In Vivo Efficacy of Contact Lens Drug-Delivery Systems in Glaucoma Management. A Systematic Review



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
3. Results
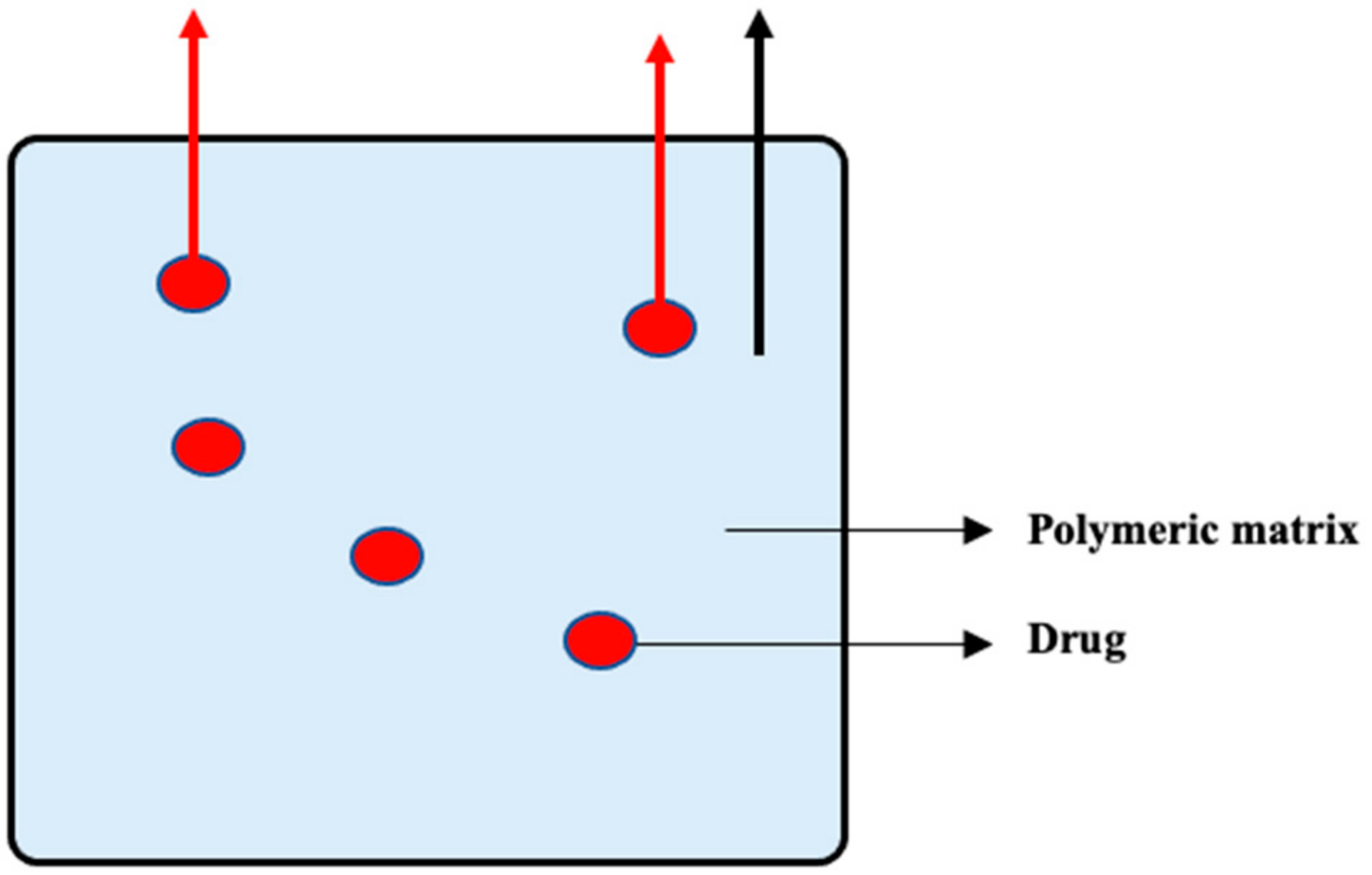
3.1. The Drug-Soaked CL
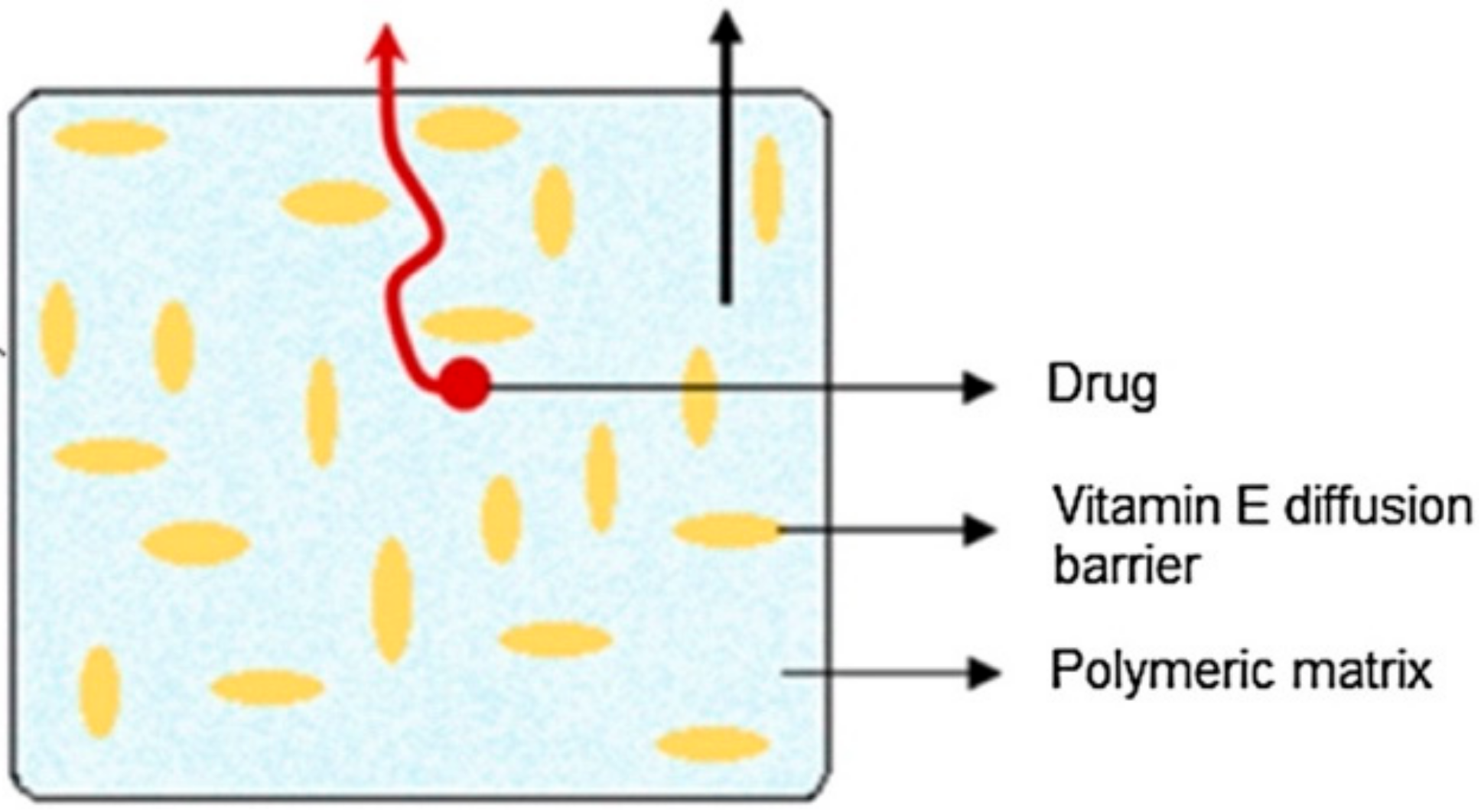
3.2. Vitamin-E-Loaded CL
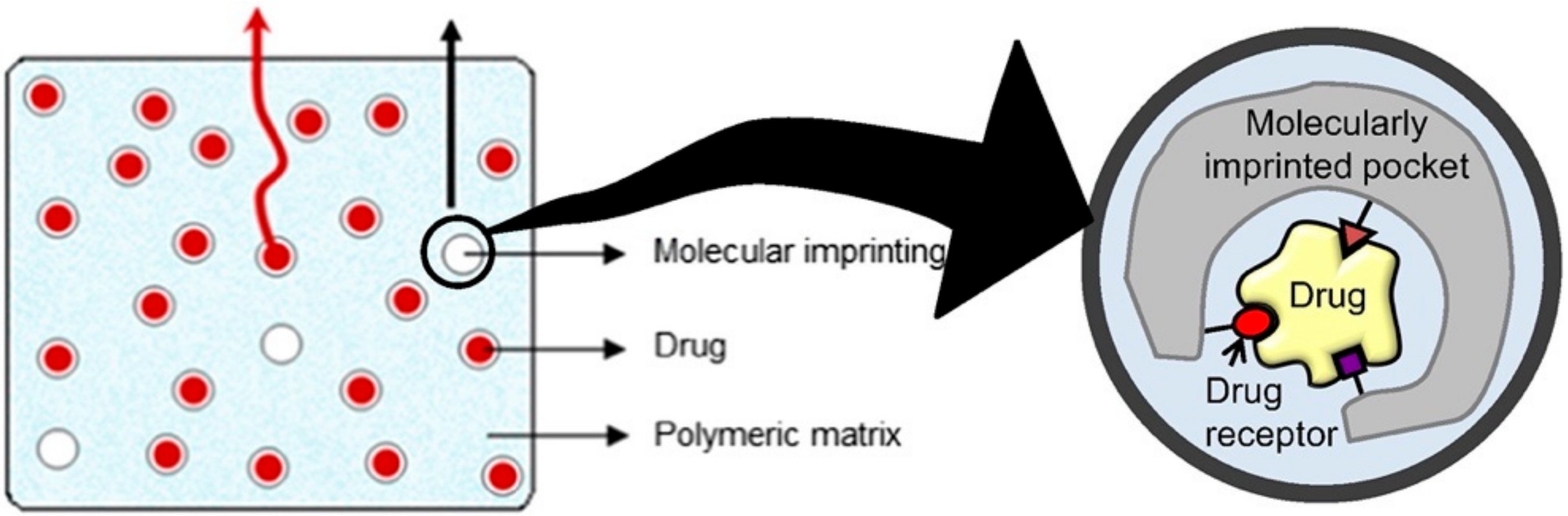
3.3. Molecularly Imprinted CL
3.4. CL with Implant
3.5. Nanoparticle-Loaded CL
4. Discussion
4.1. Barriers to Widespread Use in Clinical Practice
4.2. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Hattenhauer, M.G.; Johnson, D.H.; Ing, H.H.; Herman, D.C.; Hodge, D.O.; Yawn, B.P.; Butterfield, L.C.; Gray, D.T. The probability of blindness from open-angle glaucoma. Ophthalmology 1998, 105, 2099–2104. [Google Scholar] [CrossRef]
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition—Part 1 Supported by the EGS Foundation. Br. J. Ophthalmol. 2017, 101, 1–72. [CrossRef] [Green Version]
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition—Chapter 3: Treatment principles and options Supported by the EGS Foundation. Part 1 Foreword Introd. Gloss. Chapter 3 Treat. Princ. Options 2017, 101, 130–195. [CrossRef] [Green Version]
