
Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Enrolment
2.2. Questionnaire
2.3. Study Design
2.3.1. Homework Protocols
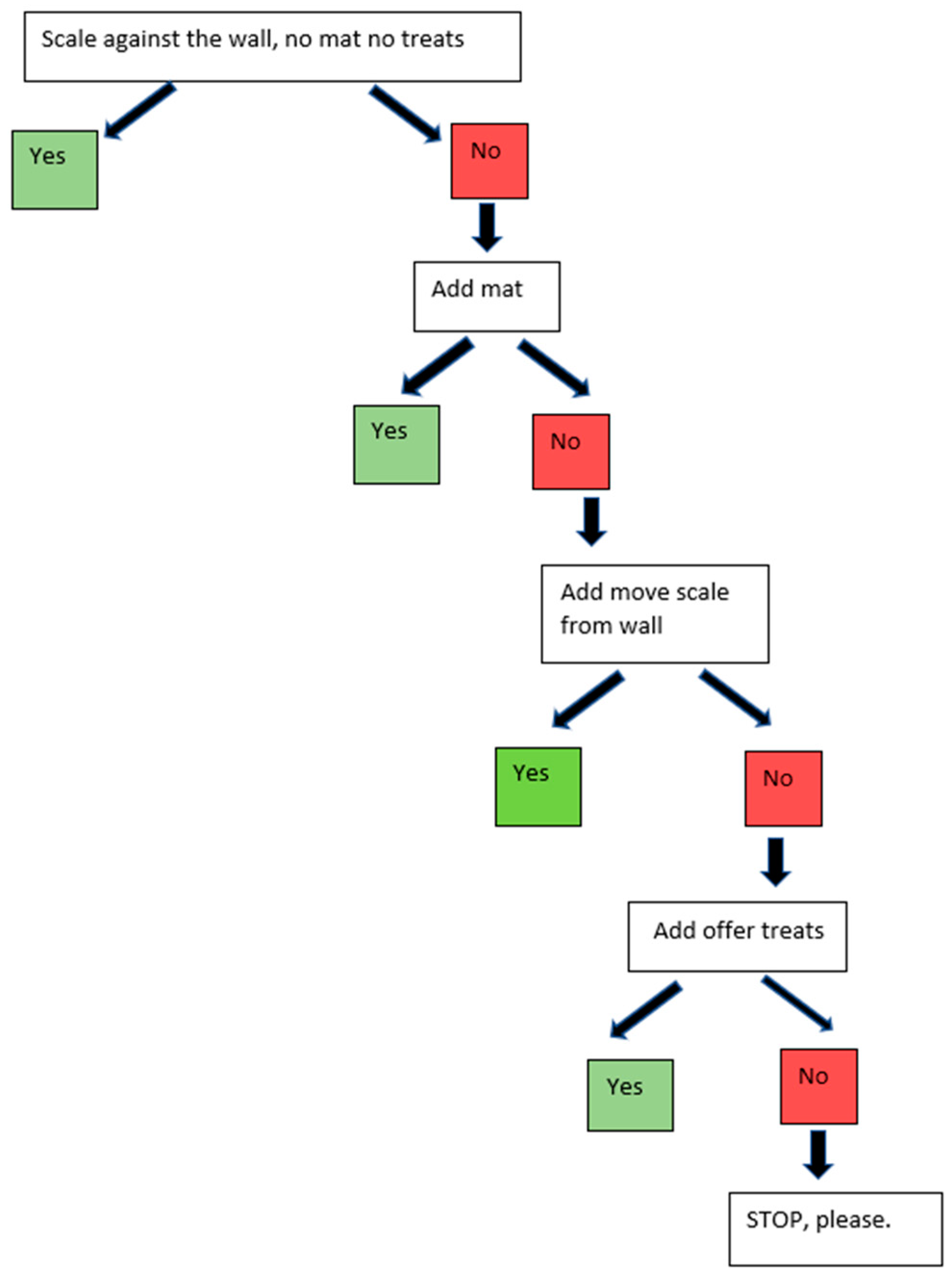
2.3.2. Scale Protocols
2.3.3. Physical Exam and Blood Draw Protocols
2.4. Physiological Measurements
2.5. Statistical Methodology
3. Results
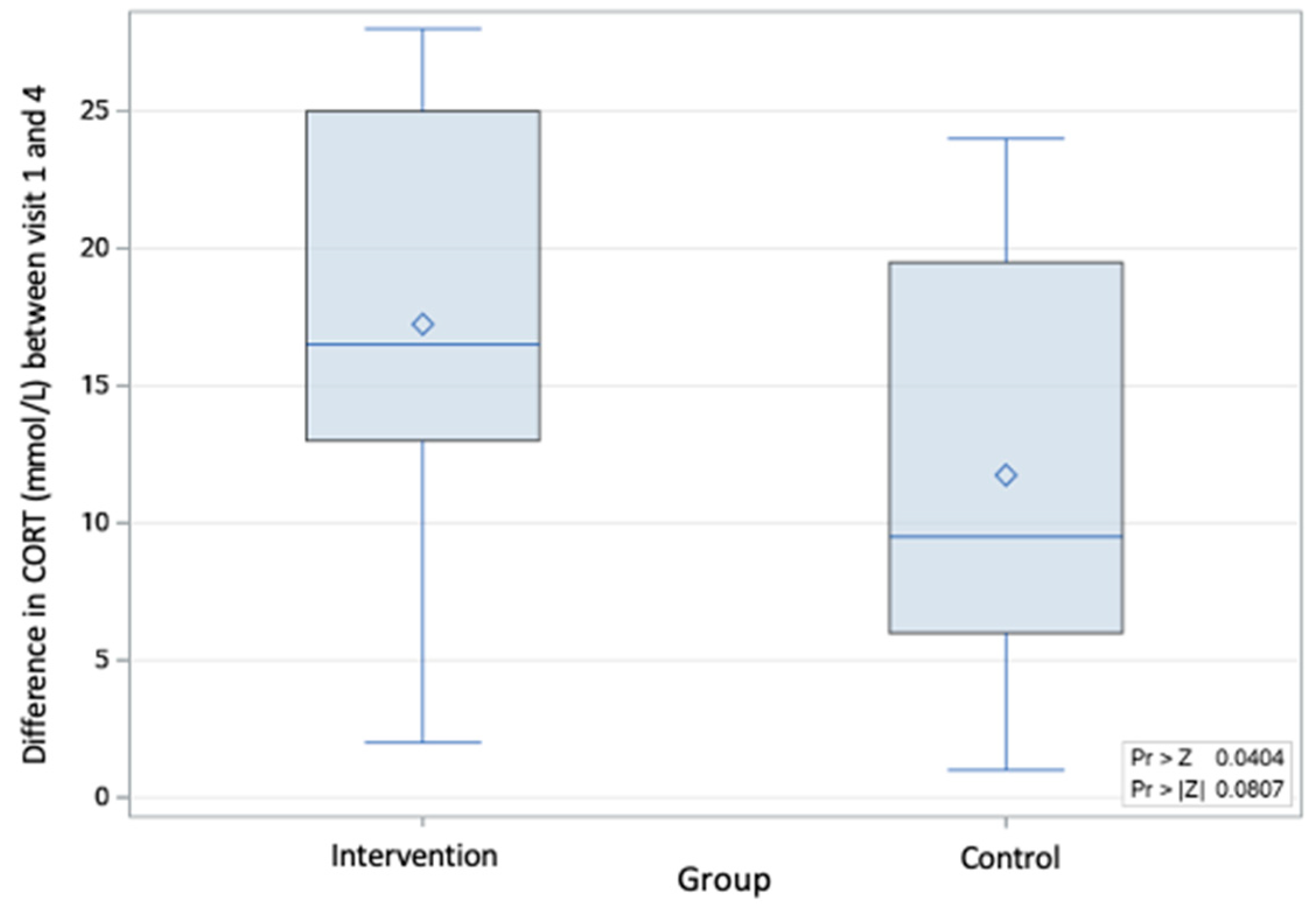
3.1. Changes between Control and Intervention Groups
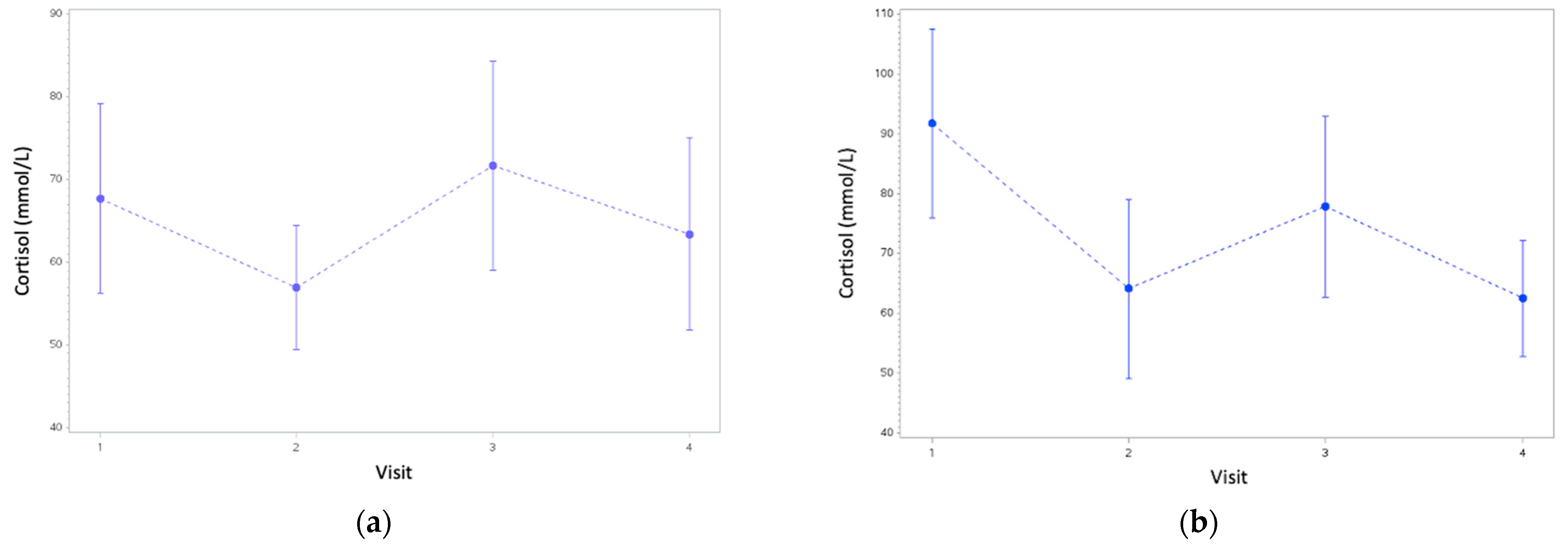
3.2. Changes within Control and Intervention Groups
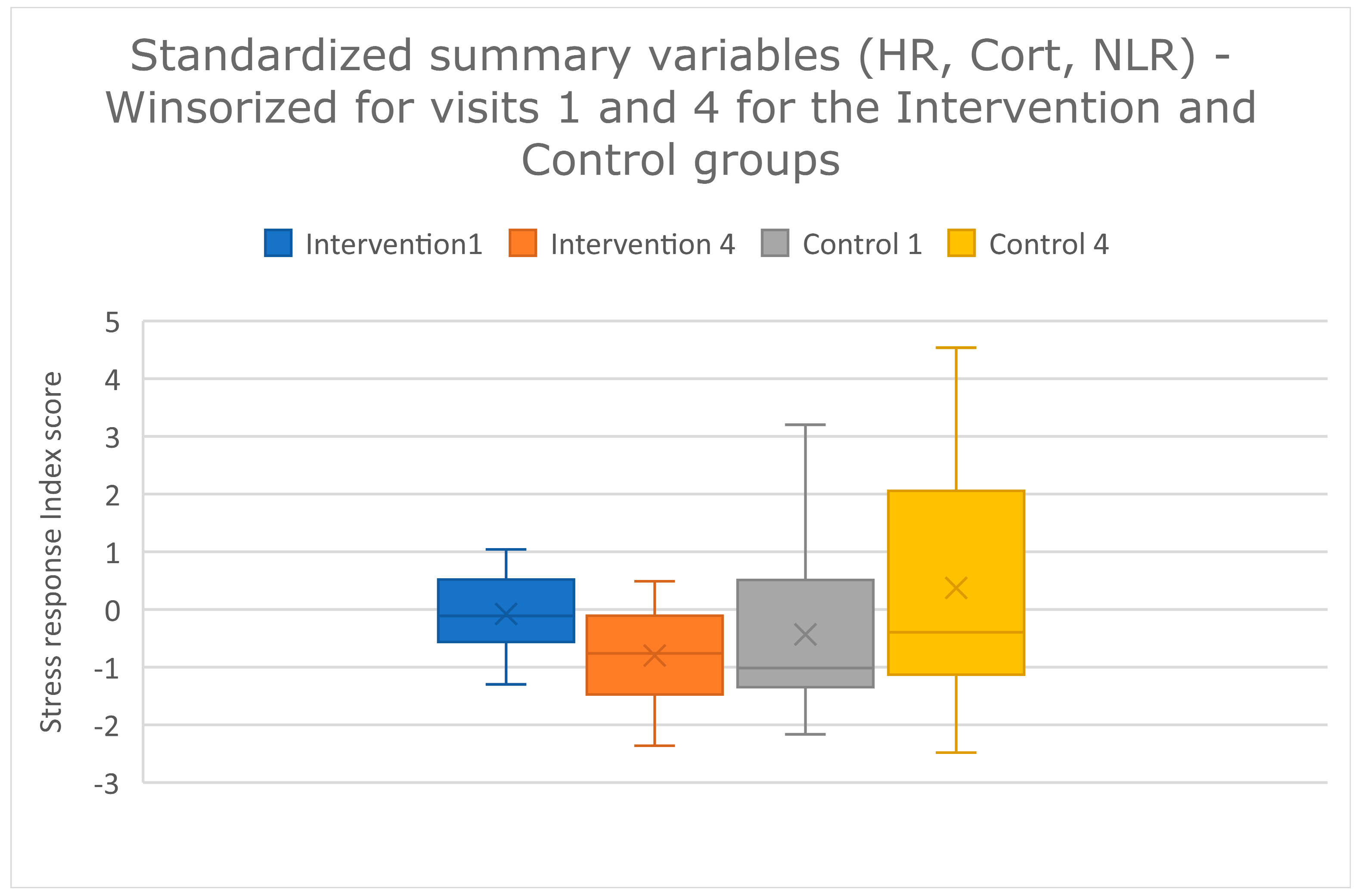
3.3. Stress Response Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Döring, D.; Roscher, A.; Scheipl, F.; Küchenhoff, H.; Erhard, M.H. Fear-Related Behaviour of Dogs in Veterinary Practice. Vet. J. 2009, 182, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Stanford, T.L. Behavior of Dogs Entering a Veterinary Clinic. Appl. Anim. Ethol. 1981, 7, 271–279. [Google Scholar] [CrossRef]
- Mariti, C.; Raspanti, E.; Zilocchi, M.; Carlone, B.; Gazzano, A. The Assessment of Dog Welfare in the Waiting Room of a Veterinary Clinic. Anim. Welf. 2015, 24, 299–305. [Google Scholar] [CrossRef]
- Hernander, L. Factors Influencing Dogs’ Stress Level in the Waiting Room at a Veterinary Clinic; Student Report; Department of Animal Environment and Health, Swedish University of Agricultural Sciences: Skara, Sweden, 2008; ISSN 1652-280X. [Google Scholar]
- Mariti, C.; Pierantoni, L.; Sighieri, C.; Gazzano, A. Guardians’ Perceptions of Dogs’ Welfare and Behaviors Related to Visiting the Veterinary Clinic. J. Appl. Anim. Welf. Sci. 2017, 20, 24–33. [Google Scholar] [CrossRef]
- Perego, R.; Proverbio, D.; Spada, E. Increases in Heart Rate and Serum Cortisol Concentrations in Healthy Dogs Are Positively Correlated with an Indoor Waiting-Room Environment. Vet. Clin. Pathol. 2014, 43, 67–71. [Google Scholar] [CrossRef] [Green Version]
- Stellato, A.C.; Hoffman, H.; Gowland, S.; Dewey, C.E.; Widowski, T.M.; Niel, L. Effect of High Levels of Background Noise on Dog Responses to a Routine Physical Examination in a Veterinary Setting. Appl. Anim. Behav. Sci. 2019, 214, 64–71. [Google Scholar] [CrossRef]
- Stellato, A.C.; Flint, H.E.; Dewey, C.E.; Widowski, T.M.; Niel, L. Risk-Factors Associated with Veterinary-Related Fear and Aggression in Owned Domestic Dogs. Appl. Anim. Behav. Sci. 2021, 241, 105374. [Google Scholar] [CrossRef]
- Dreschel, N.A. The Effects of Fear and Anxiety on Health and Lifespan in Pet Dogs. Appl. Anim. Behav. Sci. 2010, 125, 157–162. [Google Scholar] [CrossRef]
