
Brucellosis and One Health: Inherited and Future Challenges
 , , and
, , and
Abstract
:1. Introduction
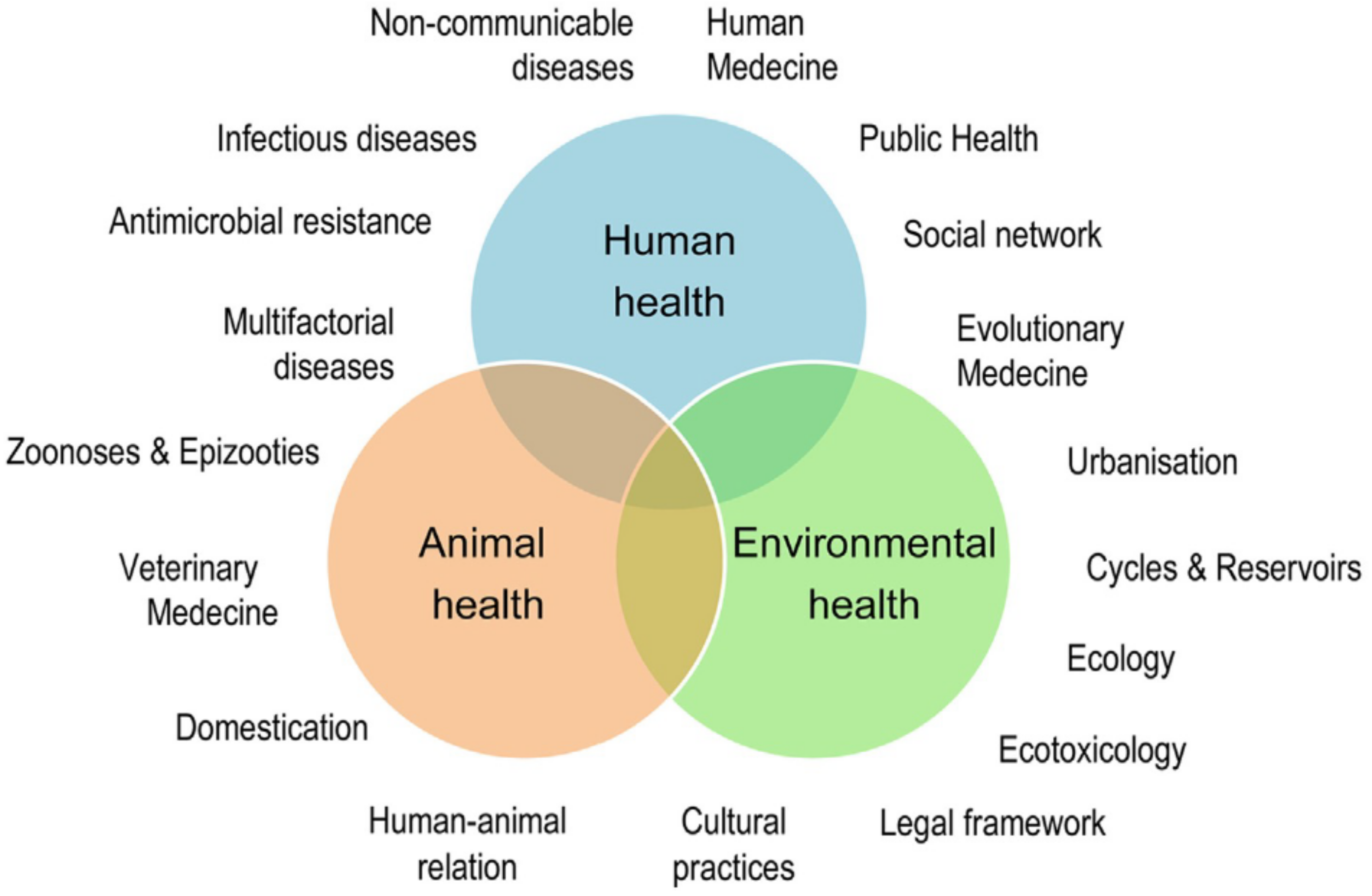
2. Is One Health a New Concept in Brucellosis?
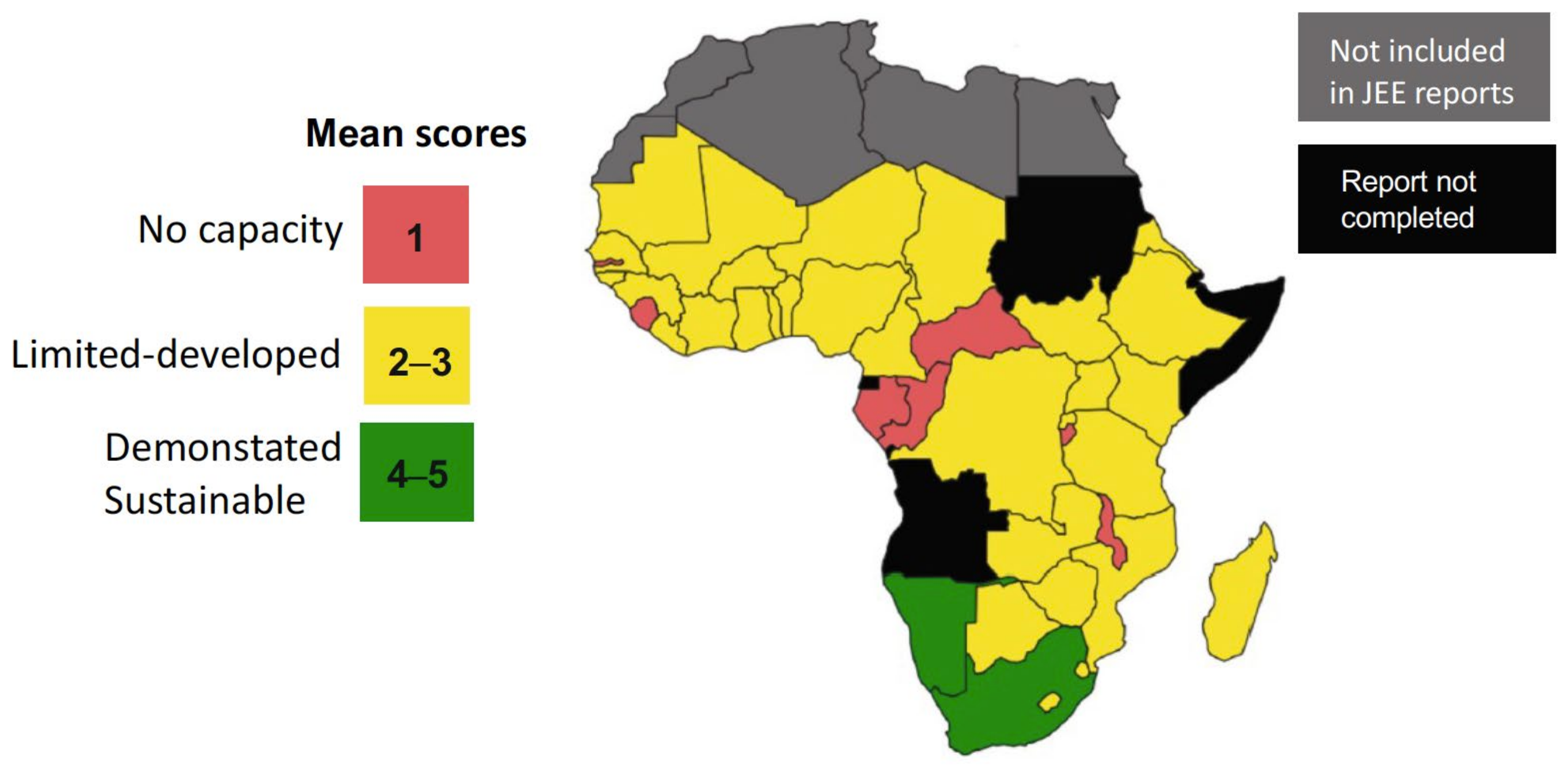
3. An Unmet Challenge: Implementing Basic One Health Structures
4. One-Health Challenges for Brucellosis
4.1. Awareness of the Disease
4.2. Geography, Climate, and Peri-Urban Growth
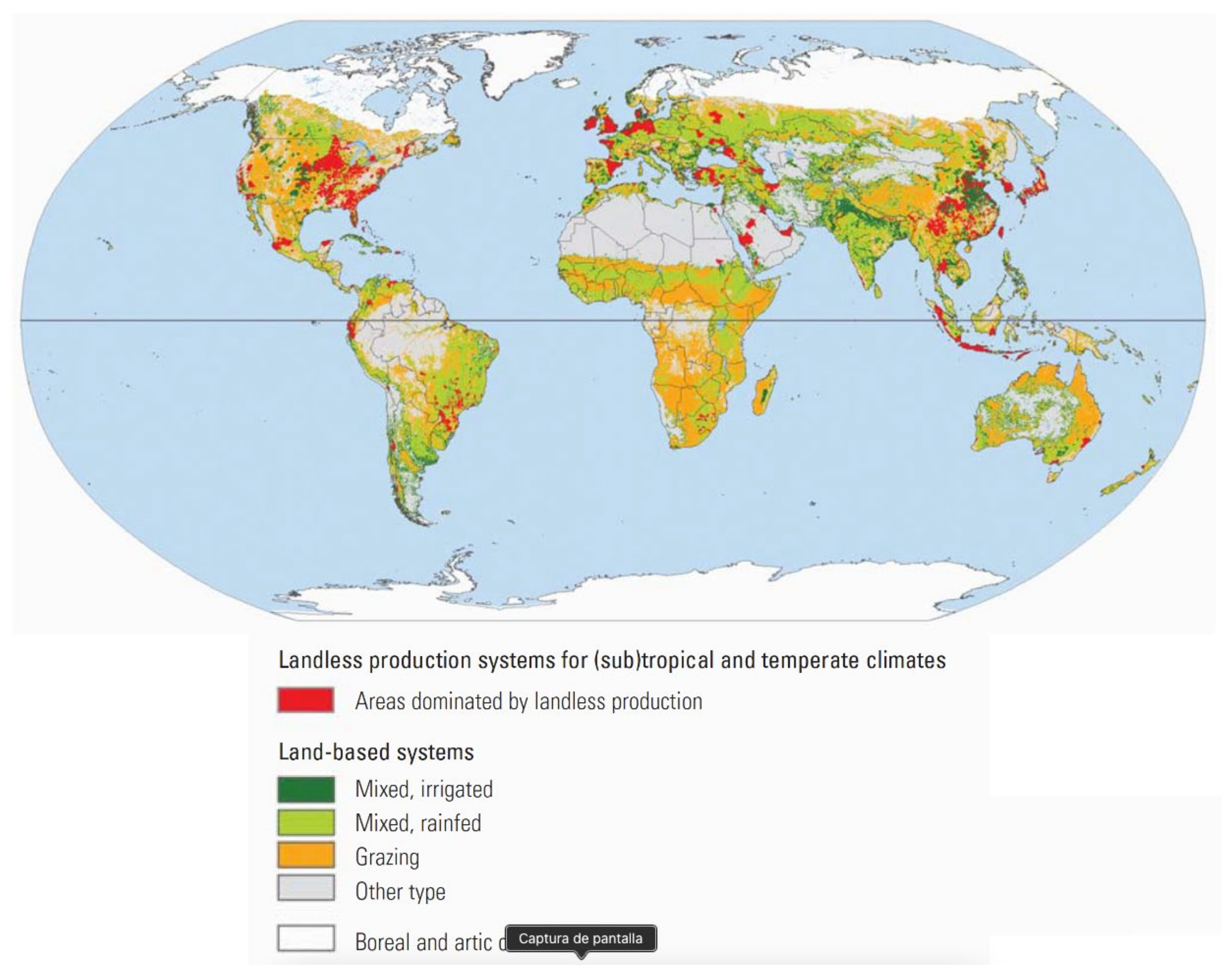
4.3. Intensification of Breeding
4.4. The overlooked Characteristics of Brucellosis
4.5. The Negative Impact of Diagnostic Test Misuse
4.6. Human Brucellosis Prevalence
4.7. Brucellosis Vaccines: Efficacy Versus the DIVA Myth
4.8. Capacity Building
4.9. Factual Technical Gaps in Diagnostics and Vaccines
4.10. Taxonomy Issues
5. The Human Factor
5.1. Building Trust in Key Brucellosis Stakeholders
5.2. Prioritization Versus Sensitization
6. Conclusions
- A.
