Medical Assistant Mobile Application for Diabetes Control by Simulating a Compartmental Model

 , , ,
, , ,
Abstract
:Featured Application
Abstract
1. Introduction
2. State of the Art
2.1. PC or Web Simulators for Glucose Concentration Levels
2.2. Mobile Applications for Diabetes Management
3. Models
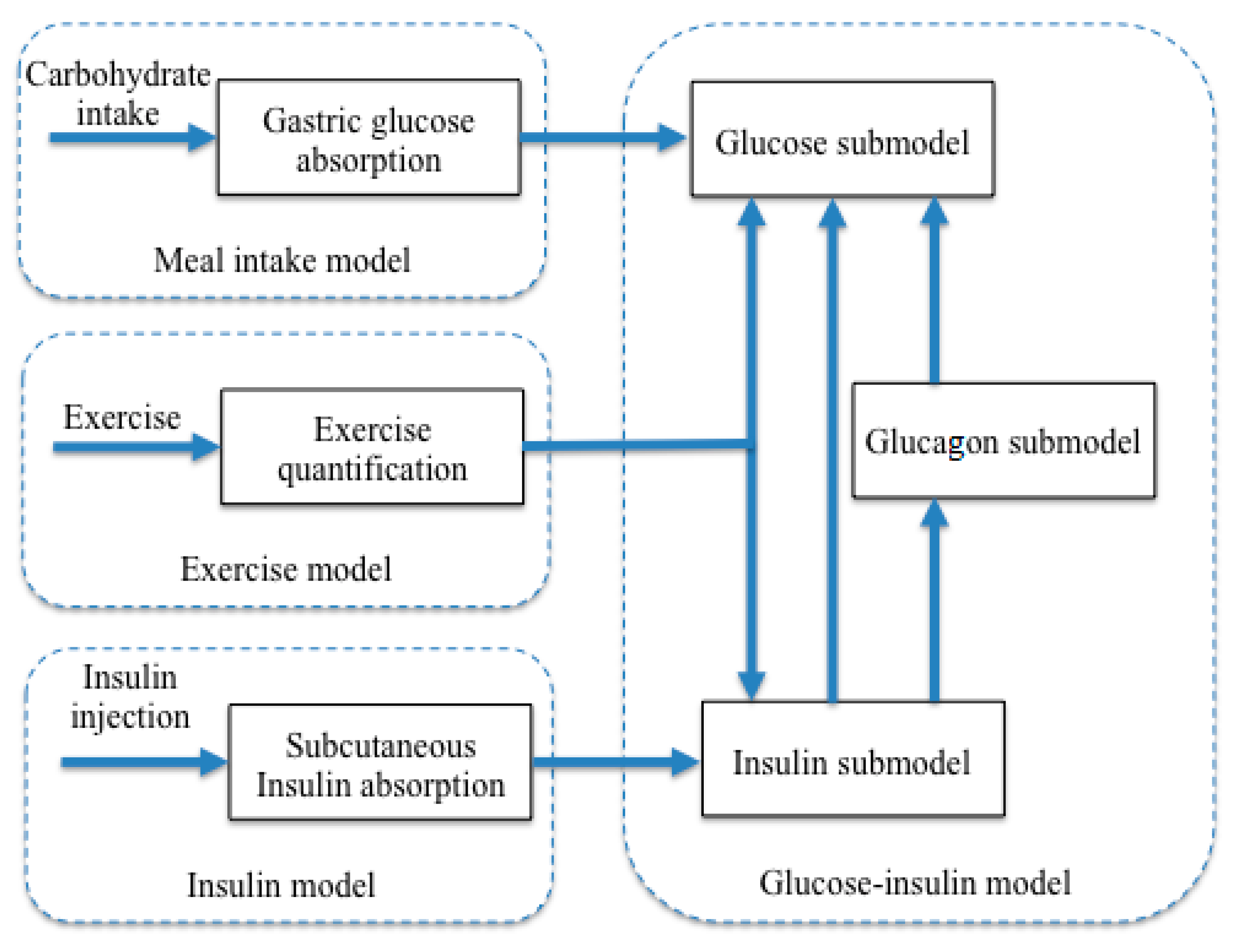
- Glucose-Insulin Model: Sorensen in [40] proposed it. This model comprises 19 nonlinear differential equations, which include significant metabolic effects related to glucose regulation. The model was obtained through a compartmental technique, where the pancreas compartment is omitted to consider a type 1 diabetic patient. Recently, this glucose-insulin model was extended to consider exercise periods [41].
- Subcutaneous Insulin model: Berger and Rodbard [42] obtained it. This model describes the subcutaneous insulin uptake pattern after an insulin injection. The model considers interactions between components after subcutaneous injections such as insulin absorption and elimination in plasma insulin, active insulin, glucose utilization, plasma glucose, and glucose input. The model is based on a set of differential equations. Variations in plasma insulin concentration (I) can be estimated by Equation (1).where Iabs represents the rate of insulin absorption, Vi is the volume of insulin distribution, and ke is the first-order rate constant of insulin elimination. The absorption of insulin can be calculated as follows:where s is a parameter associated with the insulin absorption pattern, t represents the time of the injection, T50 is when the dose (D) is absorbed in an amount of 50%.
- To estimate steady-state conditions, insulin profile (Iss) using the superposition principle is computed assuming three days as follows:where Ia is the build-up and the deactivation of the insulin pump.
- Meal Intake model: this model was proposed in 1992 by Lehmann and Deutsch [43]. It describes the gastric glucose absorption into the bloodstream by a meal intake represented by its carbohydrates content. According to this model, glucose utilization Gout (G) at plasma insulin concentration is:G represents the glucose concentration, Vmax maximal glucose utilization for reference insulin concentration, and Km is glucose concentration for the half-maximal response. Vmax depends on insulin; mathematically, this iswhere Iss is plasma insulin concentration equivalent to steady-state insulin, and Gx is the reference glucose value. Glucose utilization for any combination of plasma glucose and insulin levels is given bywhere c is insulin sensitivity, and d represents insulin-independent glucose utilization. The insulin absorption dynamics for regular, NPH, lente, ultralente formulations were characterized in [42] just by changing some specific parameters in the general model. Recently, in [44], the Lispro insulin formulation was also characterized by the model in [42].
