
Dual-Task Performance, Balance and Aerobic Capacity as Predictors of Falls in Older Adults with Cardiovascular Disease: A Comparative Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
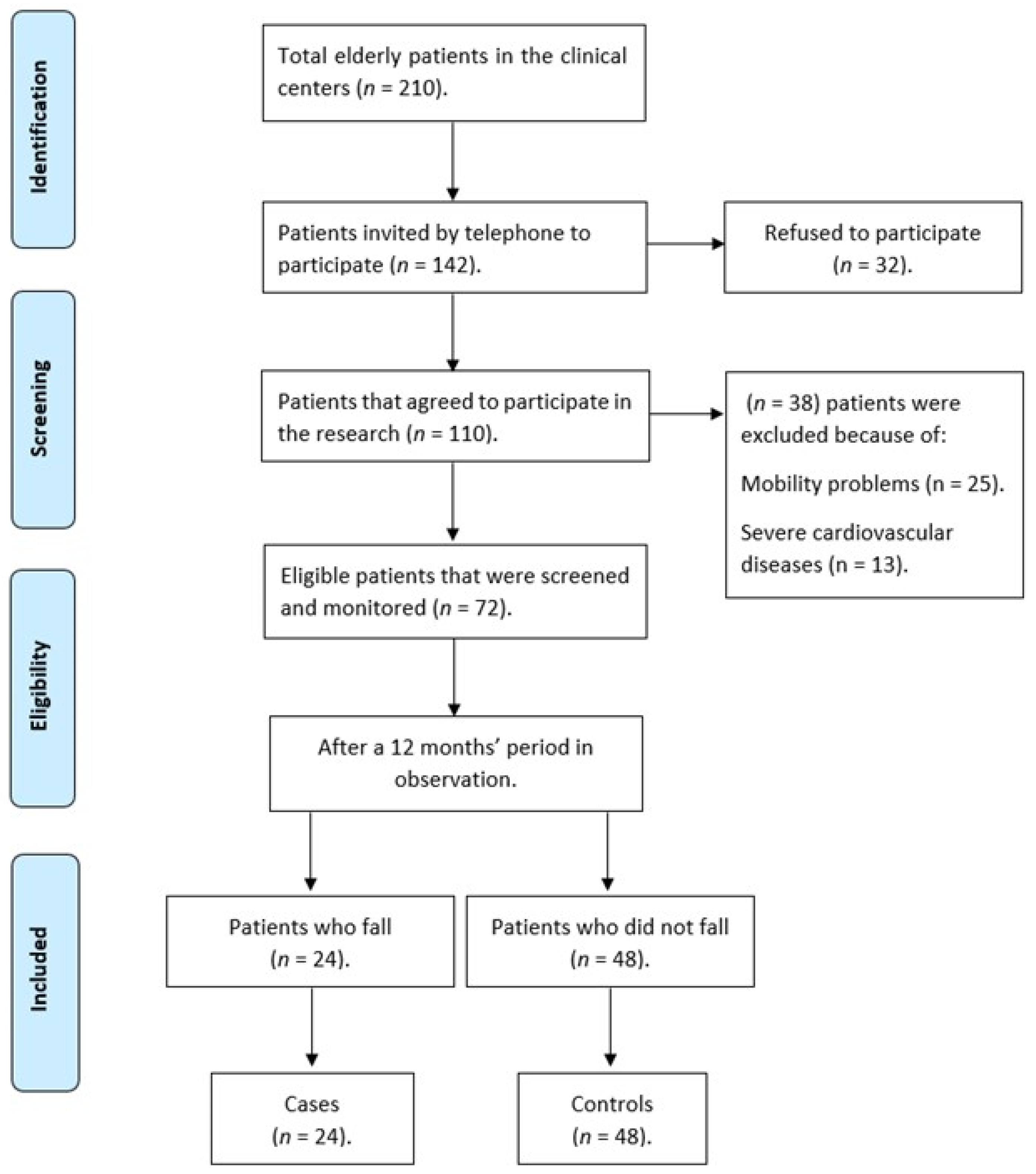
2.1. Study Design, Setting and Participants
2.2. Procedures
2.3. Statistical Analysis
3. Results
3.1. A Comparative Design Based on a Nested Case-Control by Density Approach
