
Effects of Pre-Anesthesia Anxiety on Propofol Induction Dose in Cats


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
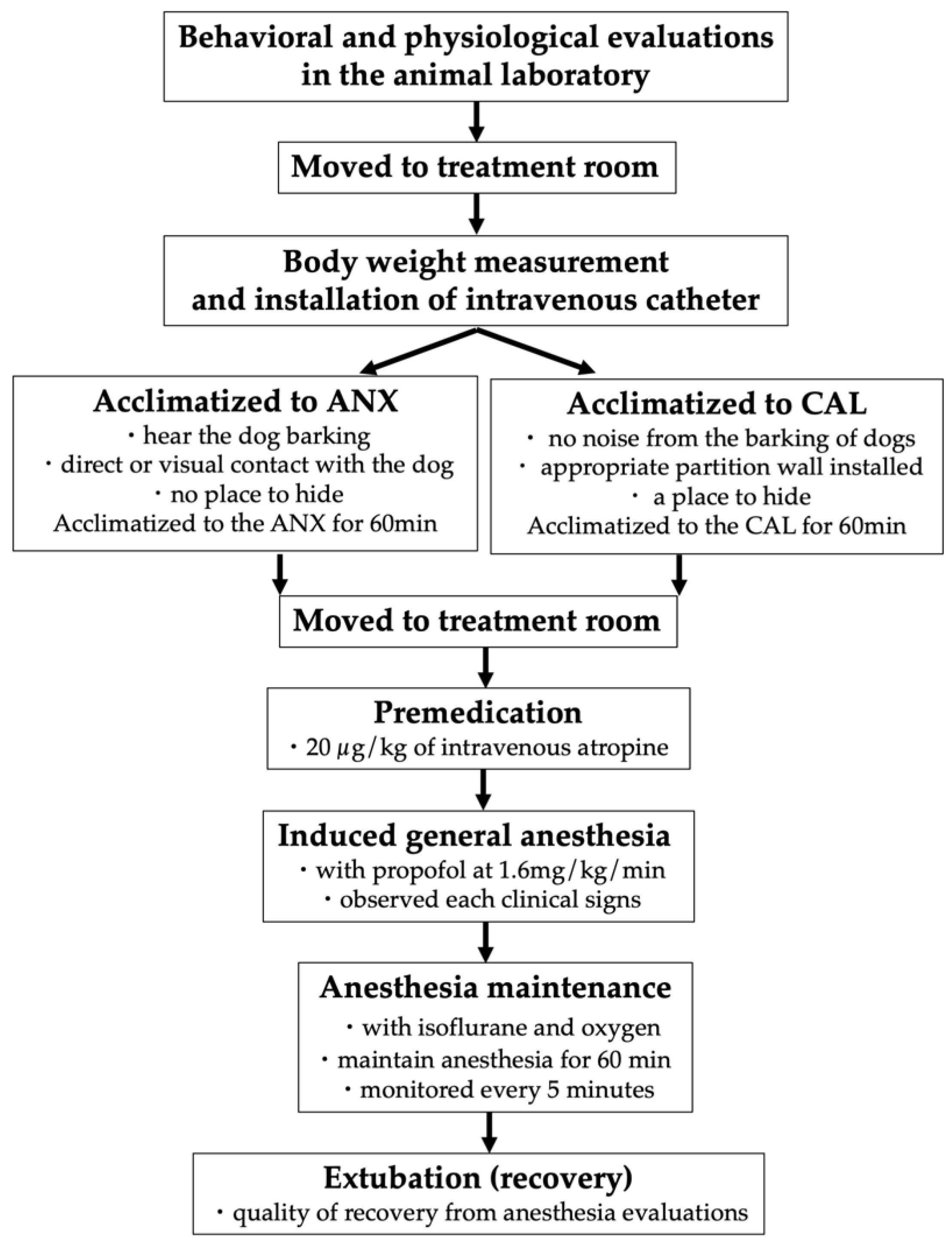
2.2. Procedures
2.3. Anesthetic Management
2.4. Physiological Evaluation
2.5. Environmental Treatments
2.6. Behavioral Evaluation
2.7. Clinical Signs Observation
2.8. The Quality of Recovery
2.9. Statistical Analyses
3. Results
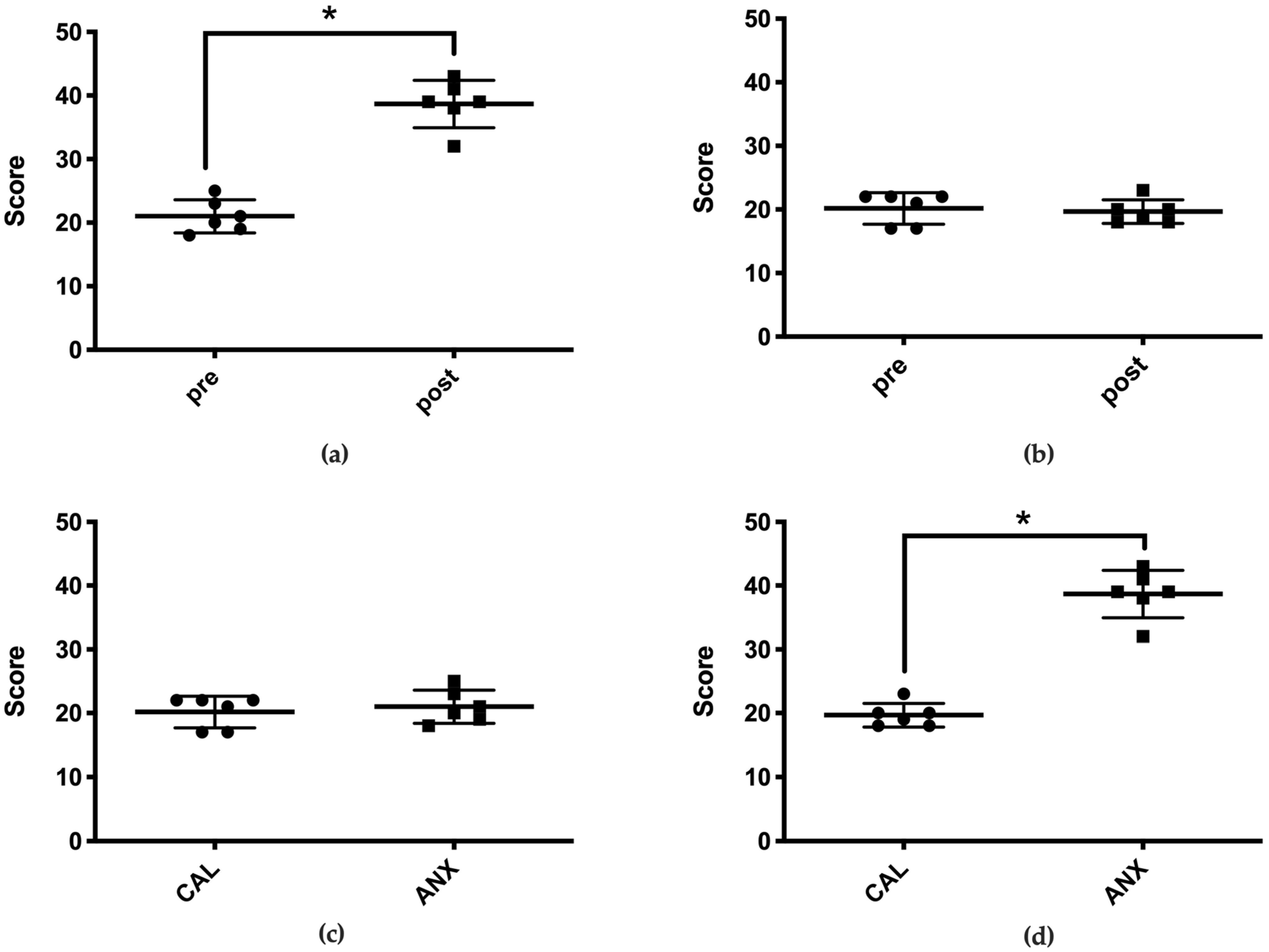
3.1. Environmental Acclimatization
3.1.1. Behavioral Evaluation
3.1.2. Physiological Evaluation
3.2. Anesthesia Induction
3.2.1. Propofol Dose Required to Observe Each Clinical Sign
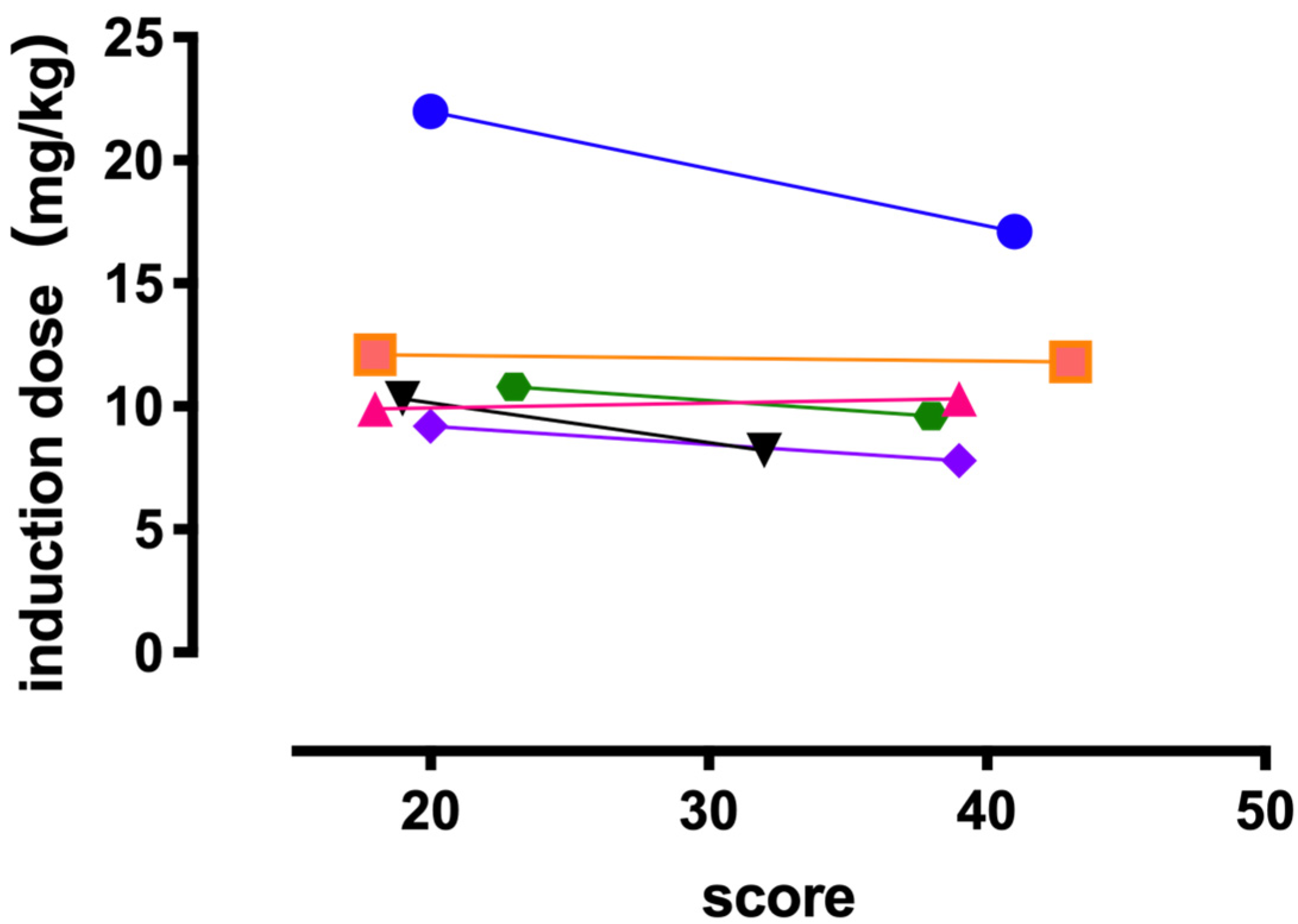
3.2.2. Behavioral Evaluation Score and Propofol Requirements
3.3. Anesthesia Maintenance
3.3.1. Heart Rate
3.3.2. Blood Pressure
3.3.3. Respiratory Rate
3.4. The Time during Which the MAP Was <65 mmHg and the Propofol Dose Required
3.5. Recovery
3.5.1. Time to Head Up (HUT: Head Up Time)
3.5.2. The Quality of Recovery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Observation | Description | Score |
|---|---|---|
| Body | Laid out on side or on back: (I) | 1 |
| NA: (A) | 1 | |
| Laid ventral or half on side: (I) | 2 | |
| Standing or moving, back horizontal: (A) | 2 | |
| Laid ventral or sitting: (I) | 3 | |
| Standing or moving: (A) | 3 | |
| Laid ventral, rolled, or sitting: (I) | 4 | |
| Standing or moving, body behind lower than in front: (A) | 4 | |
| laid ventrally or crouched directly on top of all paws, may be shaking: (I) | 5 | |
| whole body near to ground, crawling, may be shaking: (A) | 5 | |
| Belly | Exposed, slow ventilation | 1 |
| Exposed or not exposed, slow or normal ventilation | 2 | |
| Not exposed, normal ventilation | 3 | |
| Not exposed, normal or fast ventilation | 4 | |
| Legs | Fully extended: (I) | 1 |
| NA: (A) | 1 | |
| Bent, hind legs may be laid out: (I) | 2 | |
