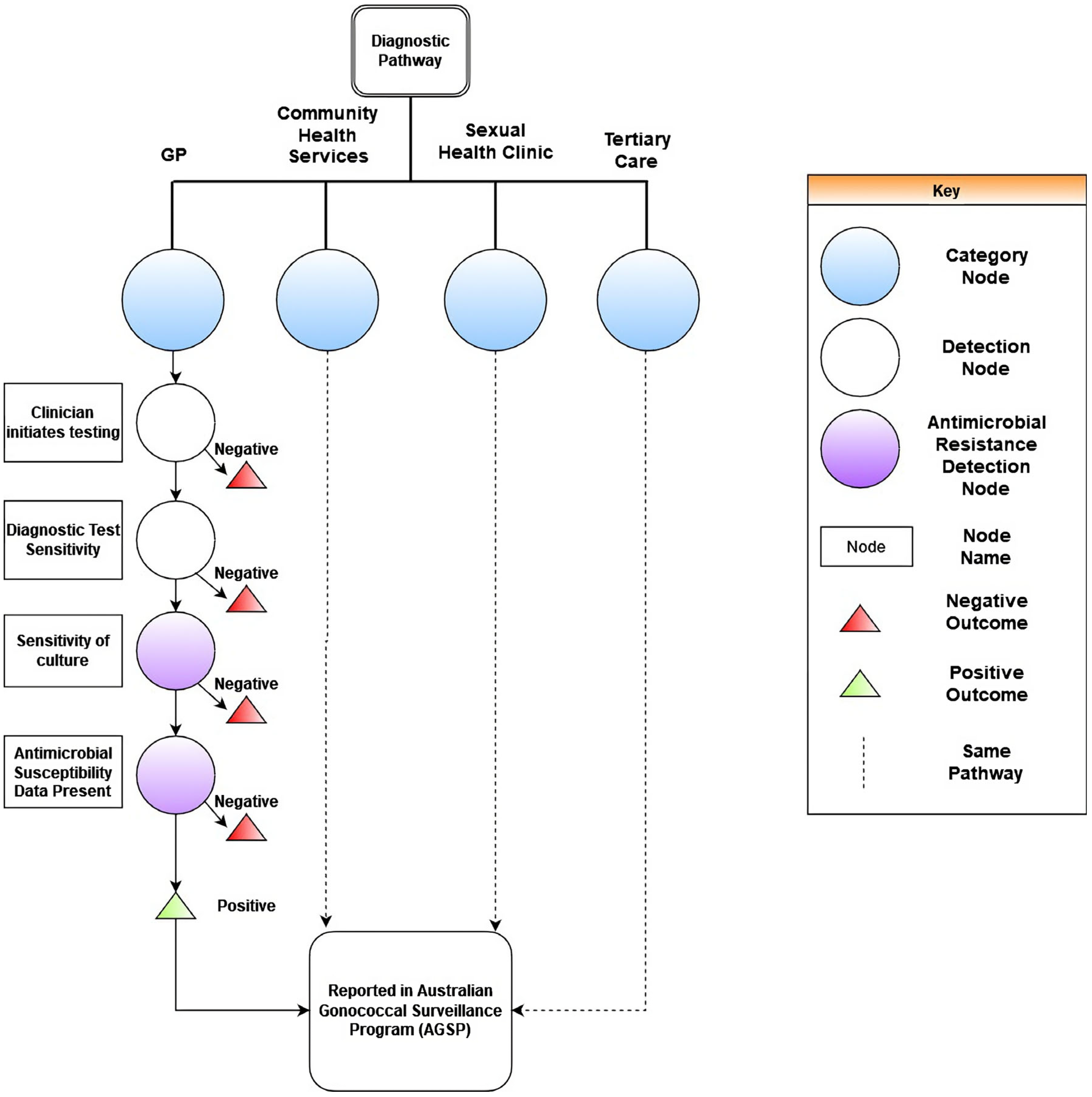
3.1. Scenario Tree Model for the Surveillance System
3.2. Scenario Tree Model Outputs from the Australian Gonococcal Surveillance Programme
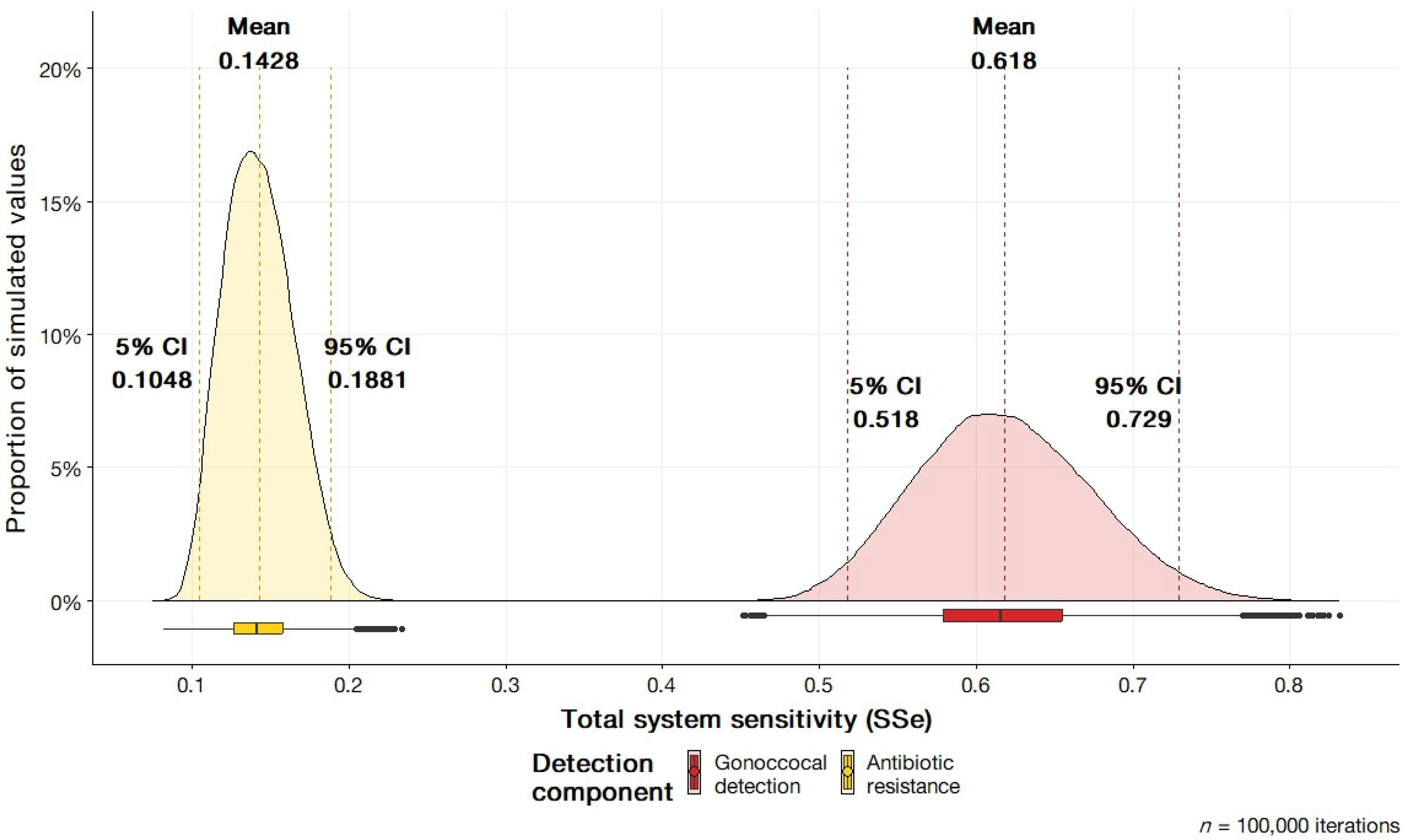
3.2.1. Overall System Sensitivity Outputs
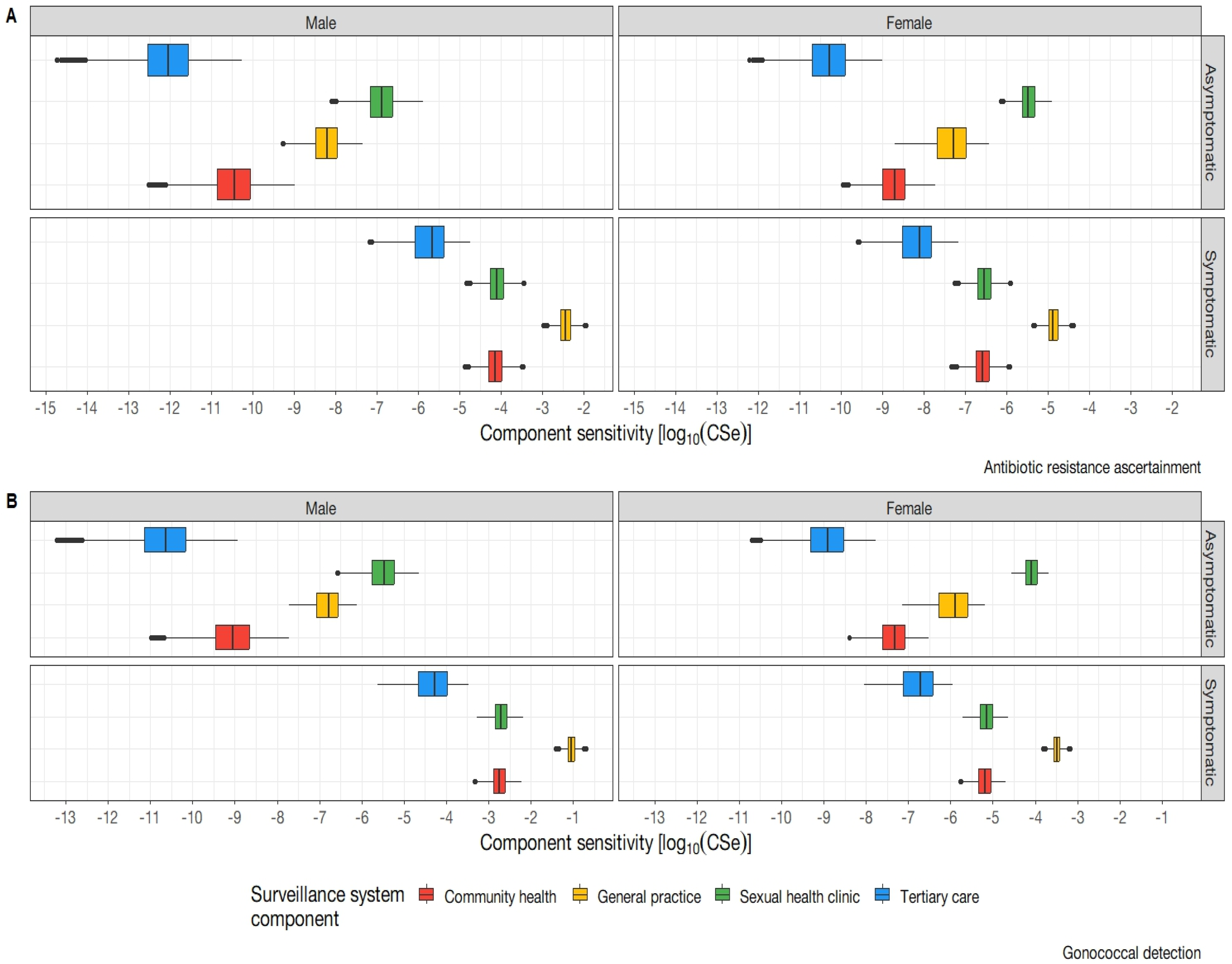
3.2.2. System Sub-Component Sensitivity Outputs
3.3. Sensitivity Analysis
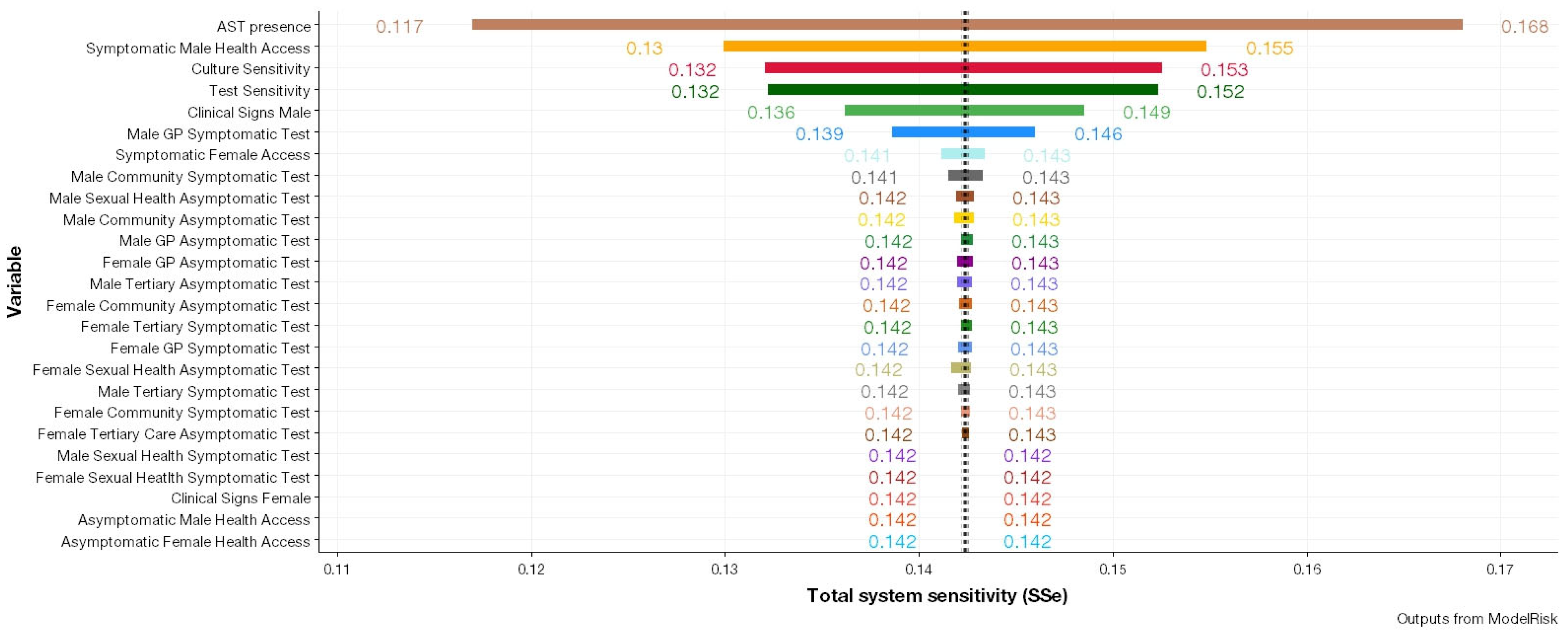
3.3.1. ModelRisk Sensitivity Analysis
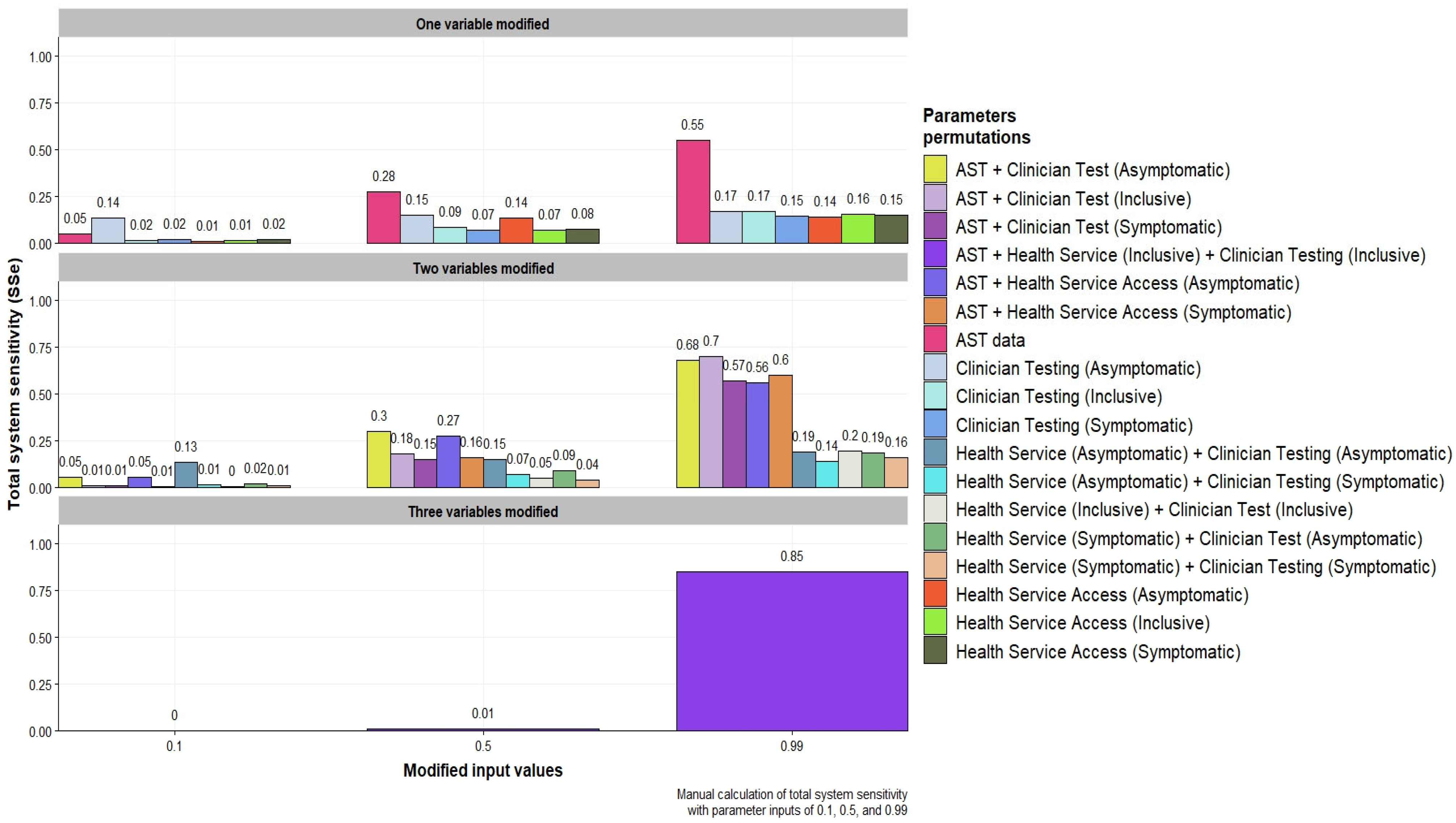
3.3.2. Modification of Parameters Identified from Sensitivity Analysis
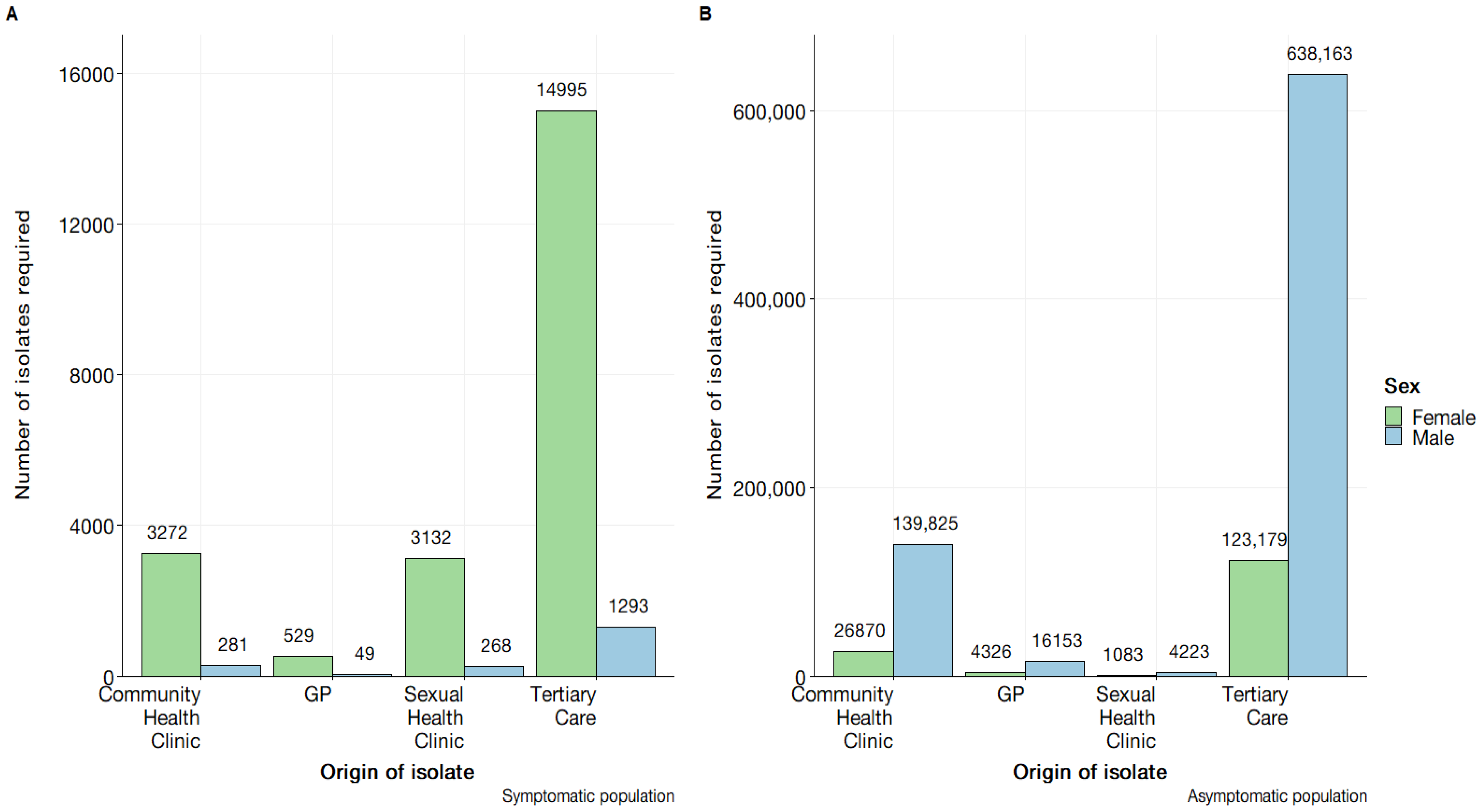
3.4. Estimation of Detection Capability
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AGSP | Australian Gonococcal Surveillance Programme |
| AMR | Antimicrobial Resistance |
| ASPREN | Australian Sentinel Practice Research Network |
| AST | Antimicrobial Susceptibility Test |
