
Common Digital Extensor Tendon Injury in Three Sporting Dogs

Abstract
:Simple Summary
Abstract
1. Introduction
2. Case Details
2.1. Case 1
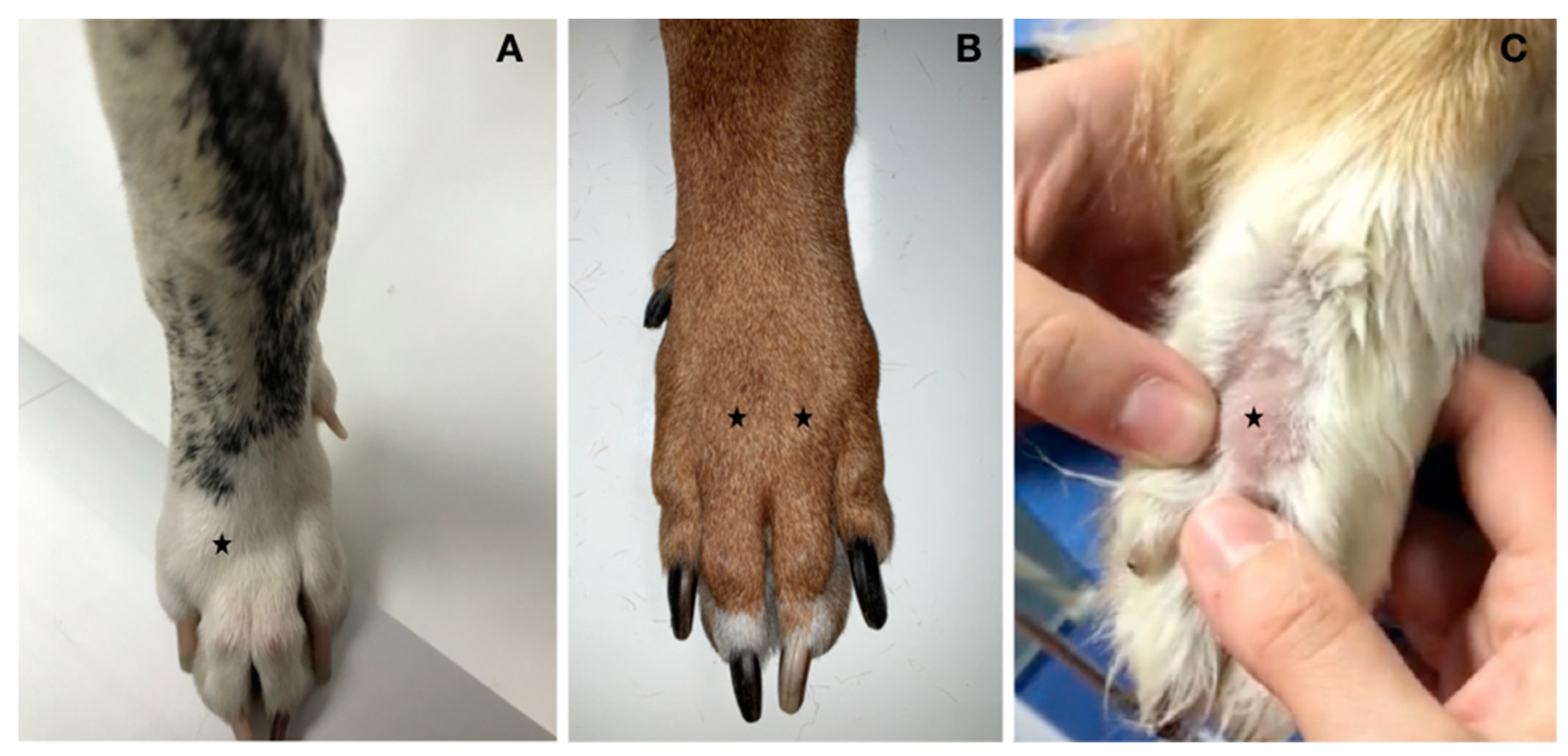
2.1.1. Clinical Examination
2.1.2. Radiographic Examination
2.1.3. Ultrasonographic Examination (US)
2.2. Case 2
2.2.1. Clinical Examination
2.2.2. Radiographic Examination
2.2.3. Ultrasonographic Examination
2.3. Case 3
2.3.1. Clinical Examination
2.3.2. Radiographic Examination
2.3.3. Ultrasonographic Examination
3. Treatment Options and Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gladden, J.R. Boxer’s knuckle: A preliminary report. Am. J. Surg. 1957, 93, 388–397. [Google Scholar] [CrossRef]
- Stracher, M.; Posner, M.A. Boxer’s knuckle. Tech. Hand Up. Extrem. Surg. 2002, 6, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Hermanson, J.W. The muscular system. In Miller’s Anatomy of the Dog, 4th ed.; Hevans, H.E., De Lahunta, A., Eds.; Elsevier-Saunders: St. Louis, MO, USA, 2013; pp. 242–243. [Google Scholar]
- Willekens, I.; Kichouh, M.; Boulet, C.; De Maeseneer, M.; Clarys, J.P.; de Mey, J. Ultrasound follow-up of posttraumatic injuries of the sagittal band of the dorsal hood treated by a conservative approach. Eur. J. Radiol. 2015, 84, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Melone, C.P., Jr.; Polatsch, D.B.; Beldner, S. Disabling hand injuries in boxing: Boxer’s knuckle and traumatic carpal boss. Clin. Sports Med. 2009, 28, 609–621. [Google Scholar] [CrossRef] [PubMed]
- Hame, S.L.; Melone, C.P., Jr. Boxer’s knuckle in the professional athlete. Am. J. Sports Med. 2000, 28, 879–882. [Google Scholar] [CrossRef] [PubMed]
- Taroni, M.; Cabon, Q.; Fèbre, M.; Cachon, T.; Saulnier, N.; Carozzo, C.; Maddens, S.; Labadie, F.; Robert, C.; Viguier, C. Evaluation of the effect of a single intra-articular injection of allogenic neonatal mesenchymal stromal cells compared to oral non-steroidal anti-inflammatory treatment on the postoperative musculoskeletal status and gait of dogs over a 6-months period after tibial plateau leveling osteotomy: A pilot study. Front. Vet. Sci. 2017, 4, 83. [Google Scholar] [CrossRef] [PubMed]
- Bertal, M.; Vezzoni, A.; Houdellier, B.; Bogaerts, E.; Stock, E.; Polis, I.; Deforce, D.; Saunders, J.H.; Broeckx, B.J.G. Intra- and inter-observer variability of measurements of the laxity index on stress radiographs performed with the Vezzoni-modified Badertscher hip distension device. Vet. Comp. Orthop. Traumatol. 2018, 31, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Piras, A.; Bruecker, K. Common pathology associated with the digits and metacarpal regions. Vet. Clin. North Am. Small Anim. Pract. 2021, 51, 263–284. [Google Scholar] [CrossRef] [PubMed]
- Chanda, M.; Klinpayom, C.; Sungsuwan, T.; Senarat, W.; Thongkham, E.; Kamlangdee, A.; Senarat, N. Diagnostic imaging features, cytological examination, and treatment of lymphocytic tenosynovitis of the common digital extensor tendon sheath in an eventing horse. Vet. Anim. Sci. 2021, 14, 100209. [Google Scholar] [CrossRef] [PubMed]
- Roe, C.S. Injuries and diseases of tendons. In Canine Sports Medicine and Surgery, 1st ed.; Bloomberg, M.S., Dee, J.F., Taylor, R.A., Eds.; Saunders Company: Philadelphia, PA, USA, 1998; pp. 92–99. [Google Scholar]