| when standing extended: (A) | 2 | |
| Bent: (I) | 3 | |
| While standing extended: (A) | 3 | |
| Bent: (I) | 4 | |
| When standing hind legs bent, in front extended: (A) | 4 | |
| Bent: (I) | 5 | |
| Bent near the surface: (A) | 5 | |
| Head | Laid on the surface with chin upwards or on the surface | 1 |
| Laid on the surface or over the body, some movement | 2 | |
| Over the body or pressed to the body, little or no movement | 3 | |
| On the plane of the body, less or no movement | 4 | |
| Lower than the body, motionless | 5 | |
| Pupils | Normal (consider ambient light) | 1 |
| Normal or partially dilated | 2 | |
| Dilated | 3 | |
| Fully dilated | 4 | |
| Ears | Normal (half back) | 1 |
| Normal (half back) or erect and moved to the front | 2 | |
| Normal (half back) or erect and moved to the front or back and forward on the head | 3 | |
| Partially flattened | 4 | |
| Fully flattened back on the head | 5 | |
| Whiskers | Normal (lateral) | 1 |
| Normal (lateral or forward) | 2 | |
| Lateral (normal) or forward and back | 3 | |
| Back | 4 | |
| Tail | Extended or loosely wrapped: (I) | 1 |
| NA: (A) | 1 | |
| Extended or loosely wrapped: (I) | 2 | |
| Tail up or loosely downwards: (A) | 2 | |
| On the body or curved backwards, may be twitching: (I) | 3 | |
| Up or tense downwards, may be twitching: (A) | 3 | |
| Close to the body: (I) | 4 | |
| Tense downwards or curled forward, may be twitching: (A) | 4 | |
| Close to the body: (I) | 5 | |
| Curled forward close to the body: (A) | 5 | |
| Eyes | Closed or half open, may be slowly blinking | 1 |
| Closed, half open or completely, normally open | 2 | |
| Normally open | 3 | |
| Widely open | 4 | |
| Completely open | 5 | |
| Vocalization | None or soft purr | 1 |
| None or Meow | 2 | |
| Meow, plaintive meow, or quiet | 3 | |
| Plaintive meow, yowling, growling, or quiet | 4 | |
| Plaintive meow, yowling, growling, hissing, or quiet | 5 | |