- Edwards, P.T.; Smith, B.P.; McArthur, M.L.; Hazel, S.J. Fearful Fido: Investigating Dog Experience in the Veterinary Context in an Effort to Reduce Distress. Appl. Anim. Behav. Sci. 2019, 213, 14–25. [Google Scholar] [CrossRef]
- Moberg, G.P. Biological Response to Stress: Implications for Animal Welfare. In The Biology of Animal Stress: Basic Principles and Implications for Animal Welfare; CABI Books: Wallingford, UK, 2000; ISBN 9780851993591. [Google Scholar]
- Gouin, J.-P.; Kiecolt-Glaser, J.K. The Impact of Psychological Stress on Wound Healing: Methods and Mechanisms. Immunol. Allergy Clin. N. Am. 2011, 31, 81–93. [Google Scholar] [CrossRef] [Green Version]
- Dhabhar, F.S. Enhancing versus Suppressive Effects of Stress on Immune Function: Implications for Immunoprotection and Immunopathology. Neuroimmunomodulation 2009, 16, 300–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volk, J.O.; Felsted, K.E.; Thomas, J.G.; Siren, C.W. Executive Summary of the Bayer Veterinary Care Usage Study. J. Am. Vet. Med. Assoc. 2011, 238, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Overall, K.L. Embracing Behavior as a Core Disipline: Creating the Behavior-Centered Practice. In Manual of Clinical Behavioral Medicine for Dogs and Cats; Elsevier: St. Louis, MO, USA, 2013; pp. 2–44. ISBN 978-0-323-00890-7. [Google Scholar]
- Lloyd, J. Minimising Stress for Patients in the Veterinary Hospital: Why It Is Important and What Can Be Done about It. Vet. Sci. 2017, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Riemer, S.; Heritier, C.; Windschnurer, I.; Pratsch, L.; Arhant, C.; Affenzeller, N. A Review on Mitigating Fear and Aggression in Dogs and Cats in a Veterinary Setting. Animals 2021, 11, 158. [Google Scholar] [CrossRef] [PubMed]
- Mandese, W.W.; Griffin, F.C.; Reynolds, P.S.; Blew, A.C.; Deriberprey, A.S.; Estrada, A.H. Stress in Client-owned Dogs Related to Clinical Exam Location: A Randomised Crossover Trial. J. Small Anim. Pract. 2021, 62, 82–88. [Google Scholar] [CrossRef]
- Overall, K.L. Evidence-Based Paradigm Shifts in Veterinary Behavioral Medicine. J. Am. Vet. Med. Assoc. 2019, 254, 798–807. [Google Scholar] [CrossRef]
- Stellato, A.; Jajou, S.; Dewey, C.E.; Widowski, T.M.; Niel, L. Effect of a Standardized Four-Week Desensitization and Counter-Conditioning Training Program on Pre-Existing Veterinary Fear in Companion Dogs. Animals 2019, 9, 767. [Google Scholar] [CrossRef] [Green Version]