3.2. Descriptive Analysis
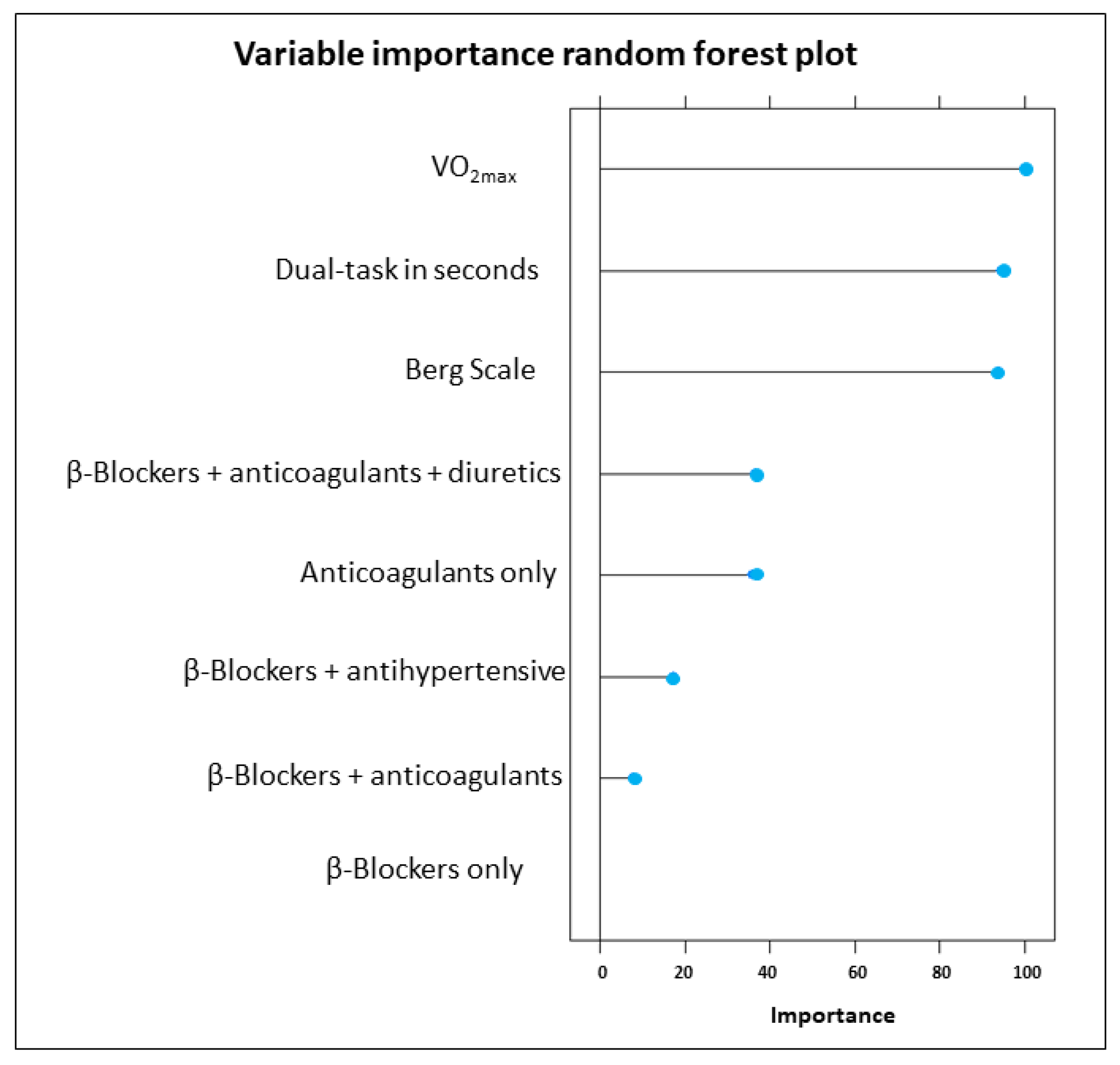
3.3. Machine Learning Analyses
3.4. Odds Ratio Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations Population Division. World Population Aging 2019 (Highlights); (ST/ESA/SER. A/430); United Nations: Vienna, Austria, 2019. [Google Scholar]
- World Health Organization. Decade of Healthy Ageing: Baseline Report; WHO: Geneva, Switzerland, 2020.