| Activity | Sleeping or resting | 1 |
| Sleeping, resting, alert or active, or may be playing | 2 | |
| Resting, awake, or actively exploring | 3 | |
| Alert, may be actively trying to escape, motionless alert, or actively prowling | 4 | |
| Immovable | 5 |
References
- Feldhahn, J.R.; Rand, J.S.; Kinnaird, E. The effect of interday variation and a short-term stressor on insulin sensitivity in clinically normal cats. J. Feline Med. Surg. 1999, 1, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Quimby, J.M.; Smith, M.L.; Lunn, K.F. Evaluation of the effects of hospital visit stress on physiologic parameters in the cat. J. Feline Med. Surg. 2011, 13, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Okaniwa, J. Study on interior design of health care environment in pediatric wards. J. Archit. Plan. (Trans. AIJ) 2008, 73, 511–518. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.P.; Sun, Y.; Wu, C.; Xu, W.H.; Zhang, R.D.; Zheng, J.J.; Huang, Y.; Chen, Y.Q.; Zhang, M.Z.; Wu, J.Z. The effectiveness of transport in a toy car for reducing preoperative anxiety in preschool children: A randomised controlled prospective trial. Br. J. Anaesth. 2018, 121, 438–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maranets, I.; Kain, Z.N. Preoperative anxiety and intraoperative anesthetic requirements. Anesth. Analg. 1999, 89, 1346–1351. [Google Scholar] [PubMed]
- Kil, H.K.; Kim, W.O.; Chung, W.Y.; Kim, G.H.; Seo, H.; Hong, J.-Y. Preoperative anxiety and pain sensitivity are independent predictors of propofol and sevoflurane requirements in general anaesthesia. Br. J. Anaesth. 