
Seasonal Testing, Results, and Effect of the Pandemic on Coxsackievirus Serum Studies


Abstract
:1. Introduction
2. Materials and Methods
3. Results
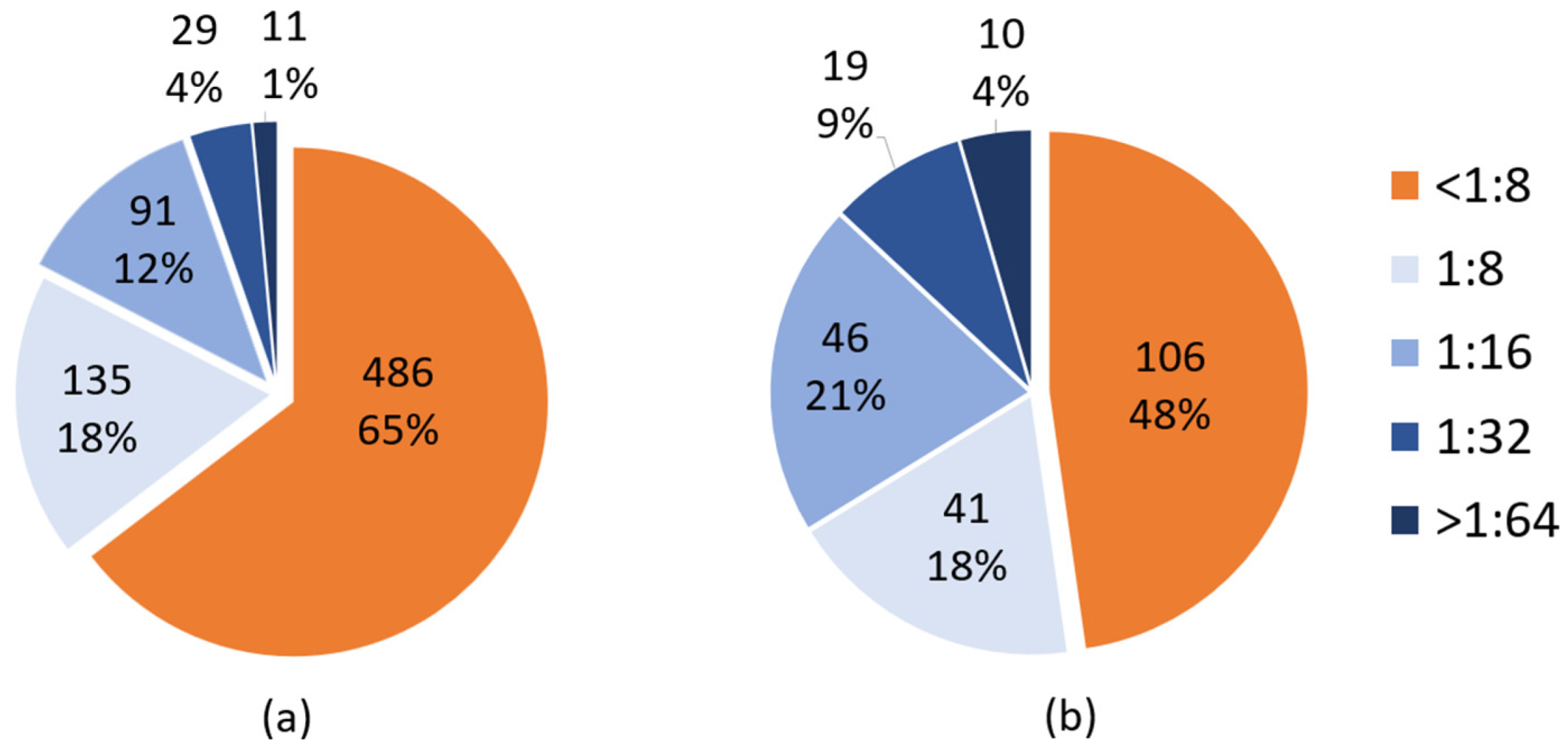
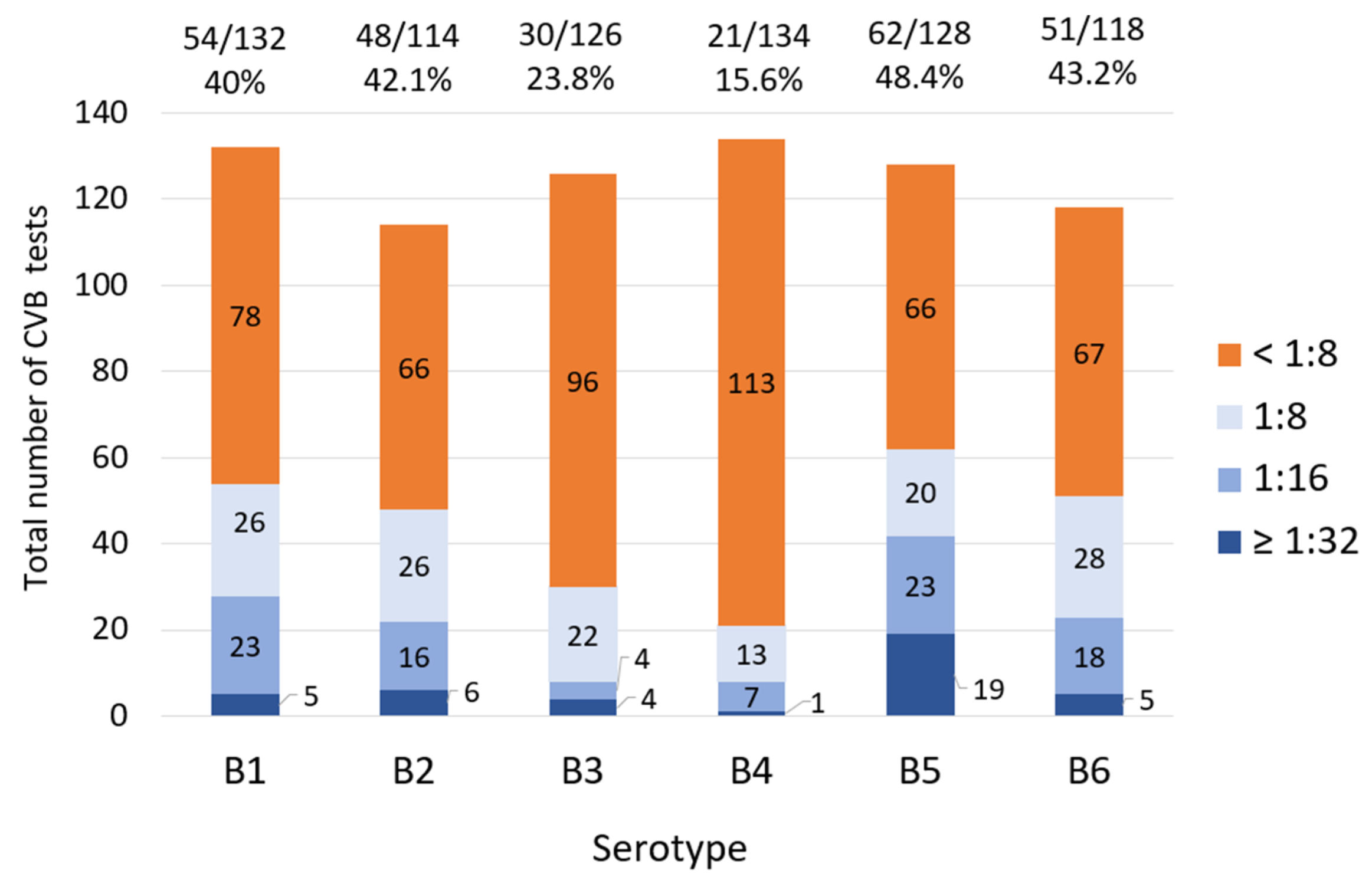
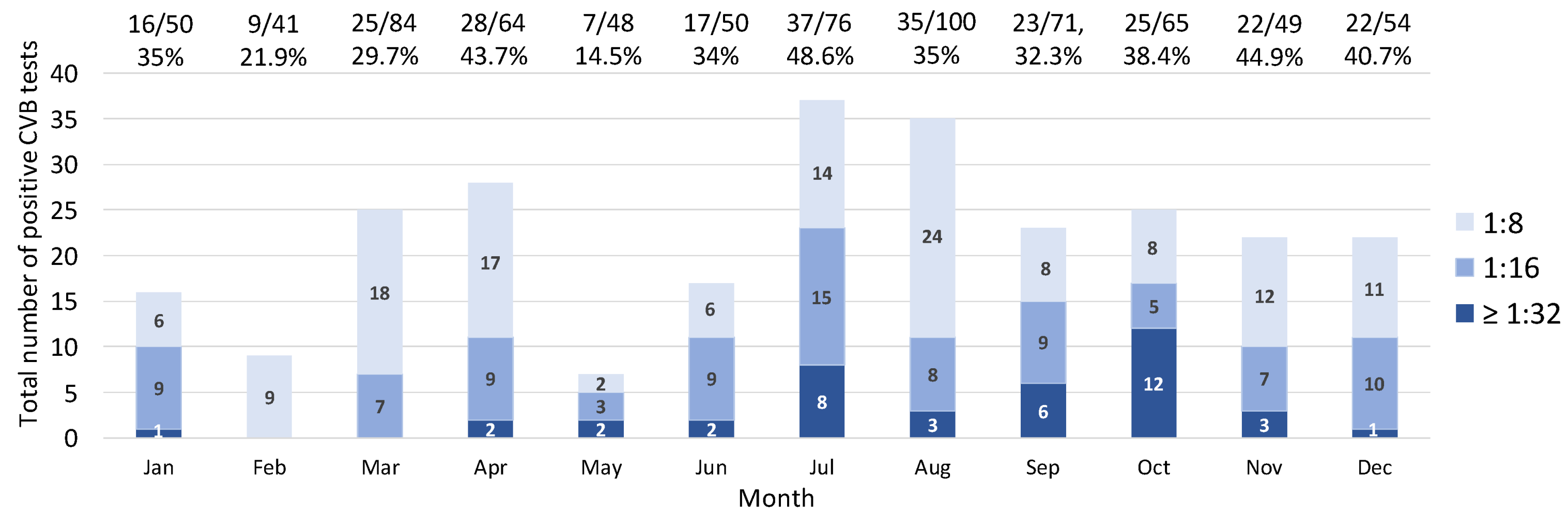
3.1. Coxsackievirus B
3.2. Coxsackievirus A
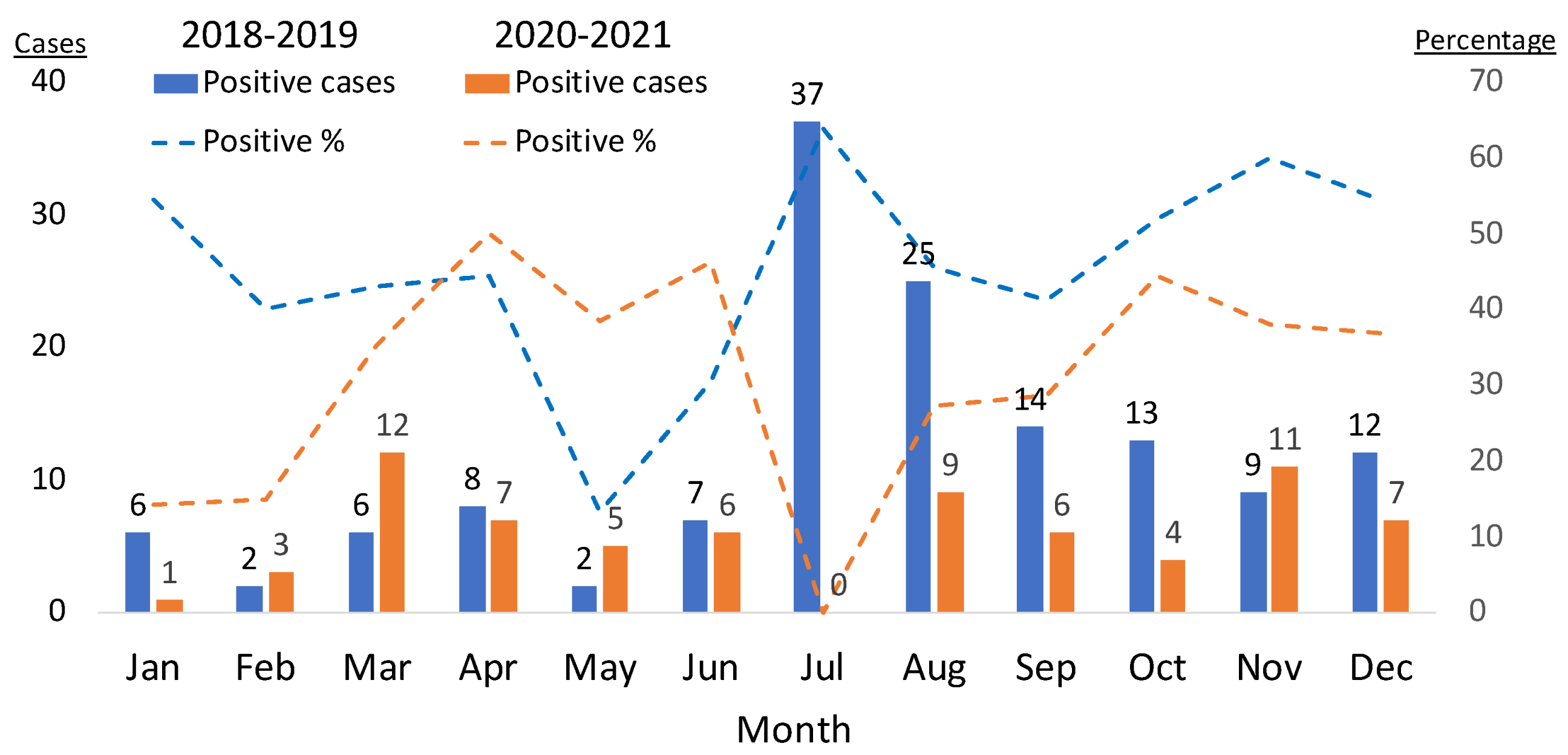
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pallansch, M. Coxsackievirus B epidemiology and public health concerns. In The Coxsackie B Viruses; Springer: Berlin/Heidelberg, Germany, 1997; pp. 13–30. [Google Scholar] [CrossRef]
- Tariq, N.; Kyriakopoulos, C. Group B Coxsackie Virus; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Nikonov, O.; Chernykh, E.; Garber, M.; Nikonova, E.Y. Enteroviruses: Classification, diseases they cause, and approaches to development of antiviral drugs. Biochemistry 2017, 82, 1615–1631. [Google Scholar] [CrossRef]
- Pons-Salort, M.; Parker, E.P.; Grassly, N.C. The epidemiology of non-polio enteroviruses: Recent advances and outstanding questions. Curr. Opin. Infect. Dis. 2015, 28, 479. [Google Scholar] [CrossRef] [PubMed]
- Khetsuriani, N.; LaMonte-Fowlkes, A.; Oberst, S.; Pallansch, M.A.; Centers for Disease Control and Prevention. Enterovirus surveillance—United States, 1970–2005. MMWR Surveill. Summ. 2006, 55, 1–20. [Google Scholar]
- Brouwer, L.; Moreni, G.; Wolthers, K.C.; Pajkrt, D. World-wide prevalence and genotype distribution of enteroviruses. Viruses 2021, 13, 434. [Google Scholar] [CrossRef]
- Bubba, L.; Broberg, E.K.; Jasir, A.; Simmonds, P.; Harvala, H.; Redlberger-Fritz, M.; Nikolaeva-Glomb, L.; Havlíčková, M.; Rainetova, P.; Fischer, T.K. Circulation of non-polio enteroviruses in 24 EU and EEA countries between 2015 and 2017: A retrospective surveillance study. Lancet Infect. Dis. 2020, 20, 350–361. [Google Scholar] [CrossRef]
- Keeren, K.; Böttcher, S.; on behalf of the LaNED; Diedrich, S. Enterovirus Surveillance (EVSurv) in Germany. Microorganisms 2021, 9, 2005. [Google Scholar] [CrossRef]
- Wong, A.H.; Lau, C.; Cheng, P.K.; Ng, A.Y.; Lim, W.W. Coxsackievirus B3-associated aseptic meningitis: An emerging infection in Hong Kong. J. Med. Virol. 2011, 83, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Zhu, R.; Cheng, T.; Yin, Z.; Liu, D.; Xu, L.; Li, Y.; Wang, W.; Liu, J.; Que, Y.; Ye, X. Serological survey of neutralizing antibodies to eight major enteroviruses among healthy population. Emerg. Microbes Infect. 2018, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Nonpolio enterovirus and human parechovirus surveillance—United States, 2006–2008. MMWR Morb. Mortal. Wkly. Rep. 2010, 59, 1577–1580. [Google Scholar]
- Abedi, G.R.; Watson, J.T.; Pham, H.; Nix, W.A.; Oberste, M.S.; Gerber, S.I. Enterovirus and human parechovirus surveillance—United States, 2009–2013. Morb. Mortal. Wkly. Rep. 2015, 64, 940–943. [Google Scholar] [CrossRef]
- Abedi, G.R.; Watson, J.T.; Nix, W.A.; Oberste, M.S.; Gerber, S.I. Enterovirus and parechovirus surveillance—United States, 2014–2016. Morb. Mortal. Wkly. Rep. 2018, 67, 515. [Google Scholar] [CrossRef]
- Rotbart, H.A.; McCracken, G.H., Jr.; Whitley, R.J.; Modlin, J.F.; Cascino, M.; Shah, S.; Blum, D. Clinical significance of enteroviruses in serious summer febrile illnesses of children. Pediatr. Infect. Dis. J. 1999, 18, 869–874. [Google Scholar] [CrossRef]
