Ultrasound-Guided Percutaneous Needle Electrolysis and Rehab and Reconditioning Program for Rectus Femoris Muscle Injuries: A Cohort Study with Professional Soccer Players and a 20-Week Follow-Up

 , , , and
, , , and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
3. Intervention Protocol
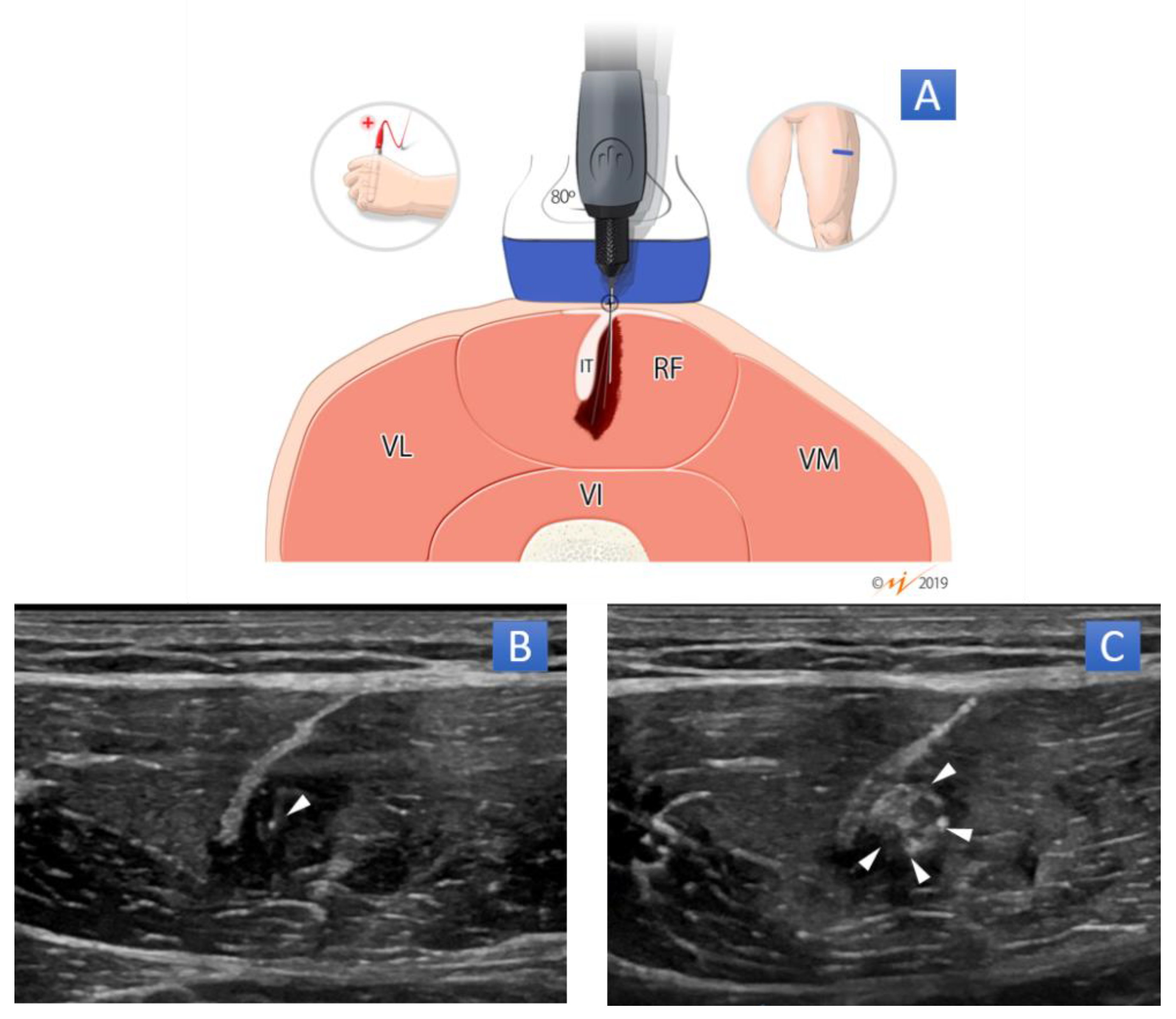
3.1. US-Guided Percutaneous Needle Electrolysis (PNE)
3.2. Rehab and Reconditioning Program (RRP)
4. Variables and Data Analysis
4.1. Return to Training and Return to Play
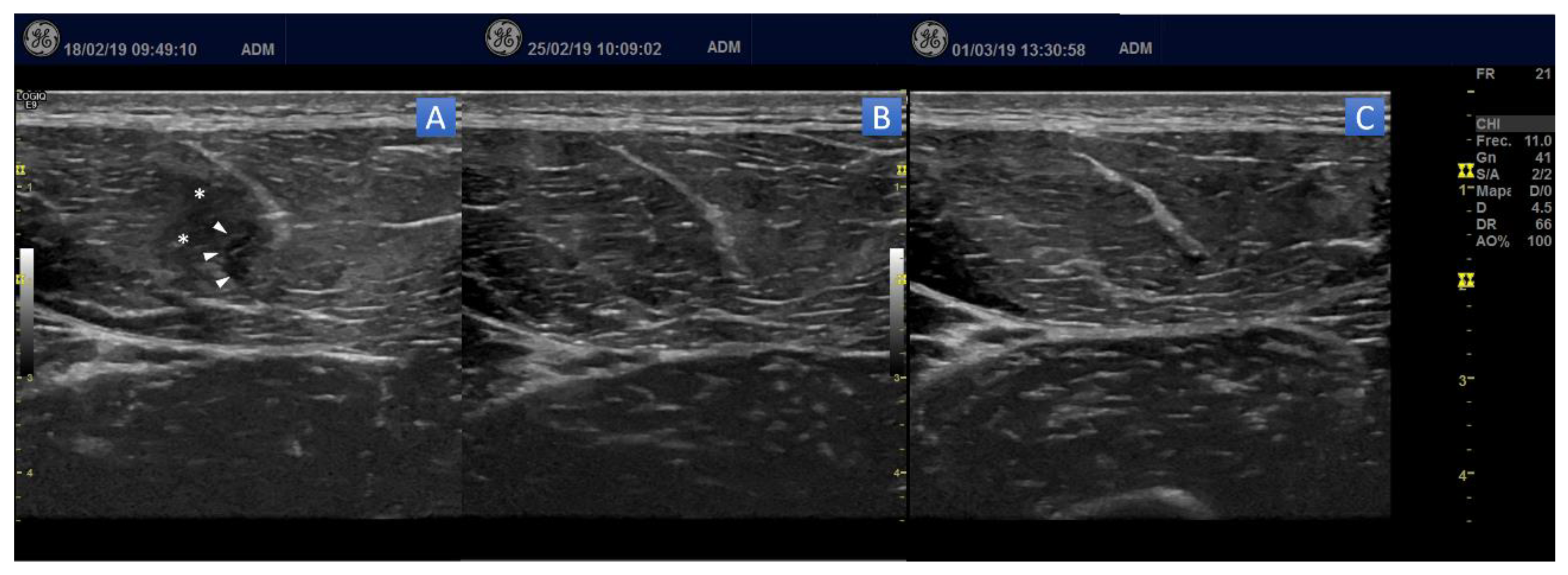
4.2. Ultrasound
4.3. GPS Match Variables
4.4. Statistical Analysis
4.5. Adverse Events
4.6. Follow-Up
5. Results
5.1. Ultrasound
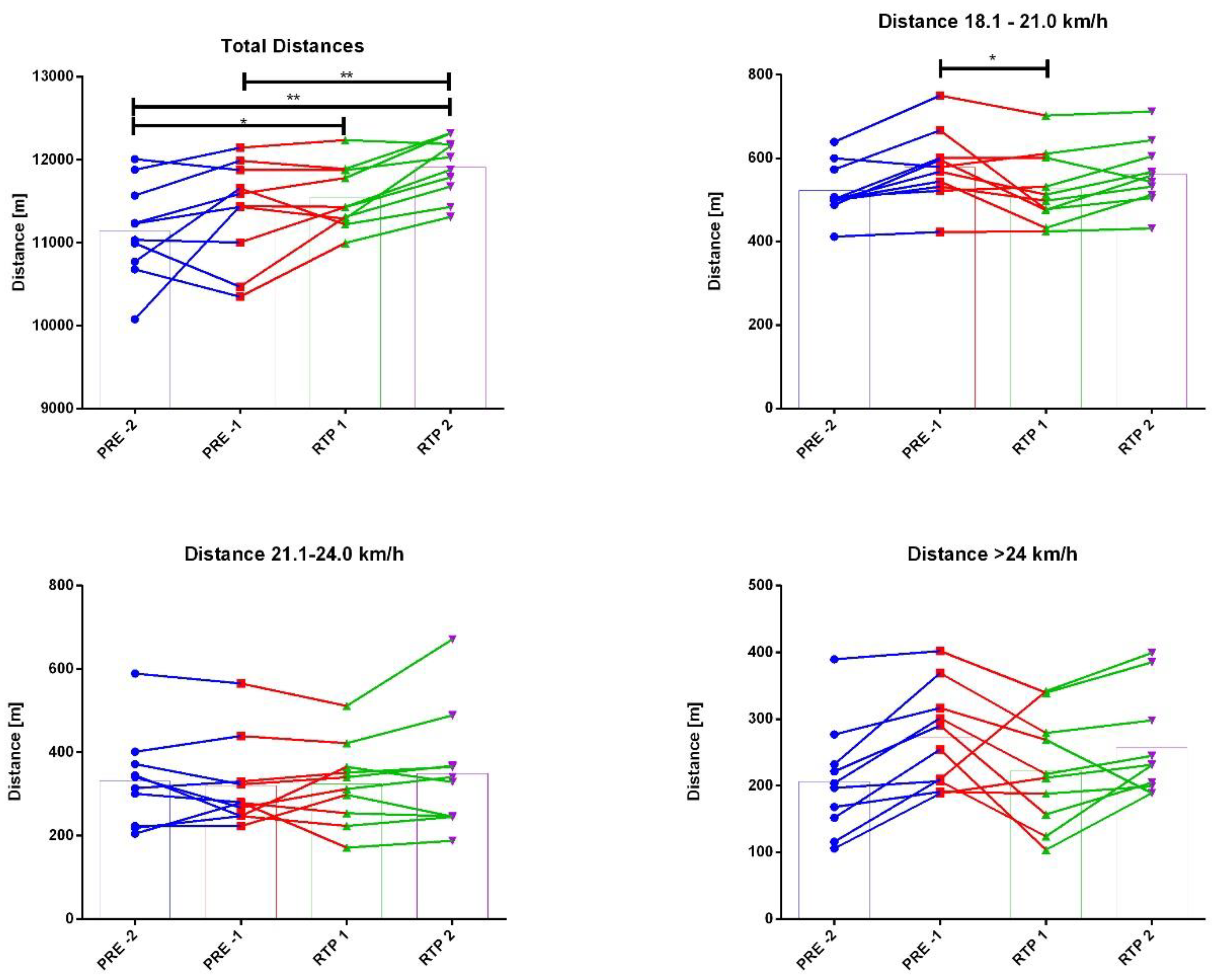
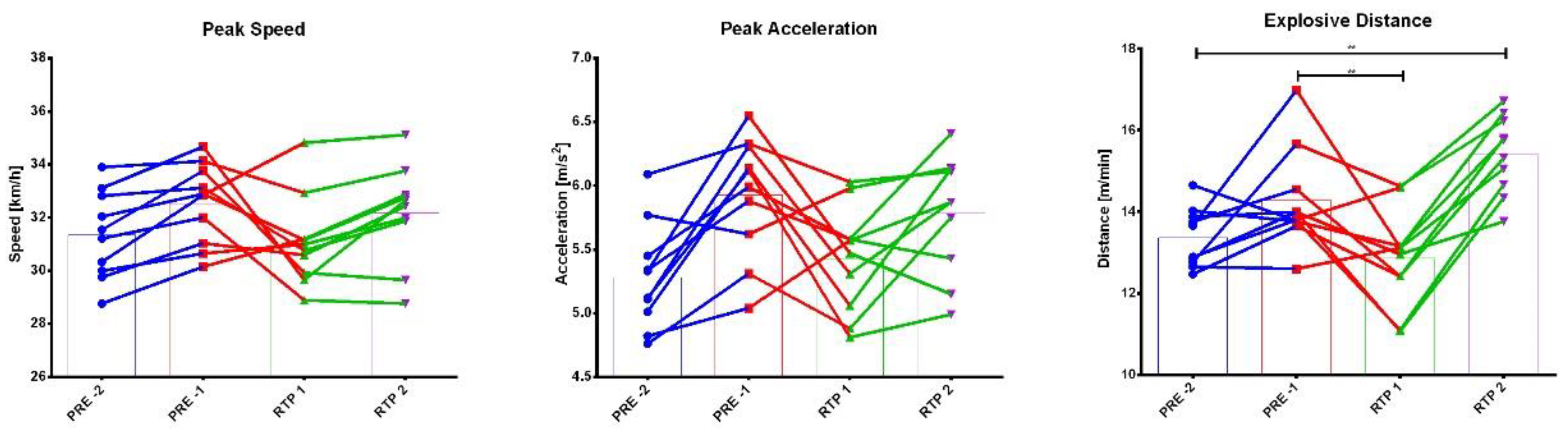
5.2. GPS Parameters
5.3. Adverse Events
5.4. Follow-Up
6. Discussions
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rivilla-García, J.; Calvo, L.C.; Jiménez-Rubio, S.; Paredes-Hernández, V.; Muñoz, A.; Van den Tillaar, R.; Navandar, A. Characteristics of very high intensity runs of soccer players in relation to their playing position and playing half in the 2013-14 Spanish La Liga Season. J. Hum. Kinet. 2019, 66, 213–222. [Google Scholar] [CrossRef] [Green Version]
- Dellal, A.; Chamari, K.; Wong, D.P.; Ahmaidi, S.; Keller, D.; Barros, R.; Bisciotti, G.N.; Carling, C. Comparison of physical and technical performance in European soccer match-play: FA Premier League and La Liga. Eur. J. Sport Sci. 2011, 11, 51–59. [Google Scholar] [CrossRef]
- Taylor, J.B.; Wright, A.A.; Dischiavi, S.L.; Townsend, M.A.; Marmon, A.R. Activity demands during multi-directional team sports: A systematic review. Sports Med. 2017, 47, 2533–2551. [Google Scholar] [CrossRef]
- Mallo, J.; Mena, E.; Nevado, F.; Paredes, V. Physical Demands of Top-Class Soccer Friendly Matches in Relation to a Playing Position Using Global Positioning System Technology. J. Hum. Kinet. 2015, 47, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Previous injury as a risk factor for injury in elite football: A prospective study over two consecutive seasons. Br. J. Sports Med. 2006, 40, 767–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Beijsterveldt, A.; van de Port, I.G.; Vereijken, A.; Backx, F. Risk factors for hamstring injuries in male soccer players: A systematic review of prospective studies. Scand. J. Med. Sci. Sports 2013, 23, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Bowen, L.; Gross, A.S.; Gimpel, M.; Bruce-Low, S.; Li, F.-X. Spikes in acute: Chronic workload ratio (ACWR) associated with a 5–7 times greater injury rate in English Premier League football players: A comprehensive 3-year study. Br. J. Sports Med. 2020, 54, 731–738. [Google Scholar] [CrossRef] [Green Version]