- Walter, R.M.; Carrier, D.R. Rapid acceleration in dogs: Ground forces and body posture dynamics. J. Exp. Biol. 2009, 212, 1930–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton-Wells, R.D. Injuries of the digits and pads. In Canine Sports Medicine and Surgery, 1st ed.; Bloomberg, M.S., Dee, J.F., Taylor, R.A., Eds.; Saunders Company: Philadelphia, PA, USA, 1998; pp. 165–173. [Google Scholar]
- Lin, J.D.; Strauch, R.J. Closed soft tissue extensor mechanism injuries (mallet, boutonniere, and sagittal band). J. Hand Surg. 2014, 39, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Arai, K.; Toh, S.; Nakahara, S.; Nishikawa, S.; Harata, S. Treatment of soft tissue injuries to the dorsum of the metacarpophalangeal joint (boxer’s knuckle). J. Hand Surg. Br. Eur. Vol. 2002, 21, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Rayan, G.M.; Murray, D. Classification and treatment of closed sagittal band injuries. J. Hand Surg. 1994, 19, 590–594. [Google Scholar] [CrossRef]
- Skinner, S.; Isaacs, J. Extensor tendon injuries in the athlete. Clin. Sports Med. 2020, 39, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.L.; Dickey, J.P.; Bent, L.R.; Thomason, J.J.; Moëns, N.M.M. Survey-based of risk factors for injury among dogs participating in agility training and competition events. J. Am. Vet. Med. Assoc. 2013, 243, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Fowler, D. Distal limb and paw injuries. Vet. Clin. Small Anim. Pract. 2006, 36, 819–845. [Google Scholar] [CrossRef] [PubMed]
- Davies, P.E. Track injuries in racing Greyhounds. Aust. Vet. J. 1967, 43, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Ben, R.; Lee, D.H.; Nicolodi, D.J. Boxer knuckle (injury of the extensor hood with extensor tendon subluxation): Diagnosis with dynamic US-report of three cases. Radiology 2003, 228, 642–646. [Google Scholar] [CrossRef] [PubMed]
- Hillman, D.; Rheinboldt, M.; Petraszko, A. Sonographic imaging of hand and wrist injuries: Applications in the ER setting. Emerg. Radiol. 2019, 26, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Kleinhenz, B.P.; Adams, B.P. Closed sagittal band injury of the metacarpophalangeal joint. J. Am. Accad. Orthop. Surg. 2015, 23, 415–423. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Degree of Lameness |
|---|---|
| 1 | No lameness |
| 2 | Intermittent weight-bearing lameness |
| 3 | Permanent weight-bearing lameness |
| 4 | Non-weight-bearing lameness |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franini, A.; Entani, M.G. Common Digital Extensor Tendon Injury in Three Sporting Dogs. Animals 2022, 12, 2619. https://doi.org/10.3390/ani12192619
Franini A, Entani MG. Common Digital Extensor Tendon Injury in Three Sporting Dogs. Animals. 2022; 12(19):2619. https://doi.org/10.3390/ani12192619
Chicago/Turabian StyleFranini, Alessio, and Maria Grazia Entani. 2022. "Common Digital Extensor Tendon Injury in Three Sporting Dogs" Animals 12, no. 19: 2619. https://doi.org/10.3390/ani12192619
APA StyleFranini, A., & Entani, M. G. (2022). Common Digital Extensor Tendon Injury in Three Sporting Dogs. Animals, 12(19), 2619. https://doi.org/10.3390/ani12192619