
Combining Unimanual and Bimanual Therapies for Children with Hemiparesis: Is There an Optimal Delivery Schedule?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
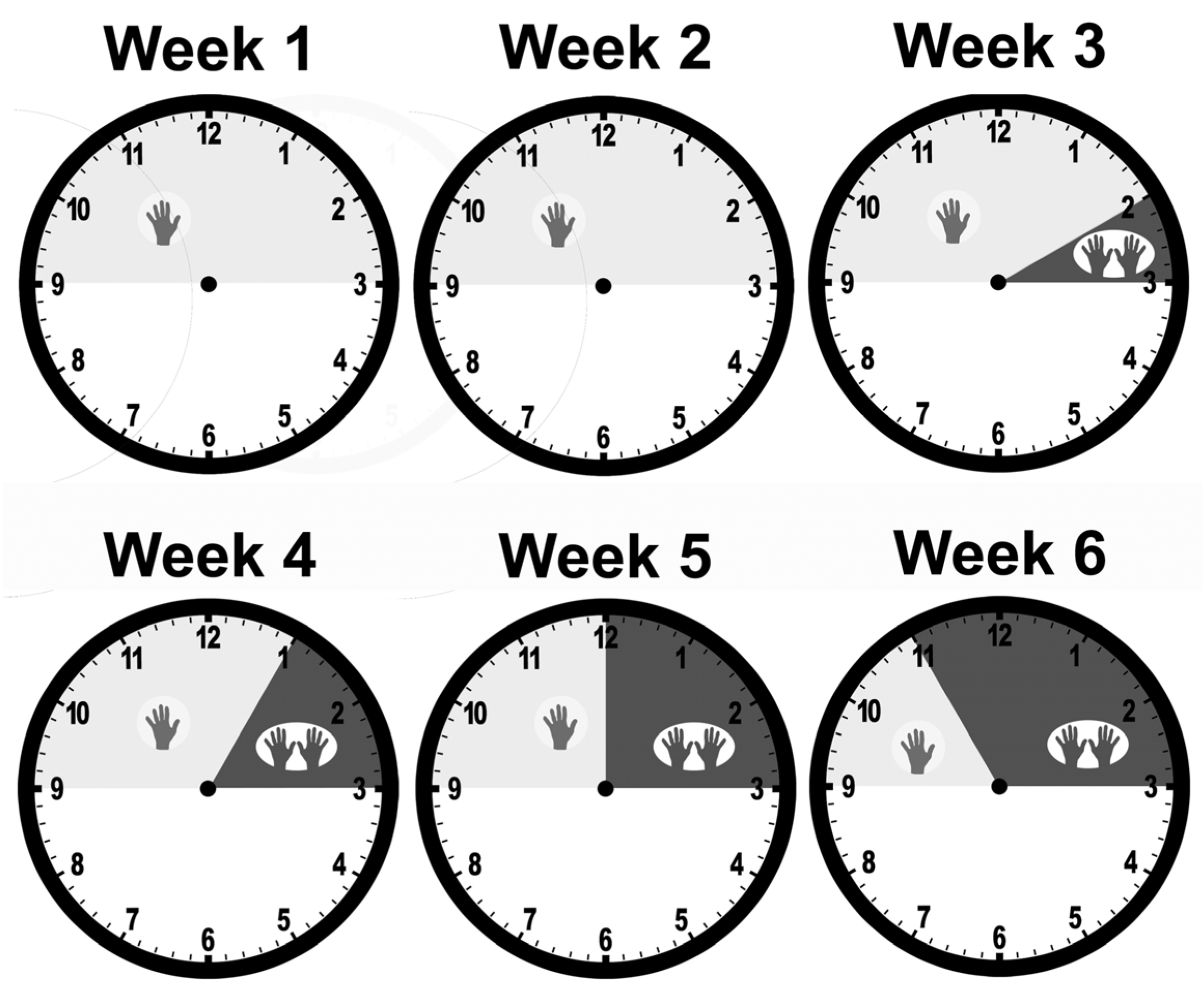
2.2. Interventions
- 3 weeks of mCIMT followed by 3 weeks of BT (group CB);
- 3 weeks of BT followed by 3 weeks of mCIMT (group BC);
- 2 weeks of mCIMT followed by stepwise incorporation of BT, increasing the amount of BT by 1 h per day for each of the next 4 weeks (group Step).