- Zaoutis, T.; Klein, J.D. Enterovirus infections. Pediatr. Rev. 1998, 19, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.K.; Ju, E.S.; Lao, D.H.; Yun, S.H.; Lee, Y.J.; Kim, D.K.; Jeon, E.S. Development of a enterovirus diagnostic assay system for diagnosis of viral myocarditis in humans. Microbiol. Immunol. 2013, 57, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.-S.; Lee, H.-C.; Lee, K.-M.; Gong, Y.-N.; Shih, S.-R. Enterovirus and encephalitis. Front. Microbiol. 2020, 11, 261. [Google Scholar] [CrossRef] [PubMed]
- Fowlkes, A.L.; Honarmand, S.; Glaser, C.; Yagi, S.; Schnurr, D.; Oberste, M.S.; Anderson, L.; Pallansch, M.A.; Khetsuriani, N. Enterovirus-associated encephalitis in the California encephalitis project, 1998–2005. J. Infect. Dis. 2008, 198, 1685–1691. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-M.; Lei, H.-Y.; Liu, C.-C. Cytokine immunopathogenesis of enterovirus 71 brain stem encephalitis. Clin. Dev. Immunol. 2012, 2012, 876241. [Google Scholar] [CrossRef] [PubMed]
- Freund, M.W.; Kleinveld, G.; Krediet, T.G.; van Loon, A.M.; Verboon-Maciolek, M.A. Prognosis for neonates with enterovirus myocarditis. Arch. Dis. Child.-Fetal Neonatal Ed. 2010, 95, F206–F212. [Google Scholar] [CrossRef]
- Badorff, C.; Knowlton, K.U. Dystrophin disruption in enterovirus-induced myocarditis and dilated cardiomyopathy: From bench to bedside. Med. Microbiol. Immunol. 2004, 193, 121–126. [Google Scholar] [CrossRef]
- Knipe, D.; Howley, P.; Griffin, D.; Lamb, R.; Martin, M.; Roizman, B.; Straus, S. Fields Virology, Volumes 1 and 2; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Puenpa, J.; Chieochansin, T.; Linsuwanon, P.; Korkong, S.; Thongkomplew, S.; Vichaiwattana, P.; Theamboonlers, A.; Poovorawan, Y. Hand, foot, and mouth disease caused by coxsackievirus A6, Thailand, 2012. Emerg. Infect. Dis. 2013, 19, 641. [Google Scholar] [CrossRef]
- Park, K.; Lee, B.; Baek, K.; Cheon, D.; Yeo, S.; Park, J.; Soh, J.; Cheon, H.; Yoon, K.; Choi, Y. Enteroviruses isolated from herpangina and hand-foot-and-mouth disease in Korean children. Virol. J. 2012, 9, 205. [Google Scholar] [CrossRef] [PubMed]
- Blomqvist, S.; Klemola, P.; Kaijalainen, S.; Paananen, A.; Simonen, M.-L.; Vuorinen, T.; Roivainen, M. Co-circulation of coxsackieviruses A6 and A10 in hand, foot and mouth disease outbreak in Finland. J. Clin. Virol. 2010, 48, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Kushner, P.; Krebs, M. Epidemiology of hand, foot, and mouth disease in a summer camp due to Coxsackie virus A16. J. Am. Osteopath. Assoc. 1972, 72, 281–283. [Google Scholar]
- Centers for Disease Control and Prevention. Notes from the field: Severe hand, foot, and mouth disease associated with coxsackievirus A6-Alabama, Connecticut, California, and Nevada, November 2011–February 2012. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 213–214. [Google Scholar]
- Hayman, R.; Shepherd, M.; Tarring, C.; Best, E. Outbreak of variant hand-foot-and-mouth disease caused by coxsackievirus A 6 in A uckland, N ew Z ealand. J. Paediatr. Child Health 2014, 50, 751–755. [Google Scholar] [CrossRef]
- Fujimoto, T.; Iizuka, S.; Enomoto, M.; Abe, K.; Yamashita, K.; Hanaoka, N.; Okabe, N.; Yoshida, H.; Yasui, Y.; Kobayashi, M. Hand, foot, and mouth disease caused by coxsackievirus A6, Japan, 2011. Emerg. Infect. Dis. 2012, 18, 337–339. [Google Scholar] [CrossRef]