- The deficiencies in Public Health and Veterinary Services and their cooperation.
- B.
- Insufficient awareness.
- C.
- The challenges related to geography and climate.
- D.
- The intensification of issues to meet food demands.
- E.
- Misconceptions about the disease, diagnostic tools and vaccines.
- F.
- Research on diagnostics and vaccines for water buffaloes, camels, yacks, etc.
- G.
- Capacity-building.
- H.
- The human condition: care for others, building trust and social justice.
Funding
Conflicts of Interest
References
- Whatmore, A.M.; Foster, J.T. Emerging diversity and ongoing expansion of the genus Brucella. Infect. Gen. Evol. 2021, 92, 104865. [Google Scholar]
- Corbel, M.J.; Alton, G.G.; Banai, M.; Díaz, R.; Dranovskaia, B.A.; Elberg, S.S.; Garin-Bastuji, B.; Kolar, J.; Mantovani, A.; Mousa, A.M.; et al. Brucellosis in Humans and Animals; WHO Press: Geneva, Switzerland, 2006. [Google Scholar]
- Moreno, E.; Blasco, J.M.; Moriyón, I. Facing the human and animal brucellosis conundrums: The forgotten lessons. Microorganisms 2022, 10, 942. [Google Scholar] [PubMed]
- Laine, C.G.; Scott, H.M.; Arenas-Gamboa, Á. Human brucellosis: Widespread information deficiency hinders an understanding of global disease frequency. PLoS Negl. Trop. Dis. 2022, 16, e0010404. [Google Scholar]
- Completed OHZDP Workshops. Available online: https://www.cdc.gov/onehealth/what-we-do/zoonotic-disease-prioritization/completed-workshops.html (accessed on 4 April 2023).
- World Animal Health Information System. Available online: https://www.woah.org/en/what-we-do/animal-health-and-welfare/disease-data-collection/world-animal-health-information-system/ (accessed on 5 July 2023).
- Ghanbari, M.K.; Gorji, H.A.; Behzadifar, M.; Sanee, N.; Mehedi, N.; Bragazzi, N.L. One health approach to tackle brucellosis: A systematic review. Trop. Med. Health 2020, 48, 86. [Google Scholar] [CrossRef]
- Carugati, M.; Kilonzo, K.G.; Crump, J.A. Fever, bacterial zoonoses, and One Health in sub-Saharan Africa. Clin. Med. 2019, 19, 375–380. [Google Scholar]
- Moreno, E. The one hundred year journey of the genus Brucella (Meyer and Shaw 1920). FEMS Microb. Rev. 2020, 45, fuaa045. [Google Scholar] [CrossRef]
- Roop, R.M.; Barton, I.S.; Hopersberger, D.; Martin, D.W. Uncovering the hidden credentials of Brucella virulence. Microbiol. Mol. Biol. Rev. 2021, 85, e00021-19. [Google Scholar]
- Kahn, L.H.; Kaplan, B.; Steele, J.H. Confronting zoonoses through closer collaboration between medicine and veterinary medicine (as ‘one medicine’). Vet. Ital. 2007, 43, 5–19. [Google Scholar]
- Plumb, G.; Olsen, S.; Pappas, G. Brucellosis: Recent developments towards ‘One Health’. Rev. Sci. Tech. Off. Int. Epiz 2013, 32, 13–16. [Google Scholar]
- Kaplan, B. ‘One Medicine—One Health’: An Historic Perspective. 2021. Available online: https://onehealthinitiative.com/wp-content/uploads/2022/08/One-Medicine-One-Health-An-Historic-Perspective-REVISED-SEPT1-2022-from-FEB1-2021.pdf (accessed on 11 July 2023).
- Spink, W.W. The evolution of the concept that brucellosis is a disease of animals and man. In The Nature of Brucellosis; The University of Minnesota Press: Minneapolis, MN, USA, 1956; pp. 3–27. [Google Scholar]
- Abutarbush, S.M.; Hamdallah, A.; Hawawsheh, M.; Alsawalha, L.; Elizz, N.A.; Dodeen, R. Implementation of One Health approach in Jordan: Review and mapping of ministerial mechanisms of zoonotic disease reporting and control, and inter-sectoral collaboration. One Health 2022, 15, 100406. [Google Scholar]
- Buttigieg, S.C.; Savic, S.; Cauchi, D.; Lautier, E.; Canali, M.; Aragrande, M. Brucellosis control in Malta and Serbia: A One Health evaluation. Front. Vet. Sci. 2018, 5, 147. [Google Scholar] [CrossRef] [PubMed]
- Erkyihun, G.A.; Gari, F.R.; Edao, B.M.; Kassa, G.M. A review on One Health approach in Ethiopia. One Health Outlook 2022, 4, 8. [Google Scholar] [CrossRef] [PubMed]
- Hermesh, B.; Rosenthal, A.; Davidovitch, N. Rethinking “One Health” through brucellosis: Ethics, boundaries and politics. Monash Bioeth. Rev. 2019, 37, 22–37. [Google Scholar] [PubMed]
- Lindahl, J.F.; Vrentas, C.E.; Deka, R.P.; Hazarika, R.A.; Rahman, H.; Bambal, R.G.; Bedi, J.S.; Bhattacharya, C.; Chaduhuri, P.; Fairoze, N.M.; et al. Brucellosis in India: Results of a collaborative workshop to define One Health priorities. Trop. Anim. Health Prod. 2019, 52, 387–396. [Google Scholar]
- Munyua, P.M.; Njenga, M.K.; Osoro, E.M.; Onyango, C.O.; Bitek, A.O.; Mwatondo, A.; Muturi, M.K.; Musee, N.; Bigogo, G.; Otiang, E.; et al. Successes and challenges of the One Health approach in Kenya over the last decade. BMC Public Health 2019, 19, 465. [Google Scholar] [CrossRef]
- Nantima, N.; Ilukor, J.; Kaboyo, W.; Ademun, A.R.O.; Muwanguzi, D.; Sekamatte, M.; Sentumbwe, J.; Monje, F.; Bwire, G. The importance of a One Health approach for prioritising zoonotic diseases to focus on capacity-building efforts in Uganda. Rev. Sci. Tech. Off. Int. Epiz. 2019, 38, 315–325. [Google Scholar]
- Zhou, K.; Wu, B.; Pan, H.; Paudyal, N.; Jiang, J.; Zhang, L.; Li, Y.; Yue, M. One Health approach to address zoonotic brucellosis: A spatiotemporal associations study between animals and humans. Front. Vet. Sci. 2020, 7, 521. [Google Scholar] [CrossRef]
- Destoumieux-Garzón, D.; Mavingui, P.; Boetsch, G.; Boissier, J.; Darriet, F.; Duboz, P.; Fritsch, C.; Giraudoux, P.; Roux, F.L.; Morand, S.; et al. The One Health concept: 10 years old and a long road ahead. Front. Vet. Sci. 2018, 5, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Joint External Evaluation Tool (Second Edition). Available online: https://www.who.int/publications/i/item/9789240051980 (accessed on 5 May 2023).
- OIE. PVS Pathway. Available online: https://www.woah.org/en/what-we-offer/improving-veterinary-services/pvs-pathway/evaluation/pvs-evaluation-reports/ (accessed on 25 May 2023).