2.3. Group Allocation
2.4. Outcome Measures
2.5. Statistical Analyses
3. Results
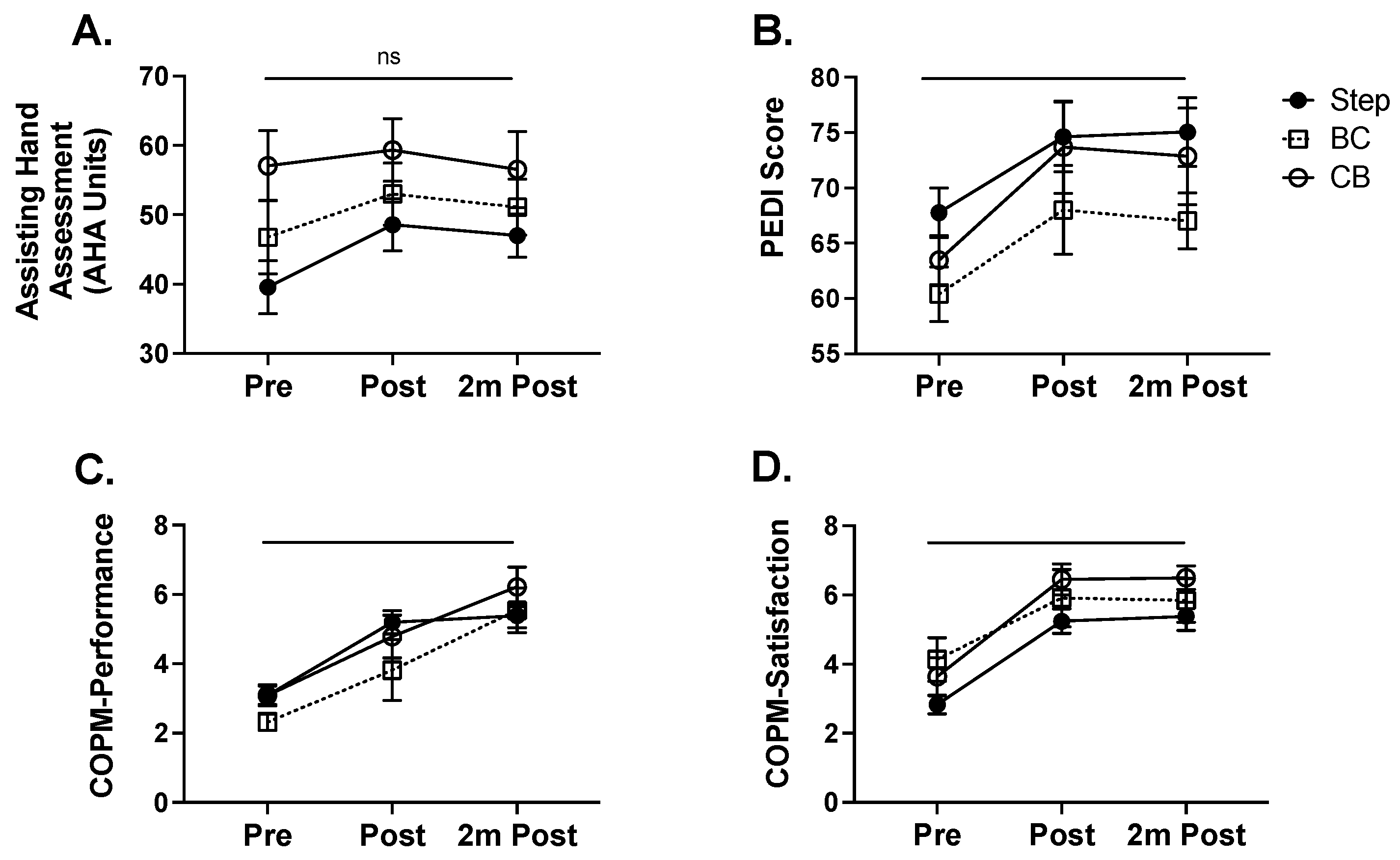
3.1. Improvements in Bimanual Hand Function after Intervention
3.2. Improvements in Self-Care Skills Independence after Intervention
3.3. Improvements in Functional Goal Performance and Satisfaction after Intervention
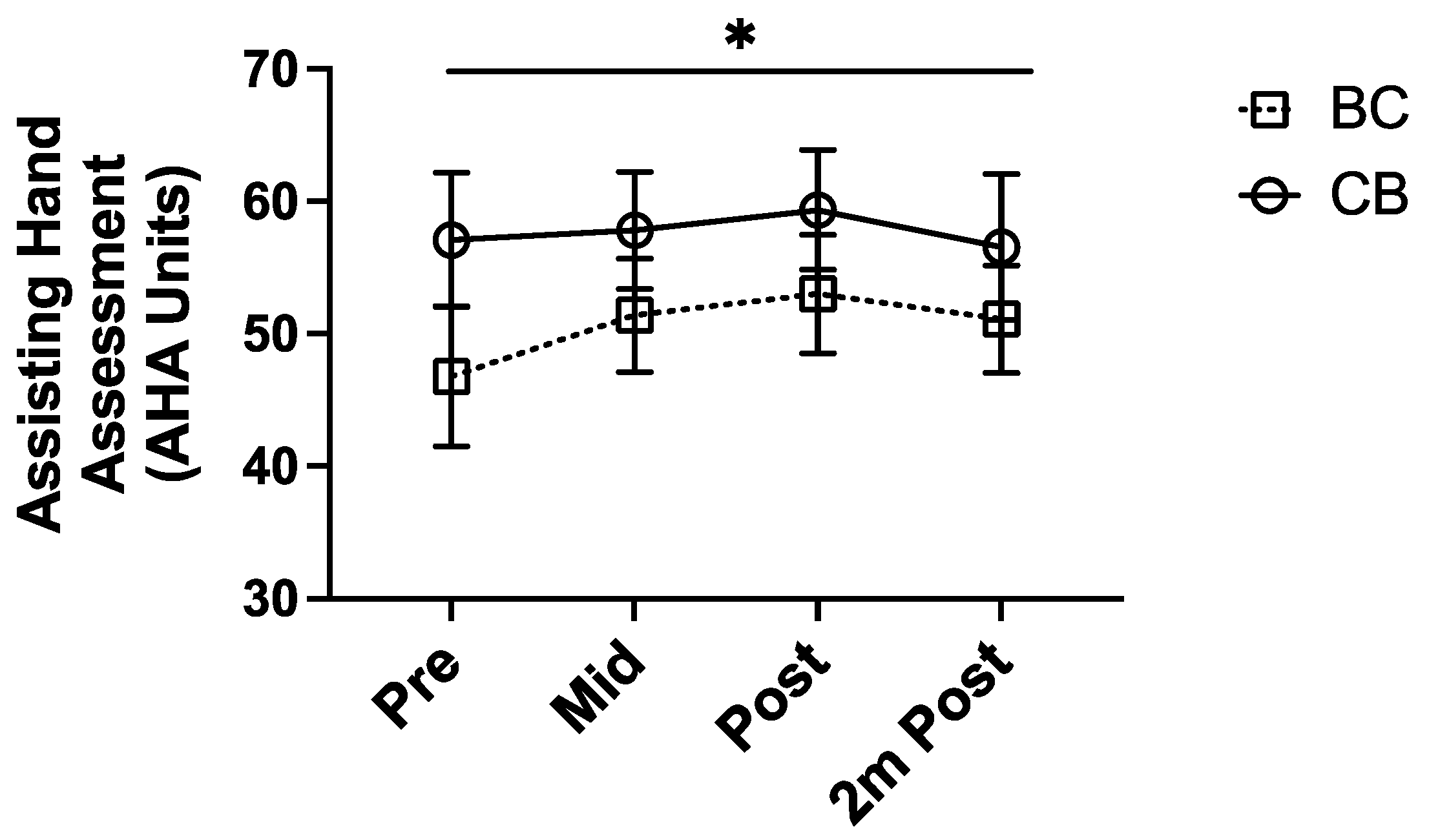
3.4. Midpoint Analysis of Bimanual Function in BC and CB Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Mc Namara, M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, J.R.; Wolf, S.L.; Schneider, J.A.; Gordon, A. Efficacy of a child-friendly form of constraint-induced movement therapy in hemiplegic cerebral palsy: A randomized control trial. Dev. Med. Child Neurol. 2006, 48, 635–642. [Google Scholar] [CrossRef] [PubMed]
- Charles, J.; Gordon, A.M. Development of hand–arm bimanual intensive training (HABIT) for improving bimanual coordination in children with hemiplegic cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Hoare, B.; Imms, C.; Carey, L.; Wasiak, J. Constraint-induced movement therapy in the treatment of the upper limb in children with hemiplegic cerebral palsy: A Cochrane systematic review. Clin. Rehabil. 2007, 21, 675–685. [Google Scholar] [CrossRef]
- Hoare, B.J.; Wasiak, J.; Imms, C.; Carey, L. Constraint-induced movement therapy in the treatment of the upper limb in children with hemiplegic cerebral palsy. Cochrane Database Syst. Rev. 2007, CD004149. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Abbott, D.F.; MacDonell, R.A.L.; Jackson, G.; Boyd, R.N. Equivalent Retention of Gains at 1 Year After Training with Constraint-Induced or Bimanual Therapy in Children with Unilateral Cerebral Palsy. Neurorehabilit. Neural Repair 2011, 25, 664–671. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Abbott, D.; MacDonell, R.A.L.; Jackson, G.D.; Boyd, R.N. Randomized trial of constraint-induced movement therapy and bimanual training on activity outcomes for children with congenital hemiplegia. Dev. Med. Child Neurol. 2011, 53, 313–320. [Google Scholar] [CrossRef]
