

Equine Gastric Ulcer Syndrome: An Update on Current Knowledge

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Terminology
2. Prevalence
3. Risk Factors
4. Clinical Signs
4.1. Colic
4.2. Inappetence and Weight Loss
4.3. Poor Coat Quality
4.4. Diarrhea
4.5. Behavior
4.6. Poor Performance
5. Pathophysiology
5.1. Equine Squamous Gastric Disease
5.2. Equine Glandular Gastric Disease
5.3. Non-Steroidal Anti-inflammatory Drugs
5.4. Helicobacter spp.
5.5. Microbiota
5.6. Management
6. Diagnosis
7. Grading
- Grade 0 Epithelium intact, no appearance of hyperkeratosis
- Grade 1 Mucosa intact, areas of hyperkeratosis
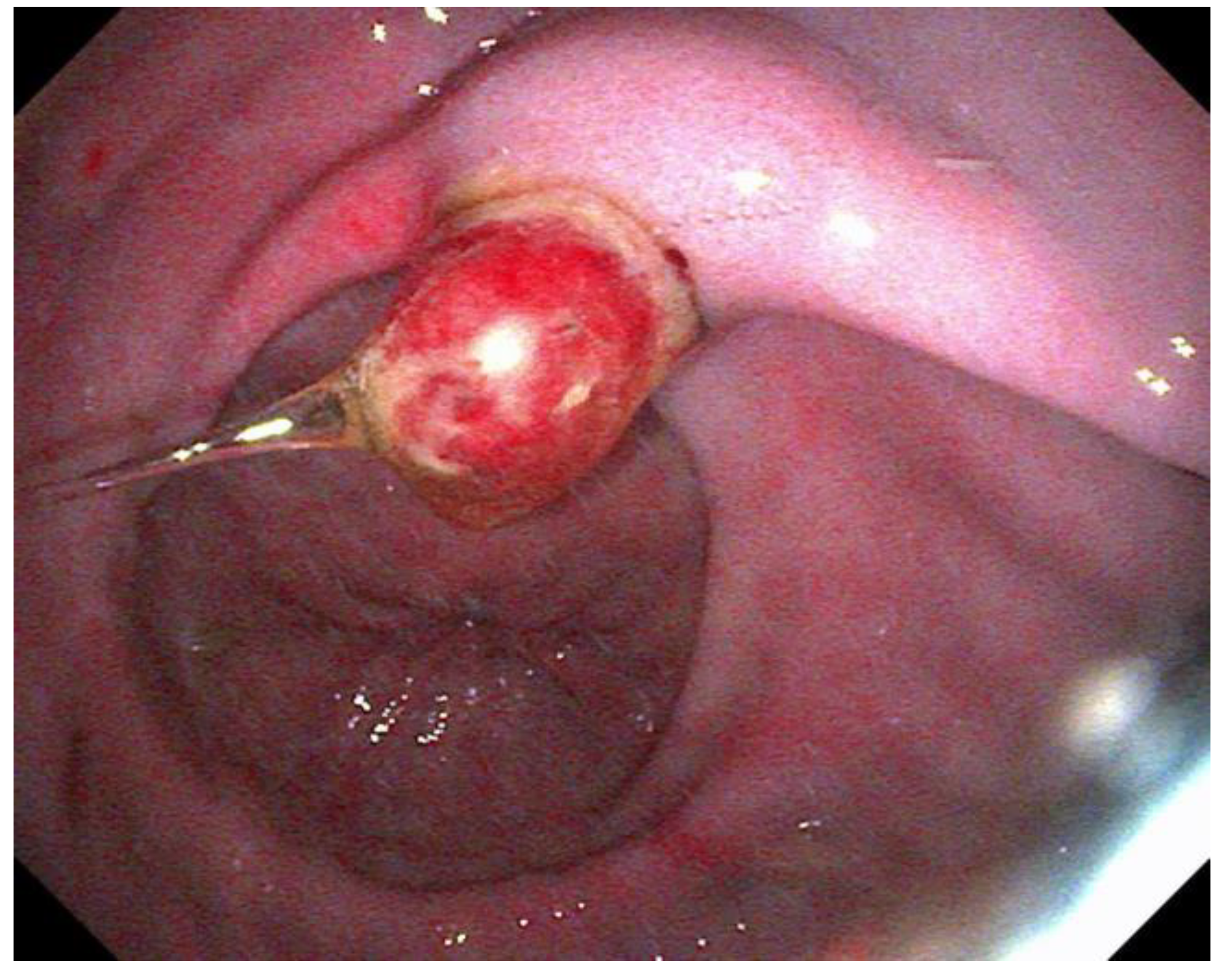
- Grade 2 Small, single or multifocal lesions (Figure 2)
- Grade 3 Large single or extensive superficial lesions
- Grade 4 Extensive lesions with areas of deep lesions
8. Treatment
8.1. Omeprazole
8.2. Sucralfate
8.3. Esomeprazole
8.4. H2 Receptor Antagonists
8.5. Misoprostol
8.6. Risks of Omeprazole
9. Discontinuation of Acid Suppressive Therapy
10. Prevention
10.1. Management
10.2. Nutraceuticals
10.3. Pharmaceuticals
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sykes, B.W.; Hewetson, M.; Hepburn, R.J.; Luthersson, N.; Tamzali, Y. European College of Equine Internal Medicine Con-sensus Statement-Equine Gastric Ulcer Syndrome in Adult Horses. J. Vet. Intern. Med. 2015, 29, 1288–1299. [Google Scholar] [CrossRef] [PubMed]
- Hewetson, M.; McGuire, C. Equine squamous gastric disease and delayed gastric emptying—The chicken or the egg? Equine Vet. Educ. 2022, 34, 460–466. [Google Scholar] [CrossRef]
- Berschneider, H.M.; Blikslager, A.T.; Roberts, M.C. Role of duodenal reflux in nonglandular gastric ulcer disease of the mature horse. Equine Vet. J. 1999, 29, 24–29. [Google Scholar] [CrossRef]
- Bezdekova, B.; Wohlsein, P.; Venner, M. Chronic severe pyloric lesions in horses: 47 cases. Equine Vet. J. 2020, 52, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Sykes, B.; Kathawala, K.; Song, Y.; Garg, S.; Page, S.; Underwood, C.; Mills, P. Preliminary investigations into a novel, long–acting, injectable, intramuscular formulation of omeprazole in the horse. Equine Vet. J. 2017, 49, 795–801. [Google Scholar] [CrossRef] [Green Version]
- Hewetson, M.; Sykes, B.W.; Hallowell, G.D.; Tulamo, R.-M. Diagnostic accuracy of blood sucrose as a screening test for equine gastric ulcer syndrome (EGUS) in adult horses. Acta Vet. Scand. 2017, 59, 15. [Google Scholar] [CrossRef] [Green Version]
- Ehlers, K.; Uhlig, A.; Recknagel, S.; Snyder, A.; Breuer, J.; Arnold, C.; Graneß, N.; Schusser, G.F. Mucosal lesions in the pyloric area—Retrospective study on 315 equine patients (2004–2013). Pferdeheilkunde 2016, 32, 96–102. [Google Scholar] [CrossRef]
- Pedersen, S.K.; Cribb, A.E.; Windeyer, M.C.; Read, E.K.; French, D.; Banse, H.E. Risk factors for equine glandular and squamous gastric disease in show jumping Warmbloods. Equine Vet. J. 2018, 50, 747–751. [Google Scholar] [CrossRef]
- Gehlen, H.; Reimer-Diesbrock, S.; Stockle, S. Prevalence, anatomical distribution and risk factors associated with equine gastric ulceration syndrome in American Quarter Horses. Pferdeheilkunde 2019, 35, 403–415. [Google Scholar] [CrossRef] [Green Version]
- Banse, H.E.; Andrews, F.M. Equine glandular gastric disease: Prevalence, impact and management strategies. Vet. Med. 2019, 10, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Hewetson, M.; Tallon, R. Equine Squamous Gastric Disease: Prevalence, Impact and Management. Vet. Med. 2021, 12, 381–399. [Google Scholar] [CrossRef]
- Cate, R.E.; Nielsen, B.D.; Spooner, H.S.; O’Connor-Robison, C.I.; Schott, H.C. Prevalence of gastric ulcers and relationship to other parameters in Standardbred racehorses. Comp. Exerc. Physiol. 2012, 8, 47–52. [Google Scholar] [CrossRef]
- Tamzali, Y.; Marguet, C.; Priymenko, N.; Lyazrhi, F. Prevalence of gastric ulcer syndrome in high-level endurance horses. Equine Vet. J. 2011, 43, 141–144. [Google Scholar] [CrossRef]
- Jonsson, H.; Egenvall, A. Prevalence of gastric ulceration in Swedish Standardbreds in race training. Equine Vet. J. 2006, 38, 209–213. [Google Scholar] [CrossRef] [Green Version]
- Nieto, J.E.; Snyder, J.R.; Beldomenico, P.; Aleman, M.; Kerr, J.W.; Spier, S.J. Prevalence of gastric ulcers in endurance horses—A preliminary report. Vet. J. 2004, 167, 33–37. [Google Scholar] [CrossRef]
- Begg, L.M.; O’Sullivan, C.B. The prevalence and distribution of gastric ulceration in 345 racehorses. Aust. Vet. J. 2003, 81, 199–201. [Google Scholar] [CrossRef]
- Hammond, C.; Mason, D.; Watkins, K. Gastric ulceration in mature Thoroughbred horses. Equine Vet. J. 1986, 18, 284–287. [Google Scholar] [CrossRef]
- Luthersson, N.; Nielsen, K.; Harris, P.; Parkin, T. The prevalence and anatomical distribution of equine gastric ulceration syndrome (EGUS) in 201 horses in Denmark. Equine Vet. J. 2009, 41, 619–624. [Google Scholar] [CrossRef]
- Roy, M.-A.; Vrins, A.; Beauchamp, G.; Doucet, M.Y. Prevalence of Ulcers of the Squamous Gastric Mucosa in Standardbred Horses. J. Vet. Intern. Med. 2005, 19, 744–750. [Google Scholar] [CrossRef]
- Shan, R.; Steel, C.; Sykes, B. The Effects of two Different Withholding Periods of Omeprazole on the Recurrence of Equine Gastric Ulcer Syndrome in Thoroughbred Racehorses. In Proceedings of the European College of Veterinary Sports Medicine and Rehabilitation Scientific Meeting, Pula, Croatia, 20 September–1 October 2022. [Google Scholar]
- Hwang, H.; Dong, H.J.; Han, J.; Cho, S.; Kim, Y.; Lee, I. Prevalence and treatment of gastric ulcers in Thoroughbred racehorses of Korea. J. Vet. Sci. 2022, 23, e19. [Google Scholar] [CrossRef]
- Chameroy, K.A.; Nadeau, J.A.; Bushmich, S.L.; Dinger, J.E.; Hoagland, T.A.; Saxton, A.M. Prevalence of non-glandular gastric ulcers in horses involved in a university riding program. J. Equine Vet. Sci. 2006, 26, 207–211. [Google Scholar] [CrossRef]
- Malmkvist, J.; Poulsen, J.M.; Luthersson, N.; Palme, R.; Christensen, J.W.; Søndergaard, E. Behaviour and stress responses in horses with gastric ulceration. Appl. Anim. Behav. Sci. 2012, 142, 160–167. [Google Scholar] [CrossRef]
- Le Jeune, S.S.; Nieto, J.E.; Dechant, J.E.; Snyder, J.R. Prevalence of gastric ulcers in Thoroughbred broodmares in pasture: A preliminary report. Vet. J. 2009, 181, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Sgorbini, M.; Bonelli, F.; Papini, R.; Busechian, S.; Briganti, A.; Laus, F.; Faillace, V.; Zappulla, F.; Rizk, A.; Rueca, F. Equine gastric ulcer syndrome in adult donkeys: Investigation on prevalence, anatomical distribution, and severity. Equine Vet. Educ. 2018, 30, 206–210. [Google Scholar] [CrossRef]
