Demographics and Epidemiology of Hepatitis B in the State of Qatar: A Five-Year Surveillance-Based Incidence Study


 ,
,  , , , ,
, , , ,
Abstract
:1. Background
2. Subjects & Methods
3. Results
3.1. Characteristics of the Study Group
3.2. Yearly Distribution and Seasonality of Hepatitis B Cases
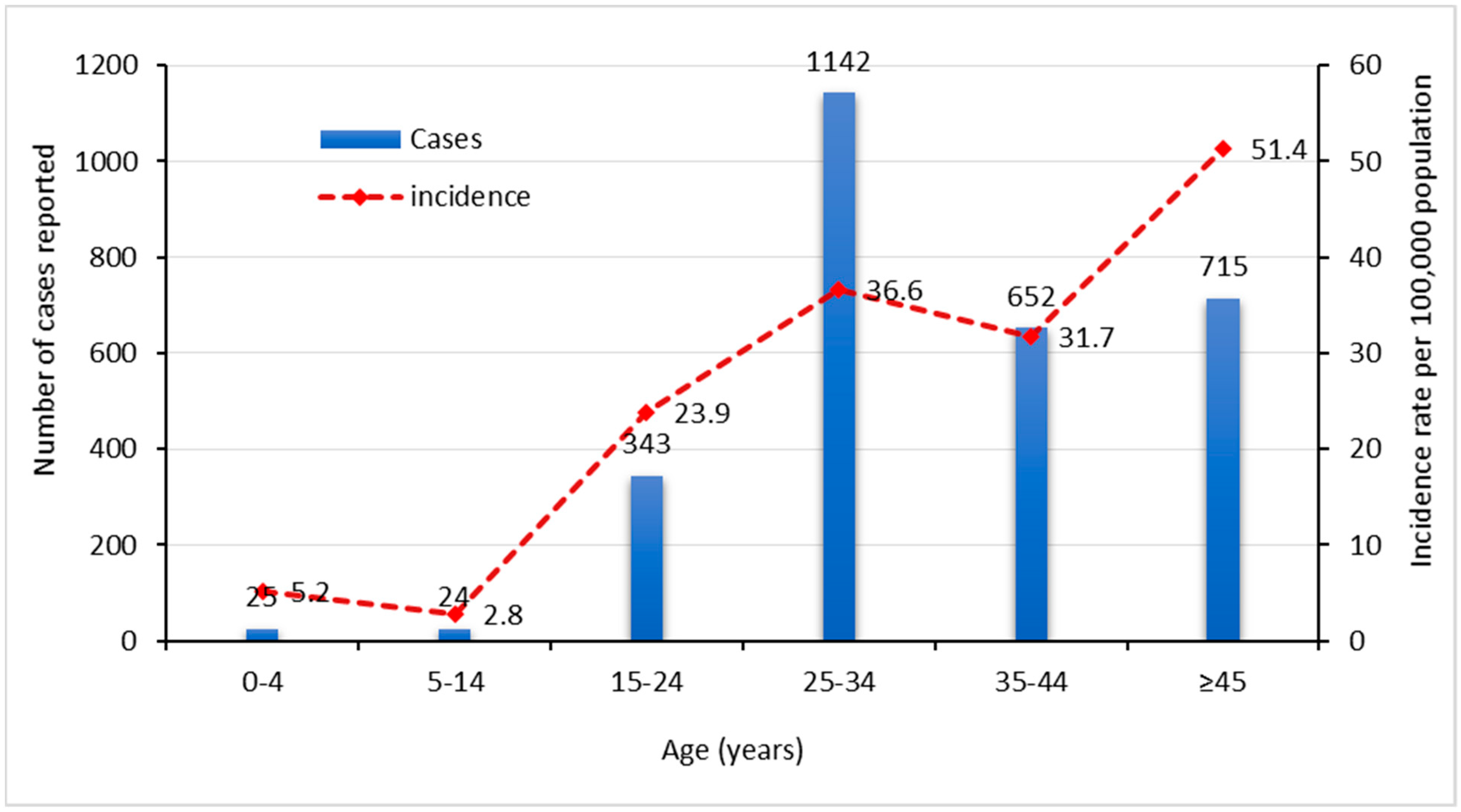
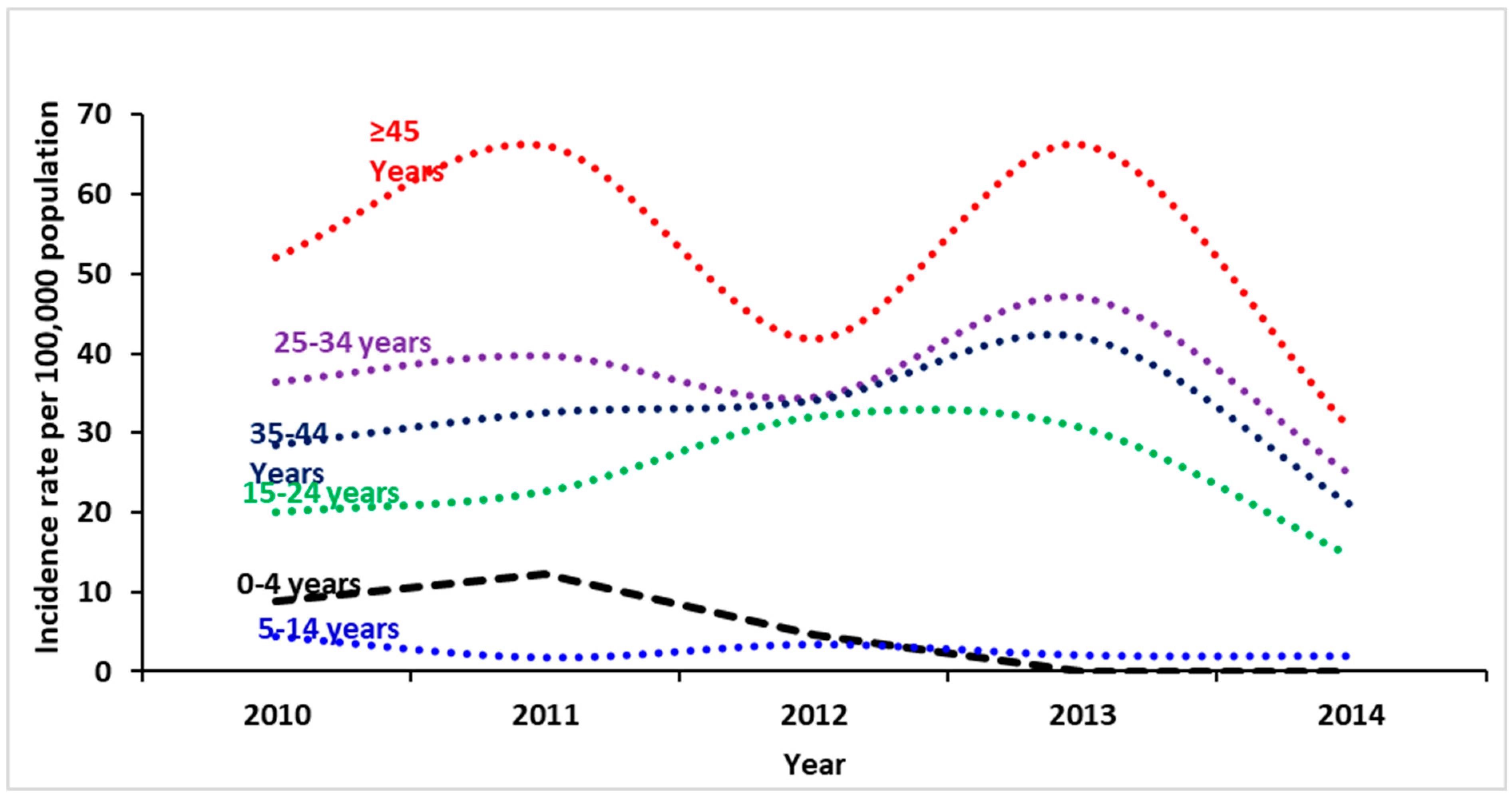
3.3. Prevalence of HBV Infection by Gender, Age, and Nationality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zur Hausen, H. Viruses in human cancers. Science 1991, 254, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Roggendorf, M. Current topics in hepatitis. J. Clin. Virol. 2004, 30 (Suppl. 1), v–vi. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, J.N.; Zuckerman, A.J. Current topics in hepatitis B. J. Infect. 2000, 41, 130–136. [Google Scholar] [CrossRef] [PubMed]
- WHO. Fact Sheet. 2015. Available online: http://www.who.int/mediacentre/factsheets/fs204/en/# (accessed on 24 March 2018).
- Andre, F. Hepatitis B epidemiology in Asia, the Middle East and Africa. Vaccine 2000, 18 (Suppl. 1), S20–S22. [Google Scholar] [CrossRef]
- Miglietta, A.; Quinten, C.; Lopalco, P.L.; Duffell, E. Impact of hepatitis B vaccination on acute hepatitis B epidemiology in European Union/European Economic Area countries, 2006 to 2014. Eurosurveillance 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, J. Hepatitis B epidemiology in Latin America. Vaccine 2000, 18 (Suppl. 1), S17–S19. [Google Scholar] [CrossRef]
- Custer, B.; Sullivan, S.D.; Hazlet, T.K.; Iloeje, U.; Veenstra, D.L.; Kowdley, K.V. Global epidemiology of hepatitis B virus. J. Clin. Gastroenterol. 2004, 38 (Suppl. 3), S158–S168. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hepatitis B. Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 6 May 2019).