- Dong, V.A.-Q.; Tung, I.H.-H.; Siu, H.W.-Y.; Fong, K.N.-K. Studies comparing the efficacy of constraint-induced movement therapy and bimanual training in children with unilateral cerebral palsy: A systematic review. Dev. Neurorehabilit. 2012, 16, 133–143. [Google Scholar] [CrossRef]
- Gordon, A.M.; Hung, Y.-C.; Brandao, M.; Ferre, C.L.; Kuo, H.-C.; Friel, K.; Petra, E.; Chinnan, A.; Charles, J.R. Bimanual Training and Constraint-Induced Movement Therapy in Children with Hemiplegic Cerebral Palsy. Neurorehabilit. Neural Repair 2011, 25, 692–702. [Google Scholar] [CrossRef]
- Friel, K.M.; Ferre, C.L.; Brandao, M.; Kuo, H.-C.; Chin, K.; Hung, Y.-C.; Robert, M.T.; Flamand, V.H.; Smorenburg, A.; Bleyenheuft, Y.; et al. Improvements in Upper Extremity Function Following Intensive Training Are Independent of Corticospinal Tract Organization in Children with Unilateral Spastic Cerebral Palsy: A Clinical Randomized Trial. Front. Neurol. 2021, 12, 660780. [Google Scholar] [CrossRef]
- Brandão, M.D.B.; Gordon, A.M.; Mancini, M.C. Functional Impact of Constraint Therapy and Bimanual Training in Children with Cerebral Palsy: A Randomized Controlled Trial. Am. J. Occup. Ther. 2012, 66, 672–681. [Google Scholar] [CrossRef] [Green Version]
- Gordon, A. Two hands are better than one: Bimanual skill development in children with hemiplegic cerebral palsy. Dev. Med. Child Neurol. 2010, 52, 315–316. [Google Scholar] [CrossRef]
- Bingöl, H.; Günel, M.K. Comparing the effects of modified constraint-induced movement therapy and bimanual training in children with hemiplegic cerebral palsy mainstreamed in regular school: A randomized controlled study. Arch. Pediatr. 2022, 29, 105–115. [Google Scholar] [CrossRef]
- Deppe, W.; Thuemmler, K.; Fleischer, J.; Berger, C.; Meyer, S.; Wiedemann, B. Modified constraint-induced movement therapy versus intensive bimanual training for children with hemiplegia—A randomized controlled trial. Clin. Rehabil. 2013, 27, 909–920. [Google Scholar] [CrossRef]
