
Study of the Antimicrobial Effect of an Ethanolic Extract of Propolis in Periodontal Disease


 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethanolic Extract of Spanish Propolis
2.2. Total Phenolic Assay
2.3. Total Flavonoid Assay
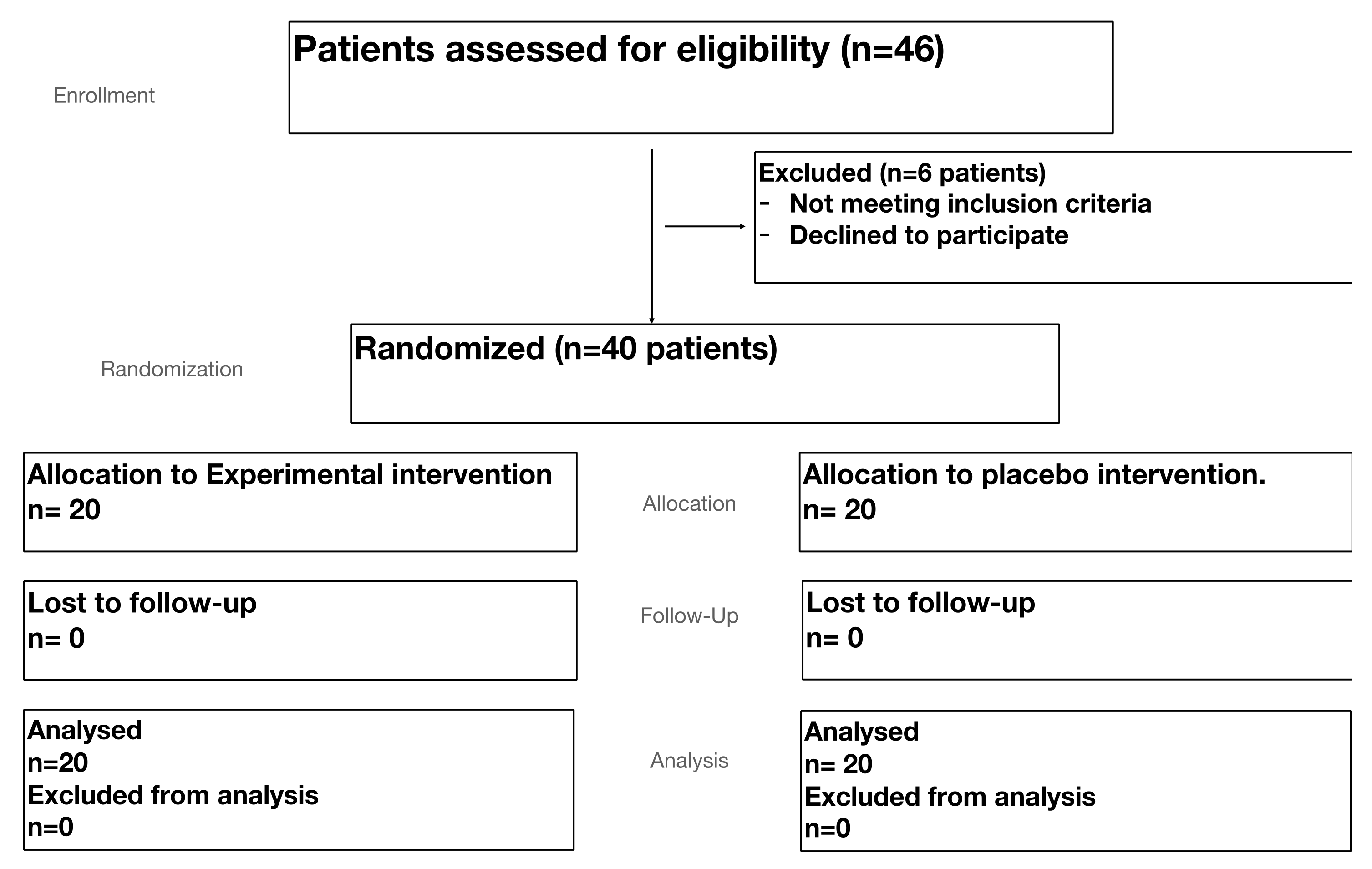
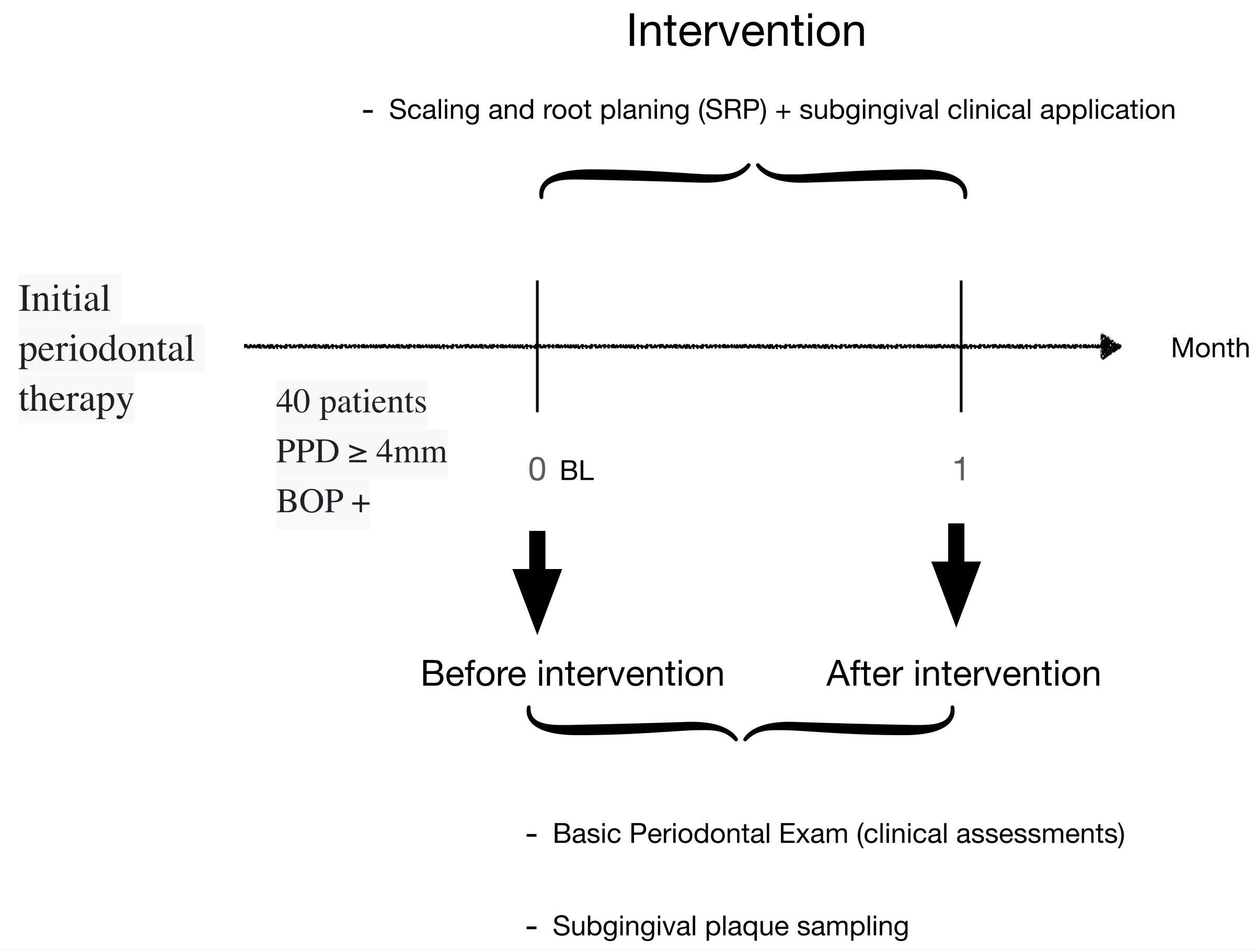
2.4. Participants and Enrolment
2.5. Microbial Sampling
2.6. DNA Extraction and Analysis
2.7. PCR Amplification
2.8. Statistical Analysis
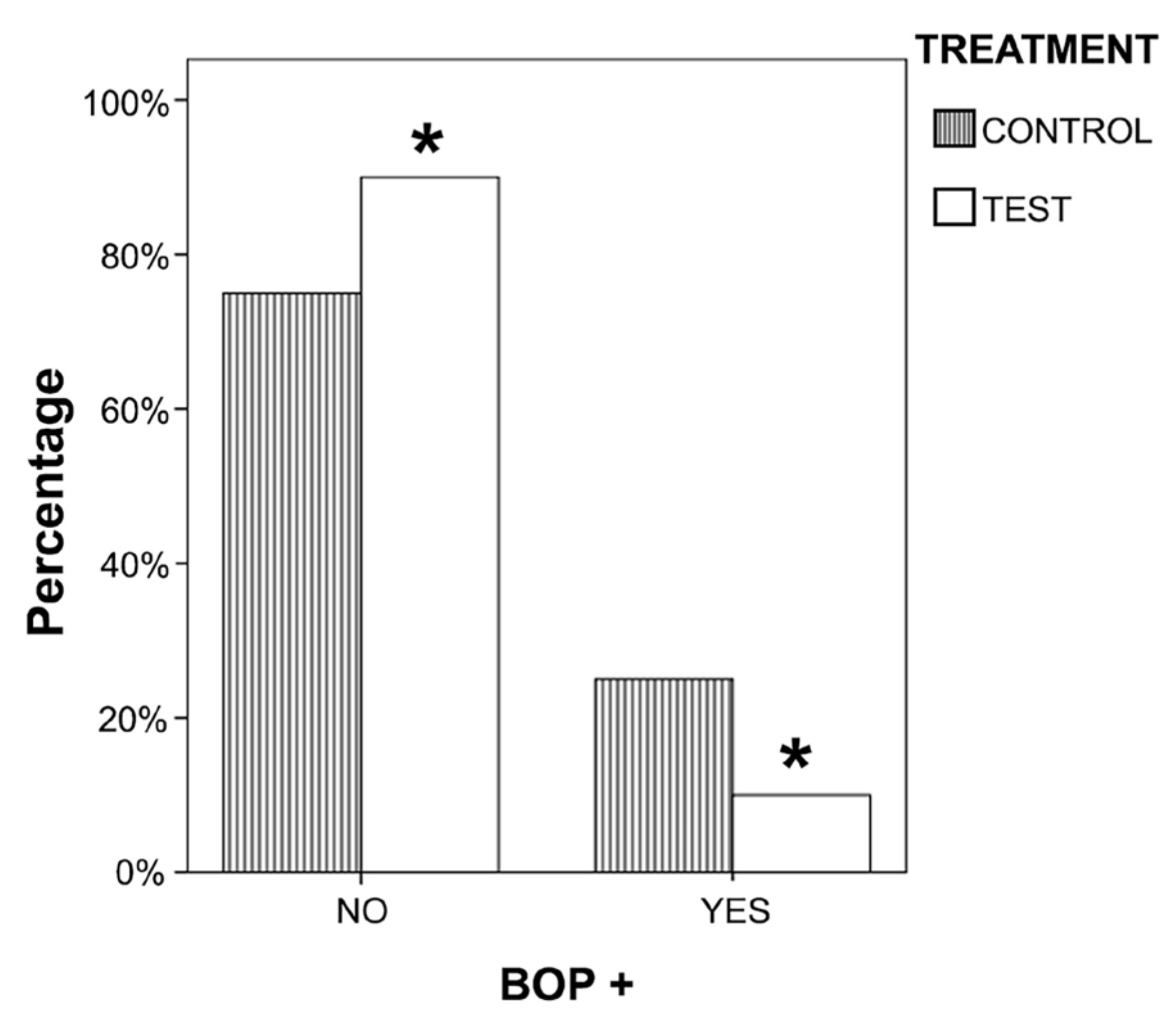
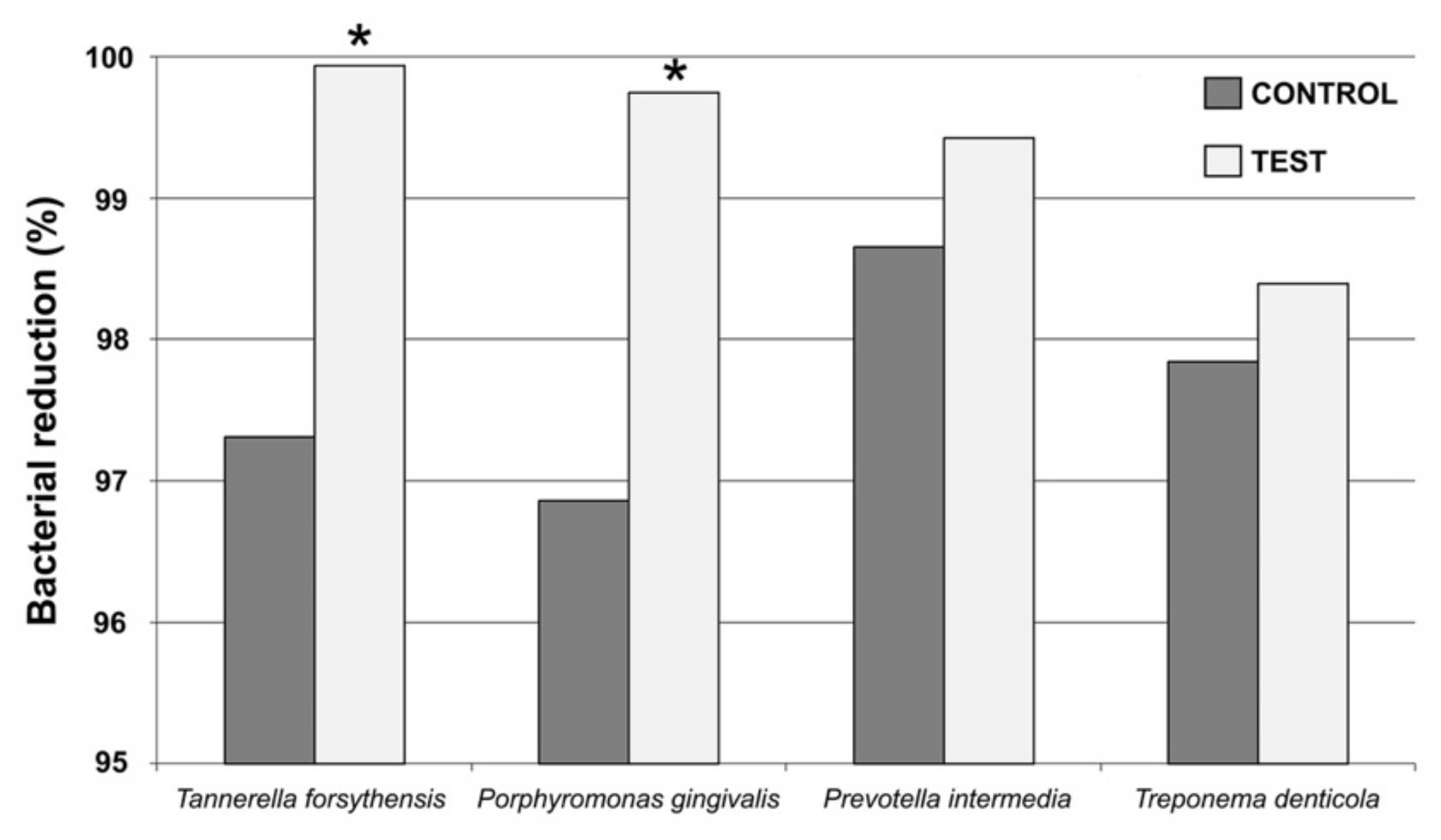
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richards, D. Review finds that severe periodontitis affects 11% of the world population. Evidence Based Dent. 2014, 15, 70–71. [Google Scholar] [CrossRef]
- Gotsman, I.; Lotan, C.; Soskolne, W.A.; Rassovsky, S.; Pugatsch, T.; Lapidus, L.; Novikov, Y.; Masrawa, S.; Stabholz, A. Periodontal destruction is associated with coronary artery disease and periodontal infection with acute coronary syndrome. J. Periodontol. 2007, 78, 849–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Prim 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, M.; Alshail, F.; Alshehri, F.A. Effect of scaling and root planing with and without adjunctive use of an essential-oil-based oral rinse in the treatment of periodontal inflammation in type-2 diabetic patients. J. Investig. Clin. Dent. 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wennström, J.L.; Dahlén, G.; Ramberg, P. Subgingival debridement of periodontal pockets by air polishing in comparison with ultrasonic instrumentation during maintenance therapy. J. Clin. Periodontol. 2011, 38, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Gebara, E.C.; Lima Luiz, A.; Mayer Marcia, P.A. Propolis antimicrobial activity against periodontopathic bacteria. Braz. J. Microbiol. 2002, 33, 365–369. [Google Scholar] [CrossRef]
