1. Introduction
In the year 2015, more than 90% of the Indian population had access to improved drinking water sources [
1]. Improved drinking water sources are defined as water sources that are protected from outside contamination, such as fecal matter, due to their construction, proper use, and/or other active interventions [
2]. This definition includes water supplies piped into dwellings or to plots, public taps, tubewells and boreholes, protected wells and springs, and rainwater. Even though improved drinking water sources in low and middle income countries have shown less fecal contamination than unimproved sources [
3], access to improved drinking water sources is only a proxy for safe water supply and does not guarantee that the drinking water is free from contamination [
4]. Population density, type and density of latrines, and sealing of wells are other factors that have been shown to influence microbiological water quality [
5,
6]. In addition, the quality of the water sources vary with the season, often indicating higher contamination levels in the wet season [
4,
7].
Large efforts have been made by the Indian government as well as by state governments to improve the conditions for water supply and sanitation. Programs such as the Central Rural Sanitation Programme and the Total Sanitation Campaign have led to an increase in coverage of water supply and sanitation infrastructure [
8]. However, the provision of, and access to, infrastructure does not automatically lead to improved health outcomes [
9,
10]. In the last decade, the water supply system in India has shifted from a top-down, supply-led water delivery approach to a demand-driven approach, requiring community participation [
11]. Community participation has been institutionalized, meaning that, for example, in practice, the surveillance of drinking water quality falls under the responsibility of the municipality [
12].
Nevertheless, most Indian water supply systems are still intermittent systems with irregular pressure and questionable water quality [
13]. Water is not continuously available, and this makes water storage at the household level necessary. This storage is considered a challenge and an opportunity at the same time: the possible recontamination of drinking water between source and point-of-use is well-recognized [
14,
15,
16,
17,
18], as is the ability of households to reduce bacterial contamination by home treatment [
19,
20,
21]. There are two concepts that have shown the potential to improve drinking water quality and lower the burden of diarrheal disease. “Household water treatment and storage” (HWTS) interventions help to ensure the microbiological safety of water. They include point-of-use water treatment technologies (e.g., boiling, solar disinfection, chlorination, filtration, or other chemical treatment) as well as improved transport, storage, and handling practices for potable water (e.g., storage in clean containers, preferably with narrow dispensers or long-handled ladles to extract the water) [
22]. “Water, sanitation, and hygiene” (WASH) practices target the issues of safe water supply, improved sanitation, and hygiene behaviors in an integrated way. WASH practices comprise good personal hygiene practices, such as regular hand-washing with soap and good food hygiene practices, the availability of sanitation facilities and the safe disposal of feces, as well as access to safe water supply points [
23]. Both HWTS interventions and WASH practices have been shown to be useful in the reduction of diarrhea occurrence [
19,
24], but their protective effect varied in different studies [
21], and their effectiveness seemed to have deteriorated over time as people stopped using them [
25].
The adoption of HWTS interventions and WASH practices by households depends on different factors. Protection motivation theory [
26] and psychological behavior models (for an overview see Dreibelbis, et al. [
27] or Parker Fiebelkorn, et al. [
28]) distinguish situational, social, and individual psychological behavior determinants influencing the personal practice of a certain behavior. Situational factors reflect circumstances that make it difficult to perform behaviors such as HWTS interventions or WASH practices. Examples include limitations of existing infrastructure, a lack of water supply reliability, and inadequate water quality. The community in which a person lives determines social factors. They encompass the behavior of peer groups such as family, friends, neighbors, and the perceived social pressure of doing something [
29], but also social benefits received by performing a certain behavior [
30]. Individual psychological factors determining behavioral changes towards HWTS and WASH applications include personal risk perception, attitudes, normative factors, ability factors, and self-regulation or control factors [
27,
29,
31]. These abstract factors can be further broken down into sub-aspects, e.g., attitudes include how individuals assess the risk or health impact of not performing safe HWTS and WASH interventions in comparison to the time and monitoring costs related to those treatments or in comparison to the result (i.e., less diarrhea, and better taste, odor, or clarity of treated water). These factors are operationalized in several survey questions, as described by, for example, Inauen
, et al. [
32]. Of great importance in this context are well-designed promotion and information campaigns [
33], aimed at increasing knowledge about HWTS and WASH interventions, to “convince” people to change their behavior.
