
Molecular Typing Reveals Distinct Mycoplasma genitalium Transmission Networks among a Cohort of Men Who Have Sex with Men and a Cohort of Women in France

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Laboratory Procedures
2.3. Data Analysis
3. Results
3.1. Sample and Patient Characteristics
3.2. Antimicrobial Resistance
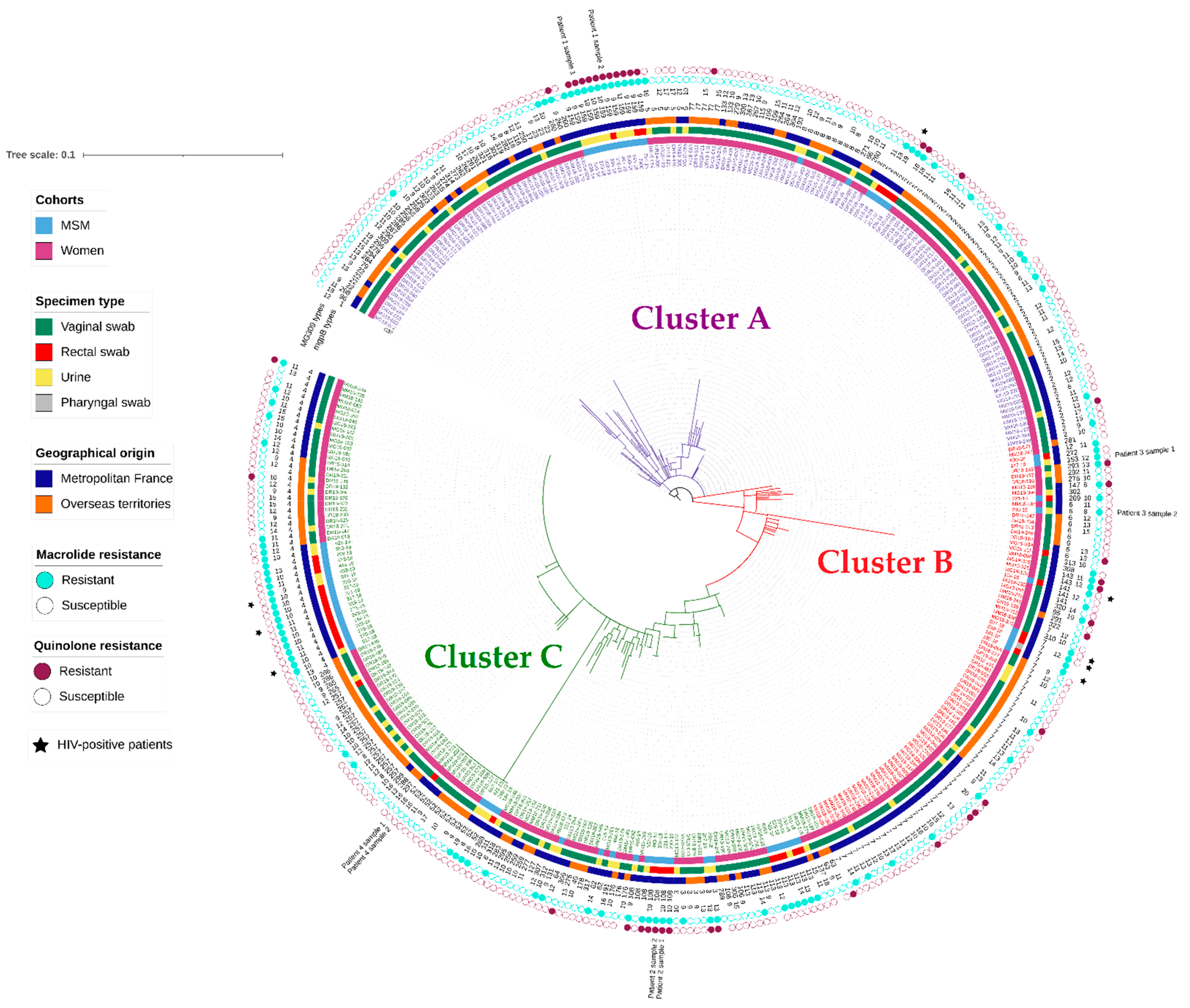
3.3. Genetic Diversity and Population Structure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gnanadurai, R.; Fifer, H. Mycoplasma genitalium: A Review. Microbiology 2020, 166, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Machalek, D.A.; Tao, Y.; Shilling, H.; Jensen, J.S.; Unemo, M.; Murray, G.; Chow, E.P.F.; Low, N.; Garland, S.M.; Vodstrcil, L.A.; et al. Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: A systematic review and meta-analysis. Lancet Infect. Dis. 2020, 20, 1302–1314. [Google Scholar] [CrossRef]
- Hamasuna, R.; Hanzawa, H.; Moritomo, A.; Matsumoto, M.; Aono, H.; Tomisaki, I.; Akasaka, T.; Fujimoto, N.; Jensen, J.S. Analysis of fluoroquinolone-resistance using MIC determination and homology modelling of ParC of contemporary Mycoplasma genitalium strains. J. Infect. Chemother. 2021, 28, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Hamasuna, R.; Le, P.T.; Kutsuna, S.; Furubayashi, K.; Matsumoto, M.; Ohmagari, N.; Fujimoto, N.; Matsumoto, T.; Jensen, J.S. Mutations in ParC and GyrA of moxifloxacin-resistant and susceptible Mycoplasma genitalium strains. PLoS ONE 2018, 13, e0198355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annual Report of the French National Reference Center for Bacterial STIs. 2020. Available online: https://www.cnr-ist.fr/ressources/editeur/2020_RAPPORT_CNR_IST_VF.pdf (accessed on 3 August 2022).
- Bercot, B.; Charreau, I.; Rousseau, C.; Delaugerre, C.; Chidiac, C.; Pialoux, G.; Capitant, C.; Bourgeois-Nicolaos, N.; Raffi, F.; Pereyre, S.; et al. High prevalence and high rate of antibiotic resistance of Mycoplasma genitalium infections in men who have sex with men: A sub-study of the ANRS Ipergay PrEP trial. Clin. Infect. Dis. 2020, 73, e2127–e2133. [Google Scholar] [CrossRef]
- Guiraud, J.; Lounnas, M.; Boissiere, A.; Le Roy, C.; Elguero, E.; Banuls, A.L.; Bébéar, C.; Godreuil, S.; Pereyre, S. Lower mgpB diversity in macrolide-resistant Mycoplasma genitalium infecting men visiting two sexually transmitted infection clinics in Montpellier, France. J. Antimicrob. Chemother. 2021, 76, 43–47. [Google Scholar] [CrossRef]
