
The Use of Platelet-Rich Plasma for Treatment of Tenodesmic Lesions in Horses: A Systematic Review and Meta-Analysis of Clinical and Experimental Data

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Studies for This Review
2.2. Data Extraction and Management
2.3. Types of Studies and Participants
2.4. Types of Interventions
2.5. Types of Outcome Measures
2.6. Measures of Treatment Effect and Assessment of Heterogeneity
2.7. Risk of Bias
3. Results
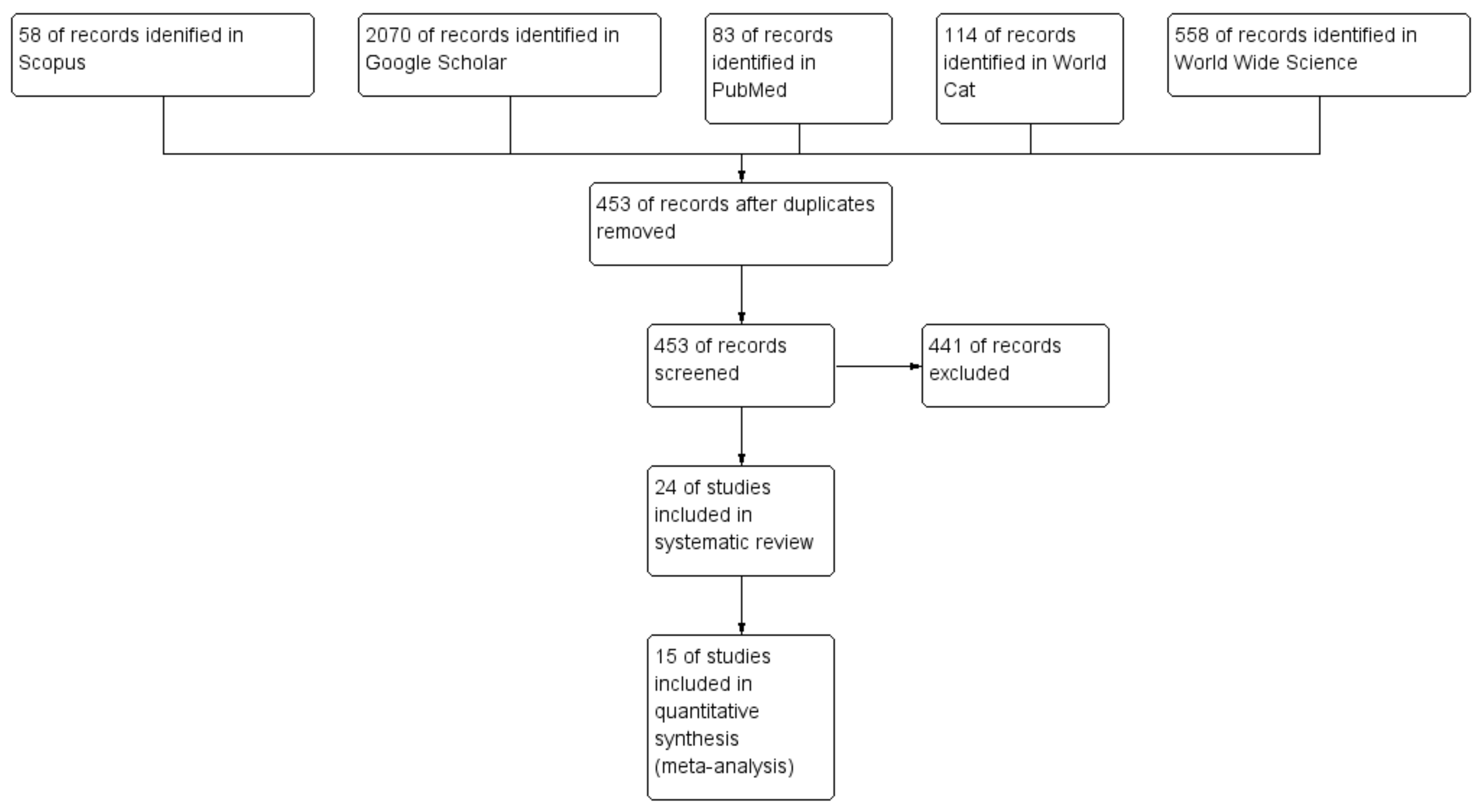
3.1. Systematic Review
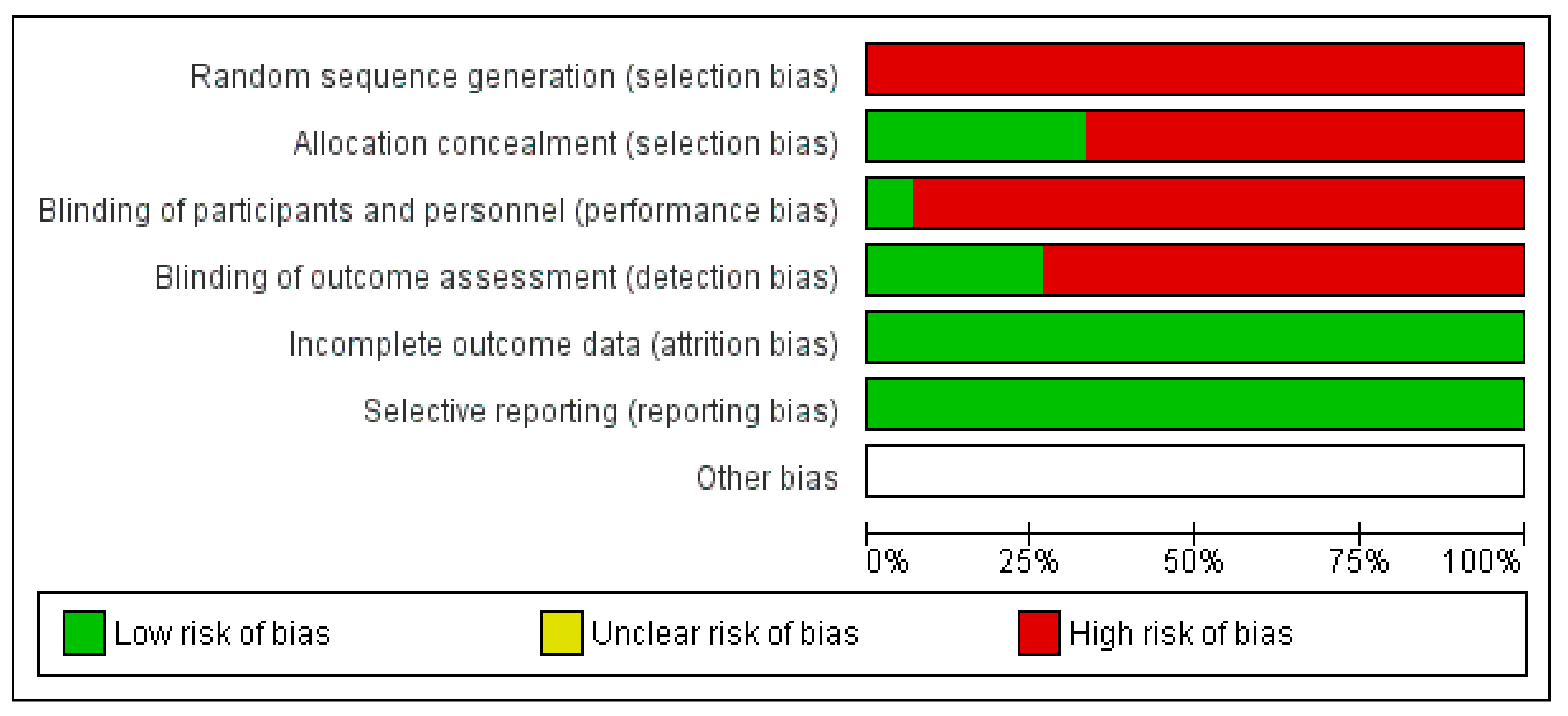
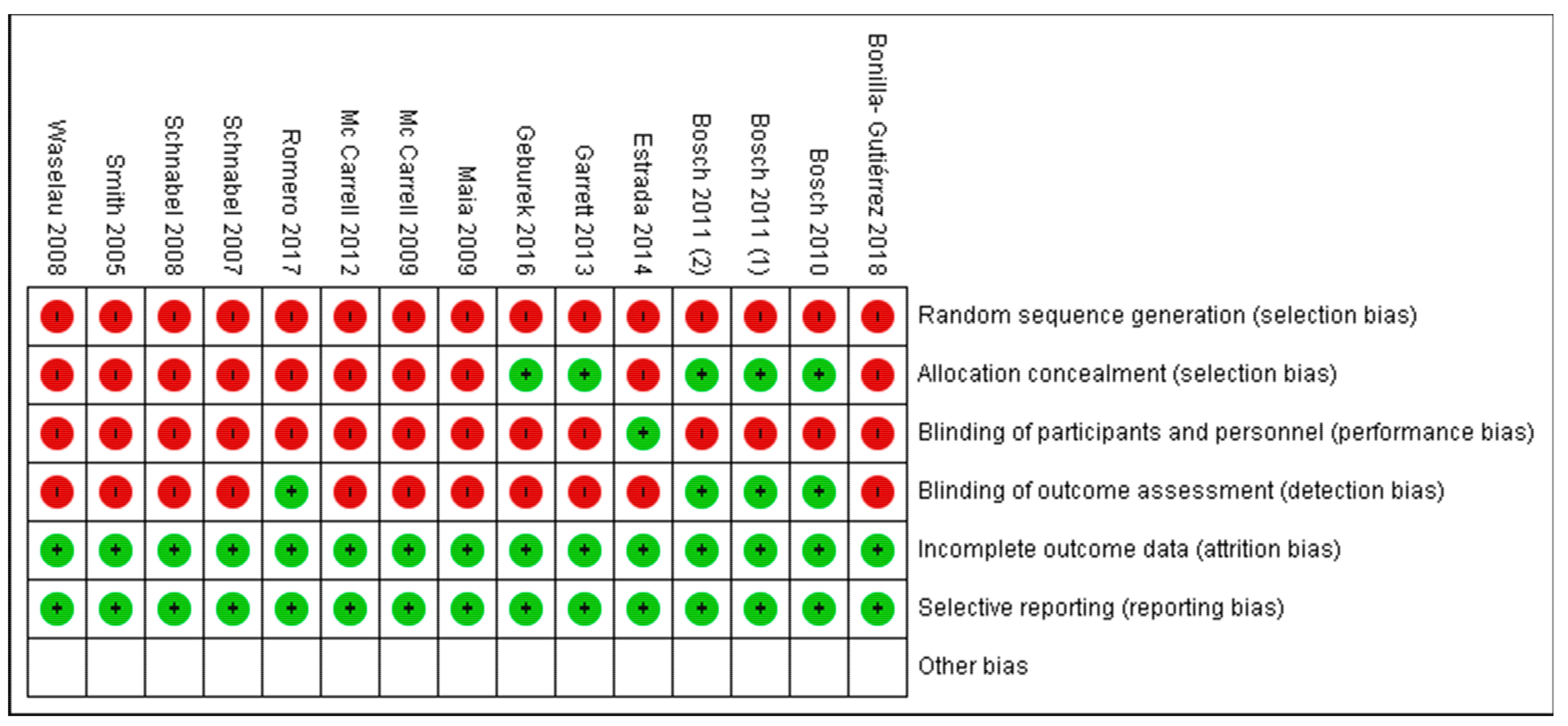
Risk of Bias of Selected Studies
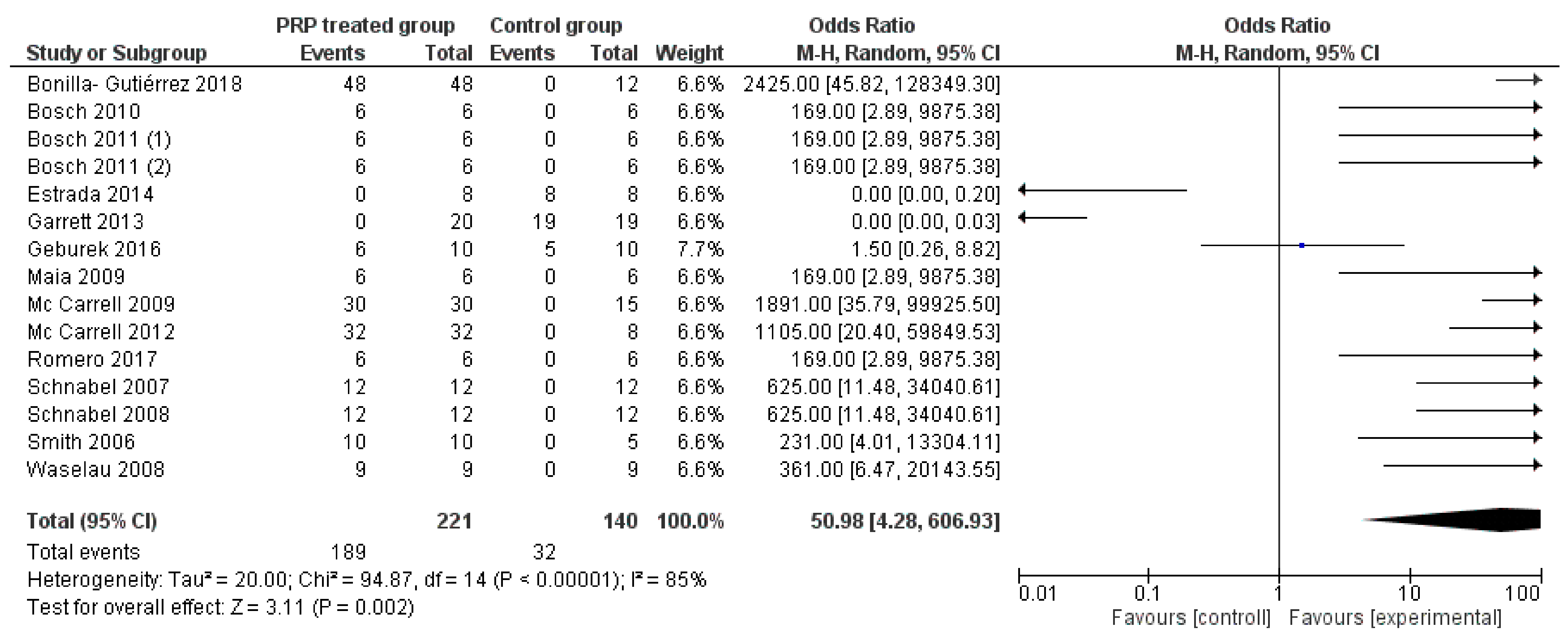
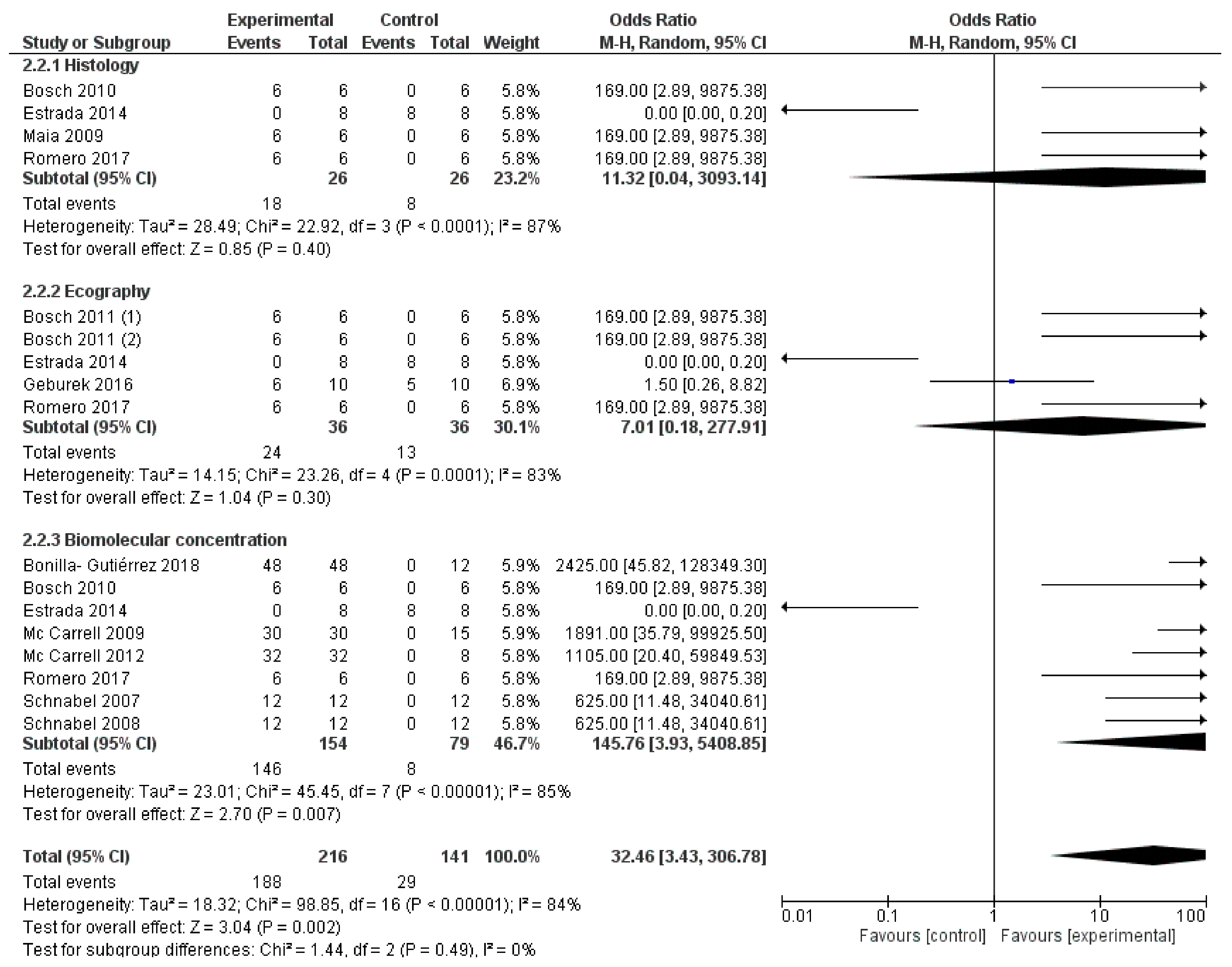
3.2. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clegg, P.D. Musculoskeletal disease and injury, now and in the future. Part 2: Tendon and ligament injuries. Equine Vet. J. 2012, 44, 371–375. [Google Scholar] [CrossRef] [Green Version]
- Trump, M.; Fürst, A.; Theiss, F. A Retrospective Study of the Prevalence of Injuries to the Suspensory Ligament, Digital Flexor Tendons and Associated Structures in a Non-Racehorse Referral-Hospital Population. Ph.D. Thesis, University of Zurich, Zurich, Switzerland, 2014. [Google Scholar]
- Bonilla-Gutiérrez, A.F.; López, C.; Carmona, J.U. Regenerative Therapies for the Treatment of Tenodesmic Injuries in Horses. J. Equine Vet. Sci. 2019, 73, 139–147. [Google Scholar] [CrossRef]
- Crevier-Denoix, N.; Collobert, C.; Pourcelot, P.; Denoix, J.M.; Sanaa, M.; Geiger, D.; Bernard, N.; Ribot, X.; Bortolussi, C.; Bousseau, B. Mechanical properties of pathological equine superficial digital flexor tendons. Equine Vet. J. Suppl. 1997, 23, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.E.; Genovese, R.; Longo, K.L.; Goodman, N.; Dyson, S. Practical management of superficial digital flexor tendinitis in the performance horse. Vet. Clin. N. Am. Equine Pract. 1994, 10, 425–481. [Google Scholar] [CrossRef]
- Dyson, S.J. Medical management of superficial digital flexor tendonitis: A comparative study in 219 horses (1992–2000). Equine Vet. J. 2004, 36, 415–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, K.H.; Parkin, T.D.H.; Riggs, C.M.; Morgan, K.L. Descriptive analysis of retirement of Thoroughbred racehorses due to tendon injuries at the Hong Kong Jockey Club (1992–2004). Equine Vet. J. 2007, 39, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Reef, V.B. Superficial digital flexor tendon healing: Ultrasonographic evaluation of therapies. Vet. Clin. N. Am. Equine Pract. 2001, 17, 159–178. [Google Scholar] [CrossRef]
- Guercio, A.; Di Marco, P.; Casella, S.; Russotto, L.; Puglisi, F.; Majolino, C.; Giudice, E.; Di Bella, S.; Purpari, G.; Cannella, V.; et al. Mesenchymal stem cells derived from subcutaneous fat and platelet-rich plasma used in athletic horses with lameness of the superficial digital flexor tendon. J. Equine Vet. Sci. 2015, 35, 19–26. [Google Scholar] [CrossRef]
- Woo, S.L.Y.; Hildebrand, K.; Watanabe, N.; Fenwick, J.A.; Papageorgiou, C.D.; Wang, J.H.C. Tissue engineering of ligament and tendon healing. Clin. Orthop. Relat. Res. 1999, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Fortier, L.A.; Smith, R.K.W. Regenerative Medicine for Tendinous and Ligamentous Injuries of Sport Horses. Vet. Clin. N. Am. Equine Pract. 2008, 24, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Nixon, A.J.; Dahlgren, L.A.; Haupt, J.L.; Yeager, A.E.; Ward, D.L. With Collagenase-Induced Tendinitis. Am. J. Vet. Res. 2008, 69, 928–937. [Google Scholar] [CrossRef] [Green Version]
- Barreira, A.P.B.; Alves, A.L.; Salto, M.E.; Arnorint, R.L.; Kohayagawa, A.; Menarim, B.C.; Mota, L.S. Autologous implant of bone marrow mononuclear cells as treatment of induced equine tendinitis. Int. J. Appl. Res. Vet. Med. 2008, 6, 46–54. [Google Scholar]
- Textor, J. Autologous Biologic Treatment for Equine Musculoskeletal Injuries: Platelet-Rich Plasma and IL-1 Receptor Antagonist Protein. Vet. Clin. N. Am. Equine Pract. 2011, 27, 275–298. [Google Scholar] [CrossRef] [PubMed]