- Godbout, M.; Frank, D. Persistence of Puppy Behaviors and Signs of Anxiety during Adulthood. J. Vet. Behav. 2011, 6, 92. [Google Scholar] [CrossRef]
- Goddard, A.W.; Ball, S.G.; Martinez, J.; Robinson, M.J.; Yang, C.R.; Russell, J.M.; Shekhar, A. Current Perspectives of the Roles of the Central Norepinephrine System in Anxiety and Depression. Depress. Anxiety 2010, 27, 339–350. [Google Scholar] [CrossRef]
- Mormède, P.; Andanson, S.; Aupérin, B.; Beerda, B.; Guémené, D.; Malmkvist, J.; Manteca, X.; Manteuffel, G.; Prunet, P.; van Reenen, C.G.; et al. Exploration of the Hypothalamic–Pituitary–Adrenal Function as a Tool to Evaluate Animal Welfare. Physiol. Behav. 2007, 92, 317–339. [Google Scholar] [CrossRef]
- Hickman, D.L. Evaluation of the Neutrophil:Lymphocyte Ratio as an Indicator of Chronic Distress in the Laboratory Mouse. Lab Anim. 2017, 46, 303–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaac, V.; Wu, C.-Y.; Huang, C.-T.; Baune, B.T.; Tseng, C.-L.; McLachlan, C.S. Elevated Neutrophil to Lymphocyte Ratio Predicts Mortality in Medical Inpatients with Multiple Chronic Conditions. Medicine 2016, 95, e3832. [Google Scholar] [CrossRef]
- Grillon, C.; Ameli, R.; Goddard, A.; Woods, S.W.; Davis, M. Baseline and Fear-Potentiated Startle in Panic Disorder Patients. Biol. Psychiatry 1994, 35, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, H. Plasma Creatine Phosphokinase Activity, Hypothermia, and Stress. Am. J. Physiol.-Leg. Content 1971, 221, 896–901. [Google Scholar] [CrossRef]
- Overall, K.L.; Dunham, A.E.; Juarbe-Diaz, S.V. Phenotypic Determination of Noise Reactivity in 3 Breeds of Working Dogs: A Cautionary Tale of Age, Breed, Behavioral Assessment, and Genetics. J. Vet. Behav. 2016, 16, 113–125. [Google Scholar] [CrossRef] [Green Version]
- Overall, K.L.; Dunham, A.E.; Scheifele, P.; Sonstrom Malowski, K. Fear of Noises Affects Canine Problem Solving Behavior and Locomotion in Standardized Cognitive Tests. Appl. Anim. Behav. Sci. 2019, 221, 104863. [Google Scholar] [CrossRef]
- Bryant, D.A.; Dunham, A.E.; Overall, K.L. Roles for Referential Focus in Effective and Efficient Canine Signaling: Do Pet and Working Dogs Differ? J. Vet. Behav. 2018, 27, 55–66. [Google Scholar] [CrossRef]
- Kolevská, J.; Brunclík, V.; Svoboda, M. Circadian Rhythm of Cortisol Secretion in Dogs of Different Daily Activities. Acta Vet. Brno 2003, 72, 599–605. [Google Scholar] [CrossRef]