- Lusthaus, J.; Goldberg, I. Current management of glaucoma. Med. J. Aust. 2019, 210, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Okeke, C.O.; Quigley, H.A.; Jampel, H.D.; Ying, G.S.; Plyler, R.J.; Jiang, Y.; Friedman, D.S. Adherence with topical glaucoma medication monitored electronically the Travatan Dosing Aid study. Ophthalmology 2009, 116, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Kinast, R.M.; Mansberger, S.L. Glaucoma Adherence-From Theriac to the Future. Am. J. Ophthalmol. 2018, 191, xiii–xv. [Google Scholar] [CrossRef]
- Gatwood, J.D.; Johnson, J.; Jerkins, B. Comparisons of Self-reported Glaucoma Medication Adherence with a New Wireless Device: A Pilot Study. J. Glaucoma 2017, 26, 1056–1061. [Google Scholar] [CrossRef]
- Tsai, J.C.; McClure, C.A.; Ramos, S.E.; Schlundt, D.G.; Pichert, J.W. Compliance barriers in glaucoma: A systematic classification. J. Glaucoma 2003, 12, 393–398. [Google Scholar] [CrossRef]
- Jaenen, N.; Baudouin, C.; Pouliquen, P.; Manni, G.; Figueiredo, A.; Zeyen, T. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur. J. Ophthalmol. 2007, 17, 341–349. [Google Scholar] [CrossRef]
- Gilissen, L.; De Decker, L.; Hulshagen, T.; Goossens, A. Allergic contact dermatitis caused by topical ophthalmic medications: Keep an eye on it! Contact Dermat. 2019, 80, 291–297. [Google Scholar] [CrossRef]