- Elton, L.; Haider, N.; Kock, R.; Thomason, M.J.; Tembo, J.; Arruda, L.B.; Ntoumi, F.; Zumla, A.; Mchugh, T.D. Zoonotic disease preparedness in sub-Saharan African countries. One Health Outlook 2021, 3, 5. [Google Scholar] [CrossRef]
- Stratton, J.; Tagliaro, E.; Weaver, J.; Sherman, D.M.; Carron, M.; Di Giacinto, A.; Sharandak, V.; Caya, F. Performance of Veterinary Services Pathway evolution and One Health aspects. Rev. Sci. Tech. Off. Int. Epiz. 2019, 38, 291–302. [Google Scholar]
- OIE. PVS Pathway. Available online: https://extranet.who.int/sph/woah-pvs-pathway (accessed on 11 July 2023).
- Maxwell, M.J.; Freire de Carvalho, M.H.; Hoet, A.E.; Vigilato, M.A.N.; Pompei, J.C.; Cosivi, O.; del Rio Vilas, V.J. Building the road to a regional zoonoses strategy: A survey of zoonoses programmes in the Americas. PLoS ONE 2017, 12, e0174175. [Google Scholar]
- Jamil, T.; Khan, A.U.; Saqib, M.; Hussain, M.H.; Melzer, F.; Rehman, A.; Shabbir, M.Z.; Khan, M.A.; Ali, S.; Shahzad, A.; et al. Animal and human brucellosis in Pakistan. Front. Public Health 2021, 9, 660508. [Google Scholar] [PubMed]
- Haken, N.; Woodburn, D.; Gallo-Carelli, J.; Cooper, A.; Souquet Moglen, D.; Faborode, J.; Asfaw, Y.; Wilson, W.; Turner, P.; Duvor, C.; et al. Fragile States Index 2022—Annual Report. Washington, DC, USA. 2022. Available online: https://fragilestatesindex.org/2022/07/13/fragile-states-index-2022-annual-report/ (accessed on 23 May 2023).
- Solera, J.; Martínez, A.E.; Espinosa, A.; Castillejos, M.L.; Geijo, P.; Rodríguez-Zapata, M. Multivariate model for predicting relapse in human brucellosis. J. Infect. 1998, 36, 85–92. [Google Scholar]
- Zhang, N.; Zhou, H.; Huang, D.S.; Guan, P. Brucellosis awareness and knowledge in communities worldwide: A systematic review and meta-analysis of 79 observational studies. PLoS Negl. Trop. Dis. 2019, 13, e0007366. [Google Scholar] [CrossRef]
- World Population by Country. Available online: https://worldpopulationreview.com (accessed on 6 July 2023).
- Cook, R. World Cattle Inventory by Country. Available online: https://beef2live.com/story-world-cattle-inventory-country-644-106898 (accessed on 10 July 2023).
- Hegde, N.G. Livestock development for sustainable livelihood of small farmers. Asian J. Res. Anim. Vet. Sci. 2019, 3, 1–17, article no. AJRAVS.48871; available at SSRN 4345390. [Google Scholar]
- Steinfeld, H.; Wassenaar, T.; Jutzi, S. Livestock production systems in developing countries: Status, drivers, trends. Rev. Sci. Tech. Off. Int. Epiz. 2006, 25, 505–516. [Google Scholar]
- Africa Center for Strategic Studies. Surge in Militant Islamist Violence in the Sahel Dominates Africa’s Fight Against Extremists. Available online: https://africacenter.org/spotlight/mig2022-01-surge-militant-islamist-violence-sahel-dominates-africa-fight-extremists/ (accessed on 6 July 2023).
- Perry, B.D.; Grace, D.; Sones, K. Current drivers and future directions of global livestock disease dynamics. Proc. Nat. Acad. Sci. USA 2011, 110, 20871–20877. [Google Scholar]
- Jones, P.G.; Thornton, P.K. Croppers to livestock keepers: Livelihood transitions to 2050 in Africa due to climate change. Environ. Sci. Policy 2009, 12, 427–437. [Google Scholar]
- Torres, C.; van Seters, J.; Karaki, K.; Kpadonou, R. An Exploratory Analysis of Measures to Make Trade Facilitation Work for Inclusive Regional Agro-Food Value Chains in West Africa. ECDPM Discussion Paper 214; ECDPM Discussion Paper 214. Available online: https://ecdpm.org/work/an-exploratory-analysis-of-measures-to-make-trade-facilitation-work-for-inclusive-regional-agro-food-value-chains-in-west-africa (accessed on 5 May 2023).
- Chirisa, I. Peri-urban dynamics and regional planning in Africa: Implications for building healthy cities. J. Afr. Stud. Dev. 2010, 2, 16–25. [Google Scholar]
- United Nations Human Settlements Programme UN Habitat. State of African Cities. Re-Imagining Sustainable Urban Transitions. United Nations Human Settlements Programme, Nairobi. 2014. Available online: https://unhabitat.org/sites/default/files/download-manager-files/StateofAfricanCities2014.pdf (accessed on 5 July 2023).
- Ducrotoy, M.J.; Bertu, W.J.; Ocholi, R.A.; Gusi, A.M.; Bryssinckx, W.; Welburn, S.; Moriyón, I. Brucellosis as an emerging threat in developing economies: Lessons from Nigeria. PLoS Negl. Trop. Dis. 2014, 8, e3008. [Google Scholar]
- Jones, B.A.; Grace, D.; Kock, R.; Alonso, S.; Rushton, J.; Said, M.Y.; McKeever, D.; Mutua, F.; Young, J.; McDermott, J.J.; et al. Zoonosis emergence linked to agricultural intensification and environmental change. Proc. Nat. Acad. Sci. USA 2013, 110, 8399–8404. [Google Scholar] [PubMed]
- Dairy-Global. Going Bigger! Big Scale Dairy Farming a Main Trend in China. Available online: https://www.dairyglobal.net/world-of-dairy/farm-visits/going-bigger-big-scale-dairy-farming-a-main-trend-in-china/ (accessed on 7 July 2023).
- Riley, J. China Builds 100,000-Cow Dairy Unit to Supply Russian Market. Farmers Weekly 6 July 2015. Available online: https://www.fwi.co.uk/livestock/dairy/china-building-100000-cow-dairy-unit-supply-russian-market (accessed on 6 July 2023).
- Blasco, J.M.; Moreno, E.; Moriyón, I. Brucellosis vaccines and vaccine candidates. In Veterinary Vaccines. Principles and Applications, 1st ed.; Metwally, S., Viljoen, G.J., El Idrissi, A., Eds.; FAO: Rome, Italy; Wiley & Sons: Hobeken, NJ, USA, 2021; pp. 295–316. [Google Scholar]
- Ran, X.; Cheng, J.; Wang, M.; Chen, X.; Wang, H.; Ge, Y.; Ni, H.; Zhang, X.X.; Wen, X. Brucellosis seroprevalence in dairy cattle in China during 2008–2018: A systematic review and meta-analysis. Acta Trop. 2019, 189, 117–123. [Google Scholar] [PubMed]
- Ducrotoy, M.J.; Muñoz, P.M.; Conde-Álvarez, R.; Blasco, J.M.; Moriyón, I. A systematic review of current immunological tests for the diagnosis of cattle brucellosis. Prev. Vet. Med. 2018, 151, 57–72. [Google Scholar] [PubMed]
- Davies, G.O. Gaiger and Davies’ Veterinary Pathology and Bacteriology; Bailliere, Tindall and Cox: London, UK, 1946. [Google Scholar]
- Ducrotoy, M.J.; Bertu, W.J.; Matope, G.; Cadmus, S.; Conde-Álvarez, R.; Gusi, A.M.; Welburn, S.; Ocholi, R.; Blasco, J.M.; Moriyón, I. Brucellosis in Sub-Saharan Africa: Current challenges for management, diagnosis and control. Acta Trop. 2017, 165, 179–193. [Google Scholar] [PubMed]
- Troupin, C.; Ellis, I.; Doukouré, B.; Camara, A.; Keita, M.; Kagbadouno, M.; Bart, J.-M.; Diallo, R.; Lacôte, S.; Marianneau, P.; et al. Seroprevalence of brucellosis, Q fever and Rift Valley fever in domestic ruminants in Guinea in 2017–2019. BMC Vet. Res. 2022, 18, 64. [Google Scholar] [CrossRef]
- Al-Marzooqi, W.; Elshafie, E.I.; Al-Toobi, A.; Al-Hamrashdi, A.; Al-Kharousi, K.; El-Tahir, H.; Jay, M.; Corde, Y.; ElTahir, Y. Seroprevalence and risk factors of brucellosis in ruminants in Dhofar province in Southern Oman. Vet. Med. Int. 2022, 2022, 3176147. [Google Scholar] [CrossRef]
- Etefa, M.; Kabeta, T.; Merga, D.; Debelo, M. Cross-sectional study of seroprevalence and associated risk factors of bovine brucellosis in selected districts of Jimma zone, South Western Oromia, Ethiopia. BioMed. Res. Int. 2022, 2022, 9549942. [Google Scholar] [CrossRef]
- Munsi, N.; Rahman, H. Seroprevalence of brucellosis in goats in some selected areas of Bangladesh. Adv. Vet. Anim. Res. 2021, 8, 123–128. [Google Scholar]
- Geletu, U.S.; Usmael, M.A.; Mummed, Y.Y. Seroprevalence and risk factors of small ruminant brucellosis in West Hararghe Zone of Oromia Regional State, Eastern Ethiopia. Vet. Med. Int. 2021, 2021, 6671554. [Google Scholar] [CrossRef] [PubMed]
- Ebid, M.; El Mola, A.; Salib, F. Seroprevalence of brucellosis in sheep and goats in the Arabian Gulf region. Vet. World 2020, 13, 1495–1509. [Google Scholar]