- The exercise model was considered from [41]. The liver’s glycogen reservoir (GLY) can be calculated as shown in Equation (8).where φ is the net glycogenolysis rate, Ψ represents the absorptive period, ζ is the glucose uptake due to exercise intensity, and PVO2max is the percentage of the maximum oxygen consumption rate.
4. Results and Discussion
4.1. Mobile Application for Educational Similar
4.1.1. Hardware and Software Tools
4.1.2. System Architecture
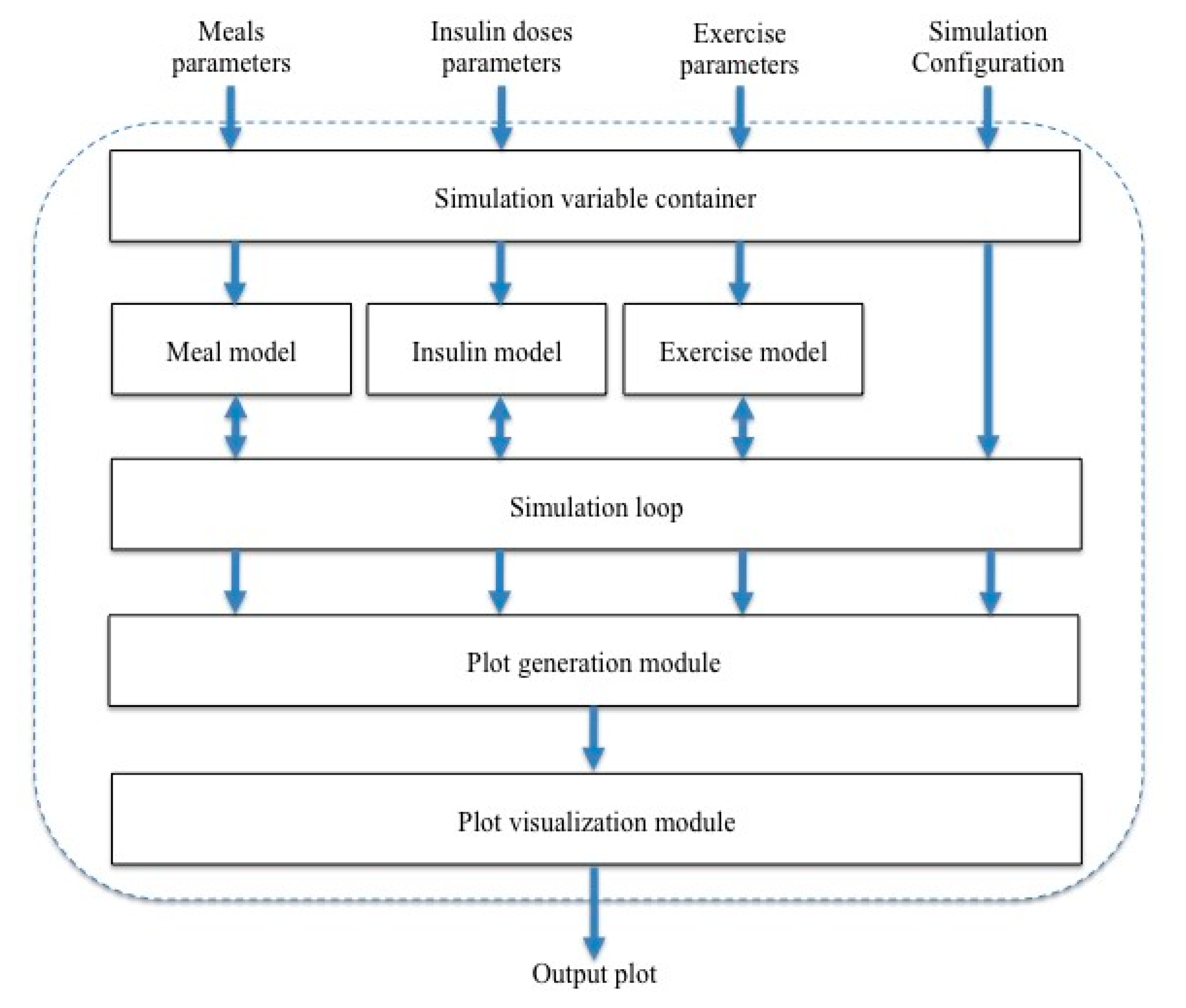
- Meal parameters: these parameters are related to carbohydrate intake (in grams) and the day´s carbohydrate intake schedule.
- Insulin dose parameters: these parameters are related to the type (fast or slow actions) and the dose of insulin (in units).
- Exercise parameters: these parameters are related to the quantity and intensity of exercise.
- Simulation configuration: these parameters are related to the simulation’s duration and the type of plot to be generated.
- The architecture contains the following blocks:
- Simulation variables container: this block stores data required to be accessed and shared by all model blocks. It contains three profiles: meal dosing, insulin dosing, and exercise quantification.
- Meal model block: this block takes as input the meal profile and generates as output the glucose obtained according to the carbohydrate intake grams.
- Insulin model block: this block takes as input the insulin dosing profile and generates as output the quantity and duration of insulin in the blood flow.
- Exercise model block: this block takes as input the exercise dosing profile and generates as output the blood redistribution volume according to the quantity of exercise.
- Simulation loop block: this block updates each model block with required data from others and controls the simulation’s start and end.
- Plot generation module: this block generates data from the simulation to be used for generating a plot.
- Plot visualization module: this block takes as input the vector generated by the plot generation module and displays the plot.