- Brossi, P.M.; Moreira, J.J.; Machado, T.S.L.; Baccarin, R.Y.A. Platelet-rich plasma in orthopedic therapy: A comparative systematic review of clinical and experimental data in equine and human musculoskeletal lesions. BMC Vet. Res. 2015, 11, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortved, K.F. Regenerative Medicine and Rehabilitation for Tendinous and Ligamentous Injuries in Sport Horses. Vet. Clin. N. Am. Equine Pract. 2018, 34, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Im, G.-I.; Kim, T.-K. Stem Cells for the Regeneration of Tendon and Ligament: A Perspective. Int. J. Stem Cells 2020, 13, 335–341. [Google Scholar] [CrossRef]
- Anitua, E.; Andia, I.; Ardanza, B.; Nurden, P.; Nurden, A.T. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb. Haemost. 2004, 91, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Blair, P.; Flaumenhaft, R. Platelet α-granules: Basic biology and clinical correlates. Blood Rev. 2009, 23, 177–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsousou, J.; Thompson, M.; Hulley, P.; Noble, A.; Willett, K. The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery: A review of the literature. J. Bone Jt. Surg. Ser. B 2009, 91, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wu, Y.; Turxun, N.; Shen, Y.; Zhang, X. Efficacy and safety of platelet-rich plasma in the treatment of severe burns. Medicine 2020, 99, e23001. [Google Scholar] [CrossRef] [PubMed]
- De Vos, R.J.; Van Veldhoven, P.L.J.; Moen, M.H.; Weir, A.; Tol, J.L.; Maffulli, N. Autologous growth factor injections in chronic tendinopathy: A systematic review. Br. Med. Bull. 2010, 95, 63–77. [Google Scholar] [CrossRef] [Green Version]
- Geburek, F.; Stadler, P. Regenerative therapie von sehnen-Und banderkrankungen bei pferden: Ergebnisse der behandlung mit stammzellen, blutprodukten, gerüstsubstanzen und wachstumsfaktoren—Eine literaturübersicht und metaanalyse. Pferdeheilkunde 2011, 27, 609–625. [Google Scholar] [CrossRef] [Green Version]
- Sheth, U.; Simunovic, N.; Klein, G.; Fu, F.; Einhorn, T.A.; Schemitsch, E.; Ayeni, O.R.; Bhandari, M. Efficacy of autologous platelet-rich plasma use for orthopaedic indications: A meta-analysis. J. Bone Jt. Surg. Ser. A 2012, 94, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Andia, I.; Latorre, P.M.; Gomez, M.C.; Burgos-Alonso, N.; Abate, M.; Maffulli, N. Platelet-rich plasma in the conservative treatment of painful tendinopathy: A systematic review and meta-analysis of controlled studies. Br. Med. Bull. 2014, 110, 99–115. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Cruciani, M.; Mengoli, C.; Marano, G.; Pupella, S.; Veropalumbo, E.; Masiello, F.; Pati, I.; Vaglio, S.; Liumbruno, G.M. Efficacy of platelet-rich plasma as conservative treatment in orthopaedics: A systematic review and meta-analysis. Blood Transfus. 2018, 16, 502–513. [Google Scholar] [CrossRef]
- Nauwelaers, A.K.; Van Oost, L.; Peers, K. Evidence for the use of PRP in chronic midsubstance Achilles tendinopathy: A systematic review with meta-analysis. Foot Ankle Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Allet, J.Z.L. How Effective are Injections of Platelet-Rich Plasma (PRP) for the Treatment of Sports Injuries: A Critical Review of the Literature. J. Sports Med. Doping Stud. 2012, 2. [Google Scholar] [CrossRef] [Green Version]
- Moraes, V.Y.; Lenza, M.; Tamaoki, M.J.; Faloppa, F.; Belloti, J.C. Platelet rich therapies for musculoskeletal soft-tissue injuries. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Bosch, G.; Van Schie, H.T.M.; De Groot, M.W.; Cadby, J.A.; Van De Lest, C.H.A.; Barneveld, A.; Van Weeren, P.R. Effects of platelet-rich plasma on the quality of repair of mechanically induced core lesions in equine superficial digital flexor tendons: A placebo-controlled experimental study. J. Orthop. Res. 2010, 28, 211–217. [Google Scholar] [CrossRef] [PubMed]
- McCarrel, T.M.; Minas, T.; Fortier, L.A. Optimization of leukocyte concentration in platelet-rich plasma for the treatment of tendinopathy. J. Bone Jt. Surg. Ser. A 2012, 94, e143. [Google Scholar] [CrossRef] [PubMed]