- Ward, S.; Sykes, B.; Brown, H.; Bishop, A.; Penaluna, L. A comparison of the prevalence of gastric ulceration in feral and domesticated horses in the UK. Equine Vet. Educ. 2015, 27, 655–657. [Google Scholar] [CrossRef]
- Lamglait, B.; Vandenbunder-Beltrame, M.; Trunet, E.; Lemberger, K. Description of gastric ulcers and of their suspected, associated risk factors in deceased wild equids at the Reserve Africaine de Sigean, France (2010–2016). J. Zoo Wildl. Med. 2017, 48, 668–674. [Google Scholar] [CrossRef]
- Sykes, B.; Bowen, M.; Habershon-Butcher, J.; Green, M.; Hallowell, G.D. Management factors and clinical implications of glandular and squamous gastric disease in horses. J. Vet. Intern. Med. 2019, 33, 233–240. [Google Scholar] [CrossRef]
- Sykes, B.W.; Sykes, K.M.; Hallowell, G.D. A comparison of three doses of omeprazole in the treatment of equine gastric ulcer syndrome: A blinded, randomised, dose-response clinical trial. Equine Vet. J. 2015, 47, 285–290. [Google Scholar] [CrossRef]
- Banse, H.E.; Macleod, H.; Crosby, C.; Windeyer, M.C. Prevalence of and risk factors for equine glandular and squamous gastric disease in polo horses. Can. Vet. J. 2018, 59, 880–884. [Google Scholar]
- Aranzales, J.R.M.; Cassou, F.; Andrade, B.S.C.; Alves, G.E.S. Presence of gastric ulcer syndrome in equine from the military police. Arch. Med. Vet. 2012, 44, 185–189. [Google Scholar] [CrossRef]
- Busechian, S.; Sgorbini, M.; Orvieto, S.; Pisello, L.; Zappulla, F.; Briganti, A.; Nocera, I.; Conte, G.; Rueca, F. Evaluation of a questionnaire to detect the risk of developing ESGD or EGGD in horses. Prev. Vet. Med. 2021, 188. [Google Scholar] [CrossRef]
- Columb, M.; Atkinson, M. Statistical analysis: Sample size and power estimations. BJA Educ. 2015, 16, 159–161. [Google Scholar] [CrossRef] [Green Version]
- Sandin, A.; Skidell, J.; Häggström, J.; Nilsson, G. Postmortem findings of gastric ulcers in Swedish horses older than age one year: A retrospective study of 3715 horses (1924–1996). Equine Vet. J. 2000, 32, 36–42. [Google Scholar] [CrossRef]
- Hepburn, R. Endoscopic examination of the squamous and glandular gastric mucosa in sport and leisure horses: 684 horses (2005–2011). In Proceedings of the 11th International Equine Colic Research Symposium, Dublin, Ireland, 7–10 July 2014. [Google Scholar]
- Mönki, J.; Hewetson, M.; Virtala, A.-M. Risk Factors for Equine Gastric Glandular Disease: A Case–Control Study in a Finnish Referral Hospital Population. J. Vet. Intern. Med. 2016, 30, 1270–1275. [Google Scholar] [CrossRef] [Green Version]
- Gehlen, H.; Prieß, A.; Doherr, M. Germany-wide multicentre study on the etiology of gastric mucosal lesions in horses. Pferdeheilkunde 2021, 37, 395–407. [Google Scholar] [CrossRef]
- Rabuffo, T.S.; Hackett, E.S.; Grenager, N.; Boston, R.; Orsini, J.A. Prevalence of Gastric Ulcerations in Horses with Colic. J. Equine Vet. Sci. 2009, 29, 540–546. [Google Scholar] [CrossRef]
- Vatistas, N.J.; Snyder, J.R.; Carlson, G.; Johnson, B.; Arthur, R.M.; Thurmond, M.; Zhou, H.; Lloyd, K.L. Cross-sectional study of gastric ulcers of the squamous mucosa in thoroughbred racehorses. Equine Vet. J. 1999, 29, 34–39. [Google Scholar] [CrossRef]
- Lester, G.; Robertson, I.; Secombe, C. Risk factors for gastric ulceration in Thoroughbred racehorses. In Proceedings of the 53rd Annual Convention of the American Association of Equine Practitioners, Orlando, FL, USA, 1–5 December 2007. [Google Scholar]
- Zuluaga, A.M.; Ramírez, N.F.; Martínez, J.R. Equine gastric ulcerative syndrome in Antioquia (Colombia): Frequency and risk factors. Rev. Colomb. Cienc. Pecu. 2018, 31, 139–149. [Google Scholar] [CrossRef]
- Dionne, R.M.; Vrins, A.; Doucet, M.Y.; Paré, J. Gastric Ulcers in Standardbred Racehorses: Prevalence, Lesion Description, and Risk Factors. J. Vet. Intern. Med. 2003, 17, 218–222. [Google Scholar] [CrossRef]
- Nicol, C.; Davidson, H.; Harris, P.; Waters, A.; Wilson, A. Study of crib-biting and gastric inflammation and ulceration in young horses. Vet. Rec. 2002, 151, 658–662. [Google Scholar] [CrossRef] [Green Version]
- Patiño, J.J.; Vélez, S.A.; Martínez, J.R. Ethological, endocrinological, and gastroscopic evaluation of crib-biting Colombian creole horses. J. Vet. Behav. 2020, 40, 92–97. [Google Scholar] [CrossRef]
- Khan, A.; Hallowell, G.; Underwood, C.; van Eps, A. Continuous fluid infusion per rectum compared with intravenous and nasogastric fluid administration in horses. Equine Vet. J. 2019, 51, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Luthersson, N.; Ýr Þorgrímsdóttir, Ú.; Harris, P.A.; Parkins, T.; Bennet, E.D. Effect of moving from being extensively managed out in pasture into training on the incidence of equine gastric ulcer syndrome in Icelandic horses. J. Am. Vet. Med. Assoc. 2022, 260, S102–S110. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.; Kingston, J.; Mogg, T.; Perkins, N. The prevalence of gastric ulceration in racehorses in New Zealand. N. Z. Vet. J. 2007, 55, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, T.C.; Simmons, R.D.; Payton, M.E.; MacAllister, C.G. Effect of repeated oral administration of hypertonic electrolyte solution on equine gastric mucosa. Equine Vet. J. 2005, 37, 501–504. [Google Scholar] [CrossRef]
- Fedtke, A.; Pfaff, M.; Volquardsen, J.; Venner, M.; Vervuert, I. Effects of feeding different roughage-based diets on gastric mucosa after weaning in Warmblood foals. Pferdeheilkunde 2015, 31, 596–601. [Google Scholar] [CrossRef] [Green Version]
- Tesena, P.; Yingchutrakul, Y.; Roytrakul, S.; Wongtawan, T.; Angkanaporn, K. Serum protein expression in equine glandular gastric disease (EGGD) induced by phenylbutazone. J. Vet. Med. Sci. 2019, 81, 418–424. [Google Scholar] [CrossRef] [Green Version]
- Murray, M.J.; Grodinsky, C.; Anderson, C.W.; Radue, P.F.; Schmidt, G.R. Gastric ulcers in horses: A comparison of endoscopic findings in horses with and without clinical signs. Equine Vet. J. 1989, 21, 68–72. [Google Scholar] [CrossRef]
- Andrews, F.; Nadeau, J. Clinical syndromes of gastric ulceration in foals and mature horses. Equine Vet. J. 1999, 31, 30–33. [Google Scholar] [CrossRef]
- Murray, M.J. Gastric ulceration in horses: 91 cases (1987–1990). J. Am. Vet. Med. Assoc. 1992, 201, 117–120. [Google Scholar]