- Beard, J.R.; Jotheeswaran, A.T.; Cesari, M.; Araujo de Carvalho, I. The structure and predictive value of intrinsic capacity in a longitudinal study of ageing. BMJ Open 2019, 9, e026119. [Google Scholar] [CrossRef] [Green Version]
- James, S.L.; Lucchesi, L.R.; Bisignano, C.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Henry, N.J.; Krohn, K.J.; Liu, Z.; et al. The global burden of falls: Global, regional and national estimates of morbidity and mortality from the Global Burden of Disease Study 2017. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 2020, 26, i3–i11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. International comparison of cost of falls in older adults living in the community: A systematic review. Osteoporos. Int. 2010, 21, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.M.; Kamkar, N.; Pieruccini-Faria, F.; Osman, A.; Sarquis-Adamson, Y.; Close, J.; Hogan, D.B.; Hunter, S.W.; Kenny, R.A.; Lipsitz, L.A.; et al. Evaluation of Clinical Practice Guidelines on Fall Prevention and Management for Older Adults: A Systematic Review. JAMA Netw. Open 2021, 4, e2138911. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Report on Falls Prevention in Older Age; World Health Organization: Geneva, Switzerland, 2008.
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, Cd012424. [Google Scholar] [CrossRef]
- Jansen, S.; Bhangu, J.; de Rooij, S.; Daams, J.; Kenny, R.A.; van der Velde, N. The Association of Cardiovascular Disorders and Falls: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 193–199. [Google Scholar] [CrossRef]
- Rivera-Chávez, J.G.; Torres-Gutiérrez, J.L.; Regalado-Villalobos, A.; Moreno-Cervantes, C.A.; Luna-Torres, S. Association between falls and cardiovascular diseases in the geriatric population. Arch. Cardiol. Mex. 2021, 91, 66–72. [Google Scholar] [CrossRef]
- Denfeld, Q.E.; Turrise, S.; MacLaughlin, E.J.; Chang, P.S.; Clair, W.K.; Lewis, E.F.; Forman, D.E.; Goodlin, S.J. Preventing and Managing Falls in Adults with Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e000108. [Google Scholar] [CrossRef]
- Huang, A.R.; Mallet, L.; Rochefort, C.M.; Eguale, T.; Buckeridge, D.L.; Tamblyn, R. Medication-related falls in the elderly: Causative factors and preventive strategies. Drugs Aging 2012, 29, 359–376. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Falls in Older People: Assessing Risk and Prevention; NICE Clinical Guideline; NICE: Sutton-in-Ashfield, UK, 2013; Volume 161, p. 33. [Google Scholar]
- Ferreira, J.V.; Araujo, N.B.d.; Oliveira, F.d.; Plácido, J.; Anna, P.S.; Monteiro-Junior, R.S.; Marinho, V.; Laks, J.; Deslandes, A. Dual task in healthy elderly, depressive and Alzheimer s disease patients. J. Bras. Psiquiatr. 2019, 68, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Plácido, J.; Ferreira, J.V.; Araújo, J.; Silva, F.O.; Ferreira, R.B.; Guimarães, C.; de Carvalho, A.N.; Laks, J.; Deslandes, A.C. Beyond the Mini-Mental State Examination: The Use of Physical and Spatial Navigation Tests to Help to Screen for Mild Cognitive Impairment and Alzheimer’s Disease. J. Alzheimer’s Dis. 2021, 81, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Hollands, K.L.; Agnihotri, D.; Tyson, S.F. Effects of dual task on turning ability in stroke survivors and older adults. Gait Posture 2014, 40, 564–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Cai, Y.; Zhao, Y.; Gao, X.; Peng, D.; Zhang, H.; Deng, W.; Fu, W.; Qin, N.; Chang, R.; et al. The Complexity of Blood Pressure Fluctuation Mediated the Effects of Hypertension on Walking Speed in Older Adults. Front. Aging Neurosci. 2021, 13, 640942. [Google Scholar] [CrossRef]