- Hassan, H.; Salami, A.; Ghssein, G.; El-Hage, J.; Nehme, N.; Awada, R. Seroprevalence of Brucella abortus in cattle in Southern Lebanon using different diagnostic tests. Vet. World 2020, 13, 2234–2242. [Google Scholar]
- Khan, A.U.; Melzer, F.; Hendam, A.; Sayour, A.E.; Khan, I.; Elschner, M.C.; Younus, M.; Ehtisham-Ul-Haque, S.; Waheed, U.; Farooq, M.; et al. Seroprevalence and molecular identification of Brucella spp. in bovines in Pakistan-investigating association with risk factors using machine learning. Front. Vet. Sci 2020, 7, 594498. [Google Scholar] [CrossRef] [PubMed]
- Nguna, J.; Dione, M.; Apamaku, M.; Majalija, S.; Mugizi, D.R.; Odoch, T.; Kato, C.D.; Tumwine, G.; Kabaasa, J.D.; Curtis, K.; et al. Seroprevalence of brucellosis and risk factors associated with its seropositivity in cattle, goats and humans in Iganga District, Uganda. Pan Afr. Med. J. 2019, 33, 99. [Google Scholar] [CrossRef]
- Selim, A.; Attia, K.; Ramadan, E.; Hafez, Y.M.; Salman, A. Seroprevalence and molecular characterization of Brucella species in naturally infected cattle and sheep. Prev. Vet. Med. 2019, 171, 104756. [Google Scholar] [CrossRef]
- Bhandi, S.; Pfukenyi, D.M.; Matope, G.; Murondoti, A.; Tivapasi, M.; Ndengu, M.; Scacchia, M.; Bonfini, B.; de Garine-Wichatitsky, M. Brucellosis and chlamydiosis seroprevalence in goats at livestock–wildlife interface areas of Zimbabwe. Onderstepoort J. Vet. Res. 2019, 86, a1670. [Google Scholar] [CrossRef]
- Olufemi, O.T.; Dantala, D.B.; Shinggu, P.A.; Dike, U.A.; Otolorin, G.R.; Nwuku, J.A.; Baba-Onoja, E.B.T.; Jatau, T.D.; Amama, F.I. Seroprevalence of brucellosis and associated risk factors among indigenous breeds of goats in Wukari, Taraba State, Nigeria. J. Pathog. 2018, 2018, 5257926. [Google Scholar] [CrossRef] [Green Version]
- Robi, D.T.; Urge, B.; Bogale, A.; Aleme, M.; Temteme, S. Herd and animal level seroprevalence and associated risk factors of bovine brucellosis in different agro-ecologies of southwest Ethiopia. Heliyon 2023, 9, e16852. [Google Scholar] [CrossRef]
- Merga Sima, D.; Abdeta Ifa, D.; Merga, A.L.; Tola, E.H. Seroprevalence of bovine brucellosis and associated risk factors in Western Ethiopia. Vet. Med. 2021, 12, 317–324. [Google Scholar]
- Mfune, R.L.; Mubanga, M.; Silwamba, I.; Sagamiko, F.; Mudenda, S.; Daka, V.; Godfroid, J.; Hangombe, B.M.; Muma, J.B. Seroprevalence of bovine brucellosis in selected districts of Zambia. Int. J. Eviron. Res. Public Health 2021, 18, 1436. [Google Scholar] [CrossRef]
- Carbonero, A.; Guzmán, L.T.; García-Bocanegra, I.; Borge, C.; Adaszek, L.; Arenas, A.; Saa, L.R. Seroprevalence and risk factors associated with Brucella seropositivity in dairy and mixed cattle herds from Ecuador. Trop. Anim. Health Prod. 2017, 50, 197–203. [Google Scholar]
- Ramdani, N.; Boussena, S.; Bouaziz, O.; Moula, N. Brucellosis in small ruminant: Seroprevalence, risk factors, and distribution in the southeast of Algeria. Trop. Anim. Health Prod. 2022, 54, 245. [Google Scholar] [CrossRef]
- Shome, R.; Kalleshamurthy, T.; Rathore, Y.; Ramanjinappa, K.D.; Skariah, S.; Nagaraj, C.; Mohandoss, N.; Sahay, S.; Shome, B.R.; Kuralayanapalya, P.S.; et al. Spatial sero-prevalence of brucellosis in small ruminants of India: Nationwide cross-sectional study for the year 2017–2018. Transbound. Emerg. Dis. 2021, 68, 2199–2208. [Google Scholar]
- Enström, S.; Nthiwa, D.; Bett, B.; Karlsson, A.; Alonso, S.; Lindahl, J.F. Brucella seroprevalence in cattle near a wildlife reserve in Kenya. BMC Res. Notes 2017, 10, e0120761. [Google Scholar] [CrossRef]
- Chaulagain, R.; Bowen, R.A. Seroprevalence and epidemiological study of bovine brucellosis in dairy cattle of Kavrepalanchowk district of Nepal. Nepal. J. Agric. Sci. 2016, 14, 123–131. [Google Scholar]
- Negash, W.; Dubie, T. Study on seroprevalence and associated factors of bovine brucellosis in selected districts of Afar National Regional State, Afar, Ethiopia. Vet. Med. Int. 2021, 2021, 8829860. [Google Scholar] [CrossRef]
- Traoré, S.; Yapi, R.B.; Coulibaly, K.; Mathew, C.; Fokou, G.; Kazwala, R.R.; Bonfoh, B.; Alambedji, R.B. Seroprevalence of brucellosis in small ruminants and related risk behaviours among humans in different husbandry systems in Mali. PLoS ONE 2021, 16, e0245283. [Google Scholar]
- Ali, S.; Akhter, S.; Neubauer, H.; Melzer, F.; Khan, I.; Abatih, E.N.; El-Adawy, H.; Irfan, M.; Muhammad, A.; Akbar, M.W.; et al. Seroprevalence and risk factors associated with bovine brucellosis in the Potohar Plateau, Pakistan. BMC Res. Notes 2017, 10, 73. [Google Scholar] [CrossRef] [Green Version]
- Asgedom, H.; Damena, D.; Duguma, R. Seroprevalence of bovine brucellosis and associated risk factors in and around Alage district, Ethiopia. SpringerPlus 2016, 5, 851. [Google Scholar] [CrossRef] [Green Version]
- Godfroid, J.; Al Dahouk, S.; Pappas, G.; Roth, F.; Matope, G.; Muma, J.; Marcotty, T.; Pfeiffer, D.; Skjerve, E.; Al-Dahouk, S.; et al. A “One Health” surveillance and control of brucellosis in developing countries: Moving away from improvisation. Comp. Immunol. Microbiol. Infect. Dis. 2013, 36, 241–248. [Google Scholar]
- Verger, J.M.B. melitensis infection of cattle. In Brucella melitensis; Verger, J.M., Plommet, M., Eds.; Martinus Nijhoff: Dordrech, Holland, 1985; pp. 197–203. [Google Scholar]
- Taleski, V.; Zerva, L.; Kantardjiev, T.; Cvetnic, Z.; Erski-Biljic, M.; Nikolovski, B.; Bosnjakovski, J.; Katalinic-Jankovic, V.; Panteliadou, A.; Stojkoski, S.; et al. An overview of the epidemiology and epizootiology of brucellosis in selected countries of Central and Southeast Europe. Vet. Microbiol. 2002, 90, 147–155. [Google Scholar] [PubMed]
- Al-Mariri, A. Isolation of Brucella melitensis strains from Syrian bovine milk samples. Bulg. J. Vet. Med. 2015, 18, 40–48. [Google Scholar]
- De Massis, F.; Zilli, K.; Donato, G.D.; Nuvoloni, R.; Pelini, S.; Sacchini, L.; D’Alterio, N.; Giannatale, E.D. Distribution of Brucella field strains isolated from livestock, wildlife populations, and humans in Italy from 2007 to 2015. PLoS ONE 2019, 14, e0213689. [Google Scholar]
- Wareth, G.; El-Diasty, M.; Melzer, F.; Schmoock, G.; Moustafa, S.A.; El-Beskawy, M.; Khater, D.F.; Hamdy, M.E.R.; Zaki, H.M.; Ferreira, A.C.; et al. MLVA-16 Genotyping of Brucella abortus and Brucella melitensis isolates from different animal species in Egypt: Geographical relatedness and the Mediterranean lineage. Pathogens 2020, 9, 498. [Google Scholar]
- Bardenstein, S.; Grupel, D.; Blum, S.E.; Motro, Y.; Moran-Gilad, J. Public and animal health risks associated with spillover of Brucella melitensis into dairy farms. Microb. Genom. 2023, 9, 001014. [Google Scholar]
- Alton, G.G.; Jones, L.M.; Angus, R.D.; Verger, J.M. Techniques for the Brucellosis Laboratory; INRA: Paris, France, 1988. [Google Scholar]
- OIE. Brucellosis (Infection with B. abortus, B. melitensis and B. suis). In OIE Manual of Diagnostic Tests and Vaccines for Terrestrial Animals (Chapter 3.1.4.); OIE: Paris, France, 2022. [Google Scholar]
- Behroozikhah, A.M.; Asli, E.; Hossani, S.D.; Etemadi, A.; Dadar, M. SWOT analysis of Brucella abortus antigens (S99) production in Iran. In Proceedings of the Iran’s 21st International Congress of Microbiology 2021, Theran, Iran, 17–20 August 2020. [Google Scholar]
- Falzon, L.C.; Traoré, S.; Kallo, V.; Assamoi, J.-B.; Bonfoh, B.; Schelling, E. Evaluation of the fluorescence polarization assay as a rapid on-spot test for ruminant brucellosis in Côte d’Ivoire. Front. Vet. Sci. 2019, 6, 287. [Google Scholar] [CrossRef] [PubMed]
- Mengele, I.J.; Shirima, G.M.; Bwatota, S.F.; Motto, S.K.; Bronsvoort, B.M.C.; Komwihangilo, D.M.; Lyatuu, E.; Cook, E.A.J.; Hernandez-Castro, L.E. The status and risk factors of brucellosis in smallholder dairy cattle in selected regions of Tanzania. Vet. Sci 2023, 10, 155. [Google Scholar] [CrossRef]