- McIver, R.; Jalocon, D.; McNulty, A.; Jeoffreys, N.J.; Chen, S.C.; Power, M.; Couldwell, D.L. Men who have sex with men with Mycoplasma genitalium-positive nongonococcal urethritis are more likely to have macrolide-resistant strains than men with only female partners: A prospective study. Sex. Transm. Dis. 2019, 46, 513–517. [Google Scholar] [CrossRef]
- Hjorth, S.V.; Bjornelius, E.; Lidbrink, P.; Falk, L.; Dohn, B.; Berthelsen, L.; Ma, L.; Martin, D.H.; Jensen, J.S. Sequence-based typing of Mycoplasma genitalium reveals sexual transmission. J. Clin. Microbiol. 2006, 44, 2078–2083. [Google Scholar] [CrossRef] [Green Version]
- Dumke, R.; Rust, M.; Glaunsinger, T. MgpB Types among Mycoplasma genitalium strains from men who have sex with men in Berlin, Germany, 2016–2018. Pathogens 2019, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Dumke, R.; Spornraft-Ragaller, P. Antibiotic resistance and genotypes of Mycoplasma genitalium during a resistance-guided treatment regime in a German university hospital. Antibiotics 2021, 10, 962. [Google Scholar] [CrossRef]
- Pineiro, L.; Idigoras, P.; Cilla, G. Molecular typing of Mycoplasma genitalium-positive specimens discriminates between persistent and recurrent infections in cases of treatment failure and supports contact tracing. Microorganisms 2019, 7, 609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumke, R. Molecular tools for typing Mycoplasma pneumoniae and Mycoplasma genitalium. Front. Microbiol. 2022, 13, 904494. [Google Scholar] [CrossRef] [PubMed]
- Chua, T.P.; Bodiyabadu, K.; Machalek, D.A.; Garland, S.M.; Bradshaw, C.S.; Plummer, E.L.; Danielewski, J.; Vodstrcil, L.A.; Doyle, M.L.; Murray, G.L. Prevalence of Mycoplasma genitalium fluoroquinolone-resistance markers, and dual-class-resistance markers, in asymptomatic men who have sex with men. J. Med. Microbiol. 2021, 70, 001429. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Huerta, M.; Serra-Pladevall, J.; Esperalba, J.; Moreno-Mingorance, A.; Fernandez-Naval, C.; Barbera, M.J.; Aparicio, D.; Pich, O.Q.; Pumarola, T.; Jensen, J.S.; et al. Single-locus-sequence-based typing of the mgpB gene reveals transmission dynamics in Mycoplasma genitalium. J. Clin. Microbiol. 2020, 58, e01886-19. [Google Scholar] [CrossRef]
- Cazanave, C.; Charron, A.; Renaudin, H.; Bébéar, C. Method comparison for molecular typing of French and Tunisian Mycoplasma genitalium-positive specimens. J. Med. Microbiol. 2012, 61, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Laumen, J.G.E.; van Alphen, L.B.; Maduna, L.D.; Hoffman, C.M.; Klausner, J.D.; Medina-Marino, A.; Kock, M.M.; Peters, R.P.H. Molecular epidemiological analysis of Mycoplasma genitalium shows low prevalence of azithromycin resistance and a well-established epidemic in South Africa. Sex. Transm. Infect. 2021, 97, 152–156. [Google Scholar] [CrossRef]