- Palombo, E.A. Traditional Medicinal Plant Extracts and Natural Products with Activity against Oral Bacteria: Potential Application in the Prevention and Treatment of Oral Diseases. Evidence Based Complement. Altern. Med. 2011, 680354. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S. Do not put too much value on conventional medicines. J. Ethnopharmacol. 2005, 100, 37–39. [Google Scholar] [CrossRef]
- Wińska, K.; Mączka, W.; Łyczko, J.; Grabarczyk, M.; Czubaszek, A.; Szumny, A. Essential Oils as Antimicrobial Agents—Myth or Real Alternative? Molecules 2019, 24, 2130. [Google Scholar] [CrossRef] [Green Version]
- Sakagami, H.; Watanabe, T.; Hoshino, T.; Suda, N.; Mori, K.; Yasui, T.; Yamauchi, N.; Kashiwagi, H.; Gomi, T.; Oizumi, T.; et al. Recent Progress of Basic Studies of Natural Products and Their Dental Application. Medicines 2018, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Yoshimasu, Y.; Ikeda, T.; Sakai, N.; Yagi, A.; Hirayama, S.; Morinaga, Y.; Furukawa, S.; Nakao, R. Rapid Bactericidal Action of Propolis against Porphyromonas gingivalis. J. Dent. Res. 2018, 97, 928–936. [Google Scholar] [CrossRef]
- Martinello, M.; Mutinelli, F. Antioxidant Activity in Bee Products: A Review. Antioxidants 2021, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Przybyłek, I.; Karpiński, T.M. Antibacterial Properties of Propolis. Molecules 2019, 24, 2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, K.M.; Saleh, Z.; Jalal, J. Effect of local propolis irrigation in experimental periodontitis in rats on inflammatory markers (IL-1β and TNF-α) and oxidative stress. Indian J. Dent. Res. 2020, 31, 893–898. [Google Scholar] [CrossRef]
