Risk Factors for Long-Term Vancomycin-Resistant Enterococci Persistence—A Prospective Longitudinal Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Setting and Infection Control Measures
2.2. Detection of VRE Long-Term Carriers
2.3. VRE Swab Samples, Culturing, Antibiotic Susceptibility Testing, PCR Testing
2.4. Whole Genome Sequence-Based Typing
2.5. Statistical Analysis
3. Results
3.1. VRE Persistence and Associated Risk Factors
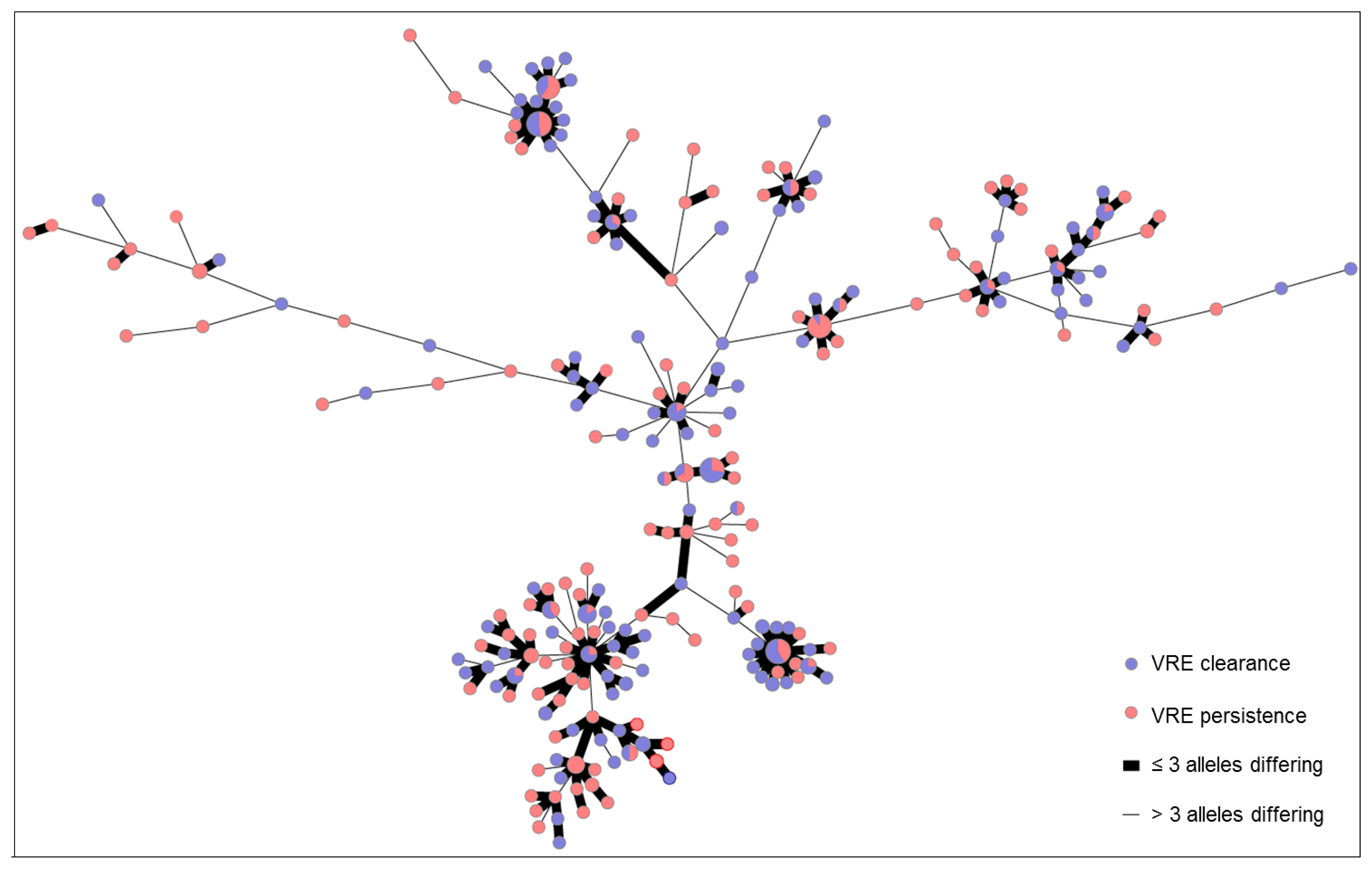
3.2. VRE Genotypes and Genetic Distribution of Strains
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Uttley, A.H.; Collins, C.H.; Naidoo, J.; George, R.C. Vancomycin-resistant enterococci. Lancet 1988, 1, 57–58. [Google Scholar] [CrossRef]
- Leclercq, R.; Derlot, E.; Duval, J.; Courvalin, P. Plasmid-mediated resistance to vancomycin and teicoplanin in Enterococcus faecium. N. Engl. J. Med. 1988, 319, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Remschmidt, C.; Schröder, C.; Behnke, M.; Gastmeier, P.; Geffers, C.; Kramer, T.S. Continuous increase of vancomycin resistance in enterococci causing nosocomial infections in Germany−10 years of surveillance. Antimicrob. Resist. Infect. Control 2018, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Cormican, M.; Flamm, R.K.; Mendes, R.E.; Jones, R.N. Temporal and Geographic Variation in Antimicrobial Susceptibility and Resistance Patterns of Enterococci: Results from the SENTRY Antimicrobial Surveillance Program, 1997–2016. Open Forum Infect. Dis. 2019, 6, S54–S62. [Google Scholar] [CrossRef] [PubMed]
- Cafini, F.; Nguyen le, T.T.; Higashide, M.; Roman, F.; Prieto, J.; Morikawa, K. Horizontal gene transmission of the cfr gene to MRSA and Enterococcus: Role of Staphylococcus epidermidis as a reservoir and alternative pathway for the spread of linezolid resistance. J. Antimicrob. Chemother. 2016, 71, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Juhas, M. Horizontal gene transfer in human pathogens. Crit. Rev. Microbiol. 2015, 41, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Willems, R.J.; Top, J.; Marga van Santen, D.; Coque, T.M.; Baquero, F.; Grundmann, H.; Bonten, M.J. Global spread of vancomycin-resistant Enterococcus faecium from distinct nosocomial genetic complex. Emerg. Infect. Dis. 2005, 11, 821. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.J.; Li, J.; Salmasian, H.; Zachariah, P.; Yang, Y.X.; Freedberg, D.E. The local hospital milieu and healthcare-associated vancomycin-resistant enterococcus acquisition. J. Hosp. Infect. 2019, 101, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Bonten, M.J.; Slaughter, S.; Ambergen, A.W.; Hayden, M.K.; van Voorhis, J.; Nathan, C.; Weinstein, R.A. The role of “colonization pressure” in the spread of vancomycin-resistant enterococci: An important infection control variable. Arch. Intern. Med. 1998, 158, 1127–1132. [Google Scholar] [CrossRef]