- Garrett, W.E., Jr. Muscle strain injuries. Am. J. Sports Med. 1996, 24, S2–S8. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football. Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Hallen, A.; Ekstrand, J. Return to play following muscle injuries in professional footballers. J. Sports Sci. 2014, 32, 1229–1236. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Risk Factors for Lower Extremity Muscle Injury in Professional Soccer: The UEFA Injury Study. Am. J. Sports Med. 2013, 41, 327–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Hagglund, M.; Walden, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, A. The relative isometric strength of type I and type II muscle fibres in the human quadriceps. Clin. Physiol. 1984, 4, 23–32. [Google Scholar] [CrossRef]
- Neumann, D.A. Kinesiology of the hip: A focus on muscular actions. J. Orthop. Sports Phys. Ther. 2010, 40, 82–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendiguchia, J.; Alentorn-Geli, E.; Brughelli, M. Hamstring strain injuries: Are we heading in the right direction? Br. J. Sports Med. 2012, 46, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Lewis, C.L.; Sahrmann, S.A.; Moran, D.W. Anterior hip joint force increases with hip extension, decreased gluteal force, or decreased iliopsoas force. J. Biomech. 2007, 40, 3725–3731. [Google Scholar] [CrossRef] [Green Version]
- Lewindon, D.; Lee, J. Muscle injuries. In Sports Injury Prevention and Rehabilitation. Integrating Medicine and Science for Performance Solutions; Joyce, D., Lewindon, D., Eds.; Routledge: Abingdon, UK, 2016; pp. 106–120. [Google Scholar]
- Svensson, K.; Eckerman, M.; Alricsson, M.; Magounakis, T.; Werner, S. Muscle injuries of the dominant or non-dominant leg in male football players at elite level. Br. J. Sports Med. 2016, 50, e4. [Google Scholar] [CrossRef]
- Ueblacker, P.; Mueller-Wohlfahrt, H.-W.; Ekstrand, J. Epidemiological and clinical outcome comparison of indirect (‘strain’) versus direct (‘contusion’) anterior and posterior thigh muscle injuries in male elite football players: UEFA Elite League study of 2287 thigh injuries (2001–2013). Br. J. Sports Med. 2015, 49, 1461–1465. [Google Scholar] [CrossRef] [Green Version]