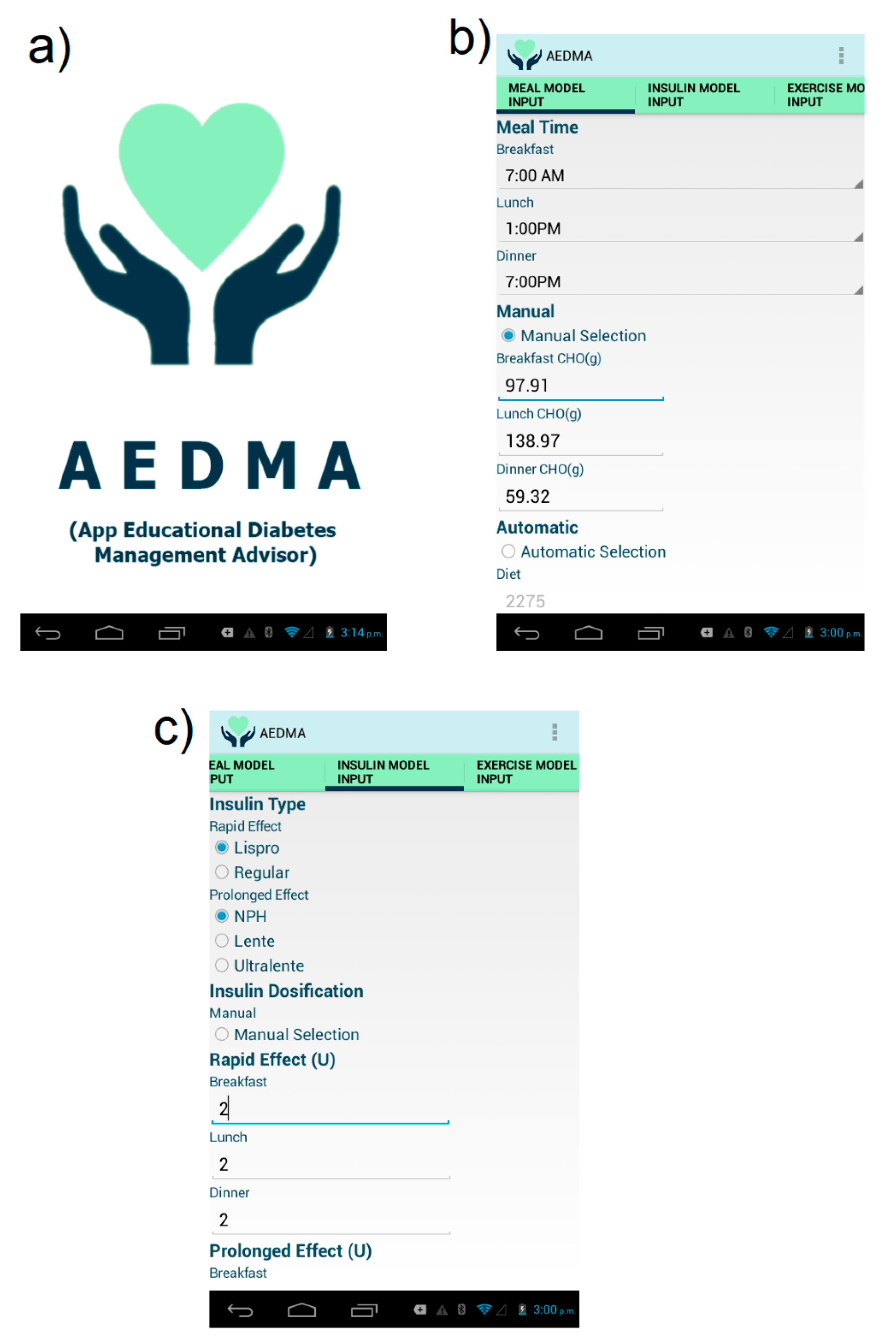
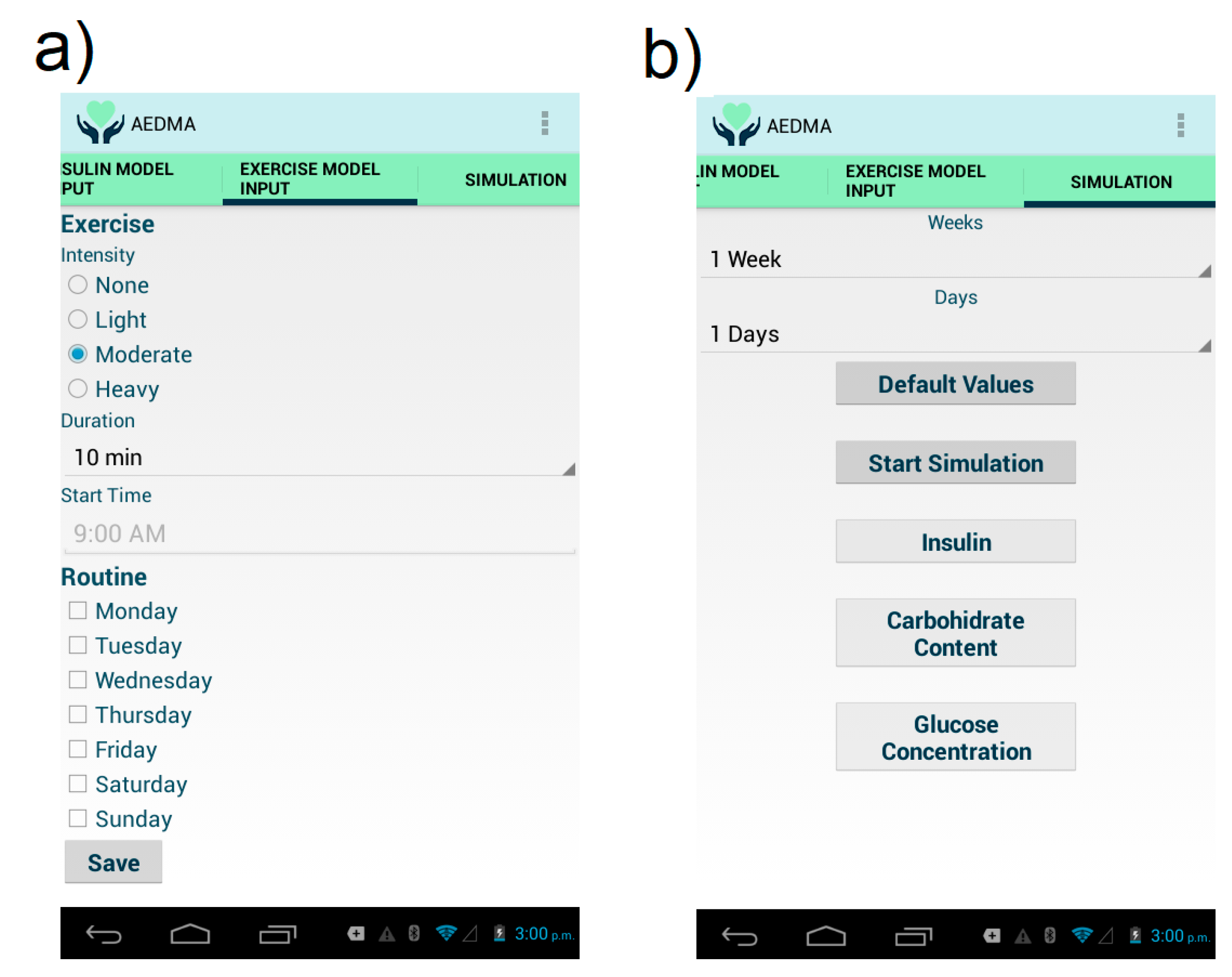
4.1.3. User Interface
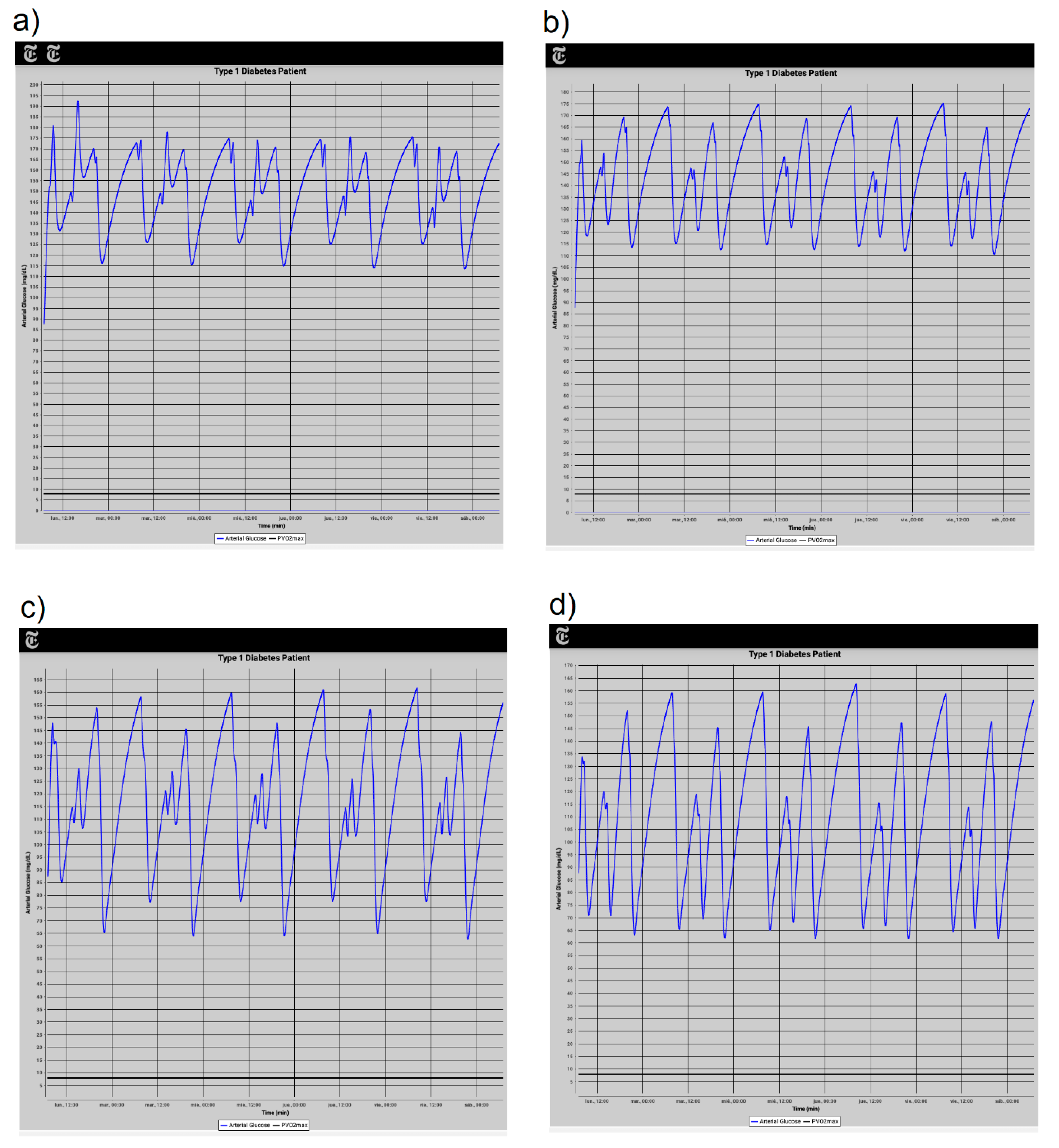
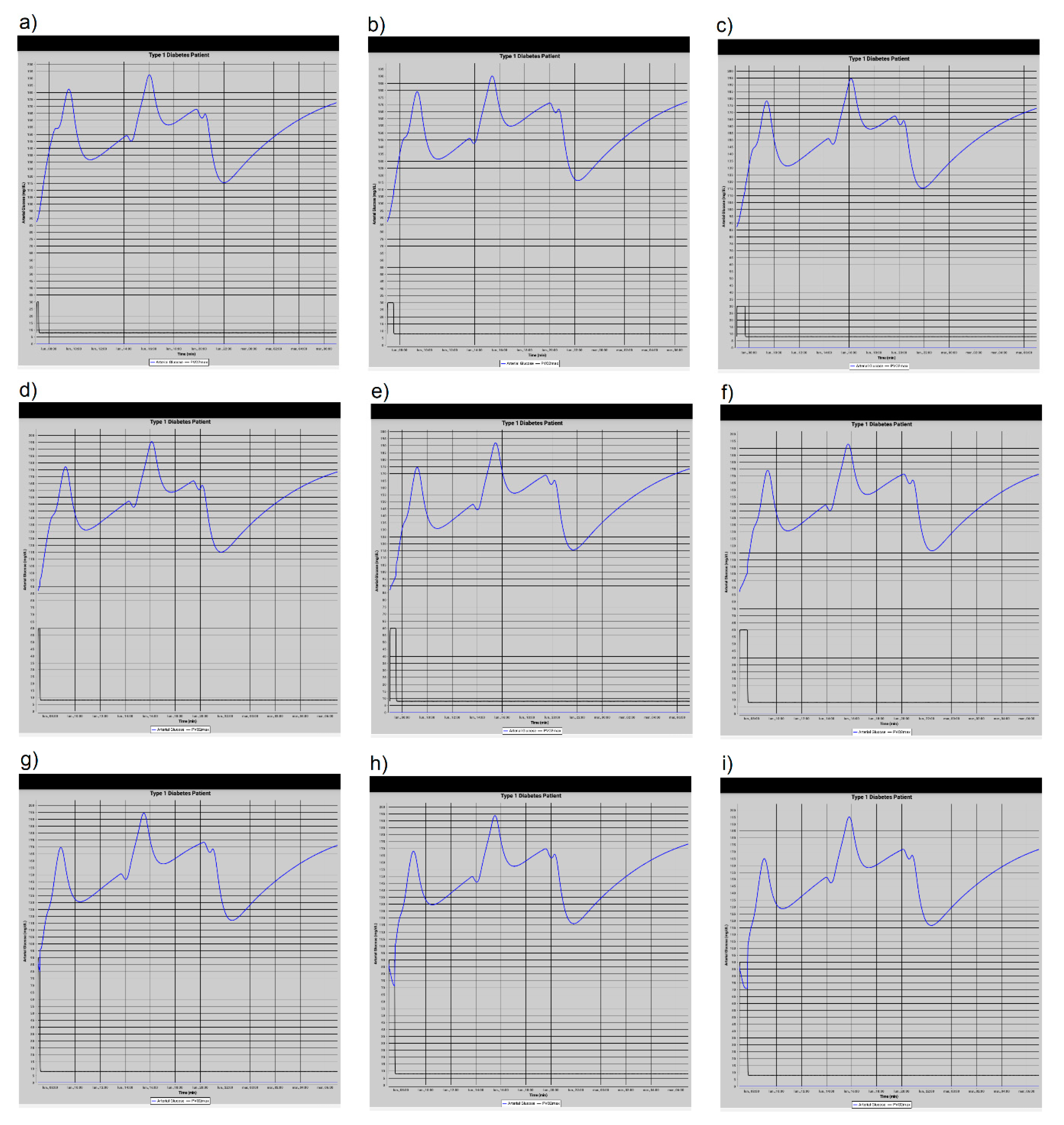
4.2. Reported Experiments
4.3. Qualitative Study
- From questions 1, 3, 4, and 5, a preliminary conclusion about important points to be improved to the AEDMA can be guessed. These points are related to improving the user interface, the clarity, and legibility of presented glucose level graphs, and the ease of use of the app. Question 8 gives a general panorama showing that the mobile app in its current state can be improved. From question 9, the variability of glucose levels is adequate from the user’s perspective.
- In general, from questions 2 and 7, we can conclude that the AEDMA is useful and to give an appropriate impression to the test user, to reuse the application if a next version is released. Question 10 allows highlighting the importance of giving users an important role to involve them in the design of these types of apps.