- Ribitsch, I.; Baptista, P.M.; Lange-Consiglio, A.; Melotti, L.; Patruno, M.; Jenner, F.; Schnabl-Feichter, E.; Dutton, L.C.; Connolly, D.J.; van Steenbeek, F.G.; et al. Large Animal Models in Regenerative Medicine and Tissue Engineering: To Do or Not to Do. Front. Bioeng. Biotechnol. 2020, 8, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd: Chichester, UK, 2019; pp. 243–296. [Google Scholar]
- Garrett, K.S.; Bramlage, L.R.; Spike-Pierce, D.L.; Cohen, N.D. Injection of platelet- and leukocyte-rich plasma at the junction of the proximal sesamoid bone and the suspensory ligament branch for treatment of yearling thoroughbreds with proximal sesamoid bone inflammation and associated suspensory ligament branch de. J. Am. Vet. Med. Assoc. 2013, 243, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Geburek, F.; Gaus, M.; van Schie, H.T.M.; Rohn, K.; Stadler, P.M. Effect of intralesional platelet-rich plasma (PRP) treatment on clinical and ultrasonographic parameters in equine naturally occurring superficial digital flexor tendinopathies—A randomized prospective controlled clinical trial. BMC Vet. Res. 2016, 12, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boswell, S.G.; Schnabel, L.V.; Mohammed, H.O.; Sundman, E.A.; Minas, T.; Fortier, L.A. Increasing platelet concentrations in leukocyte-reduced platelet-rich plasma decrease collagen gene synthesis in tendons. Am. J. Sports Med. 2014, 42, 42–49. [Google Scholar] [CrossRef] [PubMed]
- McCarrel, T.; Fortier, L. Temporal growth factor release from platelet-rich plasma, trehalose lyophilized platelets, and bone marrow aspirate and their effect on tendon and ligament gene expression. J. Orthop. Res. 2009, 27, 1033–1042. [Google Scholar] [CrossRef]
- Schnabel, L.V.; Mohammed, H.O.; Miller, B.J.; McDermott, W.G.; Jacobson, M.S.; Santangelo, K.S.; Fortier, L.A. Platelet rich plasma (PRP) enhances anabolic gene expression patterns in flexor digitorum superficialis tendons. J. Orthop. Res. 2007, 25, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, L.V.; Mohammed, H.O.; Jacobson, M.S.; Fortier, L.A. Effects of platelet rich plasma and acellular bone marrow on gene expression patterns and DNA content of equine suspensory ligament explant cultures. Equine Vet. J. 2008, 40, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J.; Ross, M.W.; Smith, R.K.W. Anabolic effects of acellular bone marrow, platelet rich plasma, and serum on equine suspensory ligament fibroblasts in vitro. Vet. Comp. Orthop. Traumatol. 2006, 19, 43–47. [Google Scholar] [PubMed] [Green Version]
- Arguelles, D.; Carmona, J.U.; Climent, F.; Munoz, E.; Prades, M. Autologous platelet concentrates as a treatment for musculoskeletal lesions in five horses. Vet. Rec. 2008, 162, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, M.; Piccione, G.; Giannetto, C.; Tosto, F.; Di Pietro, S.; Giudice, E. Platelet Rich Plasma Intralesional Injection as Bedside Therapy for Tendinitis in Athletic Horse. Acta Sci. Vet. 2013, 41, 1–7. [Google Scholar]
- Bosch, G.; Moleman, M.; Barneveld, A.; van Weeren, P.R.; van Schie, H.T.M. The effect of platelet-rich plasma on the neovascularization of surgically created equine superficial digital flexor tendon lesions. Scand. J. Med. Sci. Sport. 2011, 21, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Bosch, G.; René van Weeren, P.; Barneveld, A.; van Schie, H.T.M. Computerised analysis of standardised ultrasonographic images to monitor the repair of surgically created core lesions in equine superficial digital flexor tendons following treatment with intratendinous platelet rich plasma or placebo. Vet. J. 2011, 187, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Castelijns, G.; Crawford, A.; Schaffer, J.; Ortolano, G.A.; Beauregard, T.; Smith, R.K.W. Evaluation of a filter-prepared platelet concentrate for the treatment of suspensory branch injuries in horses. Vet. Comp. Orthop. Traumatol. 2011, 24, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Estrada, R.J.; Van Weeren, R.; Van De Lest, C.H.A.; Boere, J.; Reyes, M.; Lonita, J.C.; Estrada, M.; Lischer, C.J. Effects of Autologous Conditioned Plasma® (ACP) on the healing of surgically induced core lesions in equine superficial digital flexor tendon. Pferdeheilkunde 2014, 30, 633–642. [Google Scholar] [CrossRef] [Green Version]