Tilley, et al. [
34] looked beyond individual motivations and drivers of behavior, and identified an enabling environment, economic conditions, and the technologies used as important factors to establish and maintain sustainable water, sanitation, and hygiene practices, and infrastructure in low income countries. “Enabling environment” means that appropriate political, legal, institutional, financial, educational, and technical conditions are in place to successfully implement HWTS and WASH. Economic conditions encompass both opportunities associated with the use of a technology (e.g., income generation due to maintaining or selling water or sanitation infrastructure) and incentives to motivate the use of a technology (e.g., financial support to purchase or construct infrastructure or cover operative expenditures). In relation to HWTS interventions and WASH practices, this means, for example, to assure that households have enough money to buy chlorine solution for chemical water treatment. The last aspect is the technology itself, or the chain of technologies needed to successfully perform water, sanitation, and hygiene interventions. For sanitation, this technology chain starts at the user interface (e.g., the toilet) and ends with the final disposal or use of excreta-derived products [
29], while for drinking water it ends at the user interface, i.e., the point of consumption, and starts at the water source, or even before, in the water catchment. Tilley, et al. [
34] argue that the whole chain has to be considered, and a holistic view has to be adopted to assure sustainable operation.
All these factors should not be seen separately. In reality they interact, overlap, and complement each other. For example, insufficient individual economic resources might be backed up by governmental financial support (enabling environment), or desired behavioral changes can be influenced by economic incentives or information campaigns.
Whether a rural household’s drinking water is of a microbiologically safe standard depends on a lot of factors. These start with the quality of the water source, include the effectiveness of public treatment (the supply system), and conclude with safe storage and handling at the household level. To our knowledge, there are not many studies that follow water quality from the source to the point of consumption and consider enabling conditions and individual factors influencing the practice of HWTS and WASH interventions at the household level. The main aim of this study was two-fold: first, we wanted to investigate the water quality of different of raw water sources used for drinking purposes in the study area, as well as the water quality at the point of consumption in households; and second, we wanted to explore the links between water management practices at the community and household level, and water quality at the point of consumption. Even though the study investigates only eight rural villages in Maharashtra, and can thus not be considered as representative for the whole state, it sheds light on the “importance of the last meter”, i.e., how storage and treatment practices before consumption influence water quality and which factors encourage households to treat their water.
2. Materials and Methods
2.1. Study Design
This study takes a descriptive observational design approach. It studies the water supply system by collecting and analyzing water samples throughout its supply chain: i.e., at the raw water source, after interventions at the village level, as well as at the point of consumption in households. Storage, treatment, and supply at the village level are explored by focus group discussions, and storage and treatment at household level are investigated by household surveys.
After consultation of the Norwegian National Research Ethics Committee (NENT), the Norwegian Institute for Water Research confirmed that this research project did not require ethical approval. The project was registered with the Norwegian Centre for Research Data (NSD) to ensure proper data handling routines and privacy of personal data.