- Korpivaara, M.; Huhtinen, M.; Aspegrén, J.; Overall, K. Dexmedetomidine Oromucosal Gel Reduces Fear and Anxiety in Dogs during Veterinary Visits: A Randomised, Double-blind, Placebo-controlled Clinical Pilot Study. Vet. Rec. 2021, 189, e832. [Google Scholar] [CrossRef] [PubMed]
- Hauser, H.; Campbell, S.; Korpivaara, M.; Stefanovski, D.; Quinlan, M.; Siracusa, C. In-Hospital Administration of Dexmedetomidine Oromucosal Gel for Stress Reduction in Dogs during Veterinary Visits: A Randomized, Double-Blinded, Placebo-Controlled Study. J. Vet. Behav. 2020, 39, 77–85. [Google Scholar] [CrossRef]
- Marino, C.L.; Cober, R.E.; Iazbik, M.C.; Couto, C.G. White-Coat Effect on Systemic Blood Pressure in Retired Racing Greyhounds: Blood Pressure in Retired Racing Greyhounds. J. Vet. Intern. Med. 2011, 25, 861–865. [Google Scholar] [CrossRef]
- Haskard-Zolnierek, K.; Cobos, B.; Howard, K. White Coat Hypertension: Improving the Patient–Health Care Practitioner Relationship. Psychol. Res. Behav. Manag. 2015, 8, 133. [Google Scholar] [CrossRef] [Green Version]
- Westlund, K. To Feed or Not to Feed: Counterconditioning in the Veterinary Clinic. J. Vet. Behav. 2015, 10, 433–437. [Google Scholar] [CrossRef]
- Crisi, P.E.; De Santis, F.; Giordano, M.V.; Cerasoli, I.; Colucci, F.; Di Tommaso, M.; Luciani, A. Evaluation of Eutectic Lidocaine/Prilocaine Cream for Jugular Blood Sampling in Cats. J. Feline Med. Surg. 2021, 23, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Van Oostrom, H.; Knowles, T.G. The Clinical Efficacy of EMLA Cream for Intravenous Catheter Placement in Client-Owned Dogs. Vet. Anaesth. Analg. 2018, 45, 604–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paediatric and Neonatal Blood Sampling. In WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy; World Health Organization: Geneva, Switzerland, 2010.
- Godbout, M.; Palestrini, C.; Beauchamp, G.; Frank, D. Puppy Behavior at the Veterinary Clinic: A Pilot Study. J. Vet. Behav. 2007, 2, 126–135. [Google Scholar] [CrossRef]
- Lind, A.-K.; Hydbring-Sandberg, E.; Forkman, B.; Keeling, L.J. Assessing Stress in Dogs during a Visit to the Veterinary Clinic: Correlations between Dog Behavior in Standardized Tests and Assessments by Veterinary Staff and Owners. J. Vet. Behav. 2017, 17, 24–31. [Google Scholar] [CrossRef]
- Huber, T.J.; Issa, K.; Schik, G.; Wolf, O.T. The Cortisol Awakening Response Is Blunted in Psychotherapy Inpatients Suffering from Depression. Psychoneuroendocrinology 2006, 31, 900–904. [Google Scholar] [CrossRef]