| CDC | Centres for Disease Control and Prevention |
| CSe | Component Sensitivity |
| PERT | Program Evaluation and Review Technique |
| SeCi | Surveillance Sensitivity Component |
| SSe | System Sensitivity |
| SSeUi | System Sensitivity Unit |
| STM | Scenario Tree Model |
| WHO | World Health Organization |
References
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, J. Tackling Drug-Resistance Infections Globally: Final Report and Recommendations. Review on Antimicrobial Resistance. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 15 August 2021).
- WHO. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015; Available online: https://ahpsr.who.int/publications/i/item/global-action-plan-on-antimicrobial-resistance (accessed on 15 August 2021).
- Groseclose, S.L.; Buckeridge, D.L. Public Health Surveillance Systems: Recent Advances in Their Use and Evaluation. Annu. Rev. Public Health 2017, 38, 57–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhingra, S.; Rahman, N.A.A.; Peile, E.; Rahman, M.; Sartelli, M.; Hassali, M.A.; Islam, T.; Islam, S.; Haque, M. Microbial Resistance Movements: An Overview of Global Public Health Threats Posed by Antimicrobial Resistance, and How Best to Counter. Front. Public Health 2020, 8, 535668. [Google Scholar] [CrossRef] [PubMed]
- Bax, R.; Bywater, R.; Cornaglia, G.; Goossens, H.; Hunter, P.; Isham, V.; Jarlier, V.; Jones, R.; Phillips, I.; Sahm, D.; et al. Surveillance of antimicrobial resistance—What, how and whither? Clin. Microbiol. Infect. 2001, 7, 316–325. [Google Scholar] [CrossRef]
- Diallo, O.O.; Baron, S.A.; Abat, C.; Colson, P.; Chaudet, H.; Rolain, J.-M. Antibiotic resistance surveillance systems: A review. J. Glob. Antimicrob. Resist. 2020, 23, 430–438. [Google Scholar] [CrossRef]