2.2. Selection of Study Sites
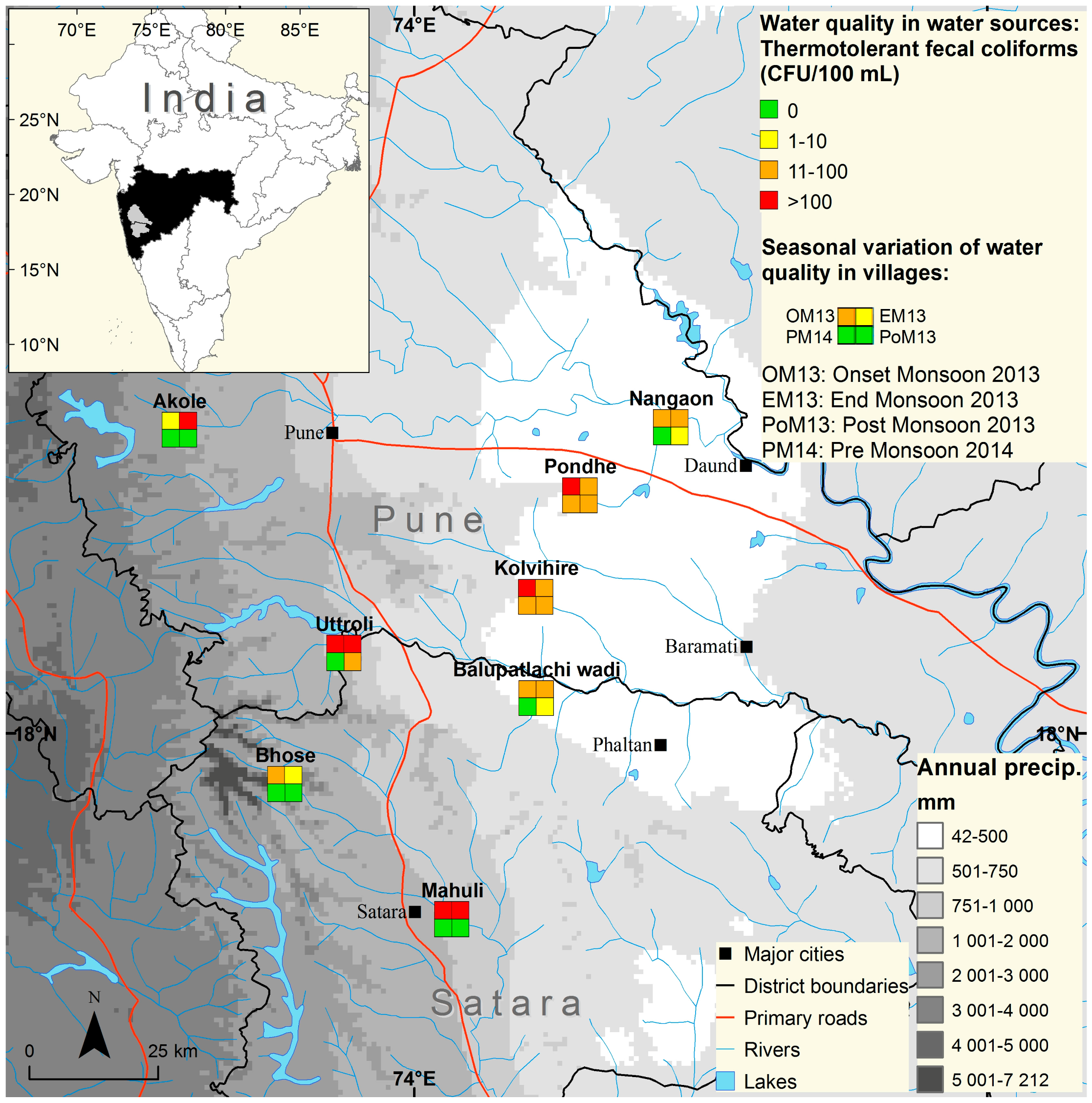
Located in the western region of India, Maharashtra is the second most populous state with over 112 million inhabitants [
35]. About 55% of the population lives in rural areas dependent on agriculture and animal husbandry. There is a high variation of annual rainfall among the regions in the state, varying from 300 to more than 6000 mm (see
Figure 1), mainly falling in the monsoon season from June to September. Future climate projections predict an increase in monsoon precipitation in coastal areas, no change or a decrease in inland areas [
36], a delay in monsoon onset [
37], and more erratic rainfall patterns in the monsoon season [
38,
39].
Eight villages located in the districts of Pune and Satara were selected for this study. The aim of the selection was to capture villages with a population of mixed socio-economic status and where fecal contamination was prevalent in the raw water source, according to a previous sampling campaign (unpublished data). Akole, Bhose, Utroli, and Sangam Mahuli are located in or close to the Western Ghats mountain range, and receive an average annual rainfall of between 783 and 5405 mm, while Pondhe, Nangaon, Balu Ptalachiwadi, and Kolvihire lie in the rain shadow area with an average annual rainfall of below 500 mm (
Figure 1).