- Almuhayawi, M.S. Propolis as a novel antibacterial agent. Saudi J. Biol. Sci. 2020, 27, 3079–3086. [Google Scholar] [CrossRef]
- Anauate-Netto, C.; Anido-Anido, A.; Leegoy, H.R.; Matsumoto, R.; Alonso, R.C.; Marcucci, M.C.; Paulino, N.; Bretz, W.A. Randomized, double-blind, placebo-controlled clinical trial on the effects of propolis and chlorhexidine mouthrinses on gingivitis. Braz. Dent. Sci. 2014, 17, 11–15. [Google Scholar] [CrossRef]
- Singleton, V.L.; Orthofer, R.; Lamuela-Raventós, R.M. Analysis of total phenols and other oxidation substrates and antioxidants by means of folin-ciocalteu reagent. In Methods in Enzymology; Academic Press: Cambridge, MA, USA, 1999; Volume 299, pp. 152–178. [Google Scholar]
- Zhishen, J.; Mengcheng, T.; Jianming, W. Research on antioxidant activity of flavonoids from natural materials. Food Chem. 1999, 64, 555–559. [Google Scholar] [CrossRef]
- Avila-Campos, M.J. PCR detection of four periodontopathogens from subgingival clinical samples. Braz. J. Microbiol. 2003, 34, 34–81. [Google Scholar] [CrossRef] [Green Version]
- Ashimoto, A.; Chen, C.; Bakker, I.; Slots, J. Polymerase chain reaction detection of 8 putative periodontal pathogens in subgingival plaque of gingivitis and advanced periodontitis lesions. Oral Microbiol. Immunol. 