- Ford, C.D.; Lopansri, B.K.; Gazdik, M.A.; Webb, B.; Snow, G.L.; Hoda, D.; Adams, B.; Petersen, F.B. Room contamination, patient colonization pressure, and the risk of vancomycin-resistant Enterococcus colonization on a unit dedicated to the treatment of hematologic malignancies and hematopoietic stem cell transplantation. Am. J. Infect. Control 2016, 44, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- Zacharioudakis, I.M.; Zervou, F.N.; Ziakas, P.D.; Rice, L.B.; Mylonakis, E. Vancomycin-resistant enterococci colonization among dialysis patients: A meta-analysis of prevalence, risk factors, and significance. Am. J. Kidney Dis. 2015, 65, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou-Olivgeris, M.; Drougka, E.; Fligou, F.; Kolonitsiou, F.; Liakopoulos, A.; Dodou, V.; Anastassiou, E.D.; Petinaki, E.; Marangos, M.; Filos, K.S.; et al. Risk factors for enterococcal infection and colonization by vancomycin-resistant enterococci in critically ill patients. Infection 2014, 42, 1013–1022. [Google Scholar] [CrossRef]
- D’Agata, E.M.; Green, W.K.; Schulman, G.; Li, H.; Tang, Y.W.; Schaffner, W. Vancomycin-resistant enterococci among chronic hemodialysis patients: A prospective study of acquisition. Clin. Infect. Dis. 2001, 32, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Remschmidt, C.; Behnke, M.; Kola, A.; Pena Diaz, L.A.; Rohde, A.M.; Gastmeier, P.; Schwab, F. The effect of antibiotic use on prevalence of nosocomial vancomycin-resistant enterococci—An ecologic study. Antimicrob. Resist. Infect. Control 2017, 6, 95. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.C.; Wang, J.T.; Chen, Y.C.; Chang, Y.Y.; Chen, M.L.; Chang, S.C. Incidence of and risk factors for infection or colonization of vancomycin-resistant enterococci in patients in the intensive care unit. PLoS ONE 2012, 7, e47297. [Google Scholar] [CrossRef] [PubMed]
- Ford, C.D.; Lopansri, B.K.; Haydoura, S.; Snow, G.; Dascomb, K.K.; Asch, J.; Bo Petersen, F.; Burke, J.P. Frequency, risk factors, and outcomes of vancomycin-resistant Enterococcus colonization and infection in patients with newly diagnosed acute leukemia: Different patterns in patients with acute myelogenous and acute lymphoblastic leukemia. Infect. Control Hosp. Epidemiol. 2015, 36, 47–53. [Google Scholar] [CrossRef]
- Carmeli, Y.; Eliopoulos, G.M.; Samore, M.H. Antecedent treatment with different antibiotic agents as a risk factor for vancomycin-resistant Enterococcus. Emerg. Infect. Dis. 2002, 8, 802. [Google Scholar] [CrossRef]
- Patterson, J.E. Antibiotic utilization: Is there an effect on antimicrobial resistance? Chest 2001, 119, 426S–430S. [Google Scholar] [CrossRef]