- Davis, S.A.; Sleath, B.; Carpenter, D.M.; Blalock, S.J.; Muir, K.W.; Budenz, D.L. Drop instillation and glaucoma. Curr. Opin. Ophthalmol. 2018, 29, 171–177. [Google Scholar] [CrossRef]
- Schwartz, G.F.; Quigley, H.A. Adherence and persistence with glaucoma therapy. Surv. Ophthalmol. 2008, 53 (Suppl. S1), S57–S68. [Google Scholar] [CrossRef] [PubMed]
- Figus, M.; Agnifili, L.; Lanzini, M.; Brescia, L.; Sartini, F.; Mastropasqua, L.; Posarelli, C. Topical preservative-free ophthalmic treatments: An unmet clinical need. Expert Opin. Drug Deliv. 2020. [Google Scholar] [CrossRef]
- Kaur, I.P.; Lal, S.; Rana, C.; Kakkar, S.; Singh, H. Ocular preservatives: Associated risks and newer options. Cutan. Ocul. Toxicol. 2009, 28, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Burstein, N.L. The effects of topical drugs and preservatives on the tears and corneal epithelium in dry eye. Trans. Ophthalmol. Soc. UK 1985, 104 (Pt 4), 402–409. [Google Scholar]
- Marx, D.; Birkhoff, M. New devices for dispensing ophthalmic treatments may be the key to managing the life cycles of established products. Drug Deliv. Technol. 2010, 10, 16–21. [Google Scholar]
- Kompella, U.B.; Hartman, R.R.; Patil, M.A. Extraocular, periocular, and intraocular routes for sustained drug delivery for glaucoma. Prog. Retin. Eye Res. 2020, 100901. [Google Scholar] [CrossRef]