- Dauvermann, M.R.; Donohoe, G. Cortisol Stress Response in Psychosis from the High-Risk to the Chronic Stage: A Systematic Review. Ir. J. Psychol. Med. 2019, 36, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.C.W.; Shields, G.S.; Trainor, B.C.; Slavich, G.M.; Yonelinas, A.P. Greater Lifetime Stress Exposure Predicts Blunted Cortisol but Heightened DHEA Responses to Acute Stress. Stress Health 2019, 35, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Cobb, M.L.; Iskandarani, K.; Chinchilli, V.M.; Dreschel, N.A. A Systematic Review and Meta-Analysis of Salivary Cortisol Measurement in Domestic Canines. Domest. Anim. Endocrinol. 2016, 57, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Beerda, B.; Schilder, M.B.H.; Bernadina, W.; Van Hooff, J.A.R.A.M.; De Vries, H.W.; Mol, J.A. Chronic Stress in Dogs Subjected to Social and Spatial Restriction. II. Hormonal and Immunological Responses. Physiol. Behav. 1999, 66, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Carbillet, J.; Rey, B.; Lavabre, T.; Chaval, Y.; Merlet, J.; Débias, F.; Régis, C.; Pardonnet, S.; Duhayer, J.; Gaillard, J.-M.; et al. The Neutrophil to Lymphocyte Ratio Indexes Individual Variation in the Behavioural Stress Response of Wild Roe Deer across Fluctuating Environmental Conditions. Behav. Ecol. Sociobiol. 2019, 73, 144. [Google Scholar] [CrossRef]
- Goessling, J.M.; Kennedy, H.; Mendonça, M.T.; Wilson, A.E. A Meta-analysis of Plasma Corticosterone and Heterophil: Lymphocyte Ratios—Is There Conservation of Physiological Stress Responses over Time? Funct. Ecol. 2015, 29, 1189–1196. [Google Scholar] [CrossRef]
- Sapolsky, R.M.; Romero, L.M.; Munck, A.U. How Do Glucocorticoids Influence Stress Responses? Integrating Permissive, Suppressive, Stimulatory, and Preparative Actions*. Endocr. Rev. 2000, 21, 55–89. [Google Scholar] [CrossRef] [Green Version]
- Edwards, P.T.; Smith, B.P.; McArthur, M.L.; Hazel, S.J. At the Heart of a Dog’s Veterinary Experience: Heart Rate Responses in Dogs Vary across a Standard Physical Examination. J. Vet. Behav. 2022, 51, 23–34. [Google Scholar] [CrossRef]
- Csoltova, E.; Martineau, M.; Boissy, A.; Gilbert, C. Behavioral and Physiological Reactions in Dogs to a Veterinary Examination: Owner-Dog Interactions Improve Canine Well-Being. Physiol. Behav. 2017, 177, 270–281. [Google Scholar] [CrossRef]
- Stellato, A.C.; Dewey, C.E.; Widowski, T.M.; Niel, L. Evaluation of Associations between Owner Presence and Indicators of Fear in Dogs during Routine Veterinary Examinations. J. Am. Vet. Med. Assoc. 2020, 257, 1031–1040. [Google Scholar] [CrossRef]