4.4. Execution Time Comparison
5. Conclusions
- The App includes glucose regulation associated with metabolism and the application of an insulin injection.
- The App is capable of taking into account the effects of food intake and physical activity.
- The developed application can simulate the behavior of glucose levels for long periods.
- The App is capable of considering three types of physical activity: light, moderate and heavy.
- The developed application is focused on type-1 diabetes, but this can be extended to consider type-2 diabetes.
- As a future improvement, the application should be modified to split the simulation processing into smaller operations running on multiple threads. This could be beneficial in devices with more than one core.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight Fact Sheet; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Diabetes Fact Sheet; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Institute for Health Metrics and Evaluation. The Global Burden of Disease: Generating Evidence, Guiding Policy; IHME: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. The Top 10 Causes of Death; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- Levy, T.S.; Nasu, L.C.; Dommarco, J.R.; Ávila, M.H. Informe Final de Resultados, Encuesta Nacional de Salud y Nutrición de Medio Camino 2016; Instituto Nacional de Salud Pública INSP: Mexico City, Mexico, 2016. [Google Scholar]
- Institute for Health Metrics and Evaluation (IHME). Country Profile Mexico. Mexico, 2017. Available online: http://www.healthdata.org/ (accessed on 7 October 2018).
- Statista Inc. Global Smartphone Sales to End Users 2007–2016. Available online: https://www.statista.com/statistics/263437/global-smartphone-sales-to-end-users-since-2007/ (accessed on 12 October 2018).
- eMarketer. Worldwide Internet and Mobile Users: eMarketer’s Updated Estimates and Forecast for 2015–2020. 2016. Available online: https://www.emarketer.com/Report/Worldwide-Internet-Mobile-Users-eMarketersUpdated-Estimates-Forecast-20152020/2001897#moreReport (accessed on 25 September 2018).