- Eirale, C.; Farooq, A.; Smiley, F.A.; Tol, J.L.; Chalabi, H. Epidemiology of football injuries in Asia: A prospective study in Qatar. J. Sci. Med. Sport 2013, 16, 113–117. [Google Scholar] [CrossRef]
- Orchard, J.W.; Jomaa, M.C.; Orchard, J.J.; Rae, K.; Hoffman, D.T.; Reddin, T.; Driscoll, T. Fifteen-week window for recurrent muscle strains in football: A prospective cohort of 3600 muscle strains over 23 years in professional Australian rules football. Br. J. Sports Med. 2020, 54, 1103–1107. [Google Scholar] [CrossRef]
- Hägglund, M.; Waldén, M.; Bengtsson, H.; Ekstrand, J. Re-injuries in professional football: The UEFA Elite Club Injury Study. In Return to Play in Football; Springer: Berlin/Heidelberg, Germany, 2018; pp. 953–962. [Google Scholar]
- Bubnov, R.; Yevseenko, V.; Semeniv, I. Ultrasound guided injections of Platelets Rich Plasma for muscle injury in professional athletes. Comparative study. Med. Ultrason. 2013, 15, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Chellini, F.; Tani, A.; Zecchi-Orlandini, S.; Sassoli, C. Influence of Platelet-Rich and Platelet-Poor Plasma on Endogenous Mechanisms of Skeletal Muscle Repair/Regeneration. Int. J. Mol. Sci. 2019, 20, 683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariani, E.; Pulsatelli, L. Platelet concentrates in musculoskeletal medicine. Int. J. Mol. Sci. 2020, 21, 1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valera-Garrido, F.; Minaya-Muñoz, F. Fundamentos y principios de la electrolisis percutánea musculoesquelética. In Fisioterapia Invasiva, 2nd ed.; Elsevier: Barcelona, Spain, 2016; Chapter 16; pp. 390–391. [Google Scholar]
- Valera-Garrido, F.; Minaya-Muñoz, F.; Sánchez-Ibáñez, J.M.; García-Palencia, P.; Valderrama-Canales, F.; Medina-Mirapeix, F.; Polidori, F. Comparison of the acute inflammatory response and proliferation of dry needling and electrolysis percutaneous intratissue in healthy rat Achilles tendons. Br. J. Sports Med. 2013, 47, e2. [Google Scholar] [CrossRef]