- Dukti, S.; Perkins, S.; Murphy, J.; Barr, B.; Boston, R.; Southwood, L.; Bernard, W. Prevalence of gastric squamous ulceration in horses with abdominal pain. Equine Vet. J. 2006, 38, 347–349. [Google Scholar] [CrossRef]
- Videla, R.; Andrews, F.M. New Perspectives in Equine Gastric Ulcer Syndrome. Vet. Clin. N. Am. Equine Pract. 2009, 25, 283–301. [Google Scholar] [CrossRef]
- Gough, S.; Hallowell, G.; Rendle, D. Evaluation of the treatment of equine glandular gastric disease with either long-acting–injectable or oral omeprazole. Vet. Med. Sci. 2022, 8, 561–567. [Google Scholar] [CrossRef]
- Gough, S.; Hallowell, G.; Rendle, D. A study investigating the treatment of equine squamous gastric disease with long-acting injectable or oral omeprazole. Vet. Med. Sci. 2020, 6, 235–241. [Google Scholar] [CrossRef]
- Bezděková, B.; Jahn, P.; Vyskočil, M. Gastric ulceration, appetite and feeding practices in Standardbred racehorses in the Czech Republic. Acta Vet. Brno 2008, 77, 603–607. [Google Scholar] [CrossRef] [Green Version]
- McClure, S.R.; Glickman, L.T.; Glickman, N.W. Prevalence of gastric ulcers in show horses. J. Am. Vet. Med. Assoc. 1999, 215, 1130–1133. [Google Scholar]
- Franklin, S.; Brazil, T.; Allen, K. Poor performance associated with equine gastric ulceration syndrome in four Thoroughbred racehorses. Equine Vet. Educ. 2008, 20, 119–124. [Google Scholar] [CrossRef]
- Kollias-Baker, C.; Cox, K.; Jones, J. Evaluation of the effects of omeprazole on physiological indices of performance of horses during incremental treadmill exercise. Vet. Ther. 2001, 2, 361–369. [Google Scholar]
- Kaya-Karasu, G.; Huntington, P.J.; Iben, C.; Onmaz, A.C. Poor Performance Associated with Equine Gastric Ulcer in an Arabian Racehorse. J. Fac. Vet. Med. 2016, 13, 187–192. [Google Scholar]
- Hewetson, M.; Hoksbergen, F.; Berger, S.; Westermann, C.; Gilders, C.; Haggett, E.; Luthersson, N.; Leroux, A.; Couroucé, A.; Wilson, A. Association between owner-perceived clinical signs and the presence of equine glandular disease on endoscopy. Equine Vet. J. 2021, 53, 7. [Google Scholar]
- Ribeiro, G.; Silva, L.C.L.C.; Belli, C.B.; Vargas, L.P.; Piffer, M.L.T.; Mirian, M.; Feijó, V.A.; Fernandes, W.R. Occurrence of gastric ulcers in horses exercised on a treadmill. Cienc. Rural 2016, 46, 909–914. [Google Scholar] [CrossRef] [Green Version]
- Rezazadeh, F.; Gharehaghajlou, Y. Endoscopic Finding of Gastric Ulcer in Rural Horse and Relation with Gasterophilus spp. Iran. J. Vet. Med. 2020, 14, 45–52. [Google Scholar] [CrossRef]
- Sundra, T.; Kelty, E.; Rendle, D. Comparison of 5– and 7–day interval dosing with long-acting injectable omeprazole in the treatment of equine squamous and glandular gastric disease. In Proceedings of the BEVA Congress, Liverpool, UK, 10 September 2022; p. 255. [Google Scholar]
- Banse, H.; Terumi Negrão Watanabe, T.; Abarca-Garcia, N.; Andrews, F.; Cruz-Sanabria, J.; Morales Yniguez, J.M.K.; Del Piero, F. Relationship of gastric and small intestinal inflammation in equine glandular gastric disease. Equine Vet. J. 2019, 51, 22. [Google Scholar] [CrossRef]
- Millares-Ramirez, E.M.; Le Jeune, S.S. Girthiness: Retrospective Study of 37 Horses (2004–2016). J. Equine Vet. Sci. 2019, 79, 100–104. [Google Scholar] [CrossRef]
- Dyson, S.; Bondi, A.; Routh, J.; Pollard, D.; Preston, T.; McConnell, C.; Kydd, J. An investigation of behaviour during tacking-up and mounting in ridden sports and leisure horses. Equine Vet. Educ. 2021, 34, e245–e257. [Google Scholar] [CrossRef]
- Hepburn, R.; Proudman, C. Treatment of ulceration of the gastric glandular mucosa: Retrospective evaluation of omeprazole and sucralfate combination therapy in 204 sport and leisure horses. In Proceedings of the 11th International Equine Colic Research Symposium, Dublin, Ireland, 7–10 July 2014. [Google Scholar]
- Scheidegger, M.D.; Gerber, V.; Bruckmaier, R.M.; van der Kolk, J.H.; Burger, D.; Ramseyer, A. Increased adrenocortical response to adrenocorticotropic hormone (ACTH) in sport horses with equine glandular gastric disease (EGGD). Vet. J. 2017, 228, 7–12. [Google Scholar] [CrossRef]
- Sauer, F.; Bruckmaier, R.; Ramseyer, A.; Vidondo, B.; Scheidegger, M.; Gerber, V. Optimization of an ACTH challenge test to predict the risk of equine glandular gastric disease (EGGD) in horses. In Proceedings of the 10th Annual European College of Equine Internal Medicine Congress, LiÈge, Belgium, 2–4 November 2017. [Google Scholar]
- Prinsloo, M.; Hynd, P.; Franklin, S.; Weaver, S.; van den Boom, R. Hair cortisol concentration is inversely related to the severity of equine squamous gastric disease. Vet. J. 2019, 249, 58–59. [Google Scholar] [CrossRef]
- Kaikkonen, R.; Niinistö, K.; Sykes, B.; Anttila, M.; Sankari, S.; Raekallio, M. Diagnostic evaluation and short-term outcome as indicators of long-term prognosis in horses with findings suggestive of inflammatory bowel disease treated with corticosteroids and anthelmintics. Acta Vet. Scand. 2014, 56, 35. [Google Scholar] [CrossRef] [Green Version]
- Nieto, J.E.; Snyder, J.R.; Vatistas, N.J.; Jones, J.H. Effect of gastric ulceration on physiologic responses to exercise in horses. Am. J. Vet. Res. 2009, 70, 787–795. [Google Scholar] [CrossRef]
- Andrews, F.M.; Buchanan, B.R.; Elliott, S.B.; Al Jassim, R.A.M.; McGowan, C.M.; Saxton, A.M. In vitro effects of hydrochloric and lactic acids on bioelectric properties of equine gastric squamous mucosa. Equine Vet. J. 2008, 40, 301–305. [Google Scholar] [CrossRef]
- Nadeau, J.; Andrews, F.; Patton, C.; Argenzio, R.; Mathew, A.; Saxton, A. Effects of hydrochloric, valeric, and other volatile fatty acids on pathogenesis of ulcers in the nonglandular portion of the stomach of horses. Am. J. Vet. Res. 2003, 64, 413–417. [Google Scholar] [CrossRef]
- Easton, H.; Stewart, A.; Lyons, T.; Parris, M.; Charrier, S. Soluble carbohydrate content of ryegrass cultivars. N. Z. Grassl. Assoc. 2009, 71, 161–166. [Google Scholar] [CrossRef]
- Husted, L.; Sanchez, L.C.; Olsen, S.N.; Baptiste, K.E.; Merritt, A.M. Effect of paddock vs. stall housing on 24 hour gastric pH within the proximal and ventral equine stomach. Equine Vet. J. 2008, 40, 337–341. [Google Scholar] [CrossRef]
- Zebeli, Q.; Tafaj, M.; Weber, I.; Dijkstra, J.; Steingass, H.; Drochner, W. Effects of Varying Dietary Forage Particle Size in Two Concentrate Levels on Chewing Activity, Ruminal Mat Characteristics, and Passage in Dairy Cows1. J. Dairy Sci. 2007, 90, 1929–1942. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo-Figueras, M.; Merritt, A. Effects of exercise on gastric volume and pH in the proximal portion of the stomach of horses. Am. J. Vet. Res. 2002, 63, 1481–1487. [Google Scholar] [CrossRef]