- Lehmann, E. Preliminary experience with the Internet release of AIDA—An interactive educational diabetes simulator. Comput. Methods Programs Biomed. 1998, 56, 109–132. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Ordonez, M.; Montano, O.; Campos-Delgado, D.U.; Palacios, E. Development of an Educational Simulator and Graphical User Interface for Diabetic Patients. In Proceedings of the 2007 4th International Conference on Electrical and Electronics Engineering, Mexico City, Mexico, 5–7 September 2007; pp. 82–85. [Google Scholar] [CrossRef]
- Lehmann, E.D.; Tarín, C.; Bondia, J.; Teufel, E.; Deutsch, T. Development of AIDA v4.3b Diabetes Simulator: Technical Upgrade to Support Incorporation of Lispro, Aspart, and Glargine Insulin Analogues. J. Electr. Comput. Eng. 2011, 2011, 427196. [Google Scholar] [CrossRef] [Green Version]
- Thestrup, J.; Gergely, T.; Beck, P. Exploring new care models in diabetes management and therapy with a wireless mobile eHealth platform. In Wireless Mobile Communication and Healthcare: Second International ICST Conference, MobiHealth 2011, Kos Island, Greece, 5–7 October 2011; Revised Selected Papers; Nikita, K.S., Lin, J.C., Fotiadis, D.I., Arredondo Waldmeyer, M.T., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 203–210. [Google Scholar]
- Erzen, F.C.; Birol, G.; Cinar, A. Glucosim: A simulator for education on the dynamics of diabetes mellitus. In Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Istambul, Turkey, 25–28 October 2001; Volume 4, pp. 3163–3166. [Google Scholar] [CrossRef] [Green Version]
- Agar, B.U.; Eren, M.; Cinar, A. Glucosim: Educational software for virtual experiments with patients with type 1 diabetes. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 845–848. [Google Scholar] [CrossRef]
- Mougiakakou, S.G.; Prountzou, K.; Nikita, K.S. A Real Time Simulation Model of Glucose-Insulin Metabolism for Type 1 Diabetes Patients. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2005; pp. 298–301. [Google Scholar] [CrossRef]
- Bergman, R.N.; Phillips, L.S.; Cobelli, C. Physiologic evaluation of factors controlling glucose tolerance in man: Measurement of insulin sensitivity and beta-cell glucose sensitivity from the response to intravenous glucose. J. Clin. Investig. 1981, 68, 1456–1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cobelli, C.; Caumo, A.; Omenetto, M.; Sacca, L. Minimal model SG overestimation and SI underestimation: Improved accuracy by a Bayesian two-compartment model. Am. J. Physiol. 1999, 277, E481–E488. [Google Scholar]
- Hovorka, R.; Shojaee-Moradie, F.; Carroll, P.V.; Chassin, L.J.; Gowrie, I.J.; Jackson, N.C.; Tudor, R.S.; Umpleby, A.M.; Jones, R.H. Partitioning glucose distribution/trans-port, disposal, and endogenous production during IVGTT. Am. J. Physiol. 2002, 282, E992–E1007. [Google Scholar]
- Liu, C.; Vehí, J.; Avari, P.; Reddy, M.; Oliver, N.; Georgiou, P.; Herrero, P. Long-Term Glucose Forecasting Using a Physiological Model and Deconvolution of the Continuous Glucose Monitoring Signal. Sensors 2019, 19, 4338. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Avari, P.; Leal, Y.; Wos, M.; Sivasithamparam, K.; Georgiou, P.; Reddy, M.; Fernández-Real, J.M.; Martin, C.; Fernández-Balsells, M.; et al. A Modular Safety System for an Insulin Dose Recommender: A Feasibility Study. J. Diabetes Sci. Technol. 2019, 14, 87–96. [Google Scholar] [CrossRef]
- Sangeetha, S.; Sreepradha, C.; Sobana, S.; Bidisha, P.; Panda, R.C. Modeling and Control of the Glucose-Insulin-Glucagon System in Type I Diabetis Mellitus. ChemBioEng Rev. 2020, 3, 89–100. [Google Scholar] [CrossRef]
- Knopp, J.L.; Hardy, A.R.; Vergeer, S.; Chase, J.G. Modelling insulin adsorption in intravenous infusion sets in the intensive care unit. IFAC J. Syst. Control 2019, 8, 100042. [Google Scholar] [CrossRef]
- Visentin, R.; Schiavon, M.; Basu, R.; Basu, A.; Man, C.D.; Cobelli, C. Physiological models for artificial pancreas development. In The Artificial Pancreas: Current Situation and Future Directions, 1st ed.; Sánchez-Peña, R.S., Cherñavvsky, D.R., Eds.; Academic Press: Cambridge, MA, USA, 2019; Volume 1, pp. 123–152. [Google Scholar]
- Maas, A.H.; van der Molen, P.; van de Vijver, R.; Chen, W.; van Pul, C.; Cottaar, E.J.; van Riel, N.A.; Hilbers, P.A.; Haak, H.R. Concept Development of the Eindhoven Diabetes Education Simulator Project. Games Health J. 2016, 5, 120–127. [Google Scholar] [CrossRef]
- Ristau, R.A.; Yang, J.; White, J.R. Evaluation and Evolution of Diabetes Mobile Applications: Key Factors for Health Care Professionals Seeking to Guide Patients. Diabetes Spectr. 2013, 26, 211–215. Available online: http://spectrum.diabetesjournals.org/content/26/4/211.full.pdf (accessed on 17 September 2018). [CrossRef] [Green Version]