1996, 11, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Pereira, E.M.; da Silva, J.L.; Silva, F.F.; De Luca, M.P.; Ferreira, E.F.; Lorentz, T.C.; Santos, V.R. Clinical Evidence of the Efficacy of a Mouthwash Containing Propolis for the Control of Plaque and Gingivitis: A Phase II Study. Evidence-Based Complement. Altern. Med. 2011, 2011, 750249. [Google Scholar] [CrossRef] [Green Version]
- Jain, S.; Rai, R.; Sharma, V.; Batra, M. Propolis in oral health: A natural remedy. World J Pharm. Sci. 2014, 2, 90–94. [Google Scholar]
- Bertolini, P.F.; Biondi Filho, O.; Pomilio, A.; Pinheiro, S.L.; Carvalho, M.S. Antimicrobial capacity of Aloe vera and propolis dentifrice against Streptococcus mutans strains in toothbrushes: An in vitro study. J. Appl. Oral Sci. 2012, 20, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skaba, D.; Morawiec, T.; Tanasiewicz, M.; Mertas, A.; Bobela, E.; Szliszka, E.; Skucha-Nowak, M.; Dawiec, M.; Yamamoto, R.; Ishiai, S.; et al. Influence of the toothpaste with brazilian ethanol extract propolis on the oral cavity health. Evidence-Based Complement. Altern. Med. 2013, 2013, 215391. [Google Scholar] [CrossRef]
- Lang, N.P.; Adler, R.; Joss, A.; Nyman, S. Absence of bleeding on probing. An indicator of periodontal stability. J. Clin. Periodontol. 1990, 17, 714–721. [Google Scholar] [CrossRef]
- Coutinho, A. Honeybee propolis extract in periodontal treatment: A clinical and microbiological study of propolis in periodontal treatment. Indian J. Dent. Res. 2012, 23, 294. [Google Scholar] [CrossRef] [PubMed]
- Sanghani, N.N.; Bm, S.; S, S. Health from the hive: Propolis as an adjuvant in the treatment of chronic periodontitis—A clinicomicrobiologic study. J. Clin. Diagn. Res. 2014, 8, ZC41–ZC44. [Google Scholar] [CrossRef] [PubMed]