- Murray, M.; Schusser, G.; Pipers, F.; Gross, S. Factors associated with gastric lesions in Thoroughbred racehorses. Equine Vet. J. 1996, 28, 368–374. [Google Scholar] [CrossRef]
- Orsini, J.; Hacjett, E.; Grenager, N. The Effect of Exercise on Equine Gastric Ulcer Syndrome in the Thoroughbred and Standardbred Athlete. J. Equine Vet. Sci. 2009, 29, 167–171. [Google Scholar] [CrossRef]
- Sanchez, C. Disorders of the Gastrointestinal System. In Equine Internal Medicine, 4th ed.; Reed, S., Bayly, W., Sellon, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; p. 808. [Google Scholar]
- Li, X.; Wong, G.; To, K.; Wong, V.; Lai, L.; Chow, D.; Lau, J.; Sung, J.; Ding, C. Bacterial microbiota profiling in gastritis without Helicobacter pylori infection or non-steroidal anti-inflammatory drug use. PLoS ONE 2009, 4, e7985. [Google Scholar] [CrossRef]
- Cardona-Álvarez, J.; Vargas-Vilória, M.; Blanco-Martínez, R. Frequency of gastric pathologies in working horses (Equus caballus) in Córdoba, Colombia. Rev. Cient. Fac. Cienc. Vet. Univ. Zulia 2015, 25, 386–394. [Google Scholar]
- Cardona, J.; Paredes, E.; Fernandez, H. Characterization histopathological of gastritis associated to Helicobacter spp presence in stomach of horses. Rev. MVZ Cord. 2009, 14, 1750–1755. [Google Scholar]
- Crumpton, S.M.; Baiker, K.; Hallowell, G.D.; Habershon–Butcher, J.L.; Bowen, I.M. Diagnostic Value of Gastric Mucosal Biopsies in Horses with Glandular Disease. Equine Vet. J. 2015, 47, 9. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Prieto, A.; Contreras-Aguilar, M.D.; Cerón, J.J.; Ayala, I.; Martin-Cuervo, M.; Gonzalez-Sanchez, J.C.; Jacobsen, S.; Kuleš, J.; Beletić, A.; Rubić, I.; et al. Changes in Proteins in Saliva and Serum in Equine Gastric Ulcer Syndrome Using a Proteomic Approach. Animals 2022, 12, 1169. [Google Scholar] [CrossRef] [PubMed]
- Marqués, F.J.; Epp, T.; Wilson, D.; Ruiz, A.J.; Tokateloff, N.; Manning, S. The prevalence and risk factors of oesophageal and nonglandular gastric lesions in Thoroughbred racehorses in Saskatchewan. Equine Vet. Educ. 2011, 23, 249–254. [Google Scholar] [CrossRef]
- Pedersen, S.K.; Cribb, A.E.; Read, E.K.; French, D.; Banse, H.E. Phenylbutazone induces equine glandular gastric disease without decreasing prostaglandin E2 concentrations. J. Vet. Pharmacol. 2018, 41, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Zuluaga, A.M.; Silveira, A.G.E.; Martínez, A.J.R. Nitric oxide and malondialdehyde in gastric contents and blood in an equine model of gastric ulcer induced by phenylbutazone. Rev. Colomb. Cienc. Pecu. 2016, 29, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.; Gholi, N.M. Long term use of flunixin meglumine and ketoprofen in Arabian horses and their digestive and cardiac injuries (biochemical, hematological and endoscopic findings). J. Anim. Vet. Adv. 2012, 11, 750–755. [Google Scholar] [CrossRef]
- Monreal, L.; Sabaté, D.; Segura, D.; Mayós, I.; Homedes, J. Lower gastric ulcerogenic effect of suxibuzone compared to phenylbutazone when administered orally to horses. Res. Vet. Sci. 2004, 76, 145–149. [Google Scholar] [CrossRef]
- Meschter, C.L.; Gilbert, M.; Krook, L.; Maylin, G.; Corradino, R. The Effects of Phenylbutazone on the Morphology and Prostaglandin Concentrations of the Pyloric Mucosa of the Equine Stomach. Vet. Pathol. 1990, 27, 244–253. [Google Scholar] [CrossRef] [Green Version]
- Ricord, M.; Andrews, F.M.; Yñiguez, F.J.M.; Keowen, M.; Garza, F., Jr.; Paul, L.; Chapman, A.; Banse, H. Impact of omeprazole on phenylbutazone-induced equine gastric ulcer syndrome. Equine Vet. Educ. 2020, 53, 356–363. [Google Scholar] [CrossRef]
- Bishop, R.; Kemper, A.; Wilkins, P.; McCoy, A. Effect of omeprazole and sucralfate on gastrointestinal injury in a fasting/NSAID model. Equine Vet. J. 2022, 54, 829–837. [Google Scholar] [CrossRef]
- Jacobs, C.; Schnabel, L.; McIlwraith, C.; Blikslager, A. Non-steroidal anti-inflammatory drugs in equine orthopaedics. Equine Vet. J. 2022, 54, 636–648. [Google Scholar] [CrossRef]
- Richardson, L.M.; Whitfield-Cargile, C.M.; Cohen, N.D.; Chamoun-Emanuelli, A.M.; Dockery, H.J. Effect of selective versus nonselective cyclooxygenase inhibitors on gastric ulceration scores and intestinal inflammation in horses. Vet. Surg. 2018, 47, 784–791. [Google Scholar] [CrossRef]
- Andrews, F.M.; Reinemeyer, C.R.; Longhofer, S.L. Effects of top-dress formulations of suxibuzone and phenylbutazone on development of gastric ulcers in horses. Vet. Ther. 2009, 10, 113–120. [Google Scholar]
- Marshall, B.; Warren, J. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1983, 36, 1273–1275. [Google Scholar]
- Paul, L.J.; Ericsson, A.C.; Andrews, F.M.; Keowen, M.L.; Morales Yniguez, F.; Garza, F., Jr.; Banse, H.E. Gastric microbiome in horses with and without equine glandular gastric disease. J. Vet. Intern. Med. 2021, 35, 2458–2464. [Google Scholar] [CrossRef]
- AbuElghait, D.A.E.; Mohamed, K.F.; Sheta, E.; AbdElkader, N.A.; Samir, A. Novel detection of Helicobacter species in gastric problems in Equine in Egypt. Syst. Rev. Pharm. 2020, 11, 553–557. [Google Scholar] [CrossRef]
- Abelardo, M.B.; Garcia, F.; Bermudez, V. Detection of helicobacter-like organisms in Thoroughbred horses from Venezuela. Braz. J. Vet. Pathol. 2010, 3, 52–55. [Google Scholar]
- Contreras, M.; Morales, A.; García-Amado, M.A.; De Vera, M.; Bermúdez, V.; Gueneau, P. Detection of Helicobacter-like DNA in the gastric mucosa of Thoroughbred horses. Lett. Appl. Microbiol. 2007, 45, 553–557. [Google Scholar] [CrossRef]
- Rezazadeh, F.; Pourebrahimi, N.; Ghotaslou, R.; Nasab, M.G.; Memar, M.Y. Frequency of endoscopic findings of equine squamous gastric disease (ESGD) in rural horses and its association with Helicobacter pylori virulence genes. Vet. Med. 2022, 67, 61–69. [Google Scholar] [CrossRef]
- Husted, L.; Jensen, T.K.; Olsen, S.N.; Mølbak, L. Examination of equine glandular stomach lesions for bacteria, including Helicobacter spp by fluorescence in situ hybridisation. BMC Microbiol. 2010, 10, 84. [Google Scholar] [CrossRef] [Green Version]