- Maia, L.; de Souza, M.V.; Ribeiro Júnior, J.I.; de Oliveira, A.C.; Alves, G.E.S.; dos Anjos Benjamin, L.; Silva, Y.F.R.S.; Zandim, B.M.; Moreira, J.d.C.L. Platelet-Rich Plasma in the Treatment of Induced Tendinopathy in Horses: Histologic Evaluation. J. Equine Vet. Sci. 2009, 29, 618–626. [Google Scholar] [CrossRef]
- Georg, R.; Maria, C.; Gisela, A.; Bianca, C. Autologous conditioned plasma as therapy of tendon and ligament lesions in seven horses. J. Vet. Sci. 2010, 11, 173–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romagnoli, N.; Rinnovati, R.; Ricciardi, G.; Lambertini, C.; Spinella, G.; Spadari, A. Clinical Evaluation of Intralesional Injection of Platelet-Rich Plasma for the Treatment of Proximal Suspensory Ligament Desmitis in Horses. J. Equine Vet. Sci. 2015, 35, 141–146. [Google Scholar] [CrossRef]
- Romero, A.; Barrachina, L.; Ranera, B.; Remacha, A.R.; Moreno, B.; de Blas, I.; Sanz, A.; Vázquez, F.J.; Vitoria, A.; Junquera, C.; et al. Comparison of autologous bone marrow and adipose tissue derived mesenchymal stem cells, and platelet rich plasma, for treating surgically induced lesions of the equine superficial digital flexor tendon. Vet. J. 2017, 224, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Scala, M.; Lenarduzzi, S.; Spagnolo, F.; Trapasso, M.; Ottonello, C.; Muraglia, A.; Barla, A.; Strada, P. Regenerative medicine for the treatment of teno-desmic injuries of the equine. A series of 150 horses treated with platelet-derived growth factors. In Vivo 2014, 28, 1119–1124. [Google Scholar] [PubMed]
- Spadari, A.; Ricciardi, G.; Rinnovati, R.; Romagnoli, N. Single Injection of Autologous Platelet Rich Plasma (PRP) in Suspensory Ligament Lesions in Horses: A Clinical Trial; European Society of Veterinary Orthopaedics and Traumatology: Cremona, Italy, 2011. [Google Scholar]
- Waselau, M.; Sutter, W.W.; Genovese, R.L.; Bertone, A.L. Intralesional injection of platelet-rich plasma followed by controlled exercise for treatment of midbody suspensory ligament desmitis in Standardbred racehorses. J. Am. Vet. Med. Assoc. 2008, 232, 1515–1520. [Google Scholar] [CrossRef] [Green Version]
- Zuffova, K.; Krisova, S.; Zert, Z. Platelet rich plasma treatment of superficial digital flexor tendon lesions in racing Thoroughbreds. Vet. Med. 2013, 58, 230–239. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Middleton, K.K.; Fu, F.H.; Im, H.J.; Wang, J.H.C. HGF Mediates the Anti-inflammatory Effects of PRP on Injured Tendons. PLoS ONE 2013, 8, e67303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacci, K.M.; Dardik, A. Platelet-rich plasma: Support for its use in wound healing. Yale J. Biol. Med. 2010, 83, 1–9. [Google Scholar] [PubMed]
- Thomopoulos, S.; Zaegel, M.; Das, R.; Harwood, F.L.; Silva, M.J.; Amiel, D.; Sakiyama-Elbert, S.; Gelberman, R.H. PDGF-BB released in tendon repair using a novel delivery system promotes cell proliferation and collagen remodeling. J. Orthop. Res. 2007, 25, 1358–1368. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Andía, I.; Sanchez, M.; Azofra, J.; del Mar Zalduendo, M.; de la Fuente, M.; Nurden, P.; Nurden, A.T. Autologous preparations rich in growth factors promote proliferation and induce VEGF and HGF production by human tendon cells in culture. J. Orthop. Res. 2005, 23, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Kajikawa, Y.; Morihara, T.; Sakamoto, H.; Matsuda, K.I.; Oshima, Y.; Yoshida, A.; Nagae, M.; Arai, Y.; Kawata, M.; Kubo, T. Platelet-rich plasma enhances the initial mobilization of circulation-derived cells for tendon healing. J. Cell. Physiol. 2008, 215, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Torricelli, P.; Fini, M.; Filardo, G.; Tschon, M.; Pischedda, M.; Pacorini, A.; Kon, E.; Giardino, R. Regenerative medicine for the treatment of musculoskeletal overuse injuries in competition horses. Int. Orthop. 2011, 35, 1569–1576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricco, S.; Renzi, S.; Del Bue, M.; Conti, V.; Merli, E.; Ramoni, R.; Lucarelli, E.; Gnudi, G.; Ferrari, M.; Grolli, S. Allogeneic Adipose Tissue-Derived Mesenchymal Stem Cells in Combination with Platelet Rich Plasma are Safe and Effective in the Therapy of Superficial Digital Flexor Tendonitis in the Horse. Int. J. Immunopathol. Pharmacol. 2013, 26, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Glasziou, P.P.; Sanders, S.L. Investigating causes of heterogeneity in systematic reviews. Stat. Med. 2002, 21, 1503–1511. [Google Scholar] [CrossRef] [PubMed]