- Sweeney, E.L.; Tickner, J.; Bletchly, C.; Nimmo, G.R.; Whiley, D.M. Genotyping of Mycoplasma genitalium suggests de novo acquisition of antimicrobial resistance in Queensland, Australia. J. Clin. Microbiol. 2020, 58, e00641-20. [Google Scholar] [CrossRef]
- Jensen, J.S.; Cusini, M.; Gomberg, M.; Moi, H. 2016 European guideline on Mycoplasma genitalium infections. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1650–1656. [Google Scholar] [CrossRef] [Green Version]
- Jensen, J.S.; Cusini, M.; Gomberg, M.; Moi, H.; Wilson, J.; Unemo, M. 2021 European guideline on the management of Mycoplasma genitalium infections. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 641–650. [Google Scholar] [CrossRef]
- Soni, S.; Horner, P.; Rayment, M.; Pinto-Sander, N.; Naous, N.; Parkhouse, A.; Bancroft, D.; Patterson, C.; Fifer, H. British Association for Sexual Health and HIV national guideline for the management of infection with Mycoplasma genitalium (2018). Int. J. STD AIDS 2019, 30, 938–950. [Google Scholar] [CrossRef]
- Le Roy, C.; Hénin, N.; Bébéar, C.; Pereyre, S. Evaluation of a commercial multiplex quantitative PCR (qPCR) assay for simultaneous detection of Mycoplasma genitalium and macrolide resistance-associated mutations in clinical specimens. J. Clin. Microbiol. 2017, 55, 978–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, J.S.; Bjornelius, E.; Dohn, B.; Lidbrink, P. Use of TaqMan 5’ nuclease real-time PCR for quantitative detection of Mycoplasma genitalium DNA in males with and without urethritis who were attendees at a sexually transmitted disease clinic. J. Clin. Microbiol. 2004, 42, 683–692. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Taylor, S.; Jensen, J.S.; Myers, L.; Lillis, R.; Martin, D.H. Short tandem repeat sequences in the Mycoplasma genitalium genome and their use in a multilocus genotyping system. BMC Microbiol. 2008, 8, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Roy, C.; Hénin, N.; Pereyre, S.; Bébéar, C. Fluoroquinolone-Resistant Mycoplasma genitalium, Southwestern France. Emerg. Infect. Dis. 2016, 22, 1677–1679. [Google Scholar] [CrossRef] [Green Version]
- Hunter, P.R.; Gaston, M.A. Numerical index of the discriminatory ability of typing systems: An application of Simpson’s index of diversity. J. Clin. Microbiol. 1988, 26, 2465–2466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fookes, M.C.; Hadfield, J.; Harris, S.; Parmar, S.; Unemo, M.; Jensen, J.S.; Thomson, N.R. Mycoplasma genitalium: Whole genome sequence analysis, recombination and population structure. BMC Genom. 2017, 18, 993. [Google Scholar] [CrossRef]