- Dong, H.J.; Ho, H.; Hwang, H.; Kim, Y.; Han, J.; Lee, I.; Cho, S. Diversity of the gastric microbiota in thoroughbred racehorses having gastric ulcer. J. Microbiol. Biotechnol. 2016, 26, 763–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, G.; den Bakker, H.; Burton, A.; Erb, H.; McDonough, S.; McDonough, P.; Parker, J.; Rosenthal, R.; Wiedmann, M.; Dowd, S.; et al. Equine stomachs harbor an abundant and diverse mucosal microbiota. Appl. Environ. Microbiol. 2012, 78, 2522–2532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martineau, H.; Thompson, H.; Taylor, D. Pathology of gastritis and gastric ulceration in the horse. Part 1: Range of lesions present in 21 mature individuals. Equine Vet. J. 2009, 41, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Voss, S.J.; McGuinness, D.H.; Weir, W.; Sutton, D.G.M. A study comparing the healthy and diseased equine glandular gastric microbiota sampled with sheathed transendoscopic cytology brushes. J. Equine Vet. Sci. 2022, 116, 104002. [Google Scholar] [CrossRef]
- Van Erck-Westergren, E.; ter Woort, F. Diet-Induced Changes in Gastric and Faecal Microbiota in Horses: Association with Gastric Ulcer Healing. Equine Vet. J. 2019, 51, 21. [Google Scholar] [CrossRef] [Green Version]
- Paul, L.J.; Ericsson, A.C.; Andrews, F.M.; McAdams, Z.; Keowen, M.L.; St Blanc, M.P.; Banse, H.E. Dietary and management factors influence the equine gastric microbiome. J. Am. Vet. Med. Assoc. 2022, 260, S111–S120. [Google Scholar] [CrossRef]
- Sykes, B.W.; Sykes, K.M.; Hallowell, G.D. Administration of trimethoprim-sulphadimidine does not improve healing of glandular gastric ulceration in horses receiving omeprazole: A randomised, blinded, clinical study. BMC Vet. Res. 2014, 10, 180. [Google Scholar] [CrossRef] [Green Version]
- Rendle, D.; Bowen, M.; Brazil, T.; Conwell, R.; Hallowell, G.; Hepburn, R.; Hewetson, M.; Sykes, B. Recommendations for the management of equine glandular gastric disease. UK Vet Equine 2018, 2, 2–11. [Google Scholar] [CrossRef] [Green Version]
- Wise, J.C.; Wilkes, E.J.A.; Raidal, S.L.; Xie, G.; Crosby, D.E.; Hale, J.N.; Hughes, K.J. Interobserver and intraobserver reliability for 2 grading systems for gastric ulcer syndrome in horses. J. Vet. Intern. Med. 2021, 35, 571–579. [Google Scholar] [CrossRef]
- Tallon, R.; Hewetson, M. Inter-observer variability of two grading systems for equine glandular gastric disease. Equine Vet. J. 2021, 53, 495–502. [Google Scholar] [CrossRef]
- Pratt, S.; Bowen, I.; Hallowell, G.; Shipman, E.; Redpath, A. Assessment of agreement using the equine glandular gastric disease grading system in 84 cases. Vet. Med. Sci. 2022, 8, 1472–1477. [Google Scholar] [CrossRef]
- Deniau, V.; Ouachée-Flé, E.; Rossignol, F. Pyloric Stenosis In Adult Horses: Retrospective Study Of 10 Cases. Equine Vet. Educ. 2017, 29, 29. [Google Scholar] [CrossRef]
- Scheidemann, W.; Schubert, S.; Kretschmer, I.; Recknagel, S.; Snyder, A.; Schusser, G. Gastric and duodenal polyps in horses. Equine Vet. Educ. 2021, 33, 35. [Google Scholar] [CrossRef]
- Fritsche, B.; Hegger, A.; Harland, M. Der klinische Fall: Therapie eines hyperplastischen Polypen im Magen eines Pferdes mit Helicobacter-spp.-Besiedelung. Pferdespiegel 2022, 25, 187–192. [Google Scholar] [CrossRef]
- Pellegrini, F.L. Results of a large-scale necroscopic study of equine colonic ulcers. J. Equine Vet. Sci. 2005, 25, 113–117. [Google Scholar] [CrossRef]
- Sykes, B.; Jokisalo, J.; Hallowell, G. Evaluation of a commercial faecal blood test for the diagnosis of gastric ulceration in Thoroughbred racehorses: A preliminary report. In Proceedings of the 11th International Equine Colic Research Symposium, Dublin, Ireland, 7–10 July 2014. [Google Scholar]
- Andrews, F.M.; Camacho-Luna, P.; Loftin, P.G.; Gaymon, G.; Garza, F.; Keowen, M.L.; Kearney, M.T. Effect of a pelleted supplement fed during and after omeprazole treatment on nonglandular gastric ulcer scores and gastric juice pH in horses. Equine Vet. Educ. 2016, 28, 196–202. [Google Scholar] [CrossRef]
- Ramey, D.; Murrell, J.; Fischer, T.; Brauer, T.; Klohnen, A.; Lee, M. Fecal Blood Hemoglobin and Albumin Test Does Not Diagnose Gastric Ulceration in the Horse. In Proceedings of the American Association of Orlando, Orlando, FL, USA, 7–10 May 2018. [Google Scholar]
- Contreras-Aguilar, M.D.; Rubio, C.P.; González-Arostegui, L.G.; Martín-Cuervo, M.; Cerón, J.J.; Ayala, I.; Henriksen, I.M.H.; Jacobsen, S.; Hansen, S. Changes in Oxidative Status Biomarkers in Saliva and Serum in the Equine Gastric Ulcer Syndrome and Colic of Intestinal Aetiology: A Pilot Study. Animals 2022, 12, 667. [Google Scholar] [CrossRef]
- Spanton, J.A.; Smith, L.; Mair, T.S. Is Serum Amyloid A elevated in horses with equine gastric ulcer syndrome? Equine Vet. Educ. 2020, 32, 16–19. [Google Scholar] [CrossRef]
- Shawaf, T.; El-Deeb, W.M.; Elgioushy, M. The Contribution of Specific and Nonspecific Biomarkers in Diagnosis of Equine Gastric Ulcer Syndrome (EGUS) Under Field Condition. J. Equine Vet. Sci. 2020, 84, 102853. [Google Scholar] [CrossRef]
- Tesena, P.; Yingchutrakul, Y.; Roytrakul, S.; Taylor, J.; Angkanaporn, K.; Wongtawan, T. Searching for serum protein markers of equine squamous gastric disease using gel electrophoresis and mass spectrometry. Equine Vet. J. 2019, 51, 581–586. [Google Scholar] [CrossRef]
- O’Conner, M.S.; Steiner, J.M.; Roussel, A.J.; Williams, D.A.; Meddings, J.B.; Pipers, F.; Cohen, N.D. Evaluation of urine sucrose concentration for detection of gastric ulcers in horses. Am. J. Vet. Res. 2004, 65, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Hewetson, M.; Cohen, N.D.; Love, S.; Buddington, R.K.; Holmes, W.; Innocent, G.T.; Roussel, A.J. Sucrose concentration in blood: A new method for assessment of gastric permeability in horses with gastric ulceration. J. Vet. Intern. Med. 2006, 20, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Hewetson, M.; Venner, M.; Volquardsen, J.; Sykes, B.W.; Hallowell, G.D.; Vervuert, I.; Fosgate, G.T.; Tulamo, R.-M. Diagnostic accuracy of blood sucrose as a screening test for equine gastric ulcer syndrome (EGUS) in weanling foals. Acta Vet. Scand. 2018, 60, 24. [Google Scholar] [CrossRef] [Green Version]
- Westermann, C.; van den Wollenberg, L.; Everts, H.; van der Kolk, J.; Counotte, G.; van Doorn, D. Evaluation of a Blood Sucrose Test for the Assessment of Gastric Ulcers in Warmblood Horses Aimed at Field Conditions. In Proceedings of the European College of Equine Internal Medicine Congress, Helsinki, Finland, 11 September 2016. [Google Scholar]
- Andrews, F.; Bernard, W.D.B.; Cohen, N.; Divers, T.; MacAllister, C.; McGladdery, A.; Merritt, A.; Murray, M.; Orsini, J.; Snider, J.; et al. Recommendations for the diagnosis and treatment of equine gastric ulcer syndrome (EGUS): The Equine Gastric Ulcer Council. Equine Vet. Educ. 1999, 11, 262–272. [Google Scholar] [CrossRef]