2.3. Drinking Water Sample Collection and Analysis
Nine major drinking water sources (open wells and boreholes) in eight villages were sampled in a period of two years. From June 2013 to May 2015, water samples were taken at the onset of the monsoon (June–July), at the end of monsoon (August–September), in the post-monsoon or winter period (December and January), and in the pre-monsoon or summer season (April–May). For the second year, additional water samples were taken from water storages in 134 households of all villages. The household samples were taken on the same day as the water sources were sampled. There were three rounds of household water sampling to cover all seasons: monsoon (August 2014), post-monsoon (December 2014), and pre-monsoon (May 2015).
Before the first sampling took place, the Gram Panchayats, the elected representatives of each village, were informed about the purpose of the study and asked for permission to include their village in the study. Households were also informed and asked for consent prior to water sampling. They were also informed about their right to withdraw consent at any stage. The Gram Panchayats were advised about the sampling results from open wells and boreholes. Individual sampling results were reported back to the households by members of the project team during personal visits in September/October 2016.
All samples were collected in clean sterile plastic bottles. For samples where we expected chlorinated water (open wells and storage tanks), sodium thiosulfate was added to the bottles before sterilization. Samples were immediately kept on ice and in dark conditions, transported to the laboratory, stored at 4 °C, and analyzed the following day, i.e., within 24 h.
Fecal coliforms (FC) were enumerated by membrane filtration through cellulose acetate, with 0.22 µ filters of 100 mL, 10 mL, and 1 mL aliquots. In order to detect FC, the filter papers were placed onto membrane-fecal coliforms (m-FC) agar and incubated at 44.5 °C for 24 h. The filter papers were then observed for blue-colored colonies. The plate in which countable isolated colonies were observed was used for enumeration and the results were expressed as Colony Forming Units (CFU) per 100 mL. According to the Indian standard for Drinking Water [
40], drinking water should not contain any FC in 100 mL water.
The sampling, transport, and analysis procedure followed standard routines [
41] with the exception that non-potable water samples had to be kept for more than the recommended 8 h due to the long distance between the sampling sites and the laboratory. However, since our sampling was not for regulatory purposes, we have treated drinking water and non-potable water the same.
2.4. Focus Groups and Household Survey
A targeted questionnaire for households was developed, pre-tested in households in neighboring villages, refined, and finally translated from English to Mahrati. It contained open and closed questions covering the following topics:
Socio-economic and family characteristics, including livelihood conditions
Demand, availability, and affordability of drinking water
Status and expectations regarding the water quality including perceived water quality
Water handling practices (HWTS-interventions)
WASH practices and diarrhea occurrence
Institutional aspects
In the period July to December 2014, trained interviewers, who conducted the survey in Mahrati, visited a total of 459 households. The households were selected by random sampling, but included those where water samples were taken.
Following general ethical standards, consent was verbally obtained before undertaking the interviews and participants were made aware that they were free to not answer questions or stop the survey at any time and for any reason. Before the survey was carried out, the elected head of the village (Sarpanch), was contacted to seek permission to conduct the survey.
The household interviews were supplemented by focus group discussions with the Gram Panchayat, including the Sarpanch, and with groups of males and females, representatives of different castes, people from different hamlets and of mixed ages. In the meetings, people actively shared their perspectives, issues, and vulnerabilities with respect to water availability and quality in the village. The focus group discussions were conducted before and after the household survey was completed in each village, to ensure the inclusion of perspectives of other village members who were not selected for the survey. Discussions were conducted over a period from July to December 2014, aiming to triangulate the opinions of different groups on the same issue.
2.5. Statistical Analysis
Data was entered manually into Microsoft Excel 2010 and independent quality checks were done to eliminate data entry errors. Statistical analysis was performed with GNU PSPP (version 0.8.5, GNU Project, Free Software Foundation, Boston, USA). Nominal scaled variables were tested for significant differences by using a χ2-homogeneity test. For dichotomous ordinal-scaled variables, the U-test of Mann and Whitney, and for ordinal variables with more than two realization possibilities the H-test of Kruskal and Wallis, was used to test for significance differences. The Spearman rank-order correlation coefficient was calculated to evaluate the strength of relationships between variables. For all tests, the level of significance was <5%.