- Dionne-Odom, J.; Geisler, W.M.; Aaron, K.J.; Waites, K.B.; Westfall, A.O.; Van Der Pol, B.; Xiao, L. High prevalence of multidrug-resistant Mycoplasma genitalium in human immunodeficiency virus-infected men who have sex with men in Alabama. Clin. Infect. Dis. 2018, 66, 796–798. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, A.E.; Wagenlehner, F.M.E.; Mulgirigama, A.; Twynholm, M. Escherichia coli resistance to fluoroquinolones in community-acquired uncomplicated urinary tract infection in women: A systematic review. Antimicrob. Agents Chemother. 2020, 64, e00862-20. [Google Scholar] [CrossRef]
- Dumke, R.; Thurmer, A.; Jacobs, E. Emergence of Mycoplasma genitalium strains showing mutations associated with macrolide and fluoroquinolone resistance in the region Dresden, Germany. Diagn. Microbiol. Infect. Dis. 2016, 86, 221–223. [Google Scholar] [CrossRef]
- Plummer, E.L.; Murray, G.L.; Bodiyabadu, K.; Su, J.; Garland, S.M.; Bradshaw, C.S.; Read, T.R.H.; Tabrizi, S.N.; Danielewski, J.A. A custom amplicon sequencing approach to detect resistance associated mutations and sequence types in Mycoplasma genitalium. J. Microbiol. Methods 2020, 179, 106089. [Google Scholar] [CrossRef]
- Sweeney, E.L.; Lowry, K.; Bletchly, C.; Nimmo, G.R.; Whiley, D.M. Mycoplasma genitalium infections can comprise a mixture of both fluoroquinolone-susceptible and fluoroquinolone-resistant strains. J. Antimicrob. Chemother. 2021, 76, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Musatovova, O.; Baseman, J.B. Analysis identifying common and distinct sequences among Texas clinical strains of Mycoplasma genitalium. J. Clin. Microbiol. 2009, 47, 1469–1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iverson-Cabral, S.L.; Astete, S.G.; Cohen, C.R.; Rocha, E.P.; Totten, P.A. Intrastrain heterogeneity of the mgpB gene in Mycoplasma genitalium is extensive in vitro and in vivo and suggests that variation is generated via recombination with repetitive chromosomal sequences. Infect Immun. 2006, 74, 3715–3726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chrisment, D.; Charron, A.; Cazanave, C.; Pereyre, S.; Bébéar, C. Detection of macrolide resistance in Mycoplasma genitalium in France. J. Antimicrob. Chemother. 2012, 67, 2598–2601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pond, M.J.; Nori, A.V.; Witney, A.A.; Lopeman, R.C.; Butcher, P.D.; Sadiq, S.T. High prevalence of antibiotic-resistant Mycoplasma genitalium in nongonococcal urethritis: The need for routine testing and the inadequacy of current treatment options. Clin. Infect. Dis. 2014, 58, 631–637. [Google Scholar] [CrossRef] [Green Version]