- Davis, M. Neurobiology of Fear Responses: The Role of the Amygdala. J. Neuropsychiatry Clin. Neurosci. 1997, 9, 382–402. [Google Scholar] [CrossRef]
- Pacák, K.; Palkovits, M. Stressor Specificity of Central Neuroendocrine Responses: Implications for Stress-Related Disorders. Endocr. Rev. 2001, 22, 502–548. [Google Scholar] [CrossRef] [Green Version]
- Jaffe, A.S.; Garfinkel, B.T.; Ritter, C.S.; Sobel, B.E. Plasma Mb Creatine Kinase after Vigorous Exercise in Professional Athletes. Am. J. Cardiol. 1984, 53, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Orsucci, D.; Trezzi, M.; Anichini, R.; Blanc, P.; Barontini, L.; Biagini, C.; Capitanini, A.; Comeglio, M.; Corsini, P.; Gemignani, F.; et al. Increased Creatine Kinase May Predict A Worse COVID-19 Outcome. J. Clin. Med. 2021, 10, 1734. [Google Scholar] [CrossRef] [PubMed]
- Overall, K.; Dunham, A.; Acland, G. Responses of Genetically Fearful Dogs to the Lactate Test: Assessment of the Test as Provocative Index and Application in Mechanistic Diagnoses. Mol. Psychiatry 1999, 4, S125. [Google Scholar]
- Yuki, M.; Aoyama, R.; Hirano, T.; Tawada, R.; Ogawa, M.; Naitoh, E.; Kainuma, D.; Nagata, N. Investigation of Serum Cortisol Concentration as a Potential Prognostic Marker in Hospitalized Dogs: A Prospective Observational Study in a Primary Care Animal Hospital. BMC Vet. Res. 2019, 15, 170. [Google Scholar] [CrossRef]
- Hekman, J.; Karas, A.; Sharp, C. Psychogenic Stress in Hospitalized Dogs: Cross Species Comparisons, Implications for Health Care, and the Challenges of Evaluation. Animals 2014, 4, 331–347. [Google Scholar] [CrossRef]
- Hannibal, K.E.; Bishop, M.D. Chronic Stress, Cortisol Dysfunction, and Pain: A Psychoneuroendocrine Rationale for Stress Management in Pain Rehabilitation. Phys. Ther. 2014, 94, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Domjan, M. Elicited Behavior, Habituation, and Sensitization. In The Principles of Learning and Behavior; Domjan, M., Ed.; Cengage Learning: Stamford, CT, USA, 2015; pp. 29–58. ISBN 978-1-285-08856-3. [Google Scholar]
- Erickson, A.; Harbin, K.; MacPherson, J.; Rundle, K.; Overall, K.L. A Review of Pre-Appointment Medications to Reduce Fear and Anxiety in Dogs and Cats at Veterinary Visits. Can. Vet. J. 2021, 62, 952–960. [Google Scholar]