- Hung, Y.-C.; Spingarn, A.; Friel, K.M.; Gordon, A.M. Intensive Unimanual Training Leads to Better Reaching and Head Control than Bimanual Training in Children with Unilateral Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2020, 40, 491–505. [Google Scholar] [CrossRef]
- Hoare, B.; Greaves, S. Unimanual versus bimanual therapy in children with unilateral cerebral palsy: Same, same, but different. J. Pediatr. Rehabil. Med. 2017, 10, 47–59. [Google Scholar] [CrossRef]
- de Brito Brandao, M.; Mancini, M.C.; Vaz, D.V.; de Melo, A.P.P.; Fonseca, S.T. Adapted version of constraint-induced movement therapy promotes functioning in children with cerebral palsy: A randomized controlled trial. Clin. Rehabil. 2010, 24, 639–647. [Google Scholar] [CrossRef]
- Klingels, K.; Feys, H.; Molenaers, G.; Verbeke, G.; Van Daele, S.; Hoskens, J.; Desloovere, K.; De Cock, P. Randomized Trial of Modified Constraint-Induced Movement Therapy with and Without an Intensive Therapy Program in Children with Unilateral Cerebral Palsy. Neurorehabilit. Neural Repair 2013, 27, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Krumlinde-Sundholm, L.; Holmefur, M.; Kottorp, A.; Eliasson, A.-C. The Assisting Hand Assessment: Current evidence of validity, reliability, and responsiveness to change. Dev. Med. Child Neurol. 2007, 49, 259–264. [Google Scholar] [CrossRef]
- Holmefur, M.; Krumlinde-Sundholm, L.; Eliasson, A.-C. Interrater and Intrarater Reliability of the Assisting Hand Assessment. Am. J. Occup. Ther. 2007, 61, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Verkerk, G.J.Q.; Wolf, M.J.M.A.G.; Louwers, A.M.; Meester-Delver, A.; Nollet, F. The reproducibility and validity of the Canadian Occupational Performance Measure in parents of children with disabilities. Clin. Rehabil. 2006, 20, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Baptiste, S.; McColl, M.; Opzoomer, A.