- McLellan, J.; Plevin, S. Does it matter which platelet-rich plasma we use? Equine Vet. Educ. 2011, 23, 101–104. [Google Scholar] [CrossRef]
- Vadim, P.; Michelle, B.; Cen, Z.; Reichert, H.J. Chapter 4: In Vitro Models for Neuroelectrodes: A Paradigm for Studying Tissue—Materials Interactions in the Brain. In Indwelling Neural Implants: Strategies for Contending with the In Vivo Environment; Reichert, W.M., Ed.; CRC Press: Boca Raton, FL, USA, 2008; ISBN 978-0-8493-9362-4. [Google Scholar]
- Wu, F.; Nerlich, M.; Docheva, D. Tendon injuries: Basic science and new repair proposals. EFORT Open Rev. 2017, 2, 332–342. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.E.; Jensen, J.L.; Rodgers, R. The Control Group and Meta-Analysis. J. Methods Meas. Soc. Sci. 2014, 6, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Giraldo, C.E.; López, C.; Álvarez, M.E.; Samudio, I.J.; Prades, M.; Carmona, J.U. Effects of the breed, sex and age on cellular content and growth factor release from equine pure-platelet rich plasma and pure-platelet rich gel. BMC Vet. Res. 2013, 9. [Google Scholar] [CrossRef] [Green Version]
- Tamimi, F.M.; Montalvo, S.; Tresguerres, I.; Blanco Jerez, L. A Comparative Study of 2 Methods for Obtaining Platelet-Rich Plasma. J. Oral Maxillofac. Surg. 2007, 65, 1084–1093. [Google Scholar] [CrossRef]
- Elbackly, R.M.; Mastrogiacomo, M.; Cancedda, R. Bone Regeneration and Bioengineering. In Regenerative Medicine Applications in Organ Transplantation; Elsevier: Amsterdam, The Netherlands, 2014; pp. 783–797. [Google Scholar]
- Schulz, K.F.; Grimes, D.A. Blinding in randomised trials: Hiding who got what. Lancet 2002, 359, 696–700. [Google Scholar] [CrossRef]
- Engebretsen, L.; Steffen, K.; Alsousou, J.; Anitua, E.; Bachl, N.; Devilee, R.; Everts, P.; Hamilton, B.; Huard, J.; Jenoure, P.; et al. IOC consensus paper on the use of platelet-rich plasma in sports medicine. Br. J. Sports Med. 2010, 44, 1072–1081. [Google Scholar] [CrossRef]
- Gillis, C.L. Rehabilitation of Tendon and Ligament Injuries. Am. Assoc. Equine Pract. 1997, 43, 306–309. [Google Scholar]
- Avella, C.S.; Smith, R.K.W. Diagnosis and Management of Tendon and Ligament Disorders. In Equine Surgery; Elsevier: Amsterdam, The Netherlands, 2012; pp. 1157–1179. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Study | Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| 1 | Argüelles, 2008 | − | − | − | − | + | + | ↑ |
| 2 | Bazzano, 2013 | − | − | − | − | + | + | ↑ |
| 3 | Bonilla–Gutiérrez, 2018 | − | − | − | − | + | + | ↑ |
| 4 | Bosch,2010 | − | + | − | + | + | + | ↓ |
| 5 | Bosch, 2011 (1) | − | + | − | + | + | + | ↓ |
| 6 | Bosch, 2011 (2) | − | + | − | + | + | + | ↓ |
| 7 | Boswell, 2014 | − | − | − | − | + | + | ↓ |
| 8 | Castelijns, 2011 | − | − | − | − | + | + | ↑ |
| 9 | Estrada, 2014 | − | − | + | − | + | + | ↓ |
| 10 | Garrett, 2013 | − | + | − | − | + | + | ↓ |
| 11 | Geburek, 2016 | − | + | − | − | + | + | ↓ |
| 12 | Maia, 2009 | − | − | − | − | + | + | ↑ |
| 13 | McCarrell, 2009 | − | − | − | − | + | + | ↑ |
| 14 | McCarrell, 2012 | − | − | − | − | + | + | ↑ |
| 15 | Rindermann, 2010 | − | − | − | − | + | + | ↑ |
| 16 | Romagnoli, 2015 | − | − | − | − | + | + | ↑ |
| 17 | Romero, 2017 | − | − | − | + | + | + | ↓ |
| 18 | Scala, 2014 | − | − | − | − | − | + | ↑ |
| 19 | Spadari, 2010 | − | − | − | − | + | + | ↑ |
| 20 | Schnabel, 2007 | − | − | − | − | + | + | ↑ |
| 21 | Schnabel, 2008 | − | − | − | − | + | + | ↑ |
| 22 | Smith, 2006 | − | − | − | − | + | + | ↑ |
| 23 | Waselau, 2008 | − | − | − | − | + | + | ↑ |