3. Results
3.1. Descriptive Demographic Statistics
Altogether, 459 households in 8 villages were interviewed. The average household size was 5.42 persons (median 5), with few households containing only one or more than ten persons. There were elderly persons (above 60 years of age) living in 57% of households and children younger than 12 years in 52% of households. Household size was stable during the year, indicating little labor-migration. Agriculture is the main economic activity in both districts, while wage employment and causal labor are important secondary activities. To assess the economic status of households, it was recorded if households were above poverty level (APL) or below poverty level (BPL) card holders. On average, 80% were APL card holders and only 20% were BPL card holders, but there were significant (χ2 = 19.06, df = 7, α < 0.01) variations between villages. In Kolvihire, 35% of surveyed households were BPL card holders, while in Utroli only 6% were BPL card holders. Of respondents, there were 54% female and 46% male, with the average age of 42.4 years (median 40), ranging from 14 to 85 years. Only 37% of interviewees had completed secondary education, 15% had higher education (university), while 17% had no formal education at all.
3.2. The Water Supply and Treatment System
In the current water supply system in our study area (
Figure 2), three “stages of intervention” can be distinguished, which determine final water quality at the consumer level:
Source level: The water quality of the source used depends on the natural conditions of the water body as well as on human and animal activities in the catchment. The available water sources are surface water and shallow and deep groundwater. Where it can be avoided, surface water is not used for drinking due to possible fecal contamination. Shallow groundwater is extracted mainly by open wells, whereas deep groundwater is obtained by boreholes. Shallow groundwater is less protected from fecal contamination than boreholes due to the more rapid infiltration of surface water. Additionally, open wells offer less protection due to their open construction, which is a direct route for contamination from the environment. Degraded water quality from high concentrations of naturally occurring substances, such as arsenic or fluoride, was not prevalent in our study area. The main contamination sources were human and animal feces, runoff from chemicals used in agriculture, and industrial pollution (steel fabrication in Kolvihire, Balu Patlachiwadi, and Mahuli).
Village level: Typical drinking water schemes for all study villages included raw sources, namely water from open or boreholes, electrically pumped through pipes to an often elevated storage tank. Water was either in the storage tank or in the open well commonly treated with chlorine for disinfection purposes before it was distributed to household or community taps around the village by gravitational pressure. Gram Panchayat and the Sarpanch oversee the management of water supply and treatment, and hence any complaints about water quality or breakdown of services goes to the Sarpanch.
The primary responsibility for the maintenance and operation of the water system in each village lies with the appointed “waterman”, who is from the same village and is paid by the Gram Panchayat. The waterman receives basic training on his duties from the health department at the block level, including on chlorination practices. This department is also in charge of taking monthly water samples and monitoring the water quality. The regularity of chlorine treatment varied among the villages between daily chlorination, regular chlorination in monsoon seasons, and irregular chlorination whenever the waterman thought it was needed.
Household level: Water supply to households is not continuous but varies between 0.5 and 2 h daily or every second day. Thus, villagers have to withdraw water when available and store it until the next supply phase. Households that do not have access to private taps or public standposts must get their water directly from the raw water source itself, usually boreholes or open wells, but also from surface water. Households that usually have access may also do this when their supply is interrupted for an unusually long period, e.g., due to technical supply failures. The water fetched at the raw water source may have undergone chlorination (e.g., in villages where chlorination is directly done in the open well), but this is not always the case. During monsoon season, when water quality is expected to be worse than in other seasons, the Gram Panchayat provides households with a free chlorine solution, making it possible to improve water quality prior to consumption.
Piped tap water into dwellings was the most common primary source of drinking water across villages (56%), while direct collection from boreholes ranked second (18%), and direct collection from open wells ranked third (13%). Purchased bottled water (6%) and surface water (2%) were also mentioned as primary drinking sources. There were large variations among villages in private tap connections, ranging from almost 100% private tap connections (Balu Patlachiwadi and Sangam Mahuli) to no private tap connections (Pondhe). The majority of respondents (71%) had access to at least one alternative drinking water source. The main reason for having to change water source was scarcity of water during the dry summer season (49%), second was failure of the technical system (43%), and some (5%) changed sources due to unacceptable water quality of the primary source. Respondents’ alternative sources were similar to primary ones, although tankers were additionally mentioned and another 10% of respondents identified their use of surface water.