- Abat, F.; Sánchez-Sánchez, J.L.; Martín-Nogueras, A.M.; Calvo-Arenillas, J.I.; Yajeya, J.; Méndez-Sánchez, R.; Monllau, J.C.; Gelber, P.-E. Randomized controlled trial comparing the effectiveness of the ultrasound-guided galvanic electrolysis technique (USGET) versus conventional electro-physiotherapeutic treatment on patellar tendinopathy. J. Exp. Orthop. 2016, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Valera-Garrido, F.; Minaya-Muñoz, F.; Medina-Mirapeix, F. Ultrasound-guided percutaneous needle electrolysis in chronic lateral epicondylitis: Short-term and long-term results. Acupunct. Med. 2014, 32, 446–454. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Huguet, M.; Góngora-Rodríguez, J.; Rodríguez-Huguet, P.; Ibañez-Vera, A.J.; Rodríguez-Almagro, D.; Martín-Valero, R.; Díaz-Fernández, Á.; Lomas-Vega, R. Effectiveness of Percutaneous Electrolysis in Supraspinatus Tendinopathy: A Single-Blinded Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1837. [Google Scholar] [CrossRef]
- Fernández-Rodríguez, T.; Fernández-Rolle, Á.; Truyols-Domínguez, S.; Benítez-Martínez, J.C.; Casaña-Granell, J. Prospective randomized trial of electrolysis for chronic plantar heel pain. Foot Ankle Int. 2018, 39, 1039–1046. [Google Scholar] [CrossRef]
- Abat, F.; Valles, S.-L.; Gelber, P.-E.; Polidori, F.; Jorda, A.; García-Herreros, S.; Monllau, J.-C.; Sanchez-Ibáñez, J.-M. An experimental study of muscular injury repair in a mouse model of notexin-induced lesion with EPI® technique. BMC Sports Sci. Med. Rehabil. 2015, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Santafé, M.; Margalef, R.; Minaya-Muñoz, F.; Valera-Garrido, F. Action of galvanic current on an experimentally generated muscle lesion: Preliminary findings. Rev. Fisioter. Invasiva 2019, 2, 108–109. [Google Scholar]
- Valera-Garrido, F.; Minaya-Muñoz, F.; Sánchez-Ibáñez, J.M. Efecto de la electrolisis percutánea en las roturas musculares agudas. Caso clínico de la lesión de “tennis leg”. In Proceedings of the II Congreso Regional de Fisioterapia de la Región de Murcia, Murcia, Spain, 3–4 May 2012. [Google Scholar]
- Jiménez-Rubio, S.; Valera-Garrido, F.; Minaya-Muñoz, F.; Navandar, A. Ultrasound-guided percutaneous needle electrolysis and rehab & reconditioning program following a hamstring injury reduces return to play time in professional soccer players: A case series. Rev. Fisioter. Invasiva 2020, 3, 2–6. [Google Scholar]
- Brughelli, M.; Nosaka, K.; Cronin, J. Application of eccentric exercise on an Australian Rules football player with recurrent hamstring injuries. Phys. Ther. Sport 2009, 10, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Mendiguchia, J.; Alentorn-Geli, E.; Idoate, F.; Myer, G.D. Rectus femoris muscle injuries in football: A clinically relevant review of mechanisms of injury, risk factors and preventive strategies. Br. J. Sports Med. 2013, 47, 359–366. [Google Scholar] [CrossRef]