| 24 | Zuffova, 2013 | − | − | − | − | + | + | ↑ |
| Study | Commercial System | Centrifugation | Filtration | Platelet Concentration |
|---|---|---|---|---|
| Arguelles, 2008 | √ | 250 × 106 platelets/mL | ||
| Bazzano, 2013 | √ | 540.000 ± 98.000 platelets/µL | ||
| Bonilla-Gutierrez, 2018 | √ | N.D | ||
| Bosch, 2010 | √ | 639.7 ± 103.2 × 109 platelets/L | ||
| Bosch, 2011 (1) | √ | N.D | ||
| Bosch, 2011 (2) | √ | 3.8 × hematic concentration | ||
| Boswell, 2014 | √ | 236.750 ± 35.714 platelets/µL | ||
| Castelijns, 2011 | √ | 850 ± 244 × 109 platelets/L | ||
| Estrada, 2014 | √ | 162.0 ± 43.6 × 103 platelets/µL | ||
| Garret, 2013 | √ | 966.000 ± 189.000 platelets/µL | ||
| Geburek, 2016 | √ | 892.37 ± 364.7 × 103 platelets/µL | ||
| Maia, 2009 | √ | 407.500 ± 58.800 platelets/µL | ||
| McCarrell, 2009 | √ | 1 × 109 platelets/mL | ||
| McCarrell, 2012 | √ | N.D | ||
| Rindermann, 2010 | √ | 160–197 × 109 platelets/L | ||
| Romagnoli, 2015 | √ | 1045 × 103 platelets/µL | ||
| Romero, 2017 | √ | 263.3 × 103 ± 99.9 × 103 platelets/µL | ||
| Scala, 2014 | √ | 1 × 106 platelets/µL | ||
| Schnabel, 2007 | √ | 395 × 103 platelets/µL | ||
| Schnabel, 2008 | √ | N.D | ||
| Smith, 2006 | √ * | 520.000 platelets/µL | ||
| Spadari, 2010 | √ | 7–11 × hematic concentration | ||
| Waselau, 2008 | √ | 1.37·106 ± 1.11 × 104 platelets/µL | ||
| Zuffova, 2013 | √ * | 466.5 × 109 platelets /L |
| Study | Type of Study | Sample | Interventions | Outcomes |
|---|---|---|---|---|
| Argüelles, 2008 | No-RCTs | Two horses with tendinopathy of SDFT and three horses with desmitis of SL. | Injection of 5–8 mL of PRP into the lesion. | Improvements in the ultrasonographic aspect of the lesions, especially in SDFT tendonitis, decreased degree of lameness and response to flexion test. All horses returned to their preinjury level of performance. |
| Bazzano, 2013 | No-RCTs | Fifteen horses affected by tendinitis of SDFT or DDFT. | Injection of 0.5–5 mL of PRP into the lesion. | The ultrasonographic aspect of tendons, 50 days after the PRP treatment, was comparable to healthy tendons; all horses showed clinical improvement. All the patients returned to train and compete; no reinjury occurred within 12 months from the beginning of the treatment. |
| Bonilla–Gutiérrez, 2018 | RCTs | SL and SDFT samples from six horses. | Four SL and 50% of concentration. One SL and 1 SDFT did not receive any treatment and were used as a control group. | The concentration of IL-1β, TNF-α, IL-4, IL-1 receptor antagonist, PDGF- ββ, TGF-β1, and HA released from incubated tendons and ligaments was higher in the PRP group than in the control group. |
| Bosch, 2010 | No-RCTs | Six horses with induced lesions of the SDFT in both forelimbs. | Injection of 3 mL of PRP in the lesion and 3 mL of saline solution in the other limb (placebo group). | The concentration of collagen, GAGs, and number of cells was higher in the PRP-treated tendons. The repair tissue in the PRP group showed a higher elastic modulus and breaking strength. Histologically, the PRP-treated tendons had a better organization of the collagen network and signs of increased metabolic activity. |
| Bosch, 2011 (1) | No-RCTs | Six horses with induced lesions of the SDFT in both forelimbs. | Injection of 3 mL of PRP in the lesion and 3 mL of saline solution in the other limb (placebo group). | Blood flow, evaluated with CFD, was significantly higher in the PRP-treated group. The total number of blood vessels 24 weeks after lesion induction, determined with the Factor VIII staining, was significantly higher in the PRP-treated tendons. |
| Bosch, 2011 (2) | No-RCTs | Six horses with induced lesions of the SDFT in both forelimbs. | Injection of 3 mL of PRP in the lesion and 3 mL of saline solution in the other limb (placebo group). | The ultrasonographic tissue characterization showed an E-value significantly higher in PRP-treated tendons than the controls at weeks 2, 3, 5 and 8; the C-value in the PRP group became significantly higher from week 12. The B-value was very similar throughout the experiment for both groups. These results suggest that the PRP treatment accelerates the collagenous matrix organization into tendon bundles and their arrangement along the stress lines. |