2012, 108, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Morley, A.P.; Papageorgiou, C.H.; Marinaki, A.M.; Cooper, D.J.; Lewis, C.M. The effect of pre-operative anxiety on induction of anaesthesia with propofol. Anaesthesia 2008, 63, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Larenza, M.P.; Althaus, H.; Conrot, A.; Balmer, C.; Schatzmann, U.; Bettschart-Wolfensberger, R. Anaesthesia recovery quality after racemic ketamine or S-ketamine administration to male cats undergoing neutering surgery. Schweiz. Arch. Tierheilkd. 2008, 150, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Rodan, I.; Sundahl, E.; Carney, H.; Gagnon, A.-C.; Heath, S.; Landsberg, G.; Seksel, K.; Yin, S. AAFP and ISFM feline-friendly handling guidelines. J. Feline Med. Surg. 2011, 13, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Rodan, I.; Sundahl, E.; Carney, H.; Gagnon, A.-C.; Heath, S.; Landsberg, G.; Seksel, K.; Yin, S. Feline focus: AAFP and ISFM feline-friendly handling guidelines. Compend. Contin. Educ. Vet. 2011, 33, E3. [Google Scholar] [PubMed]
- Kessler, M.R.; Turner, D.C. Stress and adaptation of cats (Felis silvestris catus) housed singly, in pairs and in groups in boarding catteries. Anim. Welf. 1997, 6, 243–254. [Google Scholar]
- Ogata, N.; Kanda, T.; Kawahata, M.; Ichikawa, T.; Matsumoto, Y.; Morimitsu, W.; Nishino, Y.; Itoi, T.; Furumoto, K. Sedative and physiological effects of brimonidine tartrate ophthalmic solution in healthy cats. Vet. Anaesth. Analg. 2017, 44, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.J.; Smith, L.J. A comparison of cardiopulmonary function, recovery quality, and total dosages required for induction and total intravenous anesthesia with propofol versus a propofol-ketamine combination in healthy Beagle dogs. Vet. Anaesth. Analg. 2015, 42, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Mathis, A.; Pinelas, R.; Brodbelt, D.C.; Alibhai, H.I.K. Comparison of quality of recovery from anaesthesia in cats induced with propofol or alfaxalone. Vet. Anaesth. Analg. 2012, 39, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Onaka, T. Stress and its neural mechanisms. Folia Pharmacol. Jpn. 2005, 126, 170–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakabe, H. Short reviw of stress. Bull. Inst. Public Health 1993, 42, 366–374. [Google Scholar]