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: An Outcome Measure for Occupational Therapy. Can. J. Occup. Ther. 1990, 57, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Iyer, L.V.; Haley, S.M.; Watkins, M.P.; Dumas, H.M. Establishing minimal clinically important differences for scores on the pediatric evaluation of disability inventory for inpatient rehabilitation. Phys. Ther. 2003, 83, 888–898. [Google Scholar] [CrossRef] [PubMed]
- Berg, M.; Jahnsen, R.; Frøslie, K.F.; Hussain, A. Reliability of the Pediatric Evaluation of Disability Inventory (PEDI). Phys. Occup. Ther. Pediatr. 2004, 24, 61–67. [Google Scholar] [CrossRef]
- Gordon, A.M.; Schneider, J.A.; Chinnan, A.; Charles, J.R. Efficacy of a hand–arm bimanual intensive therapy (HABIT) in children with hemiplegic cerebral palsy: A randomized control trial. Dev. Med. Child Neurol. 2007, 49, 830–838. [Google Scholar] [CrossRef]
- Mutsaarts, M.; Steenbergen, B.; Bekkering, H. Anticipatory planning deficits and task context effects in hemiparetic cerebral palsy. Exp. Brain Res. 2006, 172, 151–162. [Google Scholar] [CrossRef]
- Steenbergen, B.; Jongbloed-Pereboom, M.; Spruijt, S.; Gordon, A. Impaired motor planning and motor imagery in children with unilateral spastic cerebral palsy: Challenges for the future of pediatric rehabilitation. Dev. Med. Child Neurol. 2013, 55 (Suppl. S4), 43–46. [Google Scholar] [CrossRef] [Green Version]
- Martinie, O.; Mercier, C.; Gordon, A.M.; Robert, M.T. Upper Limb Motor Planning in Individuals with Cerebral Palsy Aged between 3 and 21 Years Old: A Systematic Review. Brain Sci. 2021, 11, 920. [Google Scholar] [CrossRef]
- Gutterman, J.; Lee-Miller, T.; Friel, K.M.; Dimitropoulou, K.; Gordon, A.M. Anticipatory Motor Planning and Control of Grasp in Children with Unilateral Spastic Cerebral Palsy. Brain Sci. 2021, 11, 1161. [Google Scholar] [CrossRef]
- Simon-Martinez, C.; Mailleux, L.; Hoskens, J.; Ortibus, E.; Jaspers, E.; Wenderoth, N.; Sgandurra, G.; Cioni, G.; Molenaers, G.; Klingels, K.; et al. Randomized controlled trial combining constraint-induced movement therapy and action-observation training in unilateral cerebral palsy: Clinical effects and influencing factors of treatment response. Ther. Adv. Neurol. Disord. 2020, 13, 1756286419898065. [Google Scholar] [CrossRef] [Green Version]