- Tacconelli, E.; Sifakis, F.; Harbarth, S.; Schrijver, R.; van Mourik, M.; Voss, A.; Sharland, M.; Rajendran, N.B.; Rodríguez-Baño, J.; Bielicki, J.; et al. Surveillance for control of antimicrobial resistance. Lancet Infect. Dis. 2018, 18, e99–e106. [Google Scholar] [CrossRef] [Green Version]
- German, R.R.; Lee, L.M.; Horan, J.M.; Milstein, R.L.; Pertowski, C.A.; Waller, M.N. Guidelines Working Group Centers for Disease C, Prevention: Updated guidelines for evaluating public health surveillance systems: Recommendations from the Guidelines Working Group. MMWR Recomm. Rep. 2001, 50, 13376. [Google Scholar]
- Martin, P.; Cameron, A.; Greiner, M. Demonstrating freedom from disease using multiple complex data sources: 1: A new methodology based on scenario trees. Prev. Vet. Med. 2007, 79, 71–97. [Google Scholar] [CrossRef]
- Calero, M.L.; Monti, G. Assessment of the Current Surveillance System for Human Leptospirosis in Ecuador by Decision Analytic Modeling. Front. Public Health 2022, 10, 711938. [Google Scholar] [CrossRef]
- Samaan, G.; Roche, P.W.; Greig, J.E.; Tapsall, J.W. Australian Gonococcal Surveillance P: Evaluation of the Australian Gonococcal Surveillance Programme. Commun. Dis. Intell. Q. Rep. 2005, 29, 143–149. [Google Scholar]
- Lahra, M.M.; Hogan, T.R.; Shoushtari, M.; Armstrong, B.H.; Network, A.T.N.N. Australian Gonococcal Surveillance Programme Annual Report, 2020. Commun. Dis. Intell. 2021, 45, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Lahra, M.M.; Hogan, T.R. Australian Gonococcal Surveillance Programme Annual Report, 2021. Commun. Dis. Intell. 2022, 46, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.; El Allaki, F.; Vallières, A. Adapting a scenario tree model for freedom from disease as surveillance progresses: The Canadian notifiable avian influenza model. Prev. Vet. Med. 2014, 114, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.; Vallières, A. Scenario