- Ott, M.; Wirick, H. Vancomycin-resistant enterococci (VRE) and the role of the healthcare worker. Can. Oper. Room Nurs. J. 2008, 26, 21–24. [Google Scholar]
- Jackson, S.S.; Harris, A.D.; Magder, L.S.; Stafford, K.A.; Johnson, J.K.; Miller, L.G.; Calfee, D.P.; Thom, K.A. Bacterial burden is associated with increased transmission to health care workers from patients colonized with vancomycin-resistant Enterococcus. Am. J. Infect. Control 2019, 47, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Suleyman, G.; Alangaden, G.; Bardossy, A.C. The Role of Environmental Contamination in the Transmission of Nosocomial Pathogens and Healthcare-Associated Infections. Curr. Infect. Dis. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Chemaly, R.F.; Simmons, S.; Dale, C., Jr.; Ghantoji, S.S.; Rodriguez, M.; Gubb, J.; Stachowiak, J.; Stibich, M. The role of the healthcare environment in the spread of multidrug-resistant organisms: Update on current best practices for containment. Ther. Adv. Infect. Dis. 2014, 2, 79–90. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, G.; Cataldo, M.A.; De Waure, C.; Venturiello, S.; La Torre, G.; Cauda, R.; Carmeli, Y.; Tacconelli, E. Infection control and prevention measures to reduce the spread of vancomycin-resistant enterococci in hospitalized patients: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2014, 69, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Biehl, L.M.; Bertz, H.; Bogner, J.; Dobermann, U.H.; Kessel, J.; Kramer, C.; Lemmen, S.; von Lilienfeld-Toal, M.; Peter, S.; Pletz, M.W.; et al. Screening and contact precautions—A survey on infection control measures for multidrug-resistant bacteria in German university hospitals. Antimicrob. Resist. Infect. Control 2017, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- RKI. Hygienemaßnahmen zur Prävention der Infektion durch Enterokokken mit speziellen Antibiotikaresistenzen. Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert-Koch-Institut. Bundesgesundheitsblatt 2018, 61, 1310–1361. [Google Scholar] [CrossRef] [PubMed]
- Sprague, E.; Reynolds, S.; Brindley, P. Patient Isolation Precautions: Are They Worth It? Can. Respir. J. 2016, 2016, 5352625. [Google Scholar] [CrossRef]
- Favero, M.S.; Gaynes, R.P.; Jarvis, W.R.; Shaw, J.; Tablan, O.C.; Tenover, F.C. Recommendations for preventing the spread of vancomycin resistance; recommendations of the Hospital Infection Control Practices Advisory Committee (HICPAC). Am. J. Infect. Control 1995, 23, 87–94. [Google Scholar]
- Shenoy, E.S.; Paras, M.L.; Noubary, F.; Walensky, R.P.; Hooper, D.C. Natural history of colonization with methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE): A systematic review. BMC Infect. Dis. 2014, 14, 177. [Google Scholar] [CrossRef]