- Gupta, D.; Barachant, A.; Gordon, A.; Ferre, C.; Kuo, H.-C.; Carmel, J.B.; Friel, K.M. Effect of sensory and motor connectivity on hand function in pediatric hemiplegia. Ann. Neurol. 2017, 82, 766–780. [Google Scholar] [CrossRef]
- Delfing, D.; Chin, K.; Hentrich, L.; Rachwani, J.; Friel, K.M.; Santamaria, V.; Imms, C.; Gordon, A.M. Assessing engagement in rehabilitation: Development, validity, reliability, and responsiveness to change of the Rehabilitation Observation Measure of Engagement (ROME). Disabil. Rehabil. 2023, 10, 1–10. [Google Scholar] [CrossRef]
- Friel, K.M.; Kuo, H.-C.; Fuller, J.; Ferre, C.L.; Brandão, M.; Carmel, J.B.; Bleyenheuft, Y.; Gowatsky, J.L.; Stanford, A.D.; Rowny, S.B.; et al. Skilled Bimanual Training Drives Motor Cortex Plasticity in Children with Unilateral Cerebral Palsy. Neurorehabilit. Neural Repair 2016, 30, 834–844. [Google Scholar] [CrossRef] [Green Version]
- Kuhnke, N.; Juenger, H.; Walther, M.; Berweck, S.; Mall, V.; Staudt, M. Do patients with congenital hemiparesis and ipsilateral corticospinal projections respond differently to constraint-induced movement therapy? Dev. Med. Child Neurol. 2008, 50, 898–903. [Google Scholar] [CrossRef]
- Smorenburg, A.R.P.; Gordon, A.M.; Kuo, H.-C.; Ferre, C.L.; Brandao, M.; Bleyenheuft, Y.; Carmel, J.B.; Friel, K.M. Does Corticospinal Tract Connectivity Influence the Response to Intensive Bimanual Therapy in Children with Unilateral Cerebral Palsy? Neurorehabilit. Neural Repair 2016, 31, 250–260. [Google Scholar] [CrossRef] [Green Version]
- Gelkop, N.; Burshtein, D.G.; Lahav, A.; Brezner, A.; Al-Oraibi, S.; Ferre, C.L.; Gordon, A. Efficacy of Constraint-Induced Movement Therapy and Bimanual Training in Children with Hemiplegic Cerebral Palsy in an Educational Setting. Phys. Occup. Ther. Pediatr. 2014, 35, 24–39. [Google Scholar] [CrossRef]