- Guesmi, K.; Kalthoum, S.; Mamlouk, A.; Baccar, M.N.; BelHajMohamed, B.; Hajlaoui, H.; Toumi, A.; Cherni, J.; Seghaier, C.; Messadi, L. Seroprevalence of zoonotic abortive diseases and their associated risk factors in Tunisian sheep. BMC Vet. Res 2023, 19, 50. [Google Scholar] [CrossRef]
- Siengsanan-Lamont, J.; Kong, L.; Heng, T.; Khoeun, S.; Tum, S.; Selleck, P.W.; Gleeson, L.J.; Blacksell, S.D. Risk mapping using serologic surveillance for selected One Health and transboundary diseases in Cambodian goats. PLoS Negl. Trop. Dis 2023, 17, e0011244. [Google Scholar]
- Robi, D.T.; Bogale, A.; Urge, B.; Aleme, M.; Temteme, S. Neglected zoonotic bacteria causes and associated risk factors of cattle abortion in different agro-ecological zones of southwest Ethiopia. Vet. Immunol. Immunopathol. 2023, 259, 110592. [Google Scholar]
- Tialla, D. The first study on seroprevalence and risk factors for zoonotic transmission of ovine and caprine brucellosis in the Province of Bam, Burkina Faso. Vet. World 2022, 15, 262–267. [Google Scholar]
- Ntivuguruzwa, J.B.; Babaman Kolo, F.; Mwikarago, E.I.; van Heerden, H. Seroprevalence of brucellosis and molecular characterization of Brucella spp. from slaughtered cattle in Rwanda. PLoS ONE 2022, 17, e0261595. [Google Scholar]
- Muema, J.; Oboge, H.; Mutono, N.; Makori, A.; Oyugi, J.; Bukania, Z.; Njuguna, J.; Jost, C.; Ogoti, B.; Omulo, S.; et al. Sero—Epidemiology of brucellosis in people and their livestock: A linked human—Animal cross-sectional study in a pastoralist community in Kenya. Front. Vet. Sci. 2022, 9, 1031639. [Google Scholar] [PubMed]
- Baltazar-Pérez, J.; Utrera-Quintana, F.; Camacho-Ronquillo, J.; González-Garduño, R.; Jiménez-Cortez, H.; Villa-Mancera, A. Prevalence of Neospora caninum, Toxoplasma gondii and Brucella abortus in water buffalo (Bubalus bubalis): Climatic and environmental risk factors in eastern and southeast Mexico. Microb. Pathog. 2022, 173, 105871. [Google Scholar] [PubMed]
- Lokamar, P.N.; Kutwah, M.A.; Munde, E.O.; Oloo, D.; Atieli, H.; Gumo, S.; Akoko, J.M.; Ouma, C. Prevalence of brucellosis in livestock keepers and domestic ruminants in Baringo County, Kenya. PLoS Glob. Public Health 2022, 2, e0000682. [Google Scholar]
- Aghamohammad, S.; Rastin, M.; Mostafavi, E.; Anaraki, A.H.; Rahravani, M.; Sadaf, R.A.; Moravedji, M.; Rohani, M. Determination of seroprevalence of brucellosis in livestock and high-risk population in Kurdistan, Western Iran. Comp. Immunol. Microbiol. infect. Dis. 2022, 93, 101942. [Google Scholar] [PubMed]
- Adabi, M.; Khazaiee, S.; Sadeghi-Nasab, A.; Alamian, S.; Arabestani, M.R.; Valiei, Z.; Gharekhani, J. Brucellosis in livestock: First study on seroepidemiology, risk factors, and preventive strategies to manage the disease in Famenin, Iran. Vet. World 2022, 15, 2102–2110. [Google Scholar]
- Subekti, D.T.; Fatmawati, M.; Khoiriyah, A.; Pramesthi, A.; Fong, S.; Desem, M.I.; Azmi, Z.; Kusumaningtyas, E.; Endrawati, D.; Purwanto, E.S. Seroprevalence of seven reproductive diseases in beef and dairy cows from three provinces in Indonesia. Vet. Med. Int. 2021, 2021, 6492289. [Google Scholar] [CrossRef]
- Mohamud, A.S.; Kothowa, J.P.; Mfune, R.L.; Mubanga, M.; Godfroid, J.; Muma, J.B. Seroprevalence and risk factors associated with Brucella infection in camels in the Puntland State of Somalia. Vet. Sci. 2021, 8, 137. [Google Scholar]
- Marami, L.M.; Gebremedhin, E.Z.; Sarba, E.J.; Tola, G.K.; Endalew, S.S.; Melkamsew, A.T.; Di Marco Lo Presti, V.; Vitale, M. Seroprevalence and associated risk factors of canine Leptospira and Brucella species infection in West Shewa Zone, Central Ethiopia. Vet. Med. 2021, 12, 33–42. [Google Scholar]
- Khan, M.R.; Rehman, A.; Khalid, S.; Ahmad, M.U.D.; Avais, M.; Sarwar, M.; Awan, F.N.; Melzer, F.; Neubauer, H.; Jamil, T. Seroprevalence and associated risk factors of bovine brucellosis in district Gujranwala, Punjab, Pakistan. Animals 2021, 11, 1744. [Google Scholar] [CrossRef]
- Khan, A.U.; Sayour, A.E.; Melzer, F.; El-soally, S.A.G.E.; Elschner, M.C.; Shell, W.S.; Moawad, A.A.; Mohamed, S.A.; Hendam, A.; Roesler, U.; et al. Seroprevalence and molecular identification of Brucella spp. in camels in Egypt. Microorganisms 2020, 8, 1035. [Google Scholar] [CrossRef] [PubMed]
- Nthiwa, D.; Alonso, S.; Odongo, D.; Kenya, E.; Bett, B. Zoonotic pathogen seroprevalence in cattle in a wildlife–livestock interface, Kenya. EcoHealth 2019, 16, 712–725. [Google Scholar] [PubMed] [Green Version]
- Lindahl, J.F.; Gill, J.P.S.; Hazarika, R.A.; Fairoze, N.M.; Bedi, J.S.; Dohoo, I.; Chauhan, A.S.; Grace, D.; Kakkar, M. Risk factors for Brucella seroprevalence in peri-urban dairy farms in five Indian cities. Trop. Med. Infect. Dis. 2019, 4, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peck, M.E.; Chanachai, K.; Jenpanich, C.; Amonsin, A.; Alexander, B.H.; Bender, J.B. Seroprevalence of brucellosis in goats and sheep in Thailand: Results from the Thai National brucellosis surveillance system from 2013 to 2015. Transbound. Emerg. Dis. 2018, 65, 799–805. [Google Scholar] [PubMed]
- Wolff, C.; Boqvist, S.; Ståhl, K.; Masembe, C.; Sternberg-Lewerin, S. Biosecurity aspects of cattle production in Western Uganda, and associations with seroprevalence of brucellosis, salmonellosis and bovine viral diarrhoea. BMC Vet. Res. 2017, 13, 382. [Google Scholar]
- Tarusikirwa, D.F.; Blacklaws, B.; Trotter, C.L. Seroprevalence and assessment of public awareness of Brucella spp., Toxoplasma gondii and Chlamydia abortus in small ruminants from selected smallholder commercial farms of Zimbabwe. PLoS ONE 2023, 18, e0287902. [Google Scholar]
- Almuzaini, A.M. An epidemiological study of brucellosis in different animal species from the Al-qassim region, Saudi Arabia. Vaccines 2023, 11, 694. [Google Scholar] [CrossRef]
- Getahun, T.; Urge, B.; Mamo, G. Seroprevalence of bovine brucellosis in selected sites of Central Highland of Ethiopia. Vet. Med. 2023, 14, 11–22. [Google Scholar] [CrossRef]
- Shurbe, M.; Wondimu, A.; Eshetu, N.; Seyoum, W.; Tora, E.; Simeon, B.; Rufael, T.; Sombo, M. Detection of antibodies against brucellosis and associated risk factors in cross breed dairy cattle in smallholder farmers, Southern Ethiopia. Vet. Med. 2023, 14, 23–33. [Google Scholar] [CrossRef]
- Faddane, K.; Moumni, H.; Cherkaoui, I.; Lakranbi, M.; Hamdi, S.; Ezzikouri, S.; Saile, R.; Azhari, M.E. Seroprevalence of human brucellosis in Morocco and associated risk factors. Vet. World 2022, 15, 2224–2233. [Google Scholar] [CrossRef]
- Araújo, L.C.S.S.C.; Costa, M.M.; Nascimento Junior, J.A.; Silva, F.D.A.; Peixoto, R.M. Bovine brucellosis seroprevalence and flow network analysis in slaughterhouses in the state of Ceará. Rev. Brasil. Med. Vet. 2022, 44, e003521. [Google Scholar] [CrossRef]
- Tilahun, A.; Kegno, S.; Adugma, T.; Mamuye, D. A seroprevalence study of brucellosis in boran (zebu) breeds of pastoral area. Vet. Med. 2022, 13, 91–99. [Google Scholar] [CrossRef]
- Kiiza, D.; Biryomumaisho, S.; Robertson, I.D.; Hernandez, J.A. Seroprevalence of and risk factors associated with exposure to Brucella spp. In dairy cattle in three different agroecological zones in Rwanda. Am. J. Trop. Med. Hyg. 2021, 104, 1241–1246. [Google Scholar] [CrossRef]
- Islam, S.; Barua, S.R.; Moni, S.P.; Islam, A.; Rahman, A.A.; Chowdhury, S. Seroprevalence and risk factors for bovine brucellosis in the Chittagong Metropolitan Area of Bangladesh. Vet. Med. Sci. 2021, 7, 86–98. [Google Scholar] [CrossRef] [PubMed]
- Ntivuguruzwa, J.B.; Kolo, F.B.; Gashururu, R.S.; Umurerwa, L.; Byaruhanga, C.; Van Heerden, H. Seroprevalence and associated risk factors of bovine brucellosis at the wildlife-livestock-human interface in Rwanda. Microorganisms 2020, 8, 1553. [Google Scholar] [CrossRef] [PubMed]