- Ruscher, C. Empfehlungen zur Prävention und Kontrolle von Methicillin-resistenten Staphylococcus aureus-Stämmen (MRSA) in medizinischen und pflegerischen Einrichtungen. Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 695–732. [Google Scholar] [CrossRef]
- Wendt, C.; Baum, H.; Kaase, M.; Meyer, E.; Suger-Wiedeck, H.; Ruscher, C. Hygienemaßnahmen bei Infektionen oder Besiedlung mit multiresistenten gramnegativen Stäbchen: Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut (RKI). Bundesgesundsheitsblatt 2012, 55, 1311–1354. [Google Scholar]
- Sohn, K.M.; Peck, K.R.; Joo, E.J.; Ha, Y.E.; Kang, C.I.; Chung, D.R.; Lee, N.Y.; Song, J.H. Duration of colonization and risk factors for prolonged carriage of vancomycin-resistant enterococci after discharge from the hospital. Int. J. Infect. Dis. 2013, 17, e240–e246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampmeier, S.; Kossow, A.; Clausen, L.M.; Knaack, D.; Ertmer, C.; Gottschalk, A.; Freise, H.; Mellmann, A. Hospital acquired vancomycin resistant enterococci in surgical intensive care patients—a prospective longitudinal study. Antimicrob. Resist. Infect. Control 2018, 7, 103. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Dobele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 9.0. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_9.0_Breakpoint_Tables.pdf (accessed on 4 July 2019).
- Mellmann, A.; Bletz, S.; Boking, T.; Kipp, F.; Becker, K.; Schultes, A.; Prior, K.; Harmsen, D. Real-Time Genome Sequencing of Resistant Bacteria Provides Precision Infection Control in an Institutional Setting. J. Clin. Microbiol. 2016, 54, 2874–2881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Been, M.; Pinholt, M.; Top, J.; Bletz, S.; Mellmann, A.; van Schaik, W.; Brouwer, E.; Rogers, M.; Kraat, Y.; Bonten, M.; et al. Core Genome Multilocus Sequence Typing Scheme for High- Resolution Typing of Enterococcus faecium. J. Clin. Microbiol. 2015, 53, 3788–3797. [Google Scholar] [CrossRef]
- Baden, L.R.; Thiemke, W.; Skolnik, A.; Chambers, R.; Strymish, J.; Gold, H.S.; Moellering, R.C., Jr.; Eliopoulos, G.M. Prolonged colonization with vancomycin-resistant Enterococcus faecium in long-term care patients and the significance of “clearance”. Clin. Infect. Dis. 2001, 33, 1654–1660. [Google Scholar] [CrossRef]
- Patel, R.; Allen, S.L.; Manahan, J.M.; Wright, A.J.; Krom, R.A.; Wiesner, R.H.; Persing, D.H.; Cockerill, F.R.; Thompson, R.L. Natural history of vancomycin-resistant enterococcal colonization in liver and kidney transplant recipients. Liver Transpl. 2001, 7, 27–31. [Google Scholar] [CrossRef]
- Klare, I.; Bender, J.K.; Werner, G.; Koppe, U.; Sin, M.A.; Eckmanns, T. Eigenschaften, Häufigkeit und Verbreitung von Vancomycinresistenten Enterokokken (VRE) in Deutschland. Epi. Bull. 2017, 46, 519–530. [Google Scholar]