- Klepper, S.E.; Krasinski, D.C.; Gilb, M.C.; Khalil, N. Comparing Unimanual and Bimanual Training in Upper Extremity Function in Children with Unilateral Cerebral Palsy. Pediatr. Phys. Ther. 2017, 29, 288–306. [Google Scholar] [CrossRef]
- Rice, D.; Barone, S., Jr. Critical periods of vulnerability for the developing nervous system: Evidence from humans and animal models. Environ. Health Perspect. 2000, 108 (Suppl. S3), 511–533. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Child/Group | Sex | Age (Y, M) | Paretic Side | AHA Baseline | COPM Baseline | PEDI Baseline |
|---|---|---|---|---|---|---|
| Step01 | M | 3, 11 | R | 21 | 3.2 (P), 2.8 (S) | 58 |
| Step02 | F | 7, 9 | R | 47 | 3.8 (P), 4.5 (S) | 74.7 |
| Step03 | M | 9, 1 | R | 53 | 3.5 (P), 2.5 (S) | 72.6 |
| Step04 | F | 6, 6 | R | 38 | 4.2 (P), 3.6 (S) | 57.4 |
| Step05 | M | 8, 1 | R | 35 | 3.4 (P), 2.6 (S) | 66 |
| Step06 | F | 12, 5 | L | 30 | 4.0 (P), 3.4 (S) | 79 |
| Step07 | M | 8, 1 | R | 17 | 4.8 (P), 4.0 (S) | 66 |
| Step08 | F | 10, 4 | R | 58 | 3.4 (P), 3.8 (S) | 77.3 |
| Step09 | F | 10, 7 | R | 44 | 1.6 (P), 1.8 (S) | 74.7 |
| Step10 | M | 5, 2 | L | 44 | 1.8 (P), 2.6 (S) | 55.6 |
| Step11 | M | 6, 7 | L | 24 | 2.0 (P), 1.6 (S) | 71.7 |
| Step12 | M | 5, 8 | R | 27 | 3.0 (P), 3.4 (S) | 61.2 |
| Step13 | M | 6, 3 | R | 58 | 3.0 (P), 2.4 (S) | 58.6 |
| Step14 | M | 9, 5 | L | 58 | 1.6 (P), 1.0 (S) | 75.9 |
| BC01 | M | 12, 0 | L | 50 | 4 (P), 7.2 (S) | 65.3 |
| BC02 | F | 5, 8 | R | 59 | 2 (P), 5 (S) | 53.7 |
| BC03 | M | 5, 3 | R | 30 | 2 (P), 4.8 (S) | 55.6 |
| BC04 | M | 4, 9 | R | 61 | 1.8 (P), 5 (S) | 59.9 |
| BC05 | M | 5, 2 | L | 7 | 1.4 (P), 2.8 (S) | 51.7 |
| BC06 | F | 9, 0 | L | 52 | 2.2 (P), 5.8 (S) | 61.2 |
| BC07 | F | 8, 8 | R | 59 | 3.2 (P), 3 (S) | 75.9 |
| BC08 | M | 4, 11 | L | 55 | 2.4 (P), 1.4 (S) | 55.6 |
| BC09 | M | 5, 9 | L | 52 | 1.8 (P), 2.2 (S) | 70 |
| BC10 | M | 5, 5 | R | 43 | 2.4 (P), 2.6 (S) | 54.9 |
| CB01 | M | 4, 8 | R | 87 | 4.2 (P), 6.8 (S) | 63.9 |
| CB02 | M | 5, 9 | R | 33 | 3.4 (P), 6.6 (S) | 59.9 |