- Jiménez-Rubio, S.; Navandar, A.; Rivilla-García, J.; Paredes-Hernández, V. Validity of an on-Field Readaptation Program Following a Hamstring Injury in Professional Soccer. J. Sport Rehabil. 2019, 28, 1–7. [Google Scholar] [CrossRef]
- Mendiguchia, J.; Martinez-Ruiz, E.; Edouard, P.; Morin, J.B.; Martinez-Martinez, F.; Idoate, F.; Mendez-Villanueva, A. A Multifactorial, Criteria-Based Progressive Algorithm for Hamstring Injury Treatment. Med. Sci. Sports Exerc. 2017. [Google Scholar] [CrossRef]
- van Dyk, N.; Bahr, R.; Whiteley, R.; Tol, J.L.; Kumar, B.D.; Hamilton, B.; Farooq, A.; Witvrouw, E. Hamstring and Quadriceps Isokinetic Strength Deficits Are Weak Risk Factors for Hamstring Strain Injuries: A 4-Year Cohort Study. Am. J. Sports Med. 2016, 44, 1789–1795. [Google Scholar] [CrossRef]
- van Dyk, N.; Farooq, A.; Bahr, R.; Witvrouw, E. Hamstring and ankle flexibility deficits are weak risk factors for hamstring injury in professional soccer players: A prospective cohort study of 438 players including 78 injuries. Am. J. Sports Med. 2018, 46, 2203–2210. [Google Scholar] [CrossRef] [Green Version]
- Guillodo, Y.; Bouttier, R.; Saraux, A. Value of sonography combined with clinical assessment to evaluate muscle injury severity in athletes. J. Athl. Train. 2011, 46, 500–504. [Google Scholar] [CrossRef] [Green Version]
- Mohamad, H.A.S.; Ashril, Y.; Mohamed, M.A.R. Pattern of muscle injuries and predictors of return-to-play duration among Malaysian athletes. Singap. Med. J. 2013, 54, 587–591. [Google Scholar]
- Renoux, J.; Brasseur, J.-L.; Wagner, M.; Frey, A.; Folinais, D.; Dibie, C.; Maiza, D.; Crema, M.D. Ultrasound-detected connective tissue involvement in acute muscle injuries in elite athletes and return to play: The French National Institute of Sports (INSEP) study. J. Sci. Med. Sport 2019, 22, 641–646. [Google Scholar] [CrossRef]
- Hall, M.M. Return to play after thigh muscle injury: Utility of serial ultrasound in guiding clinical progression. Curr. Sports Med. Rep. 2018, 17, 296–301. [Google Scholar] [CrossRef]
- Peetrons, P. Ultrasound of muscles. Eur. Radiol. 2002, 12, 35–43. [Google Scholar] [CrossRef]