- Korpivaara, M.; Laapas, K.; Huhtinen, M.; Schöning, B.; Overall, K. Dexmedetomidine Oromucosal Gel for Noise-Associated Acute Anxiety and Fear in Dogs-a Randomised, Double-Blind, Placebo-Controlled Clinical Study. Vet. Rec. 2017, 180, 356. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age in Months | Sex | Breed | Weight | Group | Status |
|---|---|---|---|---|---|---|
| 01 | 76 mo | MC | Dachshund | 7.2 kg | Control | Completed |
| 02 | 35 mo | FS | Chihuahua mix | 5.4 kg | Control | Withdrawn |
| 03 | 102 mo | MC | German Shepherd/Husky mix | 30.2 kg | Control | Completed |
| 04 | 46 mo | MC | Springer Spaniel mix | 19.2 kg | Intervention | Completed |
| 05 | 61 mo | FS | Beagle | 13.2 kg | Control | Completed |
| 06 | 73 mo | FS | Shih Tzu mix | 8.2 kg | Control | Completed |
| 07 | 31 mo | MC | Pitbull mix | 30.4 kg | Intervention | Completed |
| 08 | 120 mo | MC | Dalmatian | 27.0 kg | Intervention | Completed |
| 09 | 31 mo | MC | Bernese Mountain Dog | 38.8 kg | Intervention | Completed |
| 10 | 15 mo | MC | Maltese/Lhasa Apso mix | 4.6 kg | Intervention | Completed |
| 11 | 38 mo | FS | Springer Spaniel | 21.2 kg | Control | Completed |
| 12 | 48 mo | MC | Dalmatian | 29.4 kg | Intervention | Completed |
| 13 | 84 mo | FS | American Staffordshire Terrier Mix | 20.8 kg | Control | Completed |
| 14 | 24 mo | FS | Belgian Groenendael Sheepdog | 21.2 kg | Control | Completed |
| 15 | 31 mo | MC | Mastiff mix | 34.0 kg | Intervention | Completed |
| 16 | 50 mo | FS | Chihuahua mix | 3.0 kg | Intervention | Completed |
| 17 | 80 mo | FS | German Shepherd mix | 27.6 kg | Control | Completed |
| 18 | 29 mo | FS | Labradoodle | 28.8 kg | Control | Completed |
| 19 | 160 mo | MC | Golden Retriever | 38.8 kg | Intervention | Completed |
| 20 | 68 mo | MC | Poodle Dachshund mix | 11.4 kg | Intervention | Completed |
| 21 | 102 mo | MC | Labrador Retriever | 64.0 kg | Control | Completed |
| 22 | 127 mo | FS | Chihuahua mix | 4.2 kg | Control | Completed |
| 23 | 7 mo | FI | Golden Retriever | 23.6 kg | Control | Completed |
| 24 | 42 mo | MC | Labrador mix | 20.6 kg | Intervention | Completed |
| 25 | 19 mo | FS | Terrier mix | 6.6 kg | Intervention | Completed |
| 26 | 114 mo | FS | Newfoundland dog | 56.2 kg | Control | Completed |
| 27 | 62 mo | FS | Labrador Retriever | 25.0 kg | Intervention | Completed |
| 28 | 24 mo | FS | English Bulldog | 25.8 kg | Control | Withdrawn |
| 29 | 52 mo | MC | Toy Goldendoodle | 6.5 kg | Control | Completed |
| 30 | 9 mo | MI | Australian Cattle Dog | 21.5 kg | Control | Completed |
| Control Treatment | Intervention Treatment | |