- Sykes, B.W.; Sykes, K.M.; Hallowell, G.D. A comparison between pre- and post exercise administration of omeprazole in the treatment of equine gastric ulcer syndrome: A blinded, randomised, clinical trial. Equine Vet. J. 2014, 46, 422–426. [Google Scholar] [CrossRef]
- Bush, J.; van den Boom, R.; Franklin, S. Comparison of aloe vera and omeprazole in the treatment of equine gastric ulcer syndrome. Equine Vet. J. 2018, 50, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Murray, M.J.; Haven, M.L.; Eichorn, E.S.; Zhang, D.; Eagleson, J.; Hickey, G.J. Effects of omeprazole on healing of naturally-occurring gastric ulcers in Thoroughbred racehorses. Equine Vet. J. 1997, 29, 425–429. [Google Scholar] [CrossRef]
- Sykes, B.W.; Underwood, C.; Greer, R.; McGowan, C.M.; Mills, P.C. Pharmacokinetics and bioequivalence testing of five commercial formulations of omeprazole in the horse. J. Vet. Pharmacol. 2016, 39, 78–83. [Google Scholar] [CrossRef]
- Raidal, S.L.; Andrews, F.M.; Nielsen, S.G.; Trope, G. Pharmacokinetic and pharmacodynamic effects of two omeprazole formulations on stomach pH and gastric ulcer scores. Equine Vet. J. 2017, 49, 802–809. [Google Scholar] [CrossRef] [Green Version]
- Birkmann, K.; Junge, H.K.; Maischberger, E.; Wehrli Eser, M.; Schwarzwald, C.C. Efficacy of omeprazole powder paste or enteric-coated formulation in healing of gastric ulcers in horses. J. Vet. Intern. Med. 2014, 28, 925–933. [Google Scholar] [CrossRef] [Green Version]
- Sykes, B.; Underwood, C.; McGowan, C.; Mills, P. Pharmacokinetics of intravenous, plain oral and enteric-coated oral omeprazole in the horse. J. Vet. Pharmacol. 2015, 38, 130–136. [Google Scholar] [CrossRef]
- Huttunen, K.; Raunio, H.; Rautio, J. Prodrugs—from serendipity to rational design. Pharmacol. Rev. 2011, 63, 750–771. [Google Scholar] [CrossRef] [Green Version]
- Sykes, B.; Underwood, C.; Greer, R.; McGowan, C.; Mills, P. The effects of dose and diet on the pharmacodynamics of omeprazole in the horse. Equine Vet. J. 2017, 49, 525–531. [Google Scholar] [CrossRef]
- Husted, L.; Sanchez, L.C.; Baptiste, K.E.; Olsen, S.N. Effect of a feed/fast protocol on pH in the proximal equine stomach. Equine Vet. J. 2009, 41, 658–662. [Google Scholar] [CrossRef]
- Merritt, A.; Sanchez, L.; Burrow, J.; Church, M.; Ludzia, S. Effect of GastroGard and three compounded oral omeprazole preparations on 24 h intragastric pH in gastrically cannulated mature horses. Equine Vet. J. 2003, 37, 691–695. [Google Scholar] [CrossRef]
- Rendle, D.; Gosling, L.; Platt, A.; Duff, A. Efficacy of Long-Acting Injectable Omeprazole (LAIOMEP) in the Management of Equine Glandular Gastric Disease (EGGD) and Equine Squamous Gastric Disease (ESGD). Equine Vet. J. 2018, 50, 14. [Google Scholar] [CrossRef] [Green Version]
- Lehman, M.L.; Bass, L.; Gustafson, D.L.; Rao, S.; O’Fallon, E.S. Clinical efficacy, safety and pharmacokinetics of a novel long-acting intramuscular omeprazole in performance horses with gastric ulcers. Equine Vet. Educ. 2021, 34, 573–580. [Google Scholar] [CrossRef]
- Kranenburg, L.; Scheepbouwer, J.; van den Boom, R. A retrospective study on the effect of combined sucralfate and omeprazole therapy compared with omeprazole monotherapy for equine glandular gastric disease. In Proceedings of the 13th Annual European College of Equine Internal Medicine Congress, Online, 20 November 2020. [Google Scholar]
- Martínez, J.R.; Zuluaga, A.M.; Silveira, G.E. Effects of corn oil on the gastric mucosa of horses with induced ulcer. Rev. Colomb. Cienc. Pecu. 2016, 29, 138–148. [Google Scholar] [CrossRef] [Green Version]
- Sykes, B.W.; Underwood, C.; Mills, P.C. The effects of dose and diet on the pharmacodynamics of esomeprazole in the horse. Equine Vet. J. 2017, 49, 637–642. [Google Scholar] [CrossRef]
- Rendle, D. Oral Esomeprazole As A Treatment For Equine Gastric Ulcer Syndrome Refractory To Oral Omeprazole. Equine Vet. J. 2017, 49, 25–26. [Google Scholar] [CrossRef] [Green Version]
- Sundra, T. Esomeprazole in the treatment of equine glandular gastric disease. UK Vet. Equine 2021, 5, 216–219. [Google Scholar] [CrossRef]
- Pereira, M.C.; Levy, F.L.; Valadão, C.A.A.; Ferraz, G.C.; Queiroz–Neto, A. Preliminary Study of the Gastric Acidity in Thoroughbred Horses at Rest after Enteral Administration of Esomeprazole Magnesium (Nexium). J. Equine Vet. Sci. 2009, 29, 791–794. [Google Scholar] [CrossRef]
- Murray, M.; Grodinsky, C. The effects of famotidine, ranitidine and magnesium hydroxide/aluminium hydroxide on gastric fluid pH in adult horses. Equine Vet. J. 1992, 24, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Lester, G.; Smith, R.; Robertson, I. Effects of treatment with omeprazole or ranitidine on gastric squamous ulceration in racing Thoroughbreds. J. Am. Vet. Med. Assoc. 2005, 227, 1636–1639. [Google Scholar] [CrossRef]
- Sangiah, S.; MacAllister, C.; Amouzadeh, H. Effects of misoprostol and omeprazole on basal gastric pH and free acid content in horses. Res. Vet. Sci. 1989, 47, 350–354. [Google Scholar] [CrossRef]
- Martin, E.; Till, R.; Sheats, M.; Jones, S. Misoprostol Inhibits Equine Neutrophil Adhesion, Migration, and Respiratory Burst in an In Vitro Model of Inflammation. Front. Vet. Sci. 2017, 4, 159. [Google Scholar] [CrossRef] [Green Version]
- Martin, E.; Messenger, K.; Sheats, M.; Jones, S. Misoprostol Inhibits Lipopolysaccharide-Induced Pro-inflammatory Cytokine Production by Equine Leukocytes. Front. Vet. Sci. 2017, 4, 160. [Google Scholar] [CrossRef] [Green Version]
- Galvin, N.; Dillon, H.; McGovern, F. Right dorsal colitis in the horse: Minireview and reports on three cases in Ireland. Ir. Vet. J. 2004, 57, 467. [Google Scholar] [CrossRef] [Green Version]
- Davis, J. Nonsteroidal anti-inflammatory drug associated right dorsal colitis in the horse. Equine Vet. Educ. 2017, 29, 104–113. [Google Scholar] [CrossRef]
- Varley, G.; Bowen, I.; Habershon-Butcher, J.; Nicholls, V.; Hallowell, G. Misoprostol is superior to combined omeprazole–sucralfate for the treatment of equine gastric glandular disease. Equine Vet. J. 2020, 51, 575–580. [Google Scholar] [CrossRef]
- Blum, J.; Winikoff, B.; Gemzell-Danielsson, K.; Ho, P.; Schiavon, R.; Weeks, A. Treatment of incomplete abortion and miscarriage with misoprostol. Int. J. Gynecol. Obstet. 2007, 99, S186–S189. [Google Scholar] [CrossRef]