- Sinclair, C.; Gaunt, E.; Simmonds, P.; Broomfield, D.; Nwafor, N.; Wellington, L.; Templeton, K.; Willocks, L.; Schofield, O.; Harvala, H. Atypical hand, foot, and mouth disease associated with coxsackievirus A6 infection, Edinburgh, United Kingdom, January to February 2014. Eurosurveillance 2014, 19, 20745. [Google Scholar] [CrossRef]
- Bian, L.; Gao, F.; Mao, Q.; Sun, S.; Wu, X.; Liu, S.; Yang, X.; Liang, Z. Hand, foot, and mouth disease associated with coxsackievirus A10: More serious than it seems. Expert Rev. Anti-Infect. Ther. 2019, 17, 233–242. [Google Scholar] [CrossRef]
- Mirand, A.; Henquell, C.; Archimbaud, C.; Ughetto, S.; Antona, D.; Bailly, J.-L.; Peigue-Lafeuille, H. Outbreak of hand, foot and mouth disease/herpangina associated with coxsackievirus A6 and A10 infections in 2010, France: A large citywide, prospective observational study. Clin. Microbiol. Infect. 2012, 18, E110–E118. [Google Scholar] [CrossRef]
- Hosoya, M.; Kawasaki, Y.; Sato, M.; Honzumi, K.; Hayashi, A.; Hiroshima, T.; Ishiko, H.; Kato, K.; Suzuki, H. Genetic diversity of coxsackievirus A16 associated with hand, foot, and mouth disease epidemics in Japan from 1983 to 2003. J. Clin. Microbiol. 2007, 45, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wu, S.; Xiong, Y.; Li, T.; Wen, Z.; Yan, M.; Qin, K.; Liu, Y.; Wu, J. Co-circulation and genomic recombination of coxsackievirus A16 and enterovirus 71 during a large outbreak of hand, foot, and mouth disease in Central China. PLoS ONE 2014, 9, e96051. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.O.; Huang, K.-Y.A.; Chen, M.-H.; Chen, P.-C.; Huang, W.-T. Comparison of nonpolio enteroviruses in children with herpangina and hand, foot and mouth disease in Taiwan. Pediatr. Infect. Dis. J. 2019, 38, 887–893. [Google Scholar] [CrossRef]
- Wang, C.-Y.; Lu, F.L.; Wu, M.-H.; Lee, C.-Y.; Huang, L.-M. Fatal coxsackievirus A16 infection. Pediatr. Infect. Dis. J. 2004, 23, 275–276. [Google Scholar] [CrossRef]
- Legay, F.; Lévêque, N.; Gacouin, A.; Tattevin, P.; Bouet, J.; Thomas, R.; Chomel, J.-J. Fatal coxsackievirus A-16 pneumonitis in adult. Emerg. Infect. Dis. 2007, 13, 1084. [Google Scholar] [CrossRef] [PubMed]
- McKay, S.L.; Lee, A.D.; Lopez, A.S.; Nix, W.A.; Dooling, K.L.; Keaton, A.A.; Spence-Davizon, E.; Herlihy, R.; Clark, T.A.; Hopkins, S.E. Increase in acute flaccid myelitis—United States, 2018. Morb. Mortal. Wkly. Rep. 2018, 67, 1273. [Google Scholar] [CrossRef] [PubMed]
- Bitnun, A.; Yeh, E.A. Acute flaccid paralysis and enteroviral infections. Curr. Infect. Dis. Rep. 2018, 20, 34. [Google Scholar] [CrossRef]
- Laxmivandana, R.; Yergolkar, P.; Rajeshwari, M.; Chitambar, S.D. Genomic characterization of coxsackievirus type A24 strains associated with acute flaccid paralysis and rarely identified Hopkins syndrome. Arch. Virol. 2014, 159, 3125–3129. [Google Scholar] [CrossRef] [PubMed]
- Korukluoglu, G.; Ozdemirer, U.; Bayrakdar, F.; Unal, Z.; Cosgun, Y.; Atak, T.; Karademirtok, H.; Ata, I.; Kara, F. Detection of non-polio and polio enteroviruses in Acute Flaccid Paralysis surveillance in Turkey. Acta Microbiol. Immunol. Hung. 2021, 68, 92–98. [Google Scholar] [CrossRef]