- Mondeja, B.A.; Jensen, J.S.; Rodríguez, I.; Morier, L.F.; Kourí, V.; Rodríguez, N.M.; Fernández, C. Isolation of Mycoplasma genitalium from patients with urogenital infections: First report from the Latin-American region. New Microbes New Infect. 2013, 1, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, M.; Ito, S.; Yasuda, M.; Tsuchiya, T.; Hatazaki, K.; Takanashi, M.; Ezaki, T.; Deguchi, T. Remarkable increase in fluoroquinolone-resistant Mycoplasma genitalium in Japan. J. Antimicrob. Chemother. 2014, 69, 2376–2382. [Google Scholar] [CrossRef] [Green Version]
- Wood, G.E.; Jensen, N.L.; Astete, S.; Jensen, J.S.; Kenny, G.E.; Khosropour, C.M.; Gillespie, C.W.; Manhart, L.E.; Totten, P.A. Azithromycin and doxycycline resistance profiles of U.S. Mycoplasma genitalium strains and their association with treatment outcomes. J. Clin. Microbiol. 2021, 59, e0081921. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Women n = 305 | MSM a n = 65 | p Value |
|---|---|---|---|
| Age | |||
| Mean +/− SD | 26.3 +/− 7.9 | 36.6 +/− 12.5 | <0.001 b |
| Median (IQR) | 24 (14–52) | 33 (20–75) | |
| Geographical origin—no. (%) | |||
| Metropolitan France | 131 (43.0%) | 65 (100.0%) | |
| Paris region | 82 (62.6%) | 37 (56.9%) | 0.286 c |
| Other French regions | 49 (37.4%) | 27 (41.6%) | |
| Unknown | 0 | 1 (1.5%) | |
| French overseas territories e | 174 (57.0%) | 0 | |
| C. trachomatis coinfection—no. (%) | |||
| Available information | 200 (65.6%) | 60 (92.3%) | |
| Coinfection | 40 (20.0%) | 6 (10.0%) | 0.084 c |
| No coinfection | 160 (80.0%) | 54 (90.0%) | |
| Missing information | 105 (34.4%) | 5 (7.7%) | |
| Macrolide treatment anteriority—no. (%) | |||
| Available information | ND | 39 (60.0%) | |
| Previous macrolide regimen | ND | 35 (89.7%) | |
| No previous macrolide regimen | ND | 4 (10.3%) | |
| Missing information | ND | 26 (40.0%) | |
| Macrolide resistance—no. (%) | |||
| Resistant | 43 (14.1%) | 62 (95.4%) | <0.001 d |
| Susceptible | 262 (85.9%) | 3 (4.6%) | |
| All Patients | Cohort | ||
|---|---|---|---|
| Women | MSM | ||
| parC gene | |||
| Successful amplification | 338 | 276 | 62 |
| Wild type | 291 (86.1%) | 251 (90.9%) | 40 (64.5%) |
| Mutations detected a | 47 (13.9%) | 25 (9.1%) | 22 (35.5%) |
| Gly81Cys | 1 | 1 | - |
| Ser83Arg | 1 | 1 | - |
| Ser83Asn | 4 | 2 | 2 |
| Ser83Ile | 32 | 13 | 19 |
| Asp87Asn | 2 | 2 | - |
| Asp87Tyr | 3 | 3 | - |
| Ser95Asn | 1 | 1 | - |
| Ile105Phe | 1 | 1 | - |
| His106Tyr | 1 | 1 | - |
| Ala119Val | 1 | - | 1 |
| No amplification | 32 | 29 | 3 |
| Total of patients | 370 | 305 | 65 |
| gyrA gene | |||
| Successful amplification | 283 | 227 | 56 |
| Wild type | 279 (98.6%) | 225 (99.1%) | 54 (96.4%) |