- Baek, C.Y.; Chang, W.N.; Park, B.Y.; Lee, K.B.; Kang, K.Y.; Choi, M.R. Effects of Dual-Task Gait Treadmill Training on Gait Ability, Dual-Task Interference, and Fall Efficacy in People With Stroke: A Randomized Controlled Trial. Phys. Ther. 2021, 101, pzab067. [Google Scholar] [CrossRef]
- Pang, M.Y.C.; Yang, L.; Ouyang, H.; Lam, F.M.H.; Huang, M.; Jehu, D.A. Dual-Task Exercise Reduces Cognitive-Motor Interference in Walking and Falls After Stroke. Stroke 2018, 49, 2990–2998. [Google Scholar] [CrossRef]
- Hsu, C.L.; Nagamatsu, L.S.; Davis, J.C.; Liu-Ambrose, T. Examining the relationship between specific cognitive processes and falls risk in older adults: A systematic review. Osteoporos. Int. 2012, 23, 2409–2424. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; Friedman, R.; Lipton, R.B.; Katz, M.; Xue, X.; Verghese, J. The relationship between specific cognitive functions and falls in aging. Neuropsychology 2007, 21, 540–548. [Google Scholar] [CrossRef] [Green Version]
- Kearney, F.C.; Harwood, R.H.; Gladman, J.R.; Lincoln, N.; Masud, T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement. Geriatr. Cogn. Disord. 2013, 36, 20–35. [Google Scholar] [CrossRef]
- Masdeu, J.C.; Wolfson, L.; Lantos, G.; Tobin, J.N.; Grober, E.; Whipple, R.; Amerman, P. Brain White-Matter Changes in the Elderly Prone to Falling. Arch. Neurol. 1989, 46, 1292–1296. [Google Scholar] [CrossRef]
- Davenport, M.H.; Hogan, D.B.; Eskes, G.A.; Longman, R.S.; Poulin, M.J. Cerebrovascular reserve: The link between fitness and cognitive function? Exerc. Sport Sci. Rev. 2012, 40, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Lundin-Olsson, L.; Nyberg, L.; Gustafson, Y. “Stops walking when talking” as a predictor of falls in elderly people. Lancet 1997, 349, 617. [Google Scholar] [CrossRef] [PubMed]
- Organização Mundial da Saúde. CID-10: Classificação Estatística Internacional de Doenças; Edusp: São Paulo, SP, Brazil, 1994; Volume 1. [Google Scholar]
- Hunt, S.; American College of Cardiology; American Heart Association Task Force on Practice Guidelines; American College of Chest Physicians; International Society for Heart and Lung Transplantation; Heart Rhythm Society. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to update the 2001 guidelines for the evaluation and management of heart failure): Developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: Endorsed by the Heart Rhythm Society. Circulation 2005, 112, e154–e235. [Google Scholar] [PubMed] [Green Version]
- Hunt, S.A.; Baker, D.W.; Chin, M.H.; Cinquegrani, M.P.; Feldman, A.M.; Francis, G.S.; Ganiats, T.G.; Goldstein, S.; Gregoratos, G.; Jessup, M.L. ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: Executive summary: A report of the american college of cardiology/american heart association task force on practice guidelines (committee to revise the 1995 guidelines for the evaluation and management of heart failure) developed in collaboration with the international society for heart and lung transplantation endorsed by the heart failure society of america. J. Am. Coll. Cardiol. 2001, 38, 2101–2113. [Google Scholar]