- Valera-Garrido, F.; Minaya-Muñoz, F. Aplicaciones clínicas de la electrolisis percutánea. In Fisioterapia Invasiva, 2nd ed.; Elsevier: Barcelona, Spain, 2016; Chapter 17; p. 425. [Google Scholar]
- Hegyi, A.; Gonçalves, B.A.; Finni, T.; Cronin, N.J. Individual Region-and Muscle-specific Hamstring Activity at Different Running Speeds. Med. Sci. Sports Exerc. 2019, 51, 2274–2285. [Google Scholar] [CrossRef]
- Oranchuk, D.J.; Storey, A.G.; Nelson, A.R.; Cronin, J.B. Scientific Basis for Eccentric Quasi-Isometric Resistance Training: A Narrative Review. J. Strength Cond. Res. 2019, 33, 2846–2859. [Google Scholar] [CrossRef]
- King, E.; Franklyn-Miller, A.; Richter, C.; O’Reilly, E.; Doolan, M.; Moran, K.; Strike, S.; Falvey, É. Clinical and biomechanical outcomes of rehabilitation targeting intersegmental control in athletic groin pain: Prospective cohort of 205 patients. Br. J. Sports Med. 2018, 52, 1054–1062. [Google Scholar] [CrossRef]
- Serner, A.; Weir, A.; Tol, J.L.; Thorborg, K.; Lanzinger, S.; Otten, R.; Hölmich, P. Return to Sport After Criteria-Based Rehabilitation of Acute Adductor Injuries in Male Athletes: A Prospective Cohort Study. Orthop. J. Sports Med. 2020, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Taberner, M.; Allen, T.; Constantine, E.; Cohen, D. From control to chaos to competition. Building a pathway for return to performance following ACL reconstruction. Aspetar Sports Med. J. 2020, 9, 84–94. [Google Scholar]
- Schache, A.G.; Dorn, T.W.; Williams, G.P.; Brown, N.A.; Pandy, M.G. Lower-limb muscular strategies for increasing running speed. J. Orthop. Sports Phys. Ther. 2014, 44, 813–824. [Google Scholar] [CrossRef] [Green Version]
- Carlesso, L.C.; Macdermid, J.C.; Santaguida, L.P. Standardization of adverse event terminology and reporting in orthopaedic physical therapy: Application to the cervical spine. J. Orthop. Sports Phys. Ther. 2010, 40, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Balius, R.; Maestro, A.; Pedret, C.; Estruch, A.; Mota, J.; Rodriguez, L.; García, P.; Mauri, E. Central aponeurosis tears of the rectus femoris: Practical sonographic prognosis. Br. J. Sports Med. 2009, 43, 818–824. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Rubio, S.; Navandar, A.; Rivilla-García, J.; Paredes-Hernández, V.; Gómez-Ruano, M.Á. Improvements in Match-Related Physical Performance of Professional Soccer Players After the Application of an on-Field Training Program for Hamstring Injury Rehabilitation. J. Sport Rehabil. 2019, 1, 1. [Google Scholar] [CrossRef]