- Gear, J.; Measroch, V. Coxsackievirus infections of the newborn. Prog. Med. Virol. Fortschritte Med. Virusforschung. Prog. Virol. Medicale 1973, 15, 42–62. [Google Scholar]
- Editorial Board. Avoiding the danger of enteroviruses to newborn infants. Lancet 1986, 1, 194–195. [Google Scholar]
- Kaplan, M.H.; Klein, S.W.; McPhee, J.; Harper, R.G. Group B coxsackievirus infections in infants younger than three months of age: A serious childhood illness. Rev. Infect. Dis. 1983, 5, 1019–1032. [Google Scholar] [CrossRef] [PubMed]
- Bryant, P.A.; Tingay, D.; Dargaville, P.A.; Starr, M.; Curtis, N. Neonatal coxsackie B virus infection—A treatable disease? Eur. J. Pediatr. 2004, 163, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Cree, B.C.; Bernardini, G.L.; Hays, A.P.; Lowe, G. A fatal case of coxsackievirus B4 meningoencephalitis. Arch. Neurol. 2003, 60, 107–112. [Google Scholar] [CrossRef]
- Eyckmans, T.; Wollants, E.; Janssens, A.; Schoemans, H.; Lagrou, K.; Wauters, J.; Maertens, J. Coxsackievirus A16 encephalitis during obinutuzumab therapy, Belgium, 2013. Emerg. Infect. Dis. 2014, 20, 913–915. [Google Scholar] [CrossRef]
- Moschovi, M.A.; Sterpi, P.; Youroukos, S.; Tzortzatou-Stathopoulou, F. Encephalitis and myocarditis in a child with acute lymphoblastic leukemia: Role of coxsackievirus B5? Pediatr. Hematol. Oncol. 2002, 19, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Sabeena, S.; Bhat, K.G.; Bharani, K.C.; Ramachandran, S.; Arunkumar, G. Coxsackievirus A6 (CV-A6) Encephalomyelitis in an Immunocompromised Child: A Case Report and Brief Review of the Literature. Jpn. J. Infect. Dis. 2018, 71, 388–389. [Google Scholar] [CrossRef]
- Kim, H.; Kang, B.; Hwang, S.; Hong, J.; Chung, J.; Kim, S.; Jeong, Y.S.; Kim, K.; Cheon, D.S. Molecular characteristics of human coxsackievirus B1 infection in Korea, 2008–2009. J. Med. Virol. 2013, 85, 110–115. [Google Scholar] [CrossRef]
- Verma, N.A.; Zheng, X.T.; Harris, M.U.; Cadichon, S.B.; Melin-Aldana, H.; Khetsuriani, N.; Oberste, M.S.; Shulman, S.T. Outbreak of life-threatening coxsackievirus B1 myocarditis in neonates. Clin. Infect. Dis. 2009, 49, 759–763. [Google Scholar] [CrossRef]
- Kriger, O.; Abramovich, A.; Fratty, I.S.; Leshem, E.; Amit, S.; Stein, M.; Ben-Zeev, B.; Via-Dorembus, S.; Hoffmann, C.; Rabinowicz, S. An Outbreak of Coxsackievirus B Type 2 Acute Meningoencephalitis in Children, Israel, July–September 2022. Pediatr. Infect. Dis. J. 2023, 42, e177–e179. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Tao, Z.; Song, Y.; Liu, G.; Wang, H.; Liu, Y.; Song, L.; Li, Y.; Lin, X.; Cui, N. A coxsackievirus B5-associated aseptic meningitis outbreak in Shandong Province, China in 2009. J. Med. Virol. 2013, 85, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Fukazawa, M.; Hoshina, T.; Nanishi, E.; Nishio, H.; Doi, T.; Ohga, S.; Hara, T. Neonatal hemophagocytic lymphohistiocytosis associated with a vertical transmission of coxsackievirus B1. J. Infect. Chemother. 2013, 19, 1210–1213. [Google Scholar] [CrossRef]
- Cheng, L.L.; Ng, P.C.; Chan, P.K.-S.; Wong, H.L.; Cheng, F.W.T.; Tang, J.W.-T. Probable intrafamilial transmission of coxsackievirus b3 with vertical transmission, severe early-onset neonatal hepatitis, and prolonged viral RNA shedding. Pediatrics 2006, 118, e929–e933. [Google Scholar] [CrossRef]