The focus group discussions revealed some issues with the current water supply and treatment system. In some villages, certain hamlets or parts of the village received less water than other parts due to the unfavorable topography. In one village, people reported that the supply was only available once in 5 days for 10–15 min and so they were forced to illegally abstract water from a pipeline. In another village, during water stress, people in some hamlets had to travel for more than 1 km to fetch water. Water quality variations between hamlets were also mentioned. A steel factory’s proximity to one hamlet was related to deteriorated water quality. Water supply differed between villages, and depended to a large extent on the performance of the waterman. In one village, the village head expressed their satisfaction with the waterman’s work, while villagers complained that he was often drunken and that they did not rely on his water treatment.
3.3. Measured Water Quality
The analysis of all water sources (surface water, open wells, and boreholes) in the study villages showed a high variability of FC concentrations, ranging from ‘not detected’ in 100 mL to 6500 CFU/100 mL. There were large differences both between the types of water sources and seasons (
Table 1 and
Figure 1). The highest number of positive samples containing FC was found at the onset of monsoon season. Surface waters, such as rivers and backwaters to dams, showed the highest level of fecal contamination. Boreholes more often had undetected FC and overall lower concentrations of FC than open wells.
The analysis of drinking water samples collected in households revealed that in the post-monsoon season only 49% of all households consumed drinking water that satisfied the criteria of no FC detected in 100 mL sample. This percentage dropped to 40% in pre-monsoon and even lower to only 36% during the monsoon (data not shown). There were significant differences between the villages concerning the FC concentrations through all seasons: in monsoon (χ2 = 26.74, df = 7, α < 0.001), in post-monsoon (χ2 = 46.71, df = 7, α < 0.001), and in pre-monsoon (χ2 = 17.90, df = 7, α < 0.05). During monsoon in Utroli, only 9% of the sampled households did not have FC in their drinking water, while in Sangam Mahuli this was the case for 85% of households.
3.4. Perceived Water Quality
The majority, 93%, of respondents stated they that felt their drinking water was, in general, of sufficient quality. Differentiating seasons revealed that during the monsoon only 50% shared this opinion. During the monsoon, 14% of respondents were deeply concerned about their drinking water quality and thought it was unfit for use, while in other seasons this rating was only given by 4–5% of respondents. When asked why they perceived water quality as insufficient, 41% complained about turbidity as the major problem, 16% referred to bad taste, and 14% to bad smell as the criteria for insufficient quality, while 12% mentioned that the poor quality resulted in stomach problems or illnesses and 4% reported that the water had bugs or worms.
There was no indication that age, gender, education, or the economic conditions of households had an influence on the perception of water quality.
Supply type differentiation revealed interesting results (
Table 2): during monsoon, there were significant differences in the perceived water quality of the different drinking water supply types, but not during other seasons. Less users of piped dwelling water perceived their water quality as good compared to users of community taps.
The findings indicate that perceived water quality deterioration coincided with a measured deterioration of biological quality during the monsoon season (
Table 1), whereas for the other seasons there was no perceived difference.
There were also significant differences in perceived water quality between villages (data not shown). Year-round water quality was evaluated to be of sufficient quality by all respondents in Utroli and Bhose, but only by 79% in Pondhe. The seasonal rating of water quality also revealed significant differences between villages in the dry season (χ2 = 65.09, df = 7, α < 0.001), in monsoon (χ2 = 149.50, df = 7, α < 0.001), in winter season (χ2 = 63.52, df = 7, α < 0.001), and in post-monsoon season (χ2 = 47.77, df = 7, α < 0.01). In Balu Ptalachiwadi during the monsoon, as much as 45% of the respondents had deep concerns about their water quality or rated it as unfit for consumption, whereas, through the rest of the year, more than 95% rated it as of good to average quality (data not shown). Problems with a muddy appearance of the water, bad taste, smell, and resulting illnesses or an upset stomach were mostly reported in Balu Ptalachiwadi and Sangam Mahuli. To a lesser extent, these problems were also an issue in Kolvihire.