- Fletcher, G.F.; Balady, G.J.; Amsterdam, E.A.; Chaitman, B.; Eckel, R.; Fleg, J.; Froelicher, V.F.; Leon, A.S.; Piña, I.L.; Rodney, R.; et al. Exercise standards for testing and training: A statement for healthcare professionals from the American Heart Association. Circulation 2001, 104, 1694–1740. [Google Scholar] [CrossRef] [Green Version]
- Mancia, G.; De Backer, G.; Dominiczak, A.; Cifkova, R.; Fagard, R.; Germano, G.; Grassi, G.; Heagerty, A.M.; Kjeldsen, S.E.; Laurent, S. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 2007, 28, 1462–1536. [Google Scholar] [CrossRef]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Brucki, S.; Malheiros, S.; Okamoto, I.; Bertolucci, P. Normative data for the animals category verbal fluency test in our environment. Arq. Neuropsiquiatr. 1997, 55, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Yesavage, J.A. Geriatric depression scale. Psychopharmacol. Bull. 1988, 24, 709–711. [Google Scholar]
- McAuley, P.; Myers, J.; Abella, J.; Froelicher, V. Evaluation of a specific activity questionnaire to predict mortality in men referred for exercise testing. Am. Heart J. 2006, 151, 890.e1–890.e7. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics; California State University: Fullerton, CA, USA, 2013. [Google Scholar]
- Ye, C.; Li, J.; Hao, S.; Liu, M.; Jin, H.; Zheng, L.; Xia, M.; Jin, B.; Zhu, C.; Alfreds, S.T.; et al. Identification of elders at higher risk for fall with statewide electronic health records and a machine learning algorithm. Int. J. Med. Inform. 2020, 137, 104105. [Google Scholar] [CrossRef] [PubMed]
- Misic, M.M.; Rosengren, K.S.; Woods, J.A.; Evans, E.M. Muscle quality, aerobic fitness and fat mass predict lower-extremity physical function in community-dwelling older adults. Gerontology 2007, 53, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.M.; Hayes, J.P.; Cadden, M.; Verfaellie, M. A review of cardiorespiratory fitness-related neuroplasticity in the aging brain. Front. Aging Neurosci. 2013, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- Muir, S.W.; Gopaul, K.; Montero Odasso, M.M. The role of cognitive impairment in fall risk among older adults: A systematic review and meta-analysis. Age Ageing 2012, 41, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Pressler, S.J.; Titler, M. Falls in Patients With Heart Failure: A Systematic Review. J. Cardiovasc. Nurs. 2016, 31, 555–561. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015.



{kind=link}
{kind=link}
| Case n = 24 | Control n = 48 | T/U/χ2 (p-Value) | |
|---|---|---|---|
| Age (years) b | 76.5 (65.0–92.0) | 73.0 (60.0–86.0) | 398.5 (0.03) * |
| Male (%) | 15 (62%) | 28 (58%) | 0.11 (0.73) |
| Ethnicity | 0.85 (0.35) | ||
| Black (%) | 5 (27%) | 6 (14%) | |
| White (%) | 19 (73%) | 42 (83%) | |
| Schooling (years) b | 16 (8–22) | 16 (8–24) | 533.0 (0.59) |
| Physical activity level | 2.89 (0.23) | ||
| Inactive (%) | 4 (16%) | 13 (27%) | |
| Two times per week (%) | 10 (42%) | 11 (23%) | |
| Three times per week (%) | 10 (42%) | 24 (50%) | |
| BMI (kg/m2) b | 26.8 (20.1–45.4) | 26.7 (18.1–34.3) | 560.5 (0.85) |
| Disease duration (years) b | 10 (2–25) | 8 (2–41) | 691.0 (0.17) |
| ACC/AHA classification | 11.53 (<0.01) ** | ||