| CB03 | M | 10, 2 | R | 50 | 1.8 (P), 5.2 (S) | 75.9 |
| CB04 | F | 4, 9 | L | 65 | 2 (P), 5.2 (S) | 60.5 |
| CB05 | F | 11, 2 | R | 50 | 3.8 (P), 3.4 (S) | 60.5 |
| CB06 | F | 5, 8 | R | 52 | 4.6 (P), 4.2 (S) | 62.5 |
| CB07 | M | 11, 0 | L | 47 | 2.2 (P), 1.6 (S) | 77.3 |
| CB08 | M | 9, 8 | L | 52 | 3 (P), 1.8 (S) | 65.3 |
| CB09 | F | 5, 1 | L | 66 | 2 (P), 2 (S) | 63.2 |
| CB10 | M | 7, 6 | R | 84 | 4 (P), 2 (S) | 56.2 |
| CB11 | M | 5, 9 | R | 42 | 3 (P), 2.2 (S) | 53 |
| Summaries | Counts | Avg ± SD | Counts | Avg ± SD | Avg ± SD | Avg ± SD |
| Step (n = 14) | 9M/5F | 7.4 ± 2.3 | 10R/4L | 39.6 ± 14.3 | 3.1 ±1.0 (P), 2.8 ± 1.0 (S) | 67.8 ± 8.3 |
| BC (n = 10) | 7M/3F | 6.8 ± 2.5 | 5R/5L | 46.8 ± 16.7 | 2.3 ± 0.8 (P), 4.0 ± 1.8 (S) | 60.4 ± 7.8 |
| CB (n = 11) | 7M/4F | 7.5 ± 2.7 | 7R/4L | 57.1 ± 16.8 | 3.1 ± 1.0 (P), 3.7 ±2.0 (S) | 63.5 ± 7.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Au, K.L.K.; Knitter, J.L.; Morrow-McGinty, S.; Campos, T.C.; Carmel, J.B.; Friel, K.M. Combining Unimanual and Bimanual Therapies for Children with Hemiparesis: Is There an Optimal Delivery Schedule? Behav. Sci. 2023, 13, 490. https://doi.org/10.3390/bs13060490
Au KLK, Knitter JL, Morrow-McGinty S, Campos TC, Carmel JB, Friel KM. Combining Unimanual and Bimanual Therapies for Children with Hemiparesis: Is There an Optimal Delivery Schedule? Behavioral Sciences. 2023; 13(6):490. https://doi.org/10.3390/bs13060490
Chicago/Turabian StyleAu, Ka Lai K., Julie L. Knitter, Susan Morrow-McGinty, Talita C. Campos, Jason B. Carmel, and Kathleen M. Friel. 2023. "Combining Unimanual and Bimanual Therapies for Children with Hemiparesis: Is There an Optimal Delivery Schedule?" Behavioral Sciences 13, no. 6: 490. https://doi.org/10.3390/bs13060490
APA StyleAu, K. L. K., Knitter, J. L., Morrow-McGinty, S., Campos, T. C., Carmel, J. B., & Friel, K. M. (2023). Combining Unimanual and Bimanual Therapies for Children with Hemiparesis: Is There an Optimal Delivery Schedule? Behavioral Sciences, 13(6), 490. https://doi.org/10.3390/bs13060490