3.5. HWTS Interventions and WASH Practices
Seventy-six percent (76%) of all households reported to have access to a piped water supply, and for 56% piped water was accessible within their dwelling. Nevertheless, households had to store their drinking water for 0–2 days before consumption, as supply was not continuous. The majority (99%) of respondents had separate storage containers for domestic use and drinking water purposes, all kept their storage vessels covered, and 70% elevated these vessels. The sizes of storage containers ranged from 4 to 80 liters. The most common were metal storage vessels (95%), but people reported also to use plastic and earthen containers. The latter were used particularly in summer time to keep the water cool. The majority of respondents (91%) cleaned their storage containers every day before refilling with water, while some only cleaned the vessels on a weekly basis (8%), and 1% monthly or in less frequent intervals. The most common cleaning method was to use soap, followed by the use of wood-ash, cleaning powder, and mud. Less than 2% used only water for cleaning the vessels. Transport vessels were cleaned less frequently (79% daily, 16% once a week, and 4% once a month or more seldom) and to a larger extent (5%) only with water instead of using scrubbing agents.
The informants reported various ways of removing water from the storage container. The most common way of getting water from the vessel was by using a cup for dipping (79%), 11% had a spigot attached, 7% reported to use a ladle, and 3% reported to pour directly from the vessel. Most of the people using a cup (98%) also reported that their hands got wet during drinking water removal, but only 34–55% of them washed their hands before removal, which indicates that there is a potential for drinking water recontamination. Reported hand-washing routines showed that 96% washed their hands before eating and 82% with soap, but only 26% washed their hands after defecating. When asking about the accessibility of the drinking water container for household members, we obtained inconsistent results: while 59% indicated that all household members have access, 99% said that children under 5 have no access, and only 7% of all households’ school-aged children have access.
The majority of households (83%) practiced treatment interventions to purify their drinking water. The most common were chemical treatment (47%) by adding bleach, chlorine, or Al(OH3), filtration through a cloth (44%) or water filter (16%), boiling (11%), and “stand and settle” treatment (3%). Solar disinfection was not practiced, and 5% of households reported to buy bottled water instead of treatment interventions. While boiling and chemical treatment effectively reduce microbiological contamination, the other treatments are mainly used to decrease turbidity and remove particles. The Gram Panchayat provided a chlorine solution in small bottles to households in the village, while the other interventions had to be carried out and/or purchased by households themselves. Thirty-five percent (35%) of households practice more than one type of treatment with varying frequencies, usually applied either continuously, daily, only in monsoon, or when the water looks, smells, or tastes bad.
Concerning the sanitary situation, 62% of households reported to have a closed sewage system, usually a septic tank, and 25% to have an open sewage system. However, again, there were significant differences between the villages for closed sewage systems (χ2 = 33.31, df = 7, α < 0.001) and open sewage systems (χ2 = 47.17 df = 7, α < 0.001). In Sangam Mahuli, septic tank coverage reached 80%, while in Akole, only 38% of the households had septic tanks, but 57% reported having an open sewage system (data for the other villages not shown).
3.6. Factors Potentially Influencing HWTS and WASH Application
3.6.1. Economic Conditions
From other studies, it is known that factors such as education level [
42], socio-economic status, and gender [
43] cause differences in the application of HWTS interventions and WASH practices.
In this study, we found a significant difference between APL and BPL card households in terms of if HWTS interventions were practiced or not (χ2 = 16.77, df = 1, α < 0.001). Of the APL cardholders, 87% practiced treatment, while only 69% of BPL cardholders did so. There was no significant difference between APL and BPL households concerning the type of treatment, except for the use of water filters (χ2 = 6.07, df = 1, α < 0.05): 18% of APL cardholders used water filters, while in BPL households only 8% used them. Concerning the application frequency of different treatment options, no differences were found.