- Järvinen, T.A.; Järvinen, M.; Kalimo, H. Regeneration of injured skeletal muscle after the injury. Muscles Ligaments Tendons J. 2013, 3, 337. [Google Scholar] [CrossRef] [Green Version]
- Knowles, B. Reconditioning. A performance-based response to an injury. In Sports Injury Prevention and Rehabilitation Integrating Medicine and Science for Performance Solutions; Joyce, D., Lewindon, D., Eds.; Routledge: London, UK; New York, NY, USA, 2016; pp. 3–10. [Google Scholar]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle. Sports Med. 2013, 43, 927–954. [Google Scholar] [CrossRef]
- Valera-Garrido, F.; Minaya-Muñoz, F.; Ramírez-Martínez, P.; Medina-i-Mirapeix, F. Adverse effects associated to the application of ultrasound-guided percutaneous needle electrolysis. Rev. Fisioter. Invasiva 2019, 2, 115–116. [Google Scholar]
- Mathes, T.; Pieper, D. Clarifying the distinction between case series and cohort studies in systematic reviews of comparative studies: Potential impact on body of evidence and workload. BMC Med. Res. Methodol. 2017, 17, 107. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Players (n) | Player Position | Age (Years) | Mass (Kg) | Height (cm) | Injury Mechanism | Dominant Leg | Phenotype |
|---|---|---|---|---|---|---|---|
| 1 | Full-Back | 32 | 74 | 179 | Kicking | D | Caucasian |
| 2 | Midfielder | 28 | 77 | 184 | Sprint | D | Caucasian |
| 3 | Midfielder | 31 | 76 | 181 | CoD * | ND | Caucasian |
| 4 | Central Defender | 28 | 70 | 177 | Kicking | D | Black |
| 5 | Winger | 24 | 74 | 180 | Kicking | D | Caucasian |
| 6 | Full-Back | 25 | 75 | 181 | Kicking | D | Caucasian |
| 7 | Stricker | 27 | 73 | 179 | Sprint | D | Caucasian |
| 8 | Stricker | 26 | 69 | 176 | Sprint | ND | Caucasian |
| 9 | Winger | 27 | 70 | 180 | Kicking | D | Caucasian |
| 10 | Winger | 32 | 72 | 181 | Kicking | D | Caucasian |
| 11 | Central Defender | 31 | 81 | 189 | CoD | D | Caucasian |
| 12 | Midfielder | 30 | 78 | 185 | Kicking | D | Caucasian |
| 13 | Midfielder | 22 | 74 | 180 | Kicking | D | Caucasian |
| Indoor Phase | Date | Description | Volume (Time) |
|---|---|---|---|
| Phase 1 (ROM & Strength) | 24 h-Post PNE | Pelvic Assessment
| 40′ |
| 48 h-Post PNE | 24 h Post PNE + Strength Training Eccentric-quasi-isometric (EQI)
| 40′ | |
| 72 h-Post PNE | 48 h Post PNE + Strength Training (ISO + SSC) + Absorption/Landings (Frontal Plane)