- Andréoletti, L.; Lévêque, N.; Boulagnon, C.; Brasselet, C.; Fornes, P. Viral causes of human myocarditis. Arch. Cardiovasc. Dis. 2009, 102, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Kandolf, R.; Ameis, D.; Kirschner, P.; Canu, A.; Hofschneider, P.H. In situ detection of enteroviral genomes in myocardial cells by nucleic acid hybridization: An approach to the diagnosis of viral heart disease. Proc. Natl. Acad. Sci. USA 1987, 84, 6272–6276. [Google Scholar] [CrossRef] [PubMed]
- Leonard, E.G. Viral myocarditis. Pediatr. Infect. Dis. J. 2004, 23, 665–666. [Google Scholar] [CrossRef] [PubMed]
- Gaaloul, I.; Riabi, S.; Harrath, R.; Hunter, T.; Hamda, K.B.; Ghzala, A.B.; Huber, S.; Aouni, M. Coxsackievirus B detection in cases of myocarditis, myopericarditis, pericarditis and dilated cardiomyopathy in hospitalized patients. Mol. Med. Rep. 2014, 10, 2811–2818. [Google Scholar] [CrossRef] [PubMed]
- Spotnitz, M.D.; Lesch, M. Idiopathic dilated cardiomyopathy as a late complication of healed viral (Coxsackie B virus) myocarditis: Historical analysis, review of the lliterature, and a postulated unifying hypothesis. Prog. Cardiovasc. Dis. 2006, 49, 42–57. [Google Scholar] [CrossRef] [PubMed]
- Cambridge, G.; MacArthur, C.; Waterson, A.; Goodwin, J.; Oakley, C. Antibodies to Coxsackie B viruses in congestive cardiomyopathy. Heart 1979, 41, 692–696. [Google Scholar] [CrossRef]
- Bouin, A.; Gretteau, P.-A.; Wehbe, M.; Renois, F.; N’guyen, Y.; Lévêque, N.; Vu, M.N.; Tracy, S.; Chapman, N.M.; Bruneval, P. Enterovirus persistence in cardiac cells of patients with idiopathic dilated cardiomyopathy is linked to 5′terminal genomic RNA-deleted viral populations with viral-encoded proteinase activities. Circulation 2019, 139, 2326–2338. [Google Scholar] [CrossRef]
- Chapman, N.; Kim, K.-S. Persistent coxsackievirus infection: Enterovirus persistence in chronic myocarditis and dilated cardiomyopathy. In Group B Coxsackieviruses; Springer: Berlin/Heidelberg, Germany, 2008; pp. 275–292. [Google Scholar] [CrossRef]
- Rose, N.R. Viral myocarditis. Curr. Opin. Rheumatol. 2016, 28, 383. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.P., Jr.; Baden, L.; Pallansch, M.A.; Anderson, L.J. Enterovirus 71 infections and neurologic disease—United States, 1977–1991. J. Infect. Dis. 1994, 169, 905–908. [Google Scholar] [CrossRef]
- Li, Y.; Bourlet, T.; Andreoletti, L.; Mosnier, J.-F.; Peng, T.; Yang, Y.; Archard, L.C.; Pozzetto, B.; Zhang, H. Enteroviral capsid protein VP1 is present in myocardial tissues from some patients with myocarditis or dilated cardiomyopathy. Circulation 2000, 101, 231–234. [Google Scholar] [CrossRef]
- Allen, D.W.; Kim, K.W.; Rawlinson, W.D.; Craig, M.E. Maternal virus infections in pregnancy and type 1 diabetes in their offspring: Systematic review and meta-analysis of observational studies. Rev. Med. Virol. 2018, 28, e1974. [Google Scholar] [CrossRef] [PubMed]
- Hober, D.; Sane, F. Enteroviral pathogenesis of type 1 diabetes. Discov. Med. 2010, 10, 151–160. [Google Scholar] [CrossRef]
- Honkanen, H.-R. Epidemiology of Enteroviruses and Their Association with Type 1 Diabetes in Finland; Tampere University Press: Tampere, Finland, 2016. [Google Scholar]