- Kolo, F.B.; Adesiyun, A.A.; Fasina, F.O.; Katsande, C.T.; Dogonyaro, B.B.; Potts, A.; Matle, I.; Gelaw, A.K.; van Heerden, H. Seroprevalence and characterization of Brucella species in cattle slaughtered at Gauteng abattoirs, South Africa. Vet. Med. Sci. 2019, 5, 545–555. [Google Scholar] [CrossRef] [Green Version]
- Bugeza, J.; Muwonge, A.; Munyeme, M.; Lasuba, P.; Godfroid, J.; Kankya, C.; Jacques, G.; Kankya, C. Seroprevalence of bovine brucellosis and associated risk factors in Nakasongola district, Uganda. Trop. Anim. Health Prod. 2018, 51, 2073–2076. [Google Scholar] [CrossRef]
- Chaka, H.; Aboset, G.; Garoma, A.; Gumi, B.; Thys, E. Cross-sectional survey of brucellosis and associated risk factors in the livestock-wildlife interface area of Nechisar National Park, Ethiopia. Trop. Anim. Health Prod 2018, 50, 1041–1049. [Google Scholar]
- Zeng, J.; Duoji, C.; Yuan, Z.; Yuzhen, S.; Fan, W.; Tian, L.; Cai, C.; Robertson, I. Seroprevalence and risk factors for bovine brucellosis in domestic yaks (Bos grunniens) in Tibet, China. Trop. Anim. Health Prod. 2017, 49, 1339–1344. [Google Scholar] [CrossRef]
- Simonetti, M.A.; Suárez, J.L.; Rizzari, P. Prevalence of caprine brucellosis on herds of toba communities in Villa Río Bermejito, Chaco, Argentina (October 2010). Transbound. Emerg. Dis. 2019, 67, 5–8. [Google Scholar] [CrossRef]
- Vhoko, K.; Iannetti, S.; Burumu, J.; Ippoliti, C.; Bhebhe, B.; De Massis, F. Estimating the prevalence of brucellosis in cattle in Zimbabwe from samples submitted to the central veterinary laboratory between 2010 and 2014. Vet. Ital. 2018, 54, 21–27. [Google Scholar]
- Scacchia, M.; Di Provvido, A.; Ippoliti, C.; D’Angelo, A.; De Massis, F.; Kefle, U.; Sebhatu, T.T. Prevalence of brucellosis in dairy cattle from the main dairy farming regions of Eritrea. Onderstepoort J. Vet. Res. 2013, 80, 4. [Google Scholar] [CrossRef] [Green Version]
- Edao, B.M.; Hailegebreal, G.; Berg, S.; Zewude, A.; Zeleke, Y.; Sori, T.; Almaw, G.; Whatmore, A.M.; Ameni, G.; Wood, J.L.N. Brucellosis in the Addis Ababa dairy cattle: The myths and the realities. BMC Vet. Res. 2018, 14, 396. [Google Scholar] [CrossRef] [Green Version]
- Kneipp, C.C.; Sawford, K.; Wingett, K.; Malik, R.; Stevenson, M.A.; Mor, S.M.; Wiethoelter, A.K. Brucella suis seroprevalence and associated risk factors in dogs in Eastern Australia, 2016 to 2019. Front. Vet. Sci. 2021, 8, 727641. [Google Scholar] [CrossRef]
- Ducrotoy, M.J.; Conde-Álvarez, R.; Blasco, J.M.; Moriyón, I. A review of the basis of the immunological diagnosis of ruminant brucellosis. Vet. Immunol. Immunopathol. 2016, 171, 81–102. [Google Scholar]
- Al-Afifi, A.H.; Alewy Almashhadany, D.; Al-Azazi, A.S.H.; Khalaf, A.M.; Naji Ahmed Odhah, M.; Al-Gabri, N.A. Prevalence of Brucella spp. in milk from aborted and non-aborted animals in Dhamar governorate, Yemen. Ital. J. Food Saf. 2022, 11, 10370. [Google Scholar] [CrossRef]
- Rahman, S.U.; Zhu, L.; Cao, L.; Zhang, Y.; Chu, X.; Feng, S.; Li, Y.; Wu, J.; Wang, X. Prevalence of caprine brucellosis in Anhui province, China. Vet. World 2019, 12, 558–564. [Google Scholar] [CrossRef]
- Djangwani, J.; Abong’, G.O.; Njue, L.G.; Kaindi, D.W.M. Sero-prevalence and risk factors of Brucella presence in farm bulk milk from open and zero grazing cattle production systems in Rwanda. Vet. Med. Sci. 2021, 7, 1656–1670. [Google Scholar] [CrossRef]
- Asakura, S.; Makingi, G.; Kazwala, R.; Makita, K. Herd-level risk factors associated with Brucella sero-positivity in cattle, and perception and behaviours on the disease control among agro-pastoralists in Tanzania. Acta Trop. 2018, 187, 99–107. [Google Scholar] [CrossRef]
- Akinyemi, K.O.; Fakorede, C.O.; Amisu, K.O.; Wareth, G. Human and animal brucellosis in Nigeria: A systemic review and meta-analysis in the last twenty-one years (2001–2021). Vet. Sci. 2022, 9, 384. [Google Scholar] [CrossRef]
- Tahmo, N.B.; Wirsiy, F.S.; Nnamdi, D.B.; Tongo, M.; Lawler, J.V.; Broadhurst, M.J.; Wondji, C.S.; Brett-Major, D.M. An epidemiological synthesis of emerging and re-emerging zoonotic disease threats in Cameroon, 2000–2022: A systematic review. IJID Reg. 2023, 7, 84–109. [Google Scholar] [CrossRef]
- Alonso, S.; Dohoo, I.; Lindahl, J.; Verdugo, C.; Akuku, I.; Grace, D. Prevalence of tuberculosis, brucellosis and trypanosomiasis in cattle in Tanzania: A systematic review and meta-analysis. Anim. Health Res. Rev. 2016, 17, 16–27. [Google Scholar] [PubMed]
- Tadesse, G. Brucellosis seropositivity in animals and humans in Ethiopia: A meta-analysis. PLoS Negl. Trop. Dis. 2016, 10, e0005006. [Google Scholar]
- Tesfaye, A.; Dejene, H.; Admassu, B.; Kassegn, T.A.; Asfaw, D.; Dagnaw, G.G.; Bitew, A.B. Seroprevalence of bovine brucellosis in Ethiopia: Systematic review and meta-analysis. Vet. Med. 2021, 12, 1–6. [Google Scholar] [CrossRef]
- Djangwani, J.; Ooko Abong’, G.; Gicuku Njue, L.; Kaindi, D.W.M. Brucellosis: Prevalence with reference to East African community countries—A rapid review. Vet. Med. Sci. 2021, 7, 851–867. [Google Scholar] [CrossRef] [PubMed]
- Asante, J.; Noreddin, A.; Zowalaty, M.E.E. Systematic review of important bacterial zoonoses in Africa in the last decade in light of the ‘One Health’ concept. Pathogens 2019, 8, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suresh, K.P.; Patil, S.S.; Nayak, A.; Dhanze, H.; Rajamani, S.; Shivamallu, C.; Cull, C.A.; Amachawadi, R.G. Prevalence of brucellosis in livestock of African and Asian continents: A systematic review and meta-analysis. Front. Vet. Sci. 2022, 9, 923657. [Google Scholar]
- Abedi, A.-S.; Hashempour-Baltork, F.; Alizadeh, A.M.; Beikzadeh, S.; Hosseini, H.; Bashiry, M.; Taslikh, M.; Javanmardi, F.; Sheidaee, Z.; Sarlak, Z.; et al. The prevalence of Brucella spp. in dairy products in the Middle East region: A systematic review and meta-analysis. Acta Trop. 2020, 202, 105241. [Google Scholar]
- Dahl, M.O. Brucellosis in food-producing animals in Mosul, Iraq: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235862. [Google Scholar]
- Barman, N.N.; Patil, S.S.; Kurli, R.; Deka, P.; Bora, D.P.; Deka, G.; Ranjitha, K.M.; Shivaranjini, C.; Roy, P.; Suresh, K.P. Meta-analysis of the prevalence of livestock diseases in North Eastern Region of India. Vet. World 2020, 13, 80–91. [Google Scholar] [CrossRef]
- Jaismon, P.A.; Sushmitha, A.P.; Verma, M.R.; Singh, Y.P.; Borthakur, U.; Kumar, S.; Sharun, K.; Dhama, K. Prevalence of bovine brucellosis in India: A meta-analysis. Vet. Q. 2023, 43, 1–9. [Google Scholar] [CrossRef]
- Ran, X.; Chen, X.; Wang, M.; Cheng, J.; Ni, H.; Zhang, X.X.; Wen, X. Brucellosis seroprevalence in ovine and caprine flocks in China during 2000-2018: A systematic review and meta-analysis. BMC Vet. Res. 2018, 14, 393. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B.; Gong, Q.-L.; Feng, H.-F.; Wang, Q.; Shi, J.-F.; Song, Y.-H.; Liu, F.; Shi, K.; Zong, Y.; Du, R.; et al. Brucellosis prevalence in yaks in China in 1980–2019: A systematic review and meta-analysis. Prev. Vet. Med. 2021, 198, 105532. [Google Scholar]
- Shi, J.-F.; Gong, Q.-L.; Zhao, B.; Ma, B.-Y.; Chen, Z.-Y.; Yang, Y.; Sun, Y.-H.; Wang, Q.; Leng, X.; Zong, Y.; et al. Seroprevalence of brucellosis in buffalo worldwide and associated risk factors: A systematic review and meta-analysis. Front. Vet. Sci. 2021, 8, 649252. [Google Scholar] [CrossRef]
- Gong, Q.-L.; Sun, Y.-H.; Yang, Y.; Zhao, B.; Wang, Q.; Li, J.-M.; Ge, G.-Y.; Chen, Z.-Y.; Shi, K.; Leng, X.; et al. Global comprehensive literature review and meta-analysis of Brucella spp. in swine based on publications from 2000 to 2020. Front. Vet. Sci. 2021, 8, 630960. [Google Scholar]
- OIE. Reference Laboratories. Available online: https://www.woah.org/en/what-we-offer/expertise-network/reference-laboratories/ (accessed on 7 July 2023).