| Boswell, 2014 | CLS | Eight horses. | Explants of SDFT cultured in LR-PRP or placebo for 3 days. | In the LR-PRP group, the concentration of PDGF-ββ, TGF- β1, COL1A1, and COMP was increased. The concentration of IL-1 β, MMP-3, and MMP-13, instead was decreased. |
| Castelijns, 2011 | No-RCTs | Eleven horses with desmitis of SL. | 2.5 mL of platelet concentrate was injected into the lesion. | The lameness score showed a reduction in all of the treated patients. The ultrasonographic exam performed three months after the treatment showed a complete resolution of the lesion for 10 horses. Five horses returned to their previous level of work. |
| Estrada, 2014 | No-RCTs | Eight horses with induced lesions of the SDFT of both fore- and hindlimbs. | Injection of 2.5 mL of PRP or saline solution into the lesion (placebo group). The treatment assignment was randomized, and the operator was not aware of what he was injecting. | The PRP-treated tendons presented a significantly lower concentration of GAGs when compared to the control group. Other compositional, biomechanical, ultrasonographic, and histological parameters showed no significant differences. |
| Garrett, 2013 | RCTs | Thirty-nine horses with proximal sesamoid bone inflammation and SL-branch desmitis. | Injection of 3 mL of PRP or saline (placebo group) in the affected SL- branch or proximal sesamoid bone junction. | Considering the number of races started and earnings in the following 2, 3, and 4 years, most of the horses treated with PRP started at least one race during the 2nd racing year. No significant differences were found between groups regarding starts during the 3rd and 4th year of competition and earnings. |
| Geburek, 2016 | RCTs | Twenty horses with tendinitis of the SDFT of one or both forelimbs. | Injection of 3 mL of PRP or saline solution (placebo group) in the lesion. | Lameness decreased significantly at 8 weeks in the PRP-treated group, at 12 weeks in the placebo group. Ultrasonographically, there were no differences in the cross-sectional area between the two groups; 80% of the PRP-treated horses reached their previous or a higher performance level after 12 months compared to 50% in the control group. After 24 months, these proportions were 60% and 50%, respectively. |
| Maia, 2009 | No-RCTs | Six horses with induced lesions of the SDFT in both forelimbs. | 2.5 mL of activated PRP was injected in the right forelimb, 2.5 mL of saline solution was administered in the left forelimb (placebo group). | Thirty-six days after induced lesions, the histologic exam showed that injuries under PRP treatment presented a more uniform and organized tissue repair than the placebo group. |
| McCarrell, 2009 | CLS | Five horses. | Tendons and ligaments cells from treated horses were cultured with PRP and placebo. | The PRP group has a higher concentration of TGF-b1, PDGF-BB, COL1A1, COL3A1, COMP, and a lower expression of MMP-13. |
| McCarrell, 2012 | CLS | Eight horses. | Tendons were chopped into explants and placed into culture plates; then, they were cultured with standard PRP, high-concentration PRP, leukocyte-reduced PRP, concentrated-leukocyte PRP, or placebo. | The expression of COMP and COL1A1/COL3A1 ratio was increased in the PRP groups, while the expression of MMP-13 was decreased. |
| Rindermann, 2010 | Case report | Seven horses with tendinitis of SDFT, DDFT or with desmitis of inferior check ligament. | Injection of 2–4 mL of ACP into the lesion. | All horses treated with platelet concentrate returned to their previous level of work; the ultrasonographic aspect of tendons/ligaments improved. |
| Romagnoli, 2015 | No- RCTs | Twenty horses with desmitis of SL. | Injection of 0.8–4 mL of PRP into the lesion. | Twenty-four months after the treatment, sixteen horses returned to their previous activity, while four animals recidivated in different regions of SL. |