- Reimer, C.; Søndergaard, B.; Hilsted, L.; Bytzer, P. Proton-pump inhibitor therapy induces acid-related symptoms in healthy volunteers after withdrawal of therapy. Gastroenterology 2009, 137, 80–87.e81. [Google Scholar] [CrossRef]
- Niklasson, A.; Lindström, L.; Simrén, M.; Lindberg, G.; Björnsson, E. Dyspeptic symptom development after discontinuation of a proton pump inhibitor: A double-blind placebo-controlled trial. Am. J. Gastroenterol. 2010, 105, 1531–1537. [Google Scholar] [CrossRef]
- Haastrup, P.; Thompson, W.; Søndergaard, J.; Jarbøl, D. Side Effects of Long-Term Proton Pump Inhibitor Use: A Review. Basic Clin. Pharmacol. Toxicol. 2018, 123, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Sheen, E.; Triadafilopoulos, G. Adverse effects of long-term proton pump inhibitor therapy. Dig. Dis. Sci. 2011, 56, 931–950. [Google Scholar] [CrossRef]
- Freedberg, D.; Haynes, K.; Denburg, M.; Zemel, B.; Leonard, M.; Abrams, J.; Yang, Y.-X. Use of proton pump inhibitors is associated with fractures in young adults: A population-based study. Osteoporos. Int. 2015, 26, 2501–2507. [Google Scholar] [CrossRef] [Green Version]
- Malchodi, L.; Wagner, K.; Susi, A.; Gorman, G.; Hisle-Gorman, E. Early Acid Suppression Therapy Exposure and Fracture in Young Children. Pediatrics 2019, 144, e20182625. [Google Scholar] [CrossRef]
- Clark, B.; Steel, C.; Shan, R.; Vokes, J.; Sykes, B.; Gedye, K.; Lovett, A. Evaluation of the effects of medium-term (57-day) omeprazole administration and of omeprazole discontinuation on serum gastrin and serum chromogranin A levels in the horse. 2023. [Google Scholar]
- Furr, M.; Cohen, N.D.; Axon, J.E.; Sanchez, L.C.; Pantaleon, L.; Haggett, E.; Campbell, R.; Tennent-Brown, B. Treatment with histamine-type 2 receptor antagonists and omeprazole increase the risk of diarrhoea in neonatal foals treated in intensive care units. Equine Vet. J. 2012, 44, 80–86. [Google Scholar] [CrossRef]
- Flood, J.; Stewart, A. Non-Steroidal Anti-Inflammatory Drugs and Associated Toxicities in Horses. Animals 2022, 12, 2939. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Gaier, A.; Enomoto, H.; Ishii, P.; Pilla, R.; Price, J.; Suchodolski, J.; Steiner, J.; Papich, M.; Messenger, K.; et al. The effect of combined carprofen and omeprazole administration on gastrointestinal permeability and inflammation in dogs. J. Vet. Intern. Med. 2020, 34, 1886–1893. [Google Scholar] [CrossRef] [PubMed]
- Cerri, S.; Taminiau, B.; de Lusancay, A.H.; Lecoq, L.; Amory, H.; Daube, G.; Cesarini, C. Effect of oral administration of omeprazole on the microbiota of the gastric glandular mucosa and feces of healthy horses. J. Vet. Intern. Med. 2020, 34, 2727–2737. [Google Scholar] [CrossRef] [PubMed]
- Tyma, J.F.; Epstein, K.L.; Whitfield-Cargile, C.M.; Cohen, N.D.; Giguère, S. Investigation of effects of omeprazole on the fecal and gastric microbiota of healthy adult horses. Am. J. Vet. Res. 2019, 80, 79–86. [Google Scholar] [CrossRef]
- Sykes, B. A free ride: Is long-term omeprazole therapy safe and effective? Equine Vet. Educ. 2021, 33, 556–560. [Google Scholar] [CrossRef]
- Pagan, J.D.; Petroski-Rose, L.; Mann, A.; Hauss, A. Omeprazole Reduces Calcium Digestibility in Thoroughbred Horses. J. Equine Vet. Sci. 2020, 86, 102851. [Google Scholar] [CrossRef]
- Caston, S.S.; Fredericks, D.C.; Kersh, K.D.; Wang, C. Short-Term Omeprazole Use Does Not Affect Serum Calcium Concentrations and Bone Density in Horses. J. Equine Vet. Sci. 2015, 35, 714–723. [Google Scholar] [CrossRef]
- Helgadóttir, H.; Lund, S.H.; Gizurarson, S.; Waldum, H.; Björnsson, E.S. Pharmacokinetics of single and repeated oral doses of esomeprazole and gastrin elevation in healthy males and females. Scand. J. Gastroenterol. 2021, 56, 128–136. [Google Scholar] [CrossRef]
- Brenna, E.; Waldum, H. Trophic effect of gastrin on the enterochromaffin like cells of the rat stomach: Establishment of a dose response relationship. Gut 1992, 33, 1303–1306. [Google Scholar] [CrossRef] [Green Version]
- Helgadottir, H.; Bjornsson, E.S. Problems associated with deprescribing of proton pump inhibitors. Int. J. Mol. Sci. 2019, 20, 5469. [Google Scholar] [CrossRef] [Green Version]
- Sanduleanu, S.; De Bruïne, A.; Stridsberg, M.; Jonkers, D.; Biemond, I.; Hameeteman, W.; Lundqvist, G.; Stockbrügger, R.W. Serum chromogranin A as a screening test for gastric enterochromaffin-like cell hyperplasia during acid-suppressive therapy. Eur. J. Clin. Investig. 2001, 31, 802–811. [Google Scholar] [CrossRef]
- Ellis, A.D.; Redgate, S.; Zinchenko, S.; Owen, H.; Barfoot, C.; Harris, P. The effect of presenting forage in multi-layered haynets and at multiple sites on night time budgets of stabled horses. Appl. Anim. Behav. Sci. 2015, 171, 108–116. [Google Scholar] [CrossRef] [Green Version]
- Ellis, A.D.; Fell, M.; Luck, K.; Gill, L.; Owen, H.; Briars, H.; Barfoot, C.; Harris, P. Effect of forage presentation on feed intake behaviour in stabled horses. Appl. Anim. Behav. Sci. 2015, 165, 88–94. [Google Scholar] [CrossRef]
- Luthersson, N.; Bolger, C.; Fores, P.; Barfoot, C.; Nelson, S.; Parkin, T.; Harris, P. Effect of Changing Diet on Gastric Ulceration in Exercising Horses and Ponies After Cessation of Omeprazole Treatment. J. Equine Vet. Sci. 2019, 83, 102742. [Google Scholar] [CrossRef]
- Böhm, S.; Mitterer, T.; Iben, C. The impact of feeding a high-fibre and high-fat concentrated diet on the recovery of horses suffering from gastric ulcers. Pferdeheilkunde 2018, 34, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Potter, G.; Webb, S.; Evans, J.; Webb, G. Digestible energy requirements for work and maintenance of horses fed conventional and fat-supplemented diets. J. Equine Vet. Sci. 1990, 10, 214–218. [Google Scholar] [CrossRef]
- Cargile, J.; Burrow, J.; Kim, I.; Cohen, N.; Merritt, A. Effect of Dietary Corn Oil Supplementation on Equine Gastric Fluid Acid, Sodium, and Prostaglandin E2 Content before and during Pentagastrin Infusion. J. Vet. Intern. Med. 2004, 18, 545–549. [Google Scholar] [CrossRef]
- Frank, N.; Andrews, F.M.; Elliott, S.B.; Lew, J. Effects of dietary oils on the development of gastric ulcers in mares. Am. J. Vet. Res. 2005, 66, 2006–2011. [Google Scholar] [CrossRef]
- Calder, P.C. Polyunsaturated fatty acids, inflammatory processes and inflammatory bowel diseases. Mol. Nutr. Food Res. 2008, 52, 885–897. [Google Scholar] [CrossRef]
- Calder, P.; Grimble, R. Polyunsaturated fatty acids, inflammation and immunity. Eur. J. Clin. Nutr. 2002, 56, S14–S19. [Google Scholar] [CrossRef] [Green Version]