- Nakao, R.; Senpuku, H.; Ohnishi, M.; Takai, H.; Ogata, Y. Effect of topical administration of propolis in chronic periodontitis. Odontology 2020, 108, 704–714. [Google Scholar] [CrossRef]
- Giammarinaro, E.; Marconcini, S.; Genovesi, A.; Poli, G.; Lorenzi, C.; Covani, U. Propolis as an adjuvant to non-surgical periodontal treatment: A clinical study with salivary anti-oxidant capacity assessment. Minerva Dent. Oral Sci. 2018, 67, 183–188. [Google Scholar] [CrossRef]
- Koo, H.; Gomes, B.P.; Rosalen, P.L.; Ambrosano, G.M.; Park, Y.K.; Cury, J.A. In vitro antimicrobial activity of propolis and Arnica montana against oral pathogens. Arch. Oral Biol. 2000, 45, 141–148. [Google Scholar] [CrossRef]
- Uzel, A.; Sorkun, K.; Onçağ, O.; Cogŭlu, D.; Gençay, O.; Salih, B. Chemical compositions and antimicrobial activities of four different Anatolian propolis samples. Microbiol. Res. 2005, 160, 189–195. [Google Scholar] [CrossRef]
- Feres, M.; Figueiredo, L.C.; Barreto, I.M.; Coelho, M.H.; Araujo, M.W.; Cortelli, S.C. In vitro antimicrobial activity of plant extracts and propolis in saliva samples of healthy and periodontally-involved subjects. J. Int. Acad. Periodontol. 2005, 7, 90–96. [Google Scholar] [PubMed]
- Akca, A.E.; Akca, G.; Topçu, F.T.; Macit, E.; Pikdöken, L.; Özgen, I.Ş. The Comparative Evaluation of the Antimicrobial Effect of Propolis with Chlorhexidine against Oral Pathogens: An In Vitro Study. BioMed Res. Int. 2016, 2016, 3627463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mello, B.C.B.S.; Hubinger, M.D. Antioxidant activity and polyphenol contents in Brazilian green propolis extracts prepared with the use of ethanol and water as solvents in different pH values. Int. J. Food Sci. Technol. 2012, 47, 2510–2518. [Google Scholar] [CrossRef]