| Mutations detected | 4 (1.4%) | 2 (0.9%) | 2 (3.6%) |
| Gly93Cys b | 1 | - | 1 |
| Met95Ile b | 1 | - | 1 |
| Ala105Thr | 1 | 1 | - |
| Asp107Asn | 1 | 1 | - |
| No amplification | 55 | 49 | 6 |
| Total of patients | 338 | 276 | 62 |
| Cluster A | Cluster B | Cluster C | pA-Ba | pA-Cb | pB-Cc | |
|---|---|---|---|---|---|---|
| Total number of patients (n = 370) | 149 | 80 | 141 | |||
| Cohorts | ||||||
| MSM | 17 (11.4%) | 9 (11.3%) | 39 (27.7%) | 0.971 | <0.001 | 0.004 |
| Women | 132 (88.6%) | 71 (88.7%) | 102 (72.3%) | |||
| Geographical origin | ||||||
| Metropolitan France | 67 (45.0%) | 51 (63.8%) | 78 (55.3%) | 0.007 | 0.078 | 0.222 |
| Overseas France | 82 (55.0%) | 29 (36.2%) | 63 (44.7%) | |||
| Total number of specimens (n = 374) | 150 | 81 | 143 | |||
| Specimen type | ||||||
| Vaginal swab | 115 (76.7%) | 61 (76.3%) | 83 (58.0%) | 0.400 | <0.001 | 0.021 |
| Urine | 28 (18.7%) | 12 (15.0%) | 33 (23.1%) | |||
| Rectal swab | 7 (4.6%) | 7 (8.7%) | 27 (18.9%) | |||
| Macrolide resistance | ||||||
| Resistant | 30 (20.0%) | 24 (29.6%) | 54 (37.8%) | 0.099 | <0.001 | 0.220 |
| Susceptible | 120 (80.0%) | 57 (70.4%) | 89 (62.2%) | |||
| Fluoroquinolone resistance | ||||||
| Resistant | 17 (12.5%) | 13 (17.8%) | 11 (8.3%) | 0.297 | 0.256 | 0.041 |
| Susceptible | 119 (87.5%) | 60 (82.2%) | 122 (91.7%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guiraud, J.; Helary, M.; Le Roy, C.; Elguero, E.; Pereyre, S.; Bébéar, C. Molecular Typing Reveals Distinct Mycoplasma genitalium Transmission Networks among a Cohort of Men Who Have Sex with Men and a Cohort of Women in France. Microorganisms 2022, 10, 1587. https://doi.org/10.3390/microorganisms10081587
Guiraud J, Helary M, Le Roy C, Elguero E, Pereyre S, Bébéar C. Molecular Typing Reveals Distinct Mycoplasma genitalium Transmission Networks among a Cohort of Men Who Have Sex with Men and a Cohort of Women in France. Microorganisms. 2022; 10(8):1587. https://doi.org/10.3390/microorganisms10081587
Chicago/Turabian StyleGuiraud, Jennifer, Marion Helary, Chloé Le Roy, Eric Elguero, Sabine Pereyre, and Cécile Bébéar. 2022. "Molecular Typing Reveals Distinct Mycoplasma genitalium Transmission Networks among a Cohort of Men Who Have Sex with Men and a Cohort of Women in France" Microorganisms 10, no. 8: 1587. https://doi.org/10.3390/microorganisms10081587
APA StyleGuiraud, J., Helary, M., Le Roy, C., Elguero, E., Pereyre, S., & Bébéar, C. (2022). Molecular Typing Reveals Distinct Mycoplasma genitalium Transmission Networks among a Cohort of Men Who Have Sex with Men and a Cohort of Women in France. Microorganisms, 10(8), 1587. https://doi.org/10.3390/microorganisms10081587