- Burdge, G.C.; Wootton, S.A. Conversion of α-linolenic acid to eicosapentaenoic, docosapentaenoic and docosahexaenoic acids in young women. Br. J. Nutr. 2002, 88, 411–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burdge, G.; Jones, A.; Wootton, S. Eicosapentaenoic and docosapentaenoic acids are the principal products of a-linolenic acid metabolism in young men. Br. J. Nutr. 2002, 88, 355–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagan, J.D.; Hauss, A.A.; Pagan, E.C.; Simons, J.L.; Waldridge, B.M. Long-chain polyunsaturated fatty acid supplementation increases levels in red blood cells and reduces the prevalence and severity of squamous gastric ulcers in exercised Thoroughbreds. J. Am. Vet. Med. Assoc. 2022, 260, S121–S128. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, F.; Zucca, E.; Croci, C.; Di Fabio, V.; Ferro, E. Treatment of gastric ulceration in 10 standardbred racehorses with a pectin-lecithin complex. Vet. Rec. 2003, 152, 679–681. [Google Scholar] [CrossRef]
- Venner, M.; Lauffs, S.; Deegen, E. Treatment of gastric lesions in horses with pectin-lecithin complex. Equine Vet. J. 1999, 31, 91–96. [Google Scholar] [CrossRef]
- Sykes, B.W.; Sykes, K.M.; Hallowell, G.D. Efficacy of a Combination of Apolectol, Live Yeast (Saccharomyces cerevisiae [CNCM I-1077]), and Magnesium Hydroxide in the Management of Equine Gastric Ulcer Syndrome in Thoroughbred Racehorses: A Blinded, Randomized, Placebo-Controlled Clinical Trial. J. Equine Vet. Sci. 2014, 34, 1274–1278. [Google Scholar] [CrossRef]
- Shan, R.; Steel, C.; Sykes, B. Evaluation of two Recommended Withholding Periods for omeprazole and the use of a commercial nutraceutical supplement on Equine Squamous Gastric Disease in the horse. 2023. [Google Scholar]
- Julliand, S.; Martin, A.; Julliand, V. Effect of live yeast supplementation on gastric ecosystem in horses fed a high-starch diet. Livest. Sci. 2018, 215, 25–29. [Google Scholar] [CrossRef]
- Sykes, B.W.; Sykes, K.M.; Hallowell, G.D. Efficacy of a Combination of a Unique Pectin-Lecithin Complex (Apolectol®), Live Yeast and Magnesium Hydroxide in the Prevention of EGUS and Faecal Acidosis in Thoroughbred Racehorses: A Randomised, Blinded, Placebo Controlled Clinical Trial. Equine Vet. J. 2013, 45, 13. [Google Scholar] [CrossRef]
- Agazzi, A.; Invernizzi, G.; Ferroni, M.; Fanelli, A.; Savoini, G. Effect of live yeast (Saccharomyces cerevisiae) administration on apparent digestibility of horses. Ital. J. Anim. Sci. 2009, 6, 685–687. [Google Scholar] [CrossRef]
- Ahmadnejad, M.; Jalilzadeh-Amin, G.; Sykes, B. Prophylactic effects of Glycyrrhiza glabra root extract on phenylbutazone-induced Equine Glandular Gastric Disease (EGGD). J. Equine Vet. Sci. 2022, 118, 104088. [Google Scholar] [CrossRef]
- Stucchi, L.; Zucca, E.; Serra, A.; Stancari, G.; Ceriotti, S.; Conturba, B.; Ferro, E.; Ferrucci, F. Efficacy of the administration of a natural feed supplement in the management of equine gastric ulcer syndrome in 7 sport horses: A field trial. Am. J. Anim. Vet. Sci. 2017, 12, 104–110. [Google Scholar] [CrossRef] [Green Version]
- Raidal, S.L.; Hughes, K.J. Effect of a novel fermented soy product on gastric ulcer scores in horses. J. Appl. Anim. Nutr. 2020, 8, 105–113. [Google Scholar] [CrossRef]
- Sasaki, N.; Nishi, Y.; Fujiwara, Y.; Takeyama, T.; Kumagai, H.; Senarathna, S.; Ushiya, S.; Tokuyama, T.; Tokuyama, T.; Tokuyama, T.; et al. Effect of a novel rice fermented extract on gastric ulcers in horses. J. Equine Sci. 2021, 32, 27–30. [Google Scholar] [CrossRef]
- Huff, N.K.; Auer, A.D.; Garza, F.; Keowen, M.L.; Kearney, M.T.; McMullin, R.B.; Andrews, F.M. Effect of Sea Buckthorn Berries and Pulp in a Liquid Emulsion on Gastric Ulcer Scores and Gastric Juice pH in Horses. J. Vet. Intern. Med. 2012, 26, 1186–1191. [Google Scholar] [CrossRef] [Green Version]
- Slovis, N. Polysaccharide Treatment Reduces Gastric Ulceration in Active Horses. J. Equine Vet. Sci. 2017, 50, 116–120. [Google Scholar] [CrossRef]
- Hellings, I.R.; Larsen, S. ImproWin® in the treatment of gastric ulceration of the squamous mucosa in trotting racehorses. Acta Vet. Scand. 2014, 56, 13. [Google Scholar] [CrossRef] [Green Version]
- McClure, S.R.; Campbell, J.; Polo, J.; Lognion, A. The Effect of Serum-Based Bioactive Proteins for the Prevention of Squamous Gastric Ulcers in Horses. J. Equine Vet. Sci. 2016, 43, 32–38. [Google Scholar] [CrossRef]
- St. Blanc, M.; Banse, H.; Retif, M.; Arana-Valencia, N.; Keowen, M.L.; Garza, F.; Liu, C.C.; Gray, L.F.; Andrews, F.M. Effects of supplements containing turmeric and devil’s claw on equine gastric ulcer scores and gastric juice pH. Equine Vet. Educ. 2020, 34, 241–247. [Google Scholar] [CrossRef]
- Munsterman, A.S.; Dias Moreira, A.S.; Marqués, F.J. Evaluation of a Chinese herbal supplement on equine squamous gastric disease and gastric fluid pH in mares. J. Vet. Intern. Med. 2019, 33, 2280–2285. [Google Scholar] [CrossRef] [Green Version]
- Mason, L.V.; Moroney, J.R.; Mason, R.J. Prophylactic therapy with omeprazole for prevention of equine gastric ulcer syndrome (EGUS) in horses in active training: A meta-analysis. Equine Vet. J. 2019, 51, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Di Salvo, A.; Busechian, S.; Zappulla, F.; Marchesi, M.C.; Pieramati, C.; Orvieto, S.; Boveri, M.; Predieri, P.G.; Rueca, F.; Della Rocca, G. Pharmacokinetics and tolerability of a new formulation of omeprazole in the horse. J. Vet. Pharmacol. Ther. 2017, 40, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Kerbyson, N.C.; Knottenbelt, D.K.; Carslake, H.B.; Conwell, R.C.; Sutton, D.G.M.; Parkin, T.D.H. A Comparison Between Omeprazole and a Dietary Supplement for the Management of Squamous Gastric Ulceration in Horses. J. Equine Vet. Sci. 2016, 40, 94–101. [Google Scholar] [CrossRef] [Green Version]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vokes, J.; Lovett, A.; Sykes, B. Equine Gastric Ulcer Syndrome: An Update on Current Knowledge. Animals 2023, 13, 1261. https://doi.org/10.3390/ani13071261
Vokes J, Lovett A, Sykes B. Equine Gastric Ulcer Syndrome: An Update on Current Knowledge. Animals. 2023; 13(7):1261. https://doi.org/10.3390/ani13071261
Chicago/Turabian StyleVokes, Jessica, Amy Lovett, and Benjamin Sykes. 2023. "Equine Gastric Ulcer Syndrome: An Update on Current Knowledge" Animals 13, no. 7: 1261. https://doi.org/10.3390/ani13071261
APA StyleVokes, J., Lovett, A., & Sykes, B. (2023). Equine Gastric Ulcer Syndrome: An Update on Current Knowledge. Animals, 13(7), 1261. https://doi.org/10.3390/ani13071261