- Lemos, J.A.; Burne, R.A. A model of efficiency: Stress tolerance by Streptococcus mutans. Microbiology 2008, 154, 3247–3255. [Google Scholar] [CrossRef] [Green Version]
- George, J.; Klika, A.K.; Higuera, C.A. Use of Chlorhexidine Preparations in Total Joint Arthroplasty. J. Bone Jt. Infect. 2017, 2, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, G.W.; Rael, L.T.; Bar-Or, R.; Shimonkevitz, R.; Mains, C.W.; Slone, D.S.; Craun, M.L.; Bar-Or, D. Mechanisms of delayed wound healing by commonly used antiseptics. J. Trauma Inj. Infect. Crit. Care 2009, 66, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Man, J.; Shelton, R.M.; Cooper, P.R.; Landini, G.; Scheven, B.A. Low intensity ultrasound stimulates osteoblast migration at different frequencies. J. Bone Miner. Metab. 2012, 30, 602–607. [Google Scholar] [CrossRef]
- Björkner, B.E. Industrial Airborne Dermatoses. Dermatol. Clin. 1994, 12, 501–509. [Google Scholar] [CrossRef]
- Manoil, D.; Courvoisier, D.S.; Gilbert, B.; Möller, B.; Walker, U.A.; Muehlenen, I.V.; Rubbert-Roth, A.; Finckh, A.; Bostanci, N. Associations between serum antibodies to periodontal pathogens and preclinical phases of rheumatoid arthritis. Rheumatology 2021. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Periodontal Parameters at Baseline (BL) and the Month (1 M) | ||||||
|---|---|---|---|---|---|---|
| Control | Test | |||||
| Mean | SEM | Median | Mean | SEM | Median | |
| BL-PPD (mm) | 4.75 | 0.17 | 5.00 | 4.75 | 0.18 | 5.00 |