- Dean, A.S.; Crump, L.; Greter, H.; Schelling, E.; Zinsstag, J. Global burden of human brucellosis: A systematic review of disease frequency. PLoS Negl. Trop. Dis. 2012, 6, e1865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirk, M.D.; Pires, S.M.; Black, R.E.; Caipo, M.; Crump, J.A.; Devleesschauwer, B.; Döpfer, D.; Fazil, A.; Fischer-Walker, C.L.; Hald, T.; et al. World Health Organization estimates of the global and regional disease burden of 22 foodborne bacterial, protozoal, and viral diseases, 2010: A Data synthesis. PLoS Med. 2015, 12, e1001921. [Google Scholar]
- Lai, S.; Zhou, H.; Xiong, W.; Gilbert, M.; Huang, Z.; Yu, J.; Yin, W.; Wang, L.; Chen, Q.; Li, Y.; et al. Changing epidemiology of human brucellosis, China, 1955–2014. Emerg. Infect. Dis. 2017, 23, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.; Zhao, Y.; Zhao, J.; Pan, D.; Guo, Z. The spatiotemporal distribution of human brucellosis in mainland China from 2007–2016. BMC Infect. Dis. 2020, 20, 249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, J.; Zhang, N.; Shen, G.; Liang, F.; Zhao, Y.; He, X.; Wang, Y.; He, R.; Chen, W.; Xue, H.; et al. Spatiotemporal and seasonal trends of class A and B notifiable infectious diseases in China: Retrospective analysis. JMIR Public Health Surveill 2023, 9, e42820. [Google Scholar]
- CDC. Brucellosis (Brucella spp.) 1997 Case Definition. Available online: https://ndc.services.cdc.gov/case-definitions/brucellosis-1997/ (accessed on 6 July 2023).
- Lukambagire, A.S.; Mendes, Â.J.; Bodenham, R.F.; McGiven, J.A.; Mkenda, N.A.; Mathew, C.; Rubach, M.P.; Sakasaka, P.; Shayo, D.D.; Maro, V.P.; et al. Performance characteristics and costs of serological tests for brucellosis in a pastoralist community of northern Tanzania. Sci. Rep. 2021, 11, 5480. [Google Scholar] [CrossRef] [PubMed]
- Ariza, J.; Pellicer, T.; Pallares, R.; Foz, A.; Gudiol, F. Specific antibody profile in human brucellosis. Clin. Infect. Dis. 1992, 14, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Orduña-Domingo, A.; Almaraz, A.; Prado, A.; Gutiérrez, M.P.; García-Pascual, A.; Dueñas, A.; Cuervo, M.; Abad, R.; Hernández, B.; Lorenzo, B.; et al. Evaluation of an immunocapture-agglutination test (Brucellacapt) for serodiagnosis of human brucellosis. J. Clin. Microbiol. 2000, 38, 4000–4005. [Google Scholar] [CrossRef] [PubMed]
- Díaz, R.; Casanova, A.; Ariza, J.; Moriyón, I. The rose bengal test in human brucellosis: A neglected test for the diagnosis of a neglected disease. PLoS Negl. Trop. Dis. 2011, 5, e950. [Google Scholar]
- Yagupsky, P.; Morata, P.; Colmenero, J.D. Laboratory diagnosis of human brucellosis. Clin. Microbiol. Rev. 2019, 33, e00073-19. [Google Scholar] [CrossRef]
- de Glanville, W.A.; Conde-Álvarez, R.; Moriyón, I.; Njeru, J.; Díaz, R.; Cook, E.A.J.J.; Morin, M.; Bronsvoort, B.M.D.D.C.; Thomas, L.F.; Kariuki, S.; et al. Poor performance of the rapid test for human brucellosis in health facilities in Kenya. PLoS Negl. Trop. Dis. 2017, 11, e0005508. [Google Scholar] [CrossRef] [Green Version]
- Alumasa, L.; Thomas, L.F.; Amanya, F.; Njoroge, S.M.; Moriyón, I.; Makhandia, J.; Rushton, J.; Fèvre, E.M.; Falzon, L.C. Hospital-based evidence on cost-effectiveness of brucellosis diagnostic tests and treatment in Kenyan hospitals. PLoS Negl. Trop. Dis. 2021, 15, e0008977. [Google Scholar] [CrossRef]
- Lukambagire, A.S.; Shirima, G.M.; Shayo, D.D.; Mathew, C.; Yapi, R.B.; Kasanga, C.J.; Mmbaga, B.T.; Kazwala, R.R.; Halliday, J.E.B. Brucellosis testing patterns at health facilities in Arusha region, northern Tanzania. PLoS ONE 2022, 17, e0265612. [Google Scholar] [CrossRef]
- Waringa, N.M.A.; Waiboci, L.W.; Bebora, L.; Kinyanjui, P.W.; Kosgei, P.; Kiambi, S.; Osoro, E. Human brucellosis in Baringo County, Kenya: Evaluating the diagnostic kits used and identifying infecting Brucella species. PLoS ONE 2023, 18, e0269831. [Google Scholar] [CrossRef]
- Kiambi, S.G.; Fèvre, E.M.; Omolo, J.; Oundo, J.; De Glanville, W.A. Risk factors for acute human brucellosis in Ijara, north-eastern Kenya. PLoS Neglected Trop. Dis. 2020, 14, e0008108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- RENAVE. Informe Epidemiológico Sobre la Situación de la Brucelosis en España. Resultados de la Notificación a la Red Nacional de Vigilancia Epidemiológica los Años 2019, 2020 y 2021. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/archivos%20A-Z/Brucelosis/brucelosis%20INFORME%202019-2021.pdf#search=brucelosis (accessed on 3 July 2023).
- Plumb, G.E.; Olsen, S.C.; Buttke, D. Brucellosis: ‘One Health’ challenges and opportunities. Rev. Sci. Tech. Off. Int. Epiz 2013, 32, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.C.; Boggiatto, P.M. Characterization of the duration of immunity of Brucella abortus strain RB51 vaccination in cattle after experimental challenge. Prev. Vet. Med. 2022, 206, 105705. [Google Scholar] [CrossRef]
- Ashford, D.A.; di Pietra, J.; Lingappa, J.; Woods, C.; Noll, H.; Neville, B.; Weyant, R.; Bragg, S.L.; Spiegel, R.A.; Tappero, J.; et al. Adverse events in humans associated with accidental exposure to the livestock brucellosis vaccine RB51. Vaccine 2004, 22, 3435–3439. [Google Scholar] [CrossRef]
- Tiller, R.; Quance, C.R.; Robbe-Austerman, S.; Olsen, S.; Thacker, T.; Negron, M.E.; Kharod, G.; Saile, E.; Stoddard, R.; Salzer, J.; et al. Brucella abortus RB51 vaccine strain and raw milk consumption: An emerging Public Health risk. In Proceedings of the Brucellosis 2022 International Research Conference including the 74th Brucellosis Research Conference Giulianova, Teramo, Italy, 16–19 September 2022. [Google Scholar]
- Negrón, M.E.; Kharod, G.A.; Bower, W.A.; Walke, H. Notes from the field—Human Brucella abortus RB51 infections caused by consumption of unpasteurized domestic dairy products—United States, 2017–2019. Morb. Mortal. Wkly. Rep. 2019, 68, 185. [Google Scholar] [CrossRef] [Green Version]
- Blasco, J.M.; Molina-Flores, B. Control and eradication of Brucella melitensis infection in sheep and goats. Vet. Clin. N. Am. Food Anim. Pract. 2011, 27, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Mick, V.; Le Carrou, G.; Corde, Y.; Game, Y.; Jay, M.; Garin-Bastuji, B. Brucella melitensis in France: Persistence in wildlife and probable spillover from alpine Ibex to domestic animals. PLoS ONE 2014, 9, e94168. [Google Scholar]
- National Academies of Sciences, Engineering, and Medicine; Division on Earth and Life Studies; Board on Agriculture and Natural Resources; Committee on Revisiting Brucellosis in the Greater Yellowstone Area. Ecology and epidemiology of brucella abortus in the greater yellowstone ecosystem. In Revisiting Brucellosis in the Greater Yellowstone Area; National Academies Press (US): Cambridge, MA, USA, 2017; pp. 1–195. [Google Scholar]
- Godfroid, J.; Nielsen, K.H.; Saegerman, C. Diagnosis of brucellosis in livestock and wildlife. Croat. Med. J. 2010, 51, 296–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, P.M.; Boadella, M.; Arnal, M.; de Miguel, M.J.; Revilla, M.; Martínez, D.; Vicente, J.; Acevedo, P.; Oleaga, A.; Ruiz-Fons, F.; et al. Spatial distribution and risk factors of brucellosis in iberian wild ungulates. BMC Infect. Dis. 2010, 10, 46. [Google Scholar] [CrossRef] [Green Version]
- Hördt, A.; López, M.G.; Meier-Kolthoff, J.P.; Schleuning, M.; Weinhold, L.-M.M.; Tindall, B.J.; Gronow, S.; Kyrpides, N.C.; Woyke, T.; Göker, M. Analysis of 1000+ type-strain genomes substantially improves taxonomic classification of Alphaproteobacteria. Front. Microbiol. 2020, 11, 468. [Google Scholar] [PubMed]
- Moreno, E.; Letesson, J.J.; Gorvel, J.P.; Moriyón, I. Pathogenicity and its implications in Taxonomy: The Brucella and Ochrobactrum case. Pathogens 2022, 11, 377. [Google Scholar] [CrossRef] [PubMed]
- Moreno, E.; Middlebrook, E.A.; Altamirano-Silva, P.; Al, D.S.; Araj, G.F.; Arce-Gorvel, V.; Arenas-Gamboa, Á.; Ariza, J.; Barquero-Calvo, E.; Battelli, G.; et al. If you’re not confused, you’re not paying attention: Ochrobactrum is not Brucella. J. Clin. Microbiol. 2023, e0043823. [Google Scholar] [CrossRef]
- Hermesh, B.; Rosenthal, A.; Davidovitch, N. The cycle of distrust in health policy and behavior: Lessons learned from the Negev Bedouin. PLoS ONE 2020, 15, e0237734. [Google Scholar]
- Stahl, Z.; Alsana, F.; Dochan, L.; Haas, E.J.; Gdalevich, M. Preventing brucellosis in the Bedouin society in Israel. J. Community Med. Health Educ. 2017, 7, 0711–1000575. [Google Scholar]