| 45′ | |
| 96 h-Post PNE | 72 h Post PNE + Strength Training + Absorption (Multiplane)
| 50′ | |
Exit Criteria
| |||
| Indoor Phase | Date | Description | Volume (Time) |
|---|---|---|---|
| Phase 2 (Development of movement skills) | Days 5–7 Post PNE | Linear Running Performance + Rate of moment production and absorption (Multi-Plane-Plyos) (18–20 contacts)
| 50′ |
Multidirectional performance + Rate of moment production and absorption (Multi-Plane-Plyos) (18–20 contacts) + Movement Skills
| 60′ | ||
Return to Running
| |||
Exit Criteria
| |||
| On Field Phase | Date | Description | Volume (Time) |
|---|---|---|---|
| Phase 3 | Day 9–10 Post PNE (OF-1) |
| 25′ |
| Day 11 Post PNE (OF-2) |
| 35′ | |
| Day 12 Post PNE |
| 20′ | |
| Day 13–14 Post PNE (OF-3) |
| 40′ | |
| Day 15 Post PNE (OF-4) |
| 50′ | |
Exit Criteria
| |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valera-Garrido, F.; Jiménez-Rubio, S.; Minaya-Muñoz, F.; Estévez-Rodríguez, J.L.; Navandar, A. Ultrasound-Guided Percutaneous Needle Electrolysis and Rehab and Reconditioning Program for Rectus Femoris Muscle Injuries: A Cohort Study with Professional Soccer Players and a 20-Week Follow-Up. Appl. Sci. 2020, 10, 7912. https://doi.org/10.3390/app10217912
Valera-Garrido F, Jiménez-Rubio S, Minaya-Muñoz F, Estévez-Rodríguez JL, Navandar A. Ultrasound-Guided Percutaneous Needle Electrolysis and Rehab and Reconditioning Program for Rectus Femoris Muscle Injuries: A Cohort Study with Professional Soccer Players and a 20-Week Follow-Up. Applied Sciences. 2020; 10(21):7912. https://doi.org/10.3390/app10217912
Chicago/Turabian StyleValera-Garrido, Fermín, Sergio Jiménez-Rubio, Francisco Minaya-Muñoz, José Luis Estévez-Rodríguez, and Archit Navandar. 2020. "Ultrasound-Guided Percutaneous Needle Electrolysis and Rehab and Reconditioning Program for Rectus Femoris Muscle Injuries: A Cohort Study with Professional Soccer Players and a 20-Week Follow-Up" Applied Sciences 10, no. 21: 7912. https://doi.org/10.3390/app10217912
APA StyleValera-Garrido, F., Jiménez-Rubio, S., Minaya-Muñoz, F., Estévez-Rodríguez, J. L., & Navandar, A. (2020). Ultrasound-Guided Percutaneous Needle Electrolysis and Rehab and Reconditioning Program for Rectus Femoris Muscle Injuries: A Cohort Study with Professional Soccer Players and a 20-Week Follow-Up. Applied Sciences, 10(21), 7912. https://doi.org/10.3390/app10217912