- Ziegler, M.G. Chapter 61—Psychological Stress and the Autonomic Nervous System. In Primer on the Autonomic Nervous System; Robertson, D., Biaggioni, I., Burnstock, G., Low, P.A., Paton, J.F.R.B.T., Eds.; Academic Press: San Diego, Chile, 2012; pp. 291–293. [Google Scholar]
- Klein, B.G.; Cunningham, J.G. The Autonomic Nervous System and Adrenal Medulla. In Textbook of Veterinary Physiology; Klein, B.G., Cunningham, J.G., Eds.; Saunders Elsevier: St. Louis, MO, USA, 2007; pp. 136–144. [Google Scholar]
- Davis, W.B.; Thaut, M.H. The influence of preferred relaxing music on measures of state anxiety, relaxation, and physiological responses 1. J. Music Ther. 1989, 26, 168–187. [Google Scholar] [CrossRef]
- Karteroliotis, C.; Gill, D.L. Temporal changes in psychological and physiological components of state anxiety. J. Sport Psychol. 1987, 9, 261–274. [Google Scholar] [CrossRef] [Green Version]
- Sano, T.; Nishimura, R.; Mochizuki, M.; Hara, Y.; Tagawa, M.; Sasaki, N. Clinical usefulness of propofol as an anesthetic induction agent in dogs and cats. J. Vet. Med. Sci. 2003, 65, 641–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Clinical Sign | Propofol Dose Required in the ANX Group (Median [Range]) | Propofol Dose Required in the CAL Group (Median [Range]) |
|---|---|---|
| Loss of body movement | 3.1 mg/kg (2.2–4.0 mg/kg) | 4.0 mg/kg (2.4–6.9 mg/kg) |
| Appearance of nictitating membrane | 3.2 mg/kg (2.3–6.1 mg/kg) | 3.1 mg/kg (1.6–4.4 mg/kg) |
| Loss of eyelid reflex | 5.4 mg/kg (2.2–9.6 mg/kg) | 5.4 mg/kg (2.4–9.9 mg/kg) |
| Disappearance of flexion reflex | 6.9 mg/kg (5.0–9.1 mg/kg) | 7.5 mg/kg (4.3–8.5 mg/kg) |
| Disappearance of tongue retracting reflex | 5.6 mg/kg (3.9–6.6 mg/kg) | 6.4 mg/kg (4.4–7.4 mg/kg) |