- Zhang, N.; Huang, D.; Wu, W.; Liu, J.; Liang, F.; Zhou, B.; Guan, P. Animal brucellosis control or eradication programs worldwide: A systematic review of experiences and lessons learned. Prev. Vet. Med. 2018, 160, 105–115. [Google Scholar] [PubMed]
- McAlester, J.; Kanazawa, Y. Situating zoonotic diseases in peacebuilding and development theories: Prioritizing zoonoses in Jordan. PLoS ONE 2022, 17, e0265508. [Google Scholar]
- Campbell, Z.; Coleman, P.; Guest, A.; Kushwaha, P.; Ramuthivheli, T.; Osebe, T.; Perry, B.; Salt, J. Prioritizing smallholder animal health needs in East Africa, West Africa, and South Asia using three approaches: Literature review, expert workshops, and practitioner surveys. Prev. Vet. Med. 2021, 189, 105279. [Google Scholar] [PubMed]
- Kheirallah, K.A.; Al-Mistarehi, A.-H.; Alsawalha, L.; Hijazeen, Z.; Mahrous, H.; Sheikali, S.; Al-Ramini, S.; Maayeh, M.; Dodeen, R.; Farajeh, M.; et al. Prioritizing zoonotic diseases utilizing the One Health approach: Jordan’s experience. One Health 2021, 13, 100262. [Google Scholar] [PubMed]
- Mersha, T.T.; Mekonnen Wolde, B.; Shumuye, N.A.; Hailu, A.B.; Mohammed, A.H.; Redda, Y.T.; Abera, B.H.; Menghistu, H.T. Prioritization of neglected tropical zoonotic diseases: A one health perspective from Tigray region, Northern Ethiopia. PLoS ONE 2021, 16, e0254071. [Google Scholar]
- Bardosh, K.L.; Scoones, J.C.; Grace, D.; Kalema-Zikusoka, G.; Jones, K.E.; De Balogh, K.; Waltner-Toews, D.; Bett, B.; Welburn, S.C.; Mumford, E.; et al. Engaging research with policy and action: What are the challenges of responding to zoonotic disease in Africa? Phil. Trans. R. Soc. B 2017, 372, 20160172. [Google Scholar] [CrossRef] [Green Version]
- Spink, W.W. The natural course of brucellosis. In The Nature of Brucellosis; The University of Minnesota Press: Minneapolis, MN, USA, 1956; pp. 145–170. [Google Scholar]
- Hernández-Mora, G.; Bonilla-Montoya, R.; Barrantes-Granados, O.; Esquivel-Suárez, A.; Montero-Caballero, D.; González-Barrientos, R.; Fallas-Monge, Z.; Palacios-Alfaro, J.D.; Baldi, M.; Campos, E. Brucellosis in mammals of Costa Rica: An epidemiological survey. PLoS ONE 2017, 12, e0182644. [Google Scholar]
- Kropotkin, P. Mutual Aid: A Factor of Evolution. Neeland Media LLC. 1902. Available online: https://en.wikisource.org/wiki/Mutual_Aid:_A_Factor_of_Evolution (accessed on 3 May 2023).




{kind=link}
{kind=link}
{kind=link}
| Nº (%) of Countries in Each Category | ||
|---|---|---|
| Capacity Level [WHO JEE Score] c | Surveillance Systems | Response Mechanisms |
| No [1] | 8 (18) | 17 (38) |
| Limited [2] | 13 (30) | 18 (41) |
| Developed [3] | 19 (43) | 8 (19) |
| Demonstrated [4] | 3 (7) | 1 (2) |
| Sustainable [5] | 1 (2) | 0 (0) |
| Country | Human, Physical and Financial Resources | Technical Authority and Capability | Interaction with Interested Parties |
|---|---|---|---|
| Canada | 4.9 | 4.3 | 5 |
| Japan | 4.8 | 4.7 | 4.3 |
| Chile | 4.4 | 3.9 | 3.0 |
| Uruguay | 4.4 | 3.9 | 3.0 |
| Brazil | 4.0 | 3.2 | 4.5 |
| Paraguay | 3.3 | 2.4 | 3.3 |
| India | 3.2 | 2.7 | 3.0 |
| Panama | 2.8 | 3.1 | 2.8 |
| Rep. Dominicana | 2.3 | 2.5 | 2.5 |
| Bolivia | 1.8 | 2.6 | 2.5 |
| Investigated Characteristics | Positive Answers (%) |
|---|---|
| Zoonotic nature | 37.6 2 |
| Mode of transmission | 35.9 2 |
| Signs of disease | |
| Human | 41.6 2 |
| Animal | 28.4 2 |
| Existence of animal vaccines | 26.1 3 |
| No. (×106) in Resource-Limited Areas/Total World (%) | ||||
|---|---|---|---|---|
| Type of Animal | Grazing | Rainfed Mixed | Irrigated Mixed | Industrial |
| Cattle and buffaloes | 342/406 (84%) | 444/641 (69%) | 416/450 (92%) | 1/29 (3%) |
| Sheep and goats | 405/590 (69%) | 500/632 (79%) | 474/546 (87%) | 9/9 (100%) |
| Overlooked Facts | Consequences |
|---|---|
| Brucellosis is a collective disease; the proportion of infected herds/flocks is critical, even if individual seroprevalence is low. | Herd/flock prevalence is either not investigated or misjudged. Brucellosis presence is misrepresented and the potential of “chronically” infected herds/flocks to perpetuate the disease in an area is overlooked. |
| Brucellosis primarily affects animals of reproductive age. | Random selection, including young animals, reduces the detection of infected herds’ locks. |
| Relevance of cross-infections. | In mixed-breeding systems, focusing on one host (usually cattle): (1) does not provide the real picture, and (2) prevents control and eradication. Issue overlaps with two other mistakes: (1) B. melitensis does not infect cattle, and (2) B. melitensis infection in cattle clears spontaneously when contact with infected small ruminants is prevented. |
| Overlooked Facts | Consequences (Common Mistakes) |
|---|---|
| In vitro, smooth brucellae readily generate rough mutants. | For buffered agglutination 2 and complement fixation tests, false and inconsistent results are given. For all tests, strict quality control is necessary. |
| iELISA, cELISA and FPA require validation for local conditions. | Incorrect seroprevalence (use of manufacturer’s cut-offs, mostly of an unknown basis). |
| Sub-optimal sensitivity of cELISAs and SAT. | Seroprevalence sub-estimation. |
| Assays used in brucellosis-free countries for surveillance are not the best choice everywhere. | Needless infrastructure demands and costs. |
| Buffered acid pH agglutination tests 1 match iELISAs in terms of sensitivity/specificity. | It is overlooked that these agglutination tests are almost ideal under many circumstances (the misconception that these tests are negatively affected by prozones and are highly unspecific). |
| Misleading understanding of “Confirmatory tests”. | Incorrect seroprevalence estimations (e.g., RBT confirmed by iELISA, cELISA, FPA or complement fixation in the absence of S19 vaccination). |
| The milk-ring test only works in cattle (Bos taurus). | Incorrect prevalence estimations in small ruminants, buffaloes, and camels. |
| Molecular tests (PCR) require strict validation. | Unknown false-positive/negative score (identity between analytical and diagnostic parameters; “validation” in poorly defined populations (no true Brucella-free and no gold-standard positive controls) or in experimentally infected animals. |
| Vaccine | ||
|---|---|---|
| S19 | RB51 | |
| Used in successful programs | In 10 countries | None |
| Protection 2 | B. abortus and B. melitensis; (one dose is useful throughout life). | Lower than S19 against B. abortus; elapses in <4 years; no evidence that revaccination bolsters protection; no evidence of protection against B. melitensis. |
| Safety | ||
| Abortifacient | Yes (minimized by conjunctival route). | Yes. |
| Milk excretion | Yes (minimized by conjunctival route). | Yes. |
| Virulence in humans | Moderate; Standard diagnosis/treatment. | Moderate; no serological tests available; Rifampicin-resistant |
| Use in males | Not recommended. | Not recommended. |
| DIVA properties 3 | Interferes in all serological tests; minimized in calves by the conjunctival route. | Interferes in ELISAs, FPA and lateral flow immunochromato-graphy. Animals become positive in RBT and complement fixation when exposed to virulent brucellae. |
| Biological control (seed lots) | WOAH (OIE) mouse model. | None. |
| Parent | Candidate | Year Completed |
|---|---|---|
| Italy | Eritrea | 2011 |
| Italy | Kazakhstan | 2015 |
| UK | Sudan | 2014 |
| France | Thailand | 2013 |
| UK | Turkey | 2011 |
| Germany | United Arab Emirates | 2016 |
| Italy | Zimbabwe | 2016 |
| UK | Afghanistan | 2019 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moriyón, I.; Blasco, J.M.; Letesson, J.J.; De Massis, F.; Moreno, E. Brucellosis and One Health: Inherited and Future Challenges. Microorganisms 2023, 11, 2070. https://doi.org/10.3390/microorganisms11082070
Moriyón I, Blasco JM, Letesson JJ, De Massis F, Moreno E. Brucellosis and One Health: Inherited and Future Challenges. Microorganisms. 2023; 11(8):2070. https://doi.org/10.3390/microorganisms11082070
Chicago/Turabian StyleMoriyón, Ignacio, José María Blasco, Jean Jacques Letesson, Fabrizio De Massis, and Edgardo Moreno. 2023. "Brucellosis and One Health: Inherited and Future Challenges" Microorganisms 11, no. 8: 2070. https://doi.org/10.3390/microorganisms11082070
APA StyleMoriyón, I., Blasco, J. M., Letesson, J. J., De Massis, F., & Moreno, E. (2023). Brucellosis and One Health: Inherited and Future Challenges. Microorganisms, 11(8), 2070. https://doi.org/10.3390/microorganisms11082070