| Romero, 2017 | No-RCTs | Twenty horses with induced lesions in SDFT in both forelimbs. | Horses received 7 mL of PRP or 7 mL Ringer’s lactate solution (placebo group) in assigned tendons 1 week after the injury induction. | In the PRP-group, ten weeks after the treatment, there was a significant reduction in FPS, CSA, and TES. Furthermore, PRP-treatment was associated with a better histopathological outcome. |
| Scala, 2014 | No- RCTs | Ninety-nine horses with tenodesmic lesions. | Injection of PRP into the lesion (the amount of injected product varies depending on the size of the lesion). | Complete clinical and ultrasonographic healing was obtained in 81% of treated horses; 12% had an improvement and 7% a failure. |
| Schnabel, 2007 | CLS | Six horses with induced lesions in SDFT in both forelimbs. | Cultures were established by 5 tendon explants (two replicates/group); culture media were whole blood, plasma, PRP, PPP, and bone marrow aspirate at different concentrations. | Tendons cultured in PRP showed enhanced COL1A1, COL3A1, and COMP concentrations, with no increase in the catabolic molecules like MMP-3 and MMP-13. |
| Schnabel, 2008 | CLS | Six horses. | Tendons were chopped into explants; cultures were established with five explants/well of six-well plates with two replicates/treatment group (defined by culture medium)/horse. Culture media were whole blood, plasma, PRP, PPP, bone marrow aspirate at different concentrations. | Tendons cultured in PRP showed an enhanced concentration of COL1A1, COL3A1, COMP, decorin, with no concomitant increase in the catabolic molecules such as MMP-3 and MMP-13. |
| Smith, 2006 | CLS | Five horses. | Cells from SL sections were recollected and cultured with acellular bone marrow, PRP, equine serum, fetal bovine serum, and medium (placebo group). | There was an increase in mean COMP production and mean H-Leucine incorporation in ligaments treated with PRP. |
| Spadari, 2010 | No- RCTs | Ten horses with desmitis of SL. | Injection of PRP into the lesion. | Nine horses showed an improvement in the ultrasonographic aspect of the SL and returned to the activity. |
| Waselau, 2008 | No-RCTs | Nine horses. | Injection of 3 mL of PRP into the lesion. | The number of starts and earnings during the first and third year was lower than earnings and starts during the year before the injury. During the second year, the number of starts and earnings was higher. |
| Zuffova, 2013 | No-RCTs | Twenty-two horses with tendinitis of SDFT. | Injection of PRP into the lesion (the amount of injected product varies depending on the size of the lesion). | Horses with acute lesions ran 56% of races in the follow-up period, while animals with chronic injuries ran 30% of competitions. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montano, C.; Auletta, L.; Greco, A.; Costanza, D.; Coluccia, P.; Del Prete, C.; Meomartino, L.; Pasolini, M.P. The Use of Platelet-Rich Plasma for Treatment of Tenodesmic Lesions in Horses: A Systematic Review and Meta-Analysis of Clinical and Experimental Data. Animals 2021, 11, 793. https://doi.org/10.3390/ani11030793
Montano C, Auletta L, Greco A, Costanza D, Coluccia P, Del Prete C, Meomartino L, Pasolini MP. The Use of Platelet-Rich Plasma for Treatment of Tenodesmic Lesions in Horses: A Systematic Review and Meta-Analysis of Clinical and Experimental Data. Animals. 2021; 11(3):793. https://doi.org/10.3390/ani11030793
Chicago/Turabian StyleMontano, Chiara, Luigi Auletta, Adelaide Greco, Dario Costanza, Pierpaolo Coluccia, Chiara Del Prete, Leonardo Meomartino, and Maria Pia Pasolini. 2021. "The Use of Platelet-Rich Plasma for Treatment of Tenodesmic Lesions in Horses: A Systematic Review and Meta-Analysis of Clinical and Experimental Data" Animals 11, no. 3: 793. https://doi.org/10.3390/ani11030793
APA StyleMontano, C., Auletta, L., Greco, A., Costanza, D., Coluccia, P., Del Prete, C., Meomartino, L., & Pasolini, M. P. (2021). The Use of Platelet-Rich Plasma for Treatment of Tenodesmic Lesions in Horses: A Systematic Review and Meta-Analysis of Clinical and Experimental Data. Animals, 11(3), 793. https://doi.org/10.3390/ani11030793