- Monteserin, N.; Larson, E. Temporal trends and risk factors for healthcare-associated vancomycin-resistant enterococci in adults. J. Hosp. Infect. 2016, 94, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Faron, M.L.; Ledeboer, N.A.; Buchan, B.W. Resistance Mechanisms, Epidemiology, and Approaches to Screening for Vancomycin-Resistant Enterococcus in the Health Care Setting. J. Clin. Microbiol. 2016, 54, 2436–2447. [Google Scholar] [CrossRef] [PubMed]
- Van Harten, R.M.; Willems, R.J.L.; Martin, N.I.; Hendrickx, A.P.A. Multidrug-Resistant Enterococcal Infections: New Compounds, Novel Antimicrobial Therapies? Trends Microbiol. 2017, 25, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Yarlagadda, V.; Sarkar, P.; Samaddar, S.; Haldar, J. A Vancomycin Derivative with a Pyrophosphate-Binding Group: A Strategy to Combat Vancomycin-Resistant Bacteria. Angew. Chem. Int. Ed. Engl. 2016, 55, 7836–7840. [Google Scholar] [CrossRef] [PubMed]
- Martin, E.M.; Bryant, B.; Grogan, T.R.; Rubin, Z.A.; Russell, D.L.; Elashoff, D.; Uslan, D.Z. Noninfectious Hospital Adverse Events Decline After Elimination of Contact Precautions for MRSA and VRE. Infect. Control Hosp. Epidemiol. 2018, 39, 788–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zachariah, P.; Freedberg, D.E. Vancomycin use in surrounding patients during critical illness and risk for persistent colonization with vancomycin-resistant Enterococcus. J. Hosp. Infect. 2019, 102, 343–346. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Characteristic | VRE-Persistence (n = 202) | VRE-Clearance (n = 261) | p-Value |
|---|---|---|---|
| Sex (male) | 57.4% | 60.5% | 0.50 |
| Age (years) | 59.7 (range 1.8–93.1) | 55.7 (range 0.6–97.7) | 0.02 |
| Overall length of stay (days) | 76.4 (range: 1–478) | 37.8 (range 1–216) | 0.001 |
| Average length of stay per admission (days) | 35.3 (1–340) | 20.1 (1–188) | 0.001 |
| Number of stays | 3.3 (range: 1–29) | 2.3 (range: 1–10) | 0.001 |
| Hemato-oncological disease | 119 (58.9%) | 122 (46.7%) | 0.01 |
| Liver insufficiency | 41 (20.3%) | 43 (16.5%) | 0.29 |
| Liver transplantation | 9 (4.5%) | 22 (8.4%) | 0.09 |
| Kidney insufficiency | 88 (43.6%) | 114 (43.7%) | 0.98 |
| Dialysis | 37 (18.3%) | 35 (13.4%) | 0.15 |
| Immunosuppressive disease | 143 (70.8%) | 169 (64.8%) | 0.17 |
| Inflammatory bowel disease | 2 (1.0%) | 5 (1.9%) | 0.47 |
| Rheumatic disease | 1 (0.5%) | 5 (1.9%) | 0.24 |
| Granulomatosis with polyangiitis | 1 (0.5%) | 1 (0.4%) | 1.00 |
| HIV | 1 (0.5%) | 2 (0.8%) | 0.58 |
| Systemic lupus erythematosus | 1 (0.5%) | 1 (0.4%) | 1.00 |
| Idiopathic thrombocytic purpura | 0 (0.0%) | 1 (0.4%) | 1.00 |
| Transplantation | 20 (10.0%) | 39 (14.9%) | 0.13 |
| Multiple sclerosis | 1 (0.5%) | 1 (0.4%) | 1.00 |
| Systemic scleroderma | 1 (0.5%) | 0 (0.0%) | 0.44 |
| Antibiotics | 191 (94.6%) | 222 (85.1%) | 0.001 |
| Penicillin | 9 (4.5%) | 8 (3.1%) | 0.46 |