- Viskari, H.; Ludvigsson, J.; Uibo, R.; Salur, L.; Marciulionyte, D.; Hermann, R.; Soltesz, G.; Füchtenbusch, M.; Ziegler, A.G.; Kondrashova, A. Relationship between the incidence of type 1 diabetes and enterovirus infections in different European populations: Results from the EPIVIR project. J. Med. Virol. 2004, 72, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Carré, A.; Vecchio, F.; Flodström-Tullberg, M.; You, S.; Mallone, R. Coxsackievirus and type 1 diabetes: Diabetogenic mechanisms and implications for prevention. Endocr. Rev. 2023, 44, 737–751. [Google Scholar] [CrossRef] [PubMed]
- Nekoua, M.P.; Alidjinou, E.K.; Hober, D. Persistent coxsackievirus B infection and pathogenesis of type 1 diabetes mellitus. Nat. Rev. Endocrinol. 2022, 18, 503–516. [Google Scholar] [CrossRef] [PubMed]
- Wikswo, M.E.; Khetsuriani, N.; Fowlkes, A.L.; Zheng, X.; Penaranda, S.; Verma, N.; Shulman, S.T.; Sircar, K.; Robinson, C.C.; Schmidt, T. Increased Activity of Coxsackievirus B1 Strains Associated with Severe Disease among Young Infants in the United States, 2007—2008. Clin. Infect. Dis. 2009, 49, e44–e51. [Google Scholar] [CrossRef]
- Pons-Salort, M.; Grassly, N.C. Serotype-specific immunity explains the incidence of diseases caused by human enteroviruses. Science 2018, 361, 800–803. [Google Scholar] [CrossRef]
- SHINGU, M. Studies on the complement fixation test with enteroviruses. Effects of heating antigens at various temperatures on their complement fixing ability. Kurume Med. J. 1961, 8, 43–60. [Google Scholar] [CrossRef]
- Rigonan, A.S.; Mann, L.; Chonmaitree, T. Use of monoclonal antibodies to identify serotypes of enterovirus isolates. J. Clin. Microbiol. 1998, 36, 1877–1881. [Google Scholar] [CrossRef]
- Spickard, A.; Evans, H.; Knight, V.; Johnson, K. Acute respiratory disease in normal volunteers associated with Coxsackie A-21 viral infection. III. Response to nasopharyngeal and enteric inoculation. J. Clin. Investig. 1963, 42, 840–852. [Google Scholar] [CrossRef] [PubMed]
- Couch, R.B.; Cate, T.R.; Douglas Jr, R.G.; Gerone, P.J.; Knight, V. Effect of route of inoculation on experimental respiratory viral disease in volunteers and evidence for airborne transmission. Bacteriol. Rev. 1966, 30, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Dörries, R.; Ter Meulen, V. Specificity of IgM antibodies in acute human coxsackievirus B infections, analysed by indirect solid phase enzyme immunoassay and immunoblot technique. J. Gen. Virol. 1983, 64, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Muir, P.; Singh, N.B.; Banatvala, J.E. Enterovirus-specific serum IgA antibody responses in patients with acute infections, chronic cardiac disease, and recently diagnosed insulin-dependent diabetes mellitus. J. Med. Virol. 1990, 32, 236–242. [Google Scholar] [CrossRef]
- Dotzauer, A.; Kraemer, L. Innate and adaptive immune responses against picornaviruses and their counteractions: An overview. World J. Virol. 2012, 1, 91–107. [Google Scholar] [CrossRef]
- Lodge, P.A.; Herzum, M.; Olszewski, J.; Huber, S. Coxsackievirus B-3 myocarditis. Acute and chronic forms of the disease caused by different immunopathogenic mechanisms. Am. J. Pathol. 1987, 128, 455. [Google Scholar]
- Mao, Q.-y.; Wang, Y.; Bian, L.; Xu, M.; Liang, Z. EV71 vaccine, a new tool to control outbreaks of hand, foot and mouth disease (HFMD). Expert Rev. Vaccines 2016, 15, 599–606. [Google Scholar] [CrossRef]