|---|---|---|
| Scale (See Figure 1) |
|
|
| Physical exam |
|
|
| Blood draw |
|
|
| Homework |
|
| Physical Examination Protocol |
|---|
| 1. Dog stroked gently from head to base of tail three times |
| 2. Hand placed over the thigh pulse point for 30 s |
| 3. Lidocaine (2.5% lidocaine/2.5% prilocaine) put on legs (two saphenous and one cephalic) for intervention dogs (control dogs are just touched in these areas) |
| 4. Auscultation of heart and lungs 15 s from each side of the chest |
| 5. Manual manipulation of lymph nodes (in order submandibular, prescapular, popliteal) |
| 6. Gentle abdominal palpation undertaken for 15 s |
| 7. Each paw lifted for 5 s for testing placement; first hind limbs and then fore limbs |
| 8. Lifting of upper lips (control of the oral mucous membranes) |
| 9. Observation of external ear canals for 5 s each (without an otoscope) |
| 10. Ear thermometer placed in position until reading |
| 11. Eyes examined directly (observation of the conjunctiva, checking of the cornea) for 5 s each |
| 12. Venepuncture |
| 13. Gently put your hand on the dog’s back and tell them they are good |
| 14. Remove from table and give treat, or if the dog is on the floor, just give the treat (note whether the dog takes the treat on record) |
| 15. Walk client to parking lot and give treat mid-way to car (note response on record) |
| Physiological Marker | Stress Measurement |
|---|---|
| Serum cortisol | Acute stress |
| Neutrophil lymphocyte ratio | Chronic stress associated with inflammation |
| Heart rate | Acute stress—immediate sympathetic response |
| Creatine kinase | Muscle damage associated with panic response |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Squair, C.; Proudfoot, K.; Montelpare, W.; Overall, K.L. Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements. Animals 2023, 13, 1253. https://doi.org/10.3390/ani13071253
Squair C, Proudfoot K, Montelpare W, Overall KL. Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements. Animals. 2023; 13(7):1253. https://doi.org/10.3390/ani13071253
Chicago/Turabian StyleSquair, Camille, Kathryn Proudfoot, William Montelpare, and Karen L. Overall. 2023. "Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements" Animals 13, no. 7: 1253. https://doi.org/10.3390/ani13071253
APA StyleSquair, C., Proudfoot, K., Montelpare, W., & Overall, K. L. (2023). Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements. Animals, 13(7), 1253. https://doi.org/10.3390/ani13071253