| BL-CAL (mm) | 5.75 | 0.29 | 5.50 | 5.80 | 0.33 | 5.50 |
| 1M-PPD (mm) | 3.60 | 0.17 | 4.00 | 3.30 | 0.15 | 3.00 |
| 1M-CAL (mm) | 4.55 | 0.28 | 5.00 | 4.45 | 0.26 | 4.00 |
| VAR. PPD (mm) | 1.20 * | 0.14 | 1.00 | 1.45 * | 0.15 | 1.00 |
| VAR. CAL (mm) | 1.20 * | 0.17 | 1.00 | 1.35 * | 0.18 | 1.00 |
| VAR. PPD (%) | 36.42 * | 5.14 | 33.33 | 46.83 * | 6.02 | 33.33 |
| VAR. CAL (%) | 30.63 * | 5.72 | 25.00 | 31.46 * | 4.24 | 25.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lisbona-González, M.J.; Muñoz-Soto, E.; Reyes-Botella, C.; Olmedo-Gaya, M.V.; Diaz-Castro, J.; Moreno-Fernandez, J. Study of the Antimicrobial Effect of an Ethanolic Extract of Propolis in Periodontal Disease. Appl. Sci. 2021, 11, 7463. https://doi.org/10.3390/app11167463
Lisbona-González MJ, Muñoz-Soto E, Reyes-Botella C, Olmedo-Gaya MV, Diaz-Castro J, Moreno-Fernandez J. Study of the Antimicrobial Effect of an Ethanolic Extract of Propolis in Periodontal Disease. Applied Sciences. 2021; 11(16):7463. https://doi.org/10.3390/app11167463
Chicago/Turabian StyleLisbona-González, Maria Jesús, Esther Muñoz-Soto, Candela Reyes-Botella, Maria Victoria Olmedo-Gaya, Javier Diaz-Castro, and Jorge Moreno-Fernandez. 2021. "Study of the Antimicrobial Effect of an Ethanolic Extract of Propolis in Periodontal Disease" Applied Sciences 11, no. 16: 7463. https://doi.org/10.3390/app11167463
APA StyleLisbona-González, M. J., Muñoz-Soto, E., Reyes-Botella, C., Olmedo-Gaya, M. V., Diaz-Castro, J., & Moreno-Fernandez, J. (2021). Study of the Antimicrobial Effect of an Ethanolic Extract of Propolis in Periodontal Disease. Applied Sciences, 11(16), 7463. https://doi.org/10.3390/app11167463