- Wong, S.; Yip, C.; Lau, S.; Yuen, K. Human enterovirus 71 and hand, foot and mouth disease. Epidemiol. Infect. 2010, 138, 1071–1089. [Google Scholar] [CrossRef]
- De, W.; Changwen, K.; Wei, L.; Monagin, C.; Jin, Y.; Cong, M.; Hanri, Z.; Jun, S. A large outbreak of hand, foot, and mouth disease caused by EV71 and CAV16 in Guangdong, China, 2009. Arch. Virol. 2011, 156, 945–953. [Google Scholar] [CrossRef]
- Chan, K.P.; Goh, K.T.; Chong, C.Y.; Teo, E.S.; Lau, G.; Ling, A.E. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore. Emerg. Infect. Dis. 2003, 9, 78–85. [Google Scholar] [CrossRef]
- Cai, K.; Wang, Y.; Guo, Z.; Yu, H.; Li, H.; Zhang, L.; Xu, S.; Zhang, Q. Clinical characteristics and managements of severe hand, foot and mouth disease caused by enterovirus A71 and coxsackievirus A16 in Shanghai, China. BMC Infect. Dis. 2019, 19, 285. [Google Scholar] [CrossRef] [PubMed]
- Kamau, E.; Nguyen, D.; Celma, C.; Blomqvist, S.; Horby, P.; Simmonds, P.; Harvala, H. Seroprevalence and virologic surveillance of Enterovirus 71 and Coxsackievirus A6, United Kingdom, 2006–2017. Emerg. Infect. Dis. 2021, 27, 2261. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Chen, P.; Bai, Y.; Xu, X.; Liu, Y. Seroprevalence of coxsackievirus A6 and enterovirus A71 infection in humans: A systematic review and meta-analysis. Arch. Virol. 2023, 168, 37. [Google Scholar] [CrossRef]
- Lin, T.-L.; Li, Y.-S.; Huang, C.-W.; Hsu, C.-C.; Wu, H.-S.; Tseng, T.-C.; Yang, C.-F. Rapid and highly sensitive coxsackievirus a indirect immunofluorescence assay typing kit for enterovirus serotyping. J. Clin. Microbiol. 2008, 46, 785–788. [Google Scholar] [CrossRef]
- Glenet, M.; Heng, L.; Callon, D.; Lebreil, A.-L.; Gretteau, P.-A.; Nguyen, Y.; Berri, F.; Andreoletti, L. Structures and functions of viral 5′ non-coding genomic RNA domain-I in group-B enterovirus infections. Viruses 2020, 12, 919. [Google Scholar] [CrossRef] [PubMed]
- Donelan, S.V.; Spitzer, S.; Spitzer, E. 2799. Inability to Locally Differentiate Rhinovirus/Enterovirus Results Impacts Infection Control Practices. Open Forum Infect. Dis. 2019, 6, S989–S990. [Google Scholar] [CrossRef]
- Oikarinen, S.; Tauriainen, S.; Hober, D.; Lucas, B.; Vazeou, A.; Sioofy-Khojine, A.; Bozas, E.; Muir, P.; Honkanen, H.; Ilonen, J. Virus antibody survey in different European populations indicates risk association between coxsackievirus B1 and type 1 diabetes. Diabetes 2014, 63, 655–662. [Google Scholar] [CrossRef]
- Sciandra, I.; Falasca, F.; Maida, P.; Tranquilli, G.; Di Carlo, D.; Mazzuti, L.; Melengu, T.; Giannelli, G.; Antonelli, G.; Turriziani, O. Seroprevalence of group B Coxsackieviruses: Retrospective study in an Italian population. J. Med. Virol. 2020, 92, 3138–3143. [Google Scholar] [CrossRef]
- Mavrouli, M.; Spanakis, N.; Levidiotou, S.; Politi, C.; Alexiou, S.; Tseliou, P.; Hatzitaki, M.; Foundouli, K.; Tsakris, A.; Legakis, N. Serologic prevalence of coxsackievirus group B in Greece. Viral Immunol. 2007, 20, 11–18. [Google Scholar] [CrossRef]
- Terletskaia-Ladwig, E.; Metzger, C.; Schalasta, G.; Enders, G. Evaluation of enterovirus serological tests IgM-EIA and complement fixation in patients with meningitis, confirmed by detection of enteroviral RNA by RT-PCR in cerebrospinal fluid. J. Med. Virol. 2000, 61, 221–227. [Google Scholar] [CrossRef]