tree model for animal disease freedom framed in the OIE context using the example of a generic swine model for Aujeszky’s disease in commercial swine in Canada. Prev. Vet. Med. 2016, 123, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Cowled, B.D.; Sergeant, E.S.; Leslie, E.E.; Crosbie, A.; Burroughs, A.; Kingston, O.; Neill, M.; Sawford, K.; van Andel, M. Use of scenario tree modelling to plan freedom from infection surveillance: Mycoplasma bovis in New Zealand. Prev. Vet. Med. 2021, 198, 105523. [Google Scholar] [CrossRef]
- Norström, M.; Jonsson, M.E.; Åkerstedt, J.; Whist, A.C.; Kristoffersen, A.B.; Sviland, S.; Hopp, P.; Wahlström, H. Estimation of the probability of freedom from bovine virus diarrhoea virus in Norway using scenario tree modelling. Prev. Vet. Med. 2014, 116, 37–46. [Google Scholar] [CrossRef] [Green Version]
- ACSQHC. AURA 2016: First Australian Report on Antimicrobial Use and Resistance in Human Health—Full Report. Australian Comission on Safety and Quality in Health Care. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/AURA-2016-First-Australian-Report-on-Antimicrobial-use-and-resistance-in-human-health.pdf (accessed on 21 March 2022).
- ACSQHC. AURA 2021: Fourth Australian Report on Antimicrobial Use and Resistance in Human Health. Australian Comission on Safety and Quality in Health Care. Available online: https://www.safetyandquality.gov.au/sites/default/files/2021-09/aura_2021_-_report_-_final_accessible_pdf_-_for_web_publication.pdf (accessed on 23 March 2022).
- mc2d: Tools for Two-Dimensional Monte-Carlo Simulations. Available online: http://riskassessment.r-forge.r-project.org/ (accessed on 10 January 2023).
- ModelRisk. Available online: https://www.vosesoftware.com/products/modelrisk/ (accessed on 20 September 2022).