| Loss of mandibular tension | 5.4 mg/kg (3.9–6.6 mg/kg) | 6.3 mg/kg (3.8–7.4 mg/kg) |
| Disappearance of corneal reflex | 9.9 mg/kg (6.2–12.2 mg/kg) | 7.0 mg/kg (4.4–11.6 mg/kg) |
| Disappearance of laryngeal reflex | 9.9 mg/kg (7.8–17.1 mg/kg) | 10.5 mg/kg (9.2–22.0 mg/kg) |
| HR and MAP | Each Measurement Time during Maintenance of Anesthesia | ||||||
|---|---|---|---|---|---|---|---|
| T0 | T5 | T10 | T15 | T20 | T25 | T30 | |
| HR (beats/min) | |||||||
| ANX | 174 ± 16 | 166 ± 7 | 158 ± 6 | 152 ± 5 | 150 ± 5 | 152 ± 5 | 152 ± 5 |
| CAL | 153 ± 7 | 153 ± 11 | 142 ± 11 | 142 ± 8 | 144 ± 7 | 146 ± 6 | 145 ± 6 |
| MAP (mmHg) | |||||||
| ANX | 134 ± 9 | 66 ± 8 | 64 ± 5 | 64 ± 4 | 67 ± 3 | 69 ± 2 | 71 ± 3 |
| CAL | 129 ± 8 | 64 ± 5 | 66 ± 3 | 69 ± 3 | 71 ± 2 | 72 ± 2 | 77 ± 2 |
| T35 | T40 | T45 | T50 | T55 | T60 | ||
| HR (beats/min) | |||||||
| ANX | 154 ± 5 | 153 ± 6 | 151 ± 6 | 148 ± 6 | 146 ± 5 | 145 ± 5 | |
| CAL | 148 ± 6 | 147 ± 7 | 144 ± 7 | 144 ± 7 | 143 ± 7 | 143 ± 7 | |
| MAP (mmHg) | |||||||
| ANX | 79 ± 5 | 79 ± 2 | 76 ± 2 | 75 ± 3 | 72 ± 3 | 69 ± 4 | |
| CAL | 78 ± 3 | 74 ± 3 | 77 ± 3 | 78 ± 3 | 76 ± 4 | 76 ± 2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, Y.; Kanda, T. Effects of Pre-Anesthesia Anxiety on Propofol Induction Dose in Cats. Animals 2021, 11, 2126. https://doi.org/10.3390/ani11072126
Shimizu Y, Kanda T. Effects of Pre-Anesthesia Anxiety on Propofol Induction Dose in Cats. Animals. 2021; 11(7):2126. https://doi.org/10.3390/ani11072126
Chicago/Turabian StyleShimizu, Yuki, and Teppei Kanda. 2021. "Effects of Pre-Anesthesia Anxiety on Propofol Induction Dose in Cats" Animals 11, no. 7: 2126. https://doi.org/10.3390/ani11072126
APA StyleShimizu, Y., & Kanda, T. (2021). Effects of Pre-Anesthesia Anxiety on Propofol Induction Dose in Cats. Animals, 11(7), 2126. https://doi.org/10.3390/ani11072126