- Harvala, H.; Broberg, E.; Benschop, K.; Berginc, N.; Ladhani, S.; Susi, P.; Christiansen, C.; McKenna, J.; Allen, D.; Makiello, P. Recommendations for enterovirus diagnostics and characterisation within and beyond Europe. J. Clin. Virol. 2018, 101, 11–17. [Google Scholar] [CrossRef]
- Committee on Infectious Diseases 2018–2021. Enterovirus (nonpoliovirus). In Red Book: 2021–2024 Report of the Committee on Infectious Diseases, 32nd ed.; Kimberlin, D.W., Barnett, E.D., Lynfield, R., Sawyer, M.H., Eds.; American Academy of Pediatrics: Itasca, IL, USA, 2021; pp. 315–318. [Google Scholar]
- Falsey, A.R.; Cameron, A.; Branche, A.R.; Walsh, E.E. Perturbations in respiratory syncytial virus activity during the SARS-CoV-2 pandemic. J. Infect. Dis. 2023, 227, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.-C.; Lin, K.-P.; Wang, L.-A.; Yeh, T.-K.; Liu, P.-Y. The Impact of the COVID-19 pandemic on respiratory syncytial virus infection: A narrative review. Infect. Drug Resist. 2023, 16, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Redlberger-Fritz, M.; Kundi, M.; Aberle, S.W.; Puchhammer-Stöckl, E. Significant impact of nationwide SARS-CoV-2 lockdown measures on the circulation of other respiratory virus infections in Austria. J. Clin. Virol. 2021, 137, 104795. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
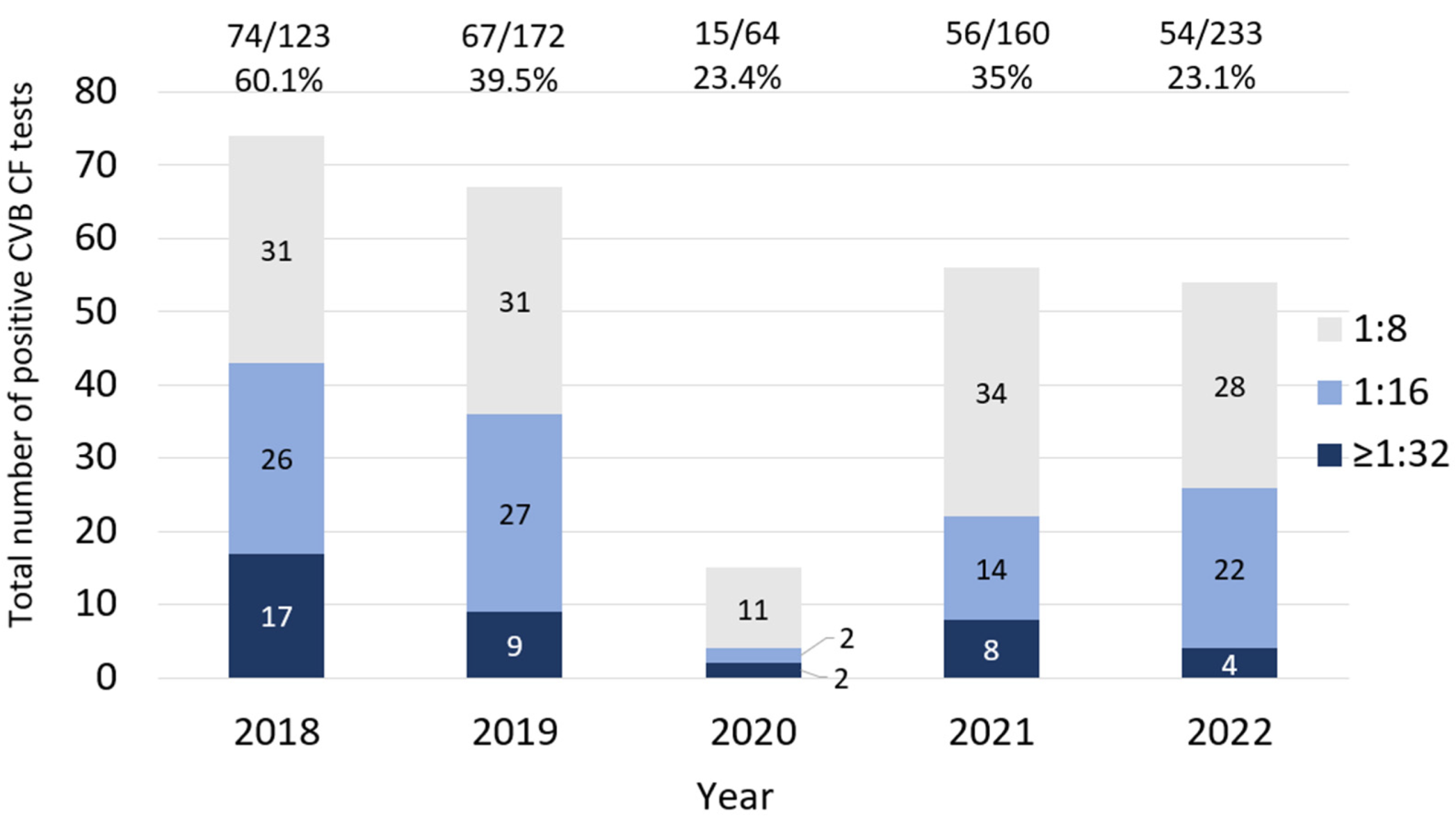
| Serotype | Year/Total Tests | |||||
|---|---|---|---|---|---|---|
| 2018 123 * | 2019 172 | 2020 64 | 2021 160 | 2022 233 | Total 752 | |
| B1 | 16 | 9 | 3 | 16 | 10 | 54 |
| B2 | 12 | 13 | 3 | 10 | 10 | 48 |
| B3 | 10 | 8 | 1 | 3 | 8 | 30 |
| B4 | 7 | 8 | 0 | 3 | 3 | 21 |
| B5 | 16 | 14 | 3 | 14 | 15 | 62 |
| B6 | 13 | 15 | 5 | 10 | 8 | 51 |
| Total positive % positive | 74 (60.1%) | 67 (39%) | 15 (23.4%) | 56 (35%) | 54 (23.1%) | 266 (35.3%) |
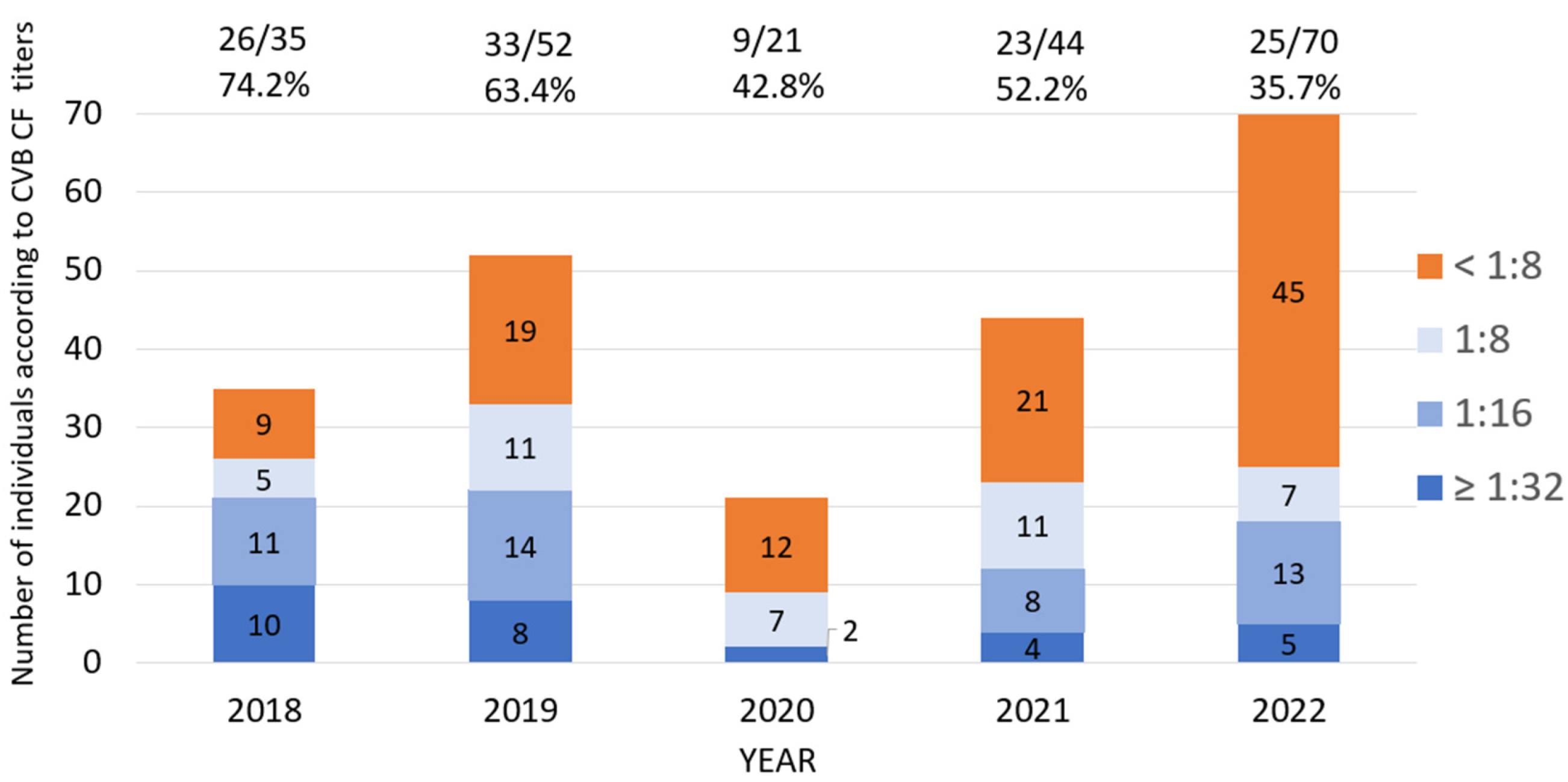
| Factor | Positive/Total n (%) | OR * | 95% CI ** | p-Value *** |
| Age: | ||||
| 0–20 | 15/27 (55.6) | 1 | - | - |
| 21–40 | 48/85 (56.5) | 0.93 | 0.43–2.48 | 0.93 |
| 41–60 | 44/80 (55) | 0.97 | 0.40–2.35 | 0.96 |
| 60+ | 10/30 (35.5) | 0.4 | 0.13–1.17 | 0.09 |
| Year: | ||||
| 2018 | 26/35 (74.2) | 1 | - | - |
| 2019 | 33/52 (63.5) | 0.55 | 0.21–1.42 | 0.29 |
| 2020 | 9/21 (42.9) | 0.26 | 0.08–0.82 | 0.02 |
| 2021 | 23/44 (52.2) | 0.38 | 0.14–0.95 | 0.04 |
| 2022 | 25/70 (35.7) | 0.19 | 0.07–0.47 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kordi, R.; Chang, A.J.; Hicar, M.D. Seasonal Testing, Results, and Effect of the Pandemic on Coxsackievirus Serum Studies. Microorganisms 2024, 12, 367. https://doi.org/10.3390/microorganisms12020367
Kordi R, Chang AJ, Hicar MD. Seasonal Testing, Results, and Effect of the Pandemic on Coxsackievirus Serum Studies. Microorganisms. 2024; 12(2):367. https://doi.org/10.3390/microorganisms12020367
Chicago/Turabian StyleKordi, Ramesh, Arthur J. Chang, and Mark D. Hicar. 2024. "Seasonal Testing, Results, and Effect of the Pandemic on Coxsackievirus Serum Studies" Microorganisms 12, no. 2: 367. https://doi.org/10.3390/microorganisms12020367
APA StyleKordi, R., Chang, A. J., & Hicar, M. D. (2024). Seasonal Testing, Results, and Effect of the Pandemic on Coxsackievirus Serum Studies. Microorganisms, 12(2), 367. https://doi.org/10.3390/microorganisms12020367