- Ryan, K.E.; Wilkinson, A.L.; Chow, E.; Read, T.; Chen, M.; Locke, P.; Leitinger, D.; Bradshaw, C.; Pedrana, A.; Hellard, M.; et al. A comparative, retrospective analysis of HIV testing among gay, bisexual and other men who have sex with men in Melbourne, Australia. Aust. N. Z. J. Public Health 2019, 43, 419–423. [Google Scholar] [CrossRef] [Green Version]
- King, J.; McManus, H.; Kwon, A.; Gray, R.; McGregor, S. HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: Annual Surveillance Report 2022; Australian Government Department of Health and Aged Care: Canberra, Australia, 2022. [CrossRef]
- Workowski, A.K.; Bachmann, L.H. Centers for Disease Control and Prevention’s Sexually Transmitted Diseases Infection Guidelines. Clin. Infect. Dis. 2022, 74, S89–S94. [Google Scholar] [CrossRef]
- Parrella, A.; Dalton, C.B.; Pearce, R.; Litt, J.C.; Stocks, N. ASPREN surveillance system for influenza-like illness—A comparison with FluTracking and the National Notifiable Diseases Surveillance System. Aust. Fam. Physician 2009, 38, 932–936. [Google Scholar]
- Whelan, J.; Abbing-Karahagopian, V.; Serino, L.; Unemo, M. Gonorrhoea: A systematic review of prevalence reporting globally. BMC Infect. Dis. 2021, 21, 1152. [Google Scholar] [CrossRef]
- Kirkcaldy, R.D.; Weston, E.; Segurado, A.C.; Hughes, G. Epidemiology of gonorrhoea: A global perspective. Sex. Health 2019, 16, 401–411. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.R.M.; Dolk, F.C.K.; Smieszek, T.; Robotham, J.V.; Pouwels, K.B. Understanding the gender gap in antibiotic prescribing: A cross-sectional analysis of English primary care. BMJ Open 2018, 8, e020203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, N.; Mitchell, J.; Cooke, P.; Baral, S.; Arjyal, A.; Shrestha, A.; King, R. Gender and Antimicrobial Resistance: What Can We Learn from Applying a Gendered Lens to Data Analysis Using a Participatory Arts Case Study? Front. Glob. Women’s Health 2022, 3, 745862. [Google Scholar] [CrossRef] [PubMed]
- Sarenje, K.L.; Ngalamika, O.; Maimbolwa, M.C.; Siame, A.; Munsaka, S.M.; Kwenda, G. Antimicrobial resistance of Neisseria gonorrhoeae isolated from patients attending sexually transmitted infection clinics in Urban Hospitals, Lusaka, Zambia. BMC Infect. Dis. 2022, 22, 688. [Google Scholar] [CrossRef]
- Cadogan, S.L.; Browne, J.P.; Bradley, C.P.; Cahill, M.R. The effectiveness of interventions to improve laboratory requesting patterns among primary care physicians: A systematic review. Implement. Sci. 2015, 10, 167. [Google Scholar] [CrossRef] [PubMed]
- Whiley, D.M.; Jennison, A.; Pearson, J.; Lahra, M.M. Genetic characterisation of Neisseria gonorrhoeae resistant to both ceftriaxone and azithromycin. Lancet Infect. Dis. 2018, 18, 717–718. [Google Scholar] [CrossRef]
- Abraha, M.; Egli-Gany, D.; Low, N. Epidemiological, behavioural, and clinical factors associated with antimicrobial-resistant gonorrhoea: A review. F1000Research 2018, 7, 400. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Node | Definition |
|---|---|
| Antimicrobial Resistance Detection Node | Refers to the points at which N. gonorrhoea antibiotic resistance is detected. Given as a dichotomous event. |
| Category Node | Category nodes refer to proportions of a population that fall on a given pathway. |
| Detection Node | Detection nodes are points at which N. gonorrhoea is detected. Given as a dichotomous event. |
| Infection Node | Infection nodes refer to the reported proportion of infections for the specified group. |
| System Component | Minimum | Lower 95% CI | Mean | Median | Upper 95% CI | Maximum |
|---|---|---|---|---|---|---|
| Gonococcal detection | 0.457 | 0.524 | 0.624 | 0.625 | 0.735 | 0.848 |
| Antibiotic resistance status | 0.08 | 0.106 | 0.144 | 0.143 | 0.189 | 0.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Do, P.C.; Alemu, Y.A.; Reid, S.A. Enhancing Insights into Australia’s Gonococcal Surveillance Programme through Stochastic Modelling. Pathogens 2023, 12, 907. https://doi.org/10.3390/pathogens12070907
Do PC, Alemu YA, Reid SA. Enhancing Insights into Australia’s Gonococcal Surveillance Programme through Stochastic Modelling. Pathogens. 2023; 12(7):907. https://doi.org/10.3390/pathogens12070907
Chicago/Turabian StyleDo, Phu Cong, Yibeltal Assefa Alemu, and Simon Andrew Reid. 2023. "Enhancing Insights into Australia’s Gonococcal Surveillance Programme through Stochastic Modelling" Pathogens 12, no. 7: 907. https://doi.org/10.3390/pathogens12070907
APA StyleDo, P. C., Alemu, Y. A., & Reid, S. A. (2023). Enhancing Insights into Australia’s Gonococcal Surveillance Programme through Stochastic Modelling. Pathogens, 12(7), 907. https://doi.org/10.3390/pathogens12070907