- El-Gayar, O.; Timsina, P.; Nawar, N.; Eid, W. Mobile Applications for Diabetes Self-Management: Status and Potential. J. Diabetes Sci. Technol. 2013, 7, 247–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chomutare, T.; Fernandez-Luque, L.; Arsand, E.; Hartvigsen, G. Features of mobile diabetes applications: Review of the literature and analysis of current applications compared against evidence-based guidelines. J. Med Internet Res. 2011, 13, e65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huckvale, K.; Adomaviciute, S.; Prieto, J.T.; Leow, M.K.S.; Car, J. Smartphone apps for calculating insulin dose: A systematic assessment. BMC Med. 2015, 13, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, M.; Wu, X.; Mao, J.; Wang, X.; Nie, M. T2DM Self-Management via Smartphone Applications: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0166718. [Google Scholar] [CrossRef] [PubMed]
- Garcia, E.; Martin, C.; Garcia, A.; Harrison, R.; Flood, D. Systematic Analysis of Mobile Diabetes Management Applications on Different Platforms. In Proceedings of the 7th Conference on Workgroup Human-Computer Interaction and Usability Engineering of the Austrian Computer Society: Information Quality in e-Health, Graz, Austria, 25–26 November 2011; Springer: Berlin/Heidelberg, Germany, 2011. USAB’11. pp. 379–396. [Google Scholar]
- Baskaran, V.; Prescod, F.; Dong, L. A Smartphone-Based Cloud Computing Tool for Managing Type 1 Diabetes in Ontarians. Can. J. Diabetes 2015, 39, 200–203. [Google Scholar] [CrossRef]
- Chomutare, T.; Tatara, N.; Arsand, E.; Hartvigsen, G. Designing a diabetes mobile application with social network support. In Studies in Health Technology and Informatics; IOS Press: Clifton, NJ, USA, 2013. [Google Scholar]
- Nguyen, H.D.; Jiang, X.; Poo, D.C.C. Designing a Social Mobile Platform for Diabetes Self-management: A Theory-Driven Perspective. In Social Computing and Social Media: 7th International Conference, SCSM 2015, Held as Part of HCI International 2015, Los Angeles, CA, USA, 2–7 August 2015, Proceedings; Meiselwitz, G., Ed.; Springer International Publishing: Cham, Switzerland, 2015; pp. 67–77. [Google Scholar]
- Garnweidner-Holme, L.M.; Borgen, I.; Garitano, I.; Noll, J.; Lukasse, M. Designing and Developing a Mobile Smartphone Application for Women with Gestational Diabetes Mellitus Followed-Up at Diabetes Outpatient Clinics in Norway. Healthcare 2015, 3, 310–323. [Google Scholar] [CrossRef] [Green Version]
- Borgen, I.; Garnweidner-Holme, L.M.; Jacobsen, A.F.; Bjerkan, K.; Fayyad, S.; Joranger, P.; Lilleengen, A.M.; Mosdøl, A.; Noll, J.; Småstuen, M.C.; et al. Smartphone application for women with gestational diabetes mellitus: A study protocol for a multicentre randomised controlled trial. BMJ Open 2017, 7, e013117. Available online: http://bmjopen.bmj.com/content/7/3/e013117.full.pdf (accessed on 12 December 2018). [CrossRef]
- Lloyd, B.; Groat, D.; Cook, C.; Kaufman, D.; Grando, A. IDECIDE: A mobile application for insulin dosing using an evidence based equation to account for patient preferences. In Studies in Health Technology and Informatics; IOS Press: Clifton, NJ, USA, 2015; Volume 216, pp. 93–97. [Google Scholar] [CrossRef]
- Keith-Hynes, P.; Mize, B.; Robert, A.; Place, J. The Diabetes Assistant: A Smartphone-Based System for Real-Time Control of Blood Glucose. Electronics 2014, 3, 609–623. [Google Scholar] [CrossRef] [Green Version]
- González, A.A.; Voos, H.; Darouach, M. Glucose-Insulin System Based on Minimal Model: A Realistic Approach. In Proceedings of the 2015 17th UKSIM-AMSS International Conference on Modelling and Simulation, Cambridge, UK, 25–27 March 2015; IEEE Computer Society: Washington, DC, USA, 2015. UKSIM ’15. pp. 55–60. [Google Scholar] [CrossRef]
- Sorensen, J.T. A Physiologic Model of Glucose Metabolism in Man and Its Use to Design and Assess Improved Insulin Therapies for Diabetes. Ph.D. Thesis, Massachusetts Institute of Technology. Dept. of Chemical Engineering, Berkeley, CA, USA, 1985. [Google Scholar]
- Hernández-Ordoñez, M.; Campos-Delgado, D. An extension to the compartmental model of type 1 diabetic patients to reproduce exercise periods with glycogen depletion and replenishment. J. Biomech. 2008, 41, 744–752. [Google Scholar] [CrossRef]
- Berger, M.; Rodbard, D. Computer simulation of plasma insulin and glucose dynamics after subcutaneous insulin injection. Diabetes Care 1989, 12, 725–736. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, E.; Deutsch, T. A physiological model of glucose-insulin interaction in type 1 diabetes mellitus. J. Biomed. Eng. 1992, 14, 235–242. [Google Scholar] [CrossRef]
- Wilinska, M.E.; Chassin, L.J.; Schaller, H.C.; Schaupp, L.; Pieber, T.R.; Hovorka, R. Insulin kinetics in type-1 diabetes: Continuous and bolus delivery of rapid acting insulin. IEEE Trans. Biomed. Eng. 2005, 52, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Jahoda, P. MPAndroidChart. 2016. Available online: https://github.com/PhilJay/MPAndroidChart (accessed on 15 November 2018).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Processor | RAM | Android Version |