| Ampicillin | 12 (5.9%) | 8 (3.1%) | 0.17 |
| Amoxicillin | 5 (2.5%) | 6 (2.3%) | 1.00 |
| Ampicillin/sulbactam | 14 (6.9%) | 20 (7.7%) | 0.86 |
| Amoxicillin/clavulanic acid | 17 (8.4%) | 16 (6.1%) | 0.37 |
| Flucloxacillin | 18 (8.9%) | 18 (6.9%) | 0.48 |
| Piperacillin/tazobactam | 145 (71.3%) | 134 (51.3%) | <0.001 |
| Cefuroxime | 19 (9.4%) | 24 (9.2%) | 1.00 |
| Ceftriaxone | 43 (21.3%) | 36 (13.8%) | 0.03 |
| Ciprofloxacin | 109 (54.0%) | 76 (29.1%) | <0.001 |
| Erythromycin | 9 (4.5%) | 10 (3.8%) | 0.82 |
| Clindamycin | 35 (17.3%) | 21 (0.8%) | 0.004 |
| Colistin | 8 (4.0%) | 3 (0.1%) | 0.06 |
| Trimethoprim/sulfamethoxazole | 102 (50.5%) | 88 (33.7%) | <0.001 |
| Metronidazole | 20 (9.9%) | 18 (6.9%) | 0.31 |
| Rifampicin | 17 (8.4%) | 18 (6.9%) | 0.60 |
| Fosfomycin | 10 (5.0%) | 10 (3.8%) | 0.65 |
| Vancomycin | 92 (45.5%) | 59 (22.6%) | <0.001 |
| Duration of treatment with antibiotics (days) | 97.7 (range: 0–430) | 25.0 (range: 0–372) | <0.001 |
| Systemic steroids | 121 (59.9%) | 116 (44.4%) | 0.001 |
| Admission from another hospital | 62 (30.7%) | 60 (23%) | 0.06 |
| Admission from other ICUs | 2 (1.0%) | 9 (3.4%) | 0.09 |
| Colonization Status | No. of Patients with Van Genotype (%) | ||||
|---|---|---|---|---|---|
| vanA | vanB | vanA + vanB | No Genotype Data Available | Total | |
| VRE-persistence | 58 (28.7%) | 142 (70.3%) | 2 (1.0%) | 0 (0.0%) | 202 (43.6%) |
| VRE-clearance | 64 (24.5%) | 186 (71.3%) | 2 (1.0%) | 9 (3.4%) | 261 (56.4%) |
| Total | 122 (26.3%) | 328 (70.8%) | 4 (1.0%) | 9 (1.9%) | 463 (100%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correa-Martinez, C.L.; Stollenwerk, V.B.; Kossow, A.; Schaumburg, F.; Mellmann, A.; Kampmeier, S. Risk Factors for Long-Term Vancomycin-Resistant Enterococci Persistence—A Prospective Longitudinal Study. Microorganisms 2019, 7, 400. https://doi.org/10.3390/microorganisms7100400
Correa-Martinez CL, Stollenwerk VB, Kossow A, Schaumburg F, Mellmann A, Kampmeier S. Risk Factors for Long-Term Vancomycin-Resistant Enterococci Persistence—A Prospective Longitudinal Study. Microorganisms. 2019; 7(10):400. https://doi.org/10.3390/microorganisms7100400
Chicago/Turabian StyleCorrea-Martinez, Carlos L., Verena B. Stollenwerk, Annelene Kossow, Frieder Schaumburg, Alexander Mellmann, and Stefanie Kampmeier. 2019. "Risk Factors for Long-Term Vancomycin-Resistant Enterococci Persistence—A Prospective Longitudinal Study" Microorganisms 7, no. 10: 400. https://doi.org/10.3390/microorganisms7100400
APA StyleCorrea-Martinez, C. L., Stollenwerk, V. B., Kossow, A., Schaumburg, F., Mellmann, A., & Kampmeier, S. (2019). Risk Factors for Long-Term Vancomycin-Resistant Enterococci Persistence—A Prospective Longitudinal Study. Microorganisms, 7(10), 400. https://doi.org/10.3390/microorganisms7100400