| B (%) | 10 (42%) | 39 (81%) | |
| C (%) | 14 (58%) | 9 (19%) | |
| GDS (score) b | 2.5 (0–16.0) | 1.0 (0–28.0) | 455.5 (0.17) |
| MMSE (score) b | 29 (22–30) | 29 (23–30) | 482.5 (0.30) |
| Verbal fluency (score) a | 18.88 (4.56) | 22.25 (5.85) | −2.69 (<0.01) ** |
| Trail-making A (seconds) b | 45.10 (29.2–148.9) | 40.30 (20.8–86.1) | 453.0 (0.17) |
| Trail-making B (seconds) a | 155.44 (86.89) | 93.5 (52.0) | 3.21 (<0.01) ** |
| Dual-task (seconds) b | 8.7 (6.9–20.0) | 7.45 (4.9–19.0) | 255.5 (<0.01) ** |
| Words DT (n animals) b | 6.5 (3.0–10) | 6 (3.0–9.0) | 500.5 (0.96) |
| TUG (seconds) b | 7.44 (5.8–11.0) | 6.84 (4.2–11.0) | 339.5 (<0.01) ** |
| STS (repetitions) b | 9 (5.0–13.0) | 11.0 (0–21.0) | 364.5 (0.04) * |
| Handgrip strength (kg) b | 23.1 (12.0–52.9) | 29.25 (15.5–52.8) | 473.0 (0.21) |
| Berg (score) a | 51.71 (4.76) | 54.62 (2.63) | −2.79 (<0.01) ** |
| VSAQ (score) b | 6.0 (3.0–11.0) | 7.0 (4.0–11.0) | 436.5 (0.08) |
| FES-I (score) b | 18.5 (16.0–39.0) | 16.0 (16.0–32.0) | 399.0 (0.03) * |
| Upper limb flexibility (cm) b | −13.0 (−35.0–0) | −13.0 (−36.0–7.0) | 433.5 (0.69) |
| Lower limb flexibility (cm) b | −12.0 (−33.0–3.0) | −13.0 (−46.0–8.0) | 519.5 (0.91) |
| VO2max (mL/kg/min) b | 14.6 (10–23.1) | 18.6 (10–29.1) | 233.0 (<0.01) ** |
| Cardiac medication use | 18.65 (<0.01) ** | ||
| Antihypertensive | 16 (70%) | 18 (38%) | |
| Beta-blockers | 24 (100%) | 41 (87%) | |
| Anticoagulants | 19 (79%) | 12 (25%) | |
| Diuretics | 14 (58%) | 9 (20%) | |
| Psychiatric medication use | 8.49 (0.07) | ||
| Antidepressants | 2 (8%) | 3 (6%) | |
| Anxiolytics | 1 (4%) | 1 (2%) | |
| Benzodiazepines | 13 (54%) | 15 (32%) | |
| Combined Ant + Benz | 4 (17%) | 4 (8%) |
| Dual-Task | VO2max | Berg Scale | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | CI95% | p | OR | CI95% | p | OR | CI95% | p |
| 0.85 | 0.6–1.1 | 0.3 | 1.07 | 0.8–1.3 | 0.5 | 1.69 | 1.2–2.8 | 0.01 * |
| 0.88 # | 0.6–1.2 | 0.4 | 1.10 # | 0.8–1.3 | 0.41 | 1.64 # | 1.1–2.4 | 0.01 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silveira, H.; Lima, J.; Plácido, J.; Ferreira, J.V.; Ferreira, R.; Laks, J.; Deslandes, A. Dual-Task Performance, Balance and Aerobic Capacity as Predictors of Falls in Older Adults with Cardiovascular Disease: A Comparative Study. Behav. Sci. 2023, 13, 488. https://doi.org/10.3390/bs13060488
Silveira H, Lima J, Plácido J, Ferreira JV, Ferreira R, Laks J, Deslandes A. Dual-Task Performance, Balance and Aerobic Capacity as Predictors of Falls in Older Adults with Cardiovascular Disease: A Comparative Study. Behavioral Sciences. 2023; 13(6):488. https://doi.org/10.3390/bs13060488
Chicago/Turabian StyleSilveira, Heitor, Juliana Lima, Jessica Plácido, José Vinícius Ferreira, Renan Ferreira, Jerson Laks, and Andrea Deslandes. 2023. "Dual-Task Performance, Balance and Aerobic Capacity as Predictors of Falls in Older Adults with Cardiovascular Disease: A Comparative Study" Behavioral Sciences 13, no. 6: 488. https://doi.org/10.3390/bs13060488
APA StyleSilveira, H., Lima, J., Plácido, J., Ferreira, J. V., Ferreira, R., Laks, J., & Deslandes, A. (2023). Dual-Task Performance, Balance and Aerobic Capacity as Predictors of Falls in Older Adults with Cardiovascular Disease: A Comparative Study. Behavioral Sciences, 13(6), 488. https://doi.org/10.3390/bs13060488