|---|---|---|---|
| Galaxy S2 | Dual-core 1.2 GHz Cortex-A9 | 1 GB | 4.1 |
| Galaxy S4 | Dual-core 1.7 GHz Krait 300 | 1.5 GB | 5.0.1 |
| Polaroid Tab | Dual-core 1.0 GHz Broadcom 21663 | 1 GB | 4.2.2 |
| Galaxy Tab 10.1 | Quad-core 2.3 GHz Krait 400 | 3 GB | 5.1.1 |
| LG G3 Stylus | Quad-core 1.3 GHz Cortex-A7 | 1 GB | 5.0.2 |
| Meal Model | |
|---|---|
| Breakfast time | 7:00 AM |
| Lunch time | 1:00 PM |
| Dinner time | 7:00 PM |
| Breakfast CHO (g) | 97.91 |
| Lunch CHO (g) | 138.97 |
| Dinner CHO (g) | 59.32 |
| Insulin Model | |
| Rapid effect insulin type | Lispro |
| Prolonged effect insulin Type | NPH |
| Rapid effect insulin units at breakfast | 2 |
| Rapid effect insulin units at lunch | 2 |
| Rapid effect insulin units at dinner | 2 |
| Prolonged effect insulin units at breakfast | 3 |
| Prolonged effect insulin units at dinner | 3 |
| Exercise Model | |
| Intensity | Light |
| Duration | 10 min |
| Start time | 9:00 AM |
| Routine | Monday checked |
| Exp | Meal | Insulin Dossification | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Carbohydrate Grams Intake | Rapid Effect | Prolongated Effect | |||||||||
| B-CHO | L-CHO | D-CHO | Type | B-u | L-u | D-u | Type | B-u | D-u | ||
| 1 | 97.91 | 138.97 | 59.32 | Lispro | 2 | 2 | 2 | NPH | 3 | 3 | |
| 2 | 49.85 | 69.48 | 29.66 | Lispro | 2 | 2 | 2 | NPH | 3 | 3 | |
| 3 | 97.91 | 138.97 | 59.32 | Lispro | 4 | 4 | 4 | NPH | 6 | 6 | |
| 4 | 49.85 | 69.48 | 29.66 | Lispro | 4 | 4 | 4 | NPH | 6 | 6 | |
| Gender | Age | Previous Knowledge of Mobiles Apps for Diabetes Treatment | |||
|---|---|---|---|---|---|
| Male | Female | 15–19 | 20–25 | Yes | No |
| 76.9% | 23.1% | 38.5% | 61.5% | 15.4% | 84.6% |
| Question | 1 (No)% | 2 (Rather No)% | 3 (Do Not Know)% | 4 (Rather Yes)% | 5 (Yes)% |
|---|---|---|---|---|---|
| (1) Are the user interface controls adequate to the type of data required by the app? | 15.4% | 15.4% | 15.4% | 38.5% | 15.4% |
| (2) Is the application useful? | 23.1% | 0% | 0% | 0% | 76.9% |
| (3) Are the generated graphs easy to understand? | 7.7% | 0% | 23.1% | 46.2% | 23.1% |
| (4) Do the application’s user interface controls allow to manage the application in an ease way? | 0% | 7.7% | 7.7% | 46.2% | 38.5% |
| (5) How difficult has been the use of the app? | 15.4% | 38.5% | 30.8% | 15.4% | 0% |
| (6) Does the application motivate to study more in depth the phenomena? | 0% | 0% | 15.4% | 46.2% | 38.5% |
| (7) Will you reuse the app? | 0% | 7.7% | 7.7% | 15.4% | 69.2% |
| (8) Do you consider that current app can be improved? | 7.7% | 0% | 0% | 23.1% | 69.2% |
| (9) Do you consider appropriate the functionality of the application for learning the glucose levels variability? | 0% | 0% | 7.7% | 38.5% | 53.8% |
| (10) Do you consider the mobile application are sufficient to assess whether in the future you would like to participate in similar experiences with mobile apps? | 0% | 0% | 23.1% | 38.5% | 38.5% |
| Device | Simulation Time Duration | |||
|---|---|---|---|---|
| 4 Days | 1 Week | 2 Weeks | 3 Weeks | |
| Polaroid Tab | 12.30 | 13.53 | 16.24 | 21.11 |
| Galaxy S2 | 9.53 | 10.97 | 13.16 | 18.16 |
| Galaxy S4 | 6.53 | 7.64 | 9.17 | 12.84 |
| LG G3 Stylus | 5.53 | 6.59 | 7.90 | 11.30 |
| Galaxy Tab 10.1 | 5.53 | 6.70 | 8.04 | 11.73 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Ordoñez, M.; Nuño-Maganda, M.A.; Calles-Arriaga, C.A.; Rodríguez-León, A.; Ovando-Chacon, G.E.; Salazar-Hernández, R.; Montaño-Rivas, O.; Canseco-Cortinas, J.M. Medical Assistant Mobile Application for Diabetes Control by Simulating a Compartmental Model. Appl. Sci. 2020, 10, 6846. https://doi.org/10.3390/app10196846
Hernández-Ordoñez M, Nuño-Maganda MA, Calles-Arriaga CA, Rodríguez-León A, Ovando-Chacon GE, Salazar-Hernández R, Montaño-Rivas O, Canseco-Cortinas JM. Medical Assistant Mobile Application for Diabetes Control by Simulating a Compartmental Model. Applied Sciences. 2020; 10(19):6846. https://doi.org/10.3390/app10196846
Chicago/Turabian StyleHernández-Ordoñez, Martín, Marco Aurelio Nuño-Maganda, Carlos Adrián Calles-Arriaga, Abelardo Rodríguez-León, Guillermo Efren Ovando-Chacon, Rolando Salazar-Hernández, Omar Montaño-Rivas, and José Margarito Canseco-Cortinas. 2020. "Medical Assistant Mobile Application for Diabetes Control by Simulating a Compartmental Model" Applied Sciences 10, no. 19: 6846. https://doi.org/10.3390/app10196846
APA StyleHernández-Ordoñez, M., Nuño-Maganda, M. A., Calles-Arriaga, C. A., Rodríguez-León, A., Ovando-Chacon, G. E., Salazar-Hernández, R., Montaño-Rivas, O., & Canseco-Cortinas, J. M. (2020). Medical Assistant Mobile Application for Diabetes Control by Simulating a Compartmental Model. Applied Sciences, 10(19), 6846. https://doi.org/10.3390/app10196846