Considering water storage, significantly more APL households elevated their water storage than BPL households (χ2 = 5.64, df = 1, α < 0.05). No differences were found concerning the material of storage containers and the type of cleaning methods applied. A significant difference (minimal) was found for the frequency of cleaning (χ2 = 6.45, df = 2, α < 0.05). APL households more frequently practiced daily cleaning of the drinking water storage containers (92%) compared to BPL households (86%).
There is an indication that the economic status of a household influences its WASH practices. Significant differences were found for “hand washing before eating” (χ2 = 8.80, df = 1, α < 0.01) and “hand washing before feeding children” (χ2 = 3.98, df = 1, α < 0.05), as well as for the “use of soap for hand washing” (χ2 = 6.51, df = 1, α < 0.05). For all three practices, APL households had a higher ratio than BPL households.
No differences between APL and BPL cardholders were found concerning their belief that diarrhea is preventable, and opinions on what can be done to prevent it.
3.6.2. Education, Sex, and Age
Compared to households with lower education levels, those that had completed higher education were significantly more often storing their drinking water in elevated tanks (χ2 = 12.34, df = 4, α < 0.05). In households where the respondent had no formal education, only 60% of the drinking water storage tanks were elevated; this number increased to 84% in households where the respondent had received higher education. Significant differences exist concerning how the drinking water is removed from the storage vessel (χ2 = 30.85, df = 12, α < 0.01). Respondents with higher education to a lesser extent reported using a cup for drinking water removal, but more often used ladles with a handle or attached a spigot or tap to their container. Similarly, significantly less respondents with higher education reported wet hands when getting drinking water out of the tank, compared to those with lower education levels (χ2 = 13.92, df = 4, α < 0.01).
There were significantly more interviewees with higher education who believe it is possible to prevent diarrhea than interviewees with no, or only primary education (χ2 = 21.92, df = 8, α < 0.01). Those with higher education also mentioned significantly more often that diarrhea can be prevented by ensuring only adequate water quality is used, or by treatment it if lacks adequate quality (χ2 = 16.93, df = 4, α < 0.01).
People with higher education washed their hands with soap significantly more often than people with lower education levels (χ2 = 21.07, df = 4, α < 0.001). Ninety-six percent (96%) of respondents with higher education used soap, but only 70% of those with no formal education and 78% of those with primary education used soap.
The sex and age of interviewees did not play an important role for the answers on WASH practices and HWTS interventions. Some techniques were mentioned considerably more often by men (e.g., using cleaning powder for scrubbing of drinking water storage containers), and others by women (e.g., using wood-ash for cleaning drinking water storage containers). Female interviewees reported washing their hands after defecating significantly more often than men, 32% compared to 19%, respectively (χ2 = 9.87, df = 1, α < 0.01), in addition to more often mentioning maintenance of cleanliness and hygiene in preventing diarrhea (χ2 = 5.28, df = 1, α < 0.05).
3.6.3. Geographic Dimension
There were significant differences between the villages concerning HWTS interventions as well as WASH practices (data not shown). The percentage of households using chemical treatment ranged from 84% in Alkole to only 4% in Nangaon, and similarly 76% of Alkole practiced two or more types of treatment, while only 2% did so in Nangaon.
Significantly more households (18% in comparison to a 7% average, χ2 = 20.49, df = 7, α < 0.01) in Balu Ptalachiwadi used earthen drinking water storage containers, whereas plastic containers were more widespread in Nangaon (13% in comparison to a 5% average, χ2 = 21.62, df = 7, α <0.01) and only metal containers were used in Alkole (100% coverage in comparison to a 95% average, χ2 = 23.79, df = 7, α < 0.01).
Balu Ptalachiwadi also had the lowest percentage of people that thought diarrhea is preventable (39% in comparison to a 50% average, χ2 = 42.54, df = 14, α < 0.001). Only 23% of respondents there thought that the consumption of safe water or the treatment of water could assist in preventing diarrhea, while 54% in Sangam Mahuli believed this to be the case (average of 40%, χ2 = 15.50, df = 7, α < 0.05).

 ,
, 


{kind=link}
{kind=link}