- Gasim, G.I. Hepatitis B virus in the Arab world: Where do we stand? Arab J. Gastroenterol. 2013, 14, 35–43. [Google Scholar] [CrossRef] [PubMed]
- EMRO-WHO. World Hepatitis Day in Egypt Focuses on Hepatitis B and C Prevention. 2015. Available online: http://www.emro.who.int/media/news/world-hepatitis-day-in-egypt-focuses-on-hepatitis-b-and-c-prevention.html (accessed on 24 March 2018).
- World Health Organization. WHO Fact Sheet. 2015. Available online: http://www.emro.who.int/media/news/world-hepatitis-day-in-egypt-focuses-on-hepatitis-b-and-c-prevention.html (accessed on 25 March 2018).
- Khan, G.; Hashim, M.J. Burden of virus-associated liver cancer in the Arab world, 1990–2010. Asian Pac. J. Cancer Prev. 2015, 16, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Habibzadeh, F. Viral hepatitis in the Middle East. Lancet 2014, 384, 1–2. [Google Scholar]
- Al-Humayed, S.M. Hepatitis B and C Viral Infections in Tihamet Aseer, South-Western Saudi Arabia: Are There Gender Differences? Saudi J. Med. Med. Sci. 2017, 5, 110–115. [Google Scholar]
- Memish, Z.A.; Knawy, B.A.; El-Saed, A. Incidence trends of viral hepatitis A, B, and C seropositivity over eight years of surveillance in Saudi Arabia. Int. J. Infect. Dis. 2010, 14, e115–e120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glynn, M.J.; Rashid, A.; Antao, A.J.; Coleman, J.C.; Howard, C.R.; Zuckerman, A.J.; Murray-Lyon, I.M. Imported epidemic non-A, non-B hepatitis in Qatar. J. Med. Virol. 1985, 17, 371–375. [Google Scholar] [CrossRef]
- Bener, A.; Al-Kaabi, S.; Derbala, M.; Al-Marri, A.; Rikabi, A. The epidemiology of viral hepatitis in Qatar. Saudi J. Kidney Dis. Transplant. 2009, 20, 300–306. [Google Scholar]
- Laboratory Medicine and Pathology. 2018. Available online: https://www.hamad.qa/EN/Hospitals-and-services/Hamad-General-Hospital/Hospital-Services/Clinical-Departments/Pages/Laboratory-Medicine-and-Pathology.aspx (accessed on 25 March 2018).
- Ministry of Public Health. Medical Commission. 2015. Available online: https://www.moph.gov.qa/health-services/Pages/medical-commission.aspx (accessed on 25 March 2018).
- Qatar National Health Strategy. 2011. Available online: www.qu.edu.qa/pharmacy/components/.../Qatar_National_Health_Strategy.pdf (accessed on 25 March 2018).
- World Health Organization. Surveillance and Control. Available online: http://www.who.int/csr/disease/hepatitis/whocdscsrlyo20022/en/index4.html (accessed on 25 March 2018).
- CDC. Interpretation of Hepatitis B Serologic Test Results. Available online: https://www.cdc.gov/hepatitis/hbv/pdfs/serologicchartv8.pdf (accessed on 25 March 2018).
- Statistical Subjects. 2015. Available online: https://www.mdps.gov.qa/en/statistics1/pages/default.aspx (accessed on 25 March 2018).
- Legatum Institute. The Ledatum Proesperity Index. Available online: http://www.prosperity.com/rankings (accessed on 26 March 2018).
- Hollinger, F.B.; Liang, T.J. Hepatitis B Virus, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011. [Google Scholar]
- Viral Hepatitis Prevention Board. Prevention and Control of Hepatitis B in the Community. Communicable Disease Series. 2017. Available online: http://www.vhpb.org/ (accessed on 26 March 2018).
- Gasim, G.I. Comment on: hepatitis C virus in Arab world: A state of concern. Sci. World J. 2012, 2012, 534173. [Google Scholar] [CrossRef] [PubMed]
- Baig, S. Gender disparity in infections of Hepatitis B virus. J. Coll. Phys. Surg. Pak. 2009, 19, 598–600. [Google Scholar]
- Khazaei, S.; Karami, M.; Ayubi, E.; Mohammadbeigi, A.; Hasanbeigi, A.; Mansori, K.; Mir-Shekar, M.R. Trends in epidemiology of Hepatitis B and C Infections in Ilam Province: National Notifiable Diseases Surveillance System data. Casp. J. Intern. Med. 2018, 9, 16–21. [Google Scholar]
- Hepatitis B Infection in Canada: Public Health Agency of Canada—Canada.ca. Available online: https://www.canada.ca/en/public-health/services/infectious-diseases/hepatitis-b-infection-canada.html#fig3 (accessed on 26 March 2018).
- Zeng, F.; Guo, P.; Huang, Y.; Xin, W.; Du, Z.; Zhu, S.; Deng, Y.; Zhang, D.; Hao, Y. Epidemiology of hepatitis B virus infection: Results from a community-based study of 0.15 million residents in South China. Sci. Rep. 2016, 6, 36186. [Google Scholar] [CrossRef] [PubMed]
- MOHP. Baby Immunization Schedule. 2018. Available online: https://eservices.moph.gov.qa/NIP/En/immschev.jsp (accessed on 26 March 2018).
- Al-Romaihi, H.; Al-Masri, H.; Shawky, S.; Al Thani, M.; Al Awaidy, S.; Janahi, M.A.; Derbala, M.; Al-Ansari, K.; Allison, R. Assessment of hepatitis B immunization programme among school students in Qatar. East. Mediterr Health J. 2018, 24, 736–744. [Google Scholar] [CrossRef] [PubMed]
- HMC Supporting Viral Hepatitis Elimination through Awareness Activities, Increased Diagnosis and Key Interventions. 2018. Available online: https://www.hamad.qa/EN/news/2017/July/Pages/HMC-Supporting-Viral-Hepatitis-Elimination-through-Awareness-Activities,-Increased-Diagnosis-and-Key-Interventions.aspx (accessed on 26 March 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epidemiological Year | Gender | Total N (%) | |
|---|---|---|---|
| Male N (%) | Female N (%) | ||
| 2010 | 315 (61.9%) | 202 (39.1%) | 517 (100%) |
| 2011 | 385 (64.9%) | 208 (35.1) | 593 (100%) |
| 2012 | 378 (67.5%) | 182 (32.5) | 560 (100%) |
| 2013 | 599 (75.5%) | 194 (24.5%) | 793 (100%) |
| 2014 | 333 (76.0%) | 105 (24.0%) | 438 (100%) |
| Overall | 2010 (69.3%) | 891 (30.7%) | 2901 (100%) |
| Epidemiological Year | Nationality | Total N (%) | |
|---|---|---|---|
| Qatari N (%) | Non-Qatari N (%) | ||
| 2010 | 81 (15.7) | 436 (84.3) | 517 (100%) |
| 2011 | 76 (12.8) | 517 (87.2) | 593 (100%) |
| 2012 | 62 (11.7) | 498 (88.9) | 560 (100%) |
| 2013 | 61 (7.7) | 732 (92.3) | 793 (100%) |
| 2014 | 27 (6.2) | 411 (93.8) | 438 (100%) |
| Overall | 307 (10.6%) | 2594 (89.4%) | 2901 (100%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Romaihi, H.E.; Ganesan, N.; Farag, E.A.; Smatti, M.K.; Nasrallah, G.K.; Himatt, S.M.; Derbala, M.F.; Alshamali, M.; Mahadoon, L.K.; Khogali, H.S.; et al. Demographics and Epidemiology of Hepatitis B in the State of Qatar: A Five-Year Surveillance-Based Incidence Study. Pathogens 2019, 8, 68. https://doi.org/10.3390/pathogens8020068
Al Romaihi HE, Ganesan N, Farag EA, Smatti MK, Nasrallah GK, Himatt SM, Derbala MF, Alshamali M, Mahadoon LK, Khogali HS, et al. Demographics and Epidemiology of Hepatitis B in the State of Qatar: A Five-Year Surveillance-Based Incidence Study. Pathogens. 2019; 8(2):68. https://doi.org/10.3390/pathogens8020068
Chicago/Turabian StyleAl Romaihi, Hamad E., Nandakumar Ganesan, Elmoubasher A. Farag, Maria K. Smatti, Gheyath K. Nasrallah, Sayed M. Himatt, Moutaz F. Derbala, Maha Alshamali, Lylu K. Mahadoon, Hayat S. Khogali, and et al. 2019. "Demographics and Epidemiology of Hepatitis B in the State of Qatar: A Five-Year Surveillance-Based Incidence Study" Pathogens 8, no. 2: 68. https://doi.org/10.3390/pathogens8020068
APA StyleAl Romaihi, H. E., Ganesan, N., Farag, E. A., Smatti, M. K., Nasrallah, G. K., Himatt, S. M., Derbala, M. F., Alshamali, M., Mahadoon, L. K., Khogali, H. S., Sallam, M., Al Thani, A. A., Al Thani, M., Al Kaabi, S., & Yassine, H. M. (2019). Demographics and Epidemiology of Hepatitis B in the State of Qatar: A Five-Year Surveillance-Based Incidence Study. Pathogens, 8(2), 68. https://doi.org/10.3390/pathogens8020068