- Souto, E.B.; Dias-Ferreira, J.; Lopez-Machado, A.; Ettcheto, M.; Cano, A.; Camins Espuny, A.; Espina, M.; Garcia, M.L.; Sanchez-Lopez, E. Advanced Formulation Approaches for Ocular Drug Delivery: State-Of-The-Art and Recent Patents. Pharmaceutics 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular drug delivery. Aaps. J. 2010, 12, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Peral, A.; Martínez Águila, A.; Pastrana, C.; Huete-Toral, F.; Carpena-Torres, C.; Carracedo, G. Contact Lenses as Drug Delivery System for Glaucoma: A Review. Appl. Sci. 2020, 10, 5151. [Google Scholar] [CrossRef]
- Barr, J.; Mack, C. Contact Lenses Yesterday, Today, and the Best Yet to Come. Contact Lens Spectr. 2011, 26, 14–15. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Keaney, M.; Lorimer, A.R. Auditing the implementation of SIGN (Scottish Intercollegiate Guidelines Network) clinical guidelines. Int. J. Health Care Qual. Assur. Inc. Lead. Health Serv. 1999, 12, 314–317. [Google Scholar] [CrossRef] [PubMed]
- Howick, J.; Glasziou, P.; Aronson, J.K. Evidence-based mechanistic reasoning. J. R. Soc. Med. 2010, 103, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Kilkenny, C.; Browne, W.; Cuthill, I.C.; Emerson, M.; Altman, D.G.; Group, N.C.R.R.G.W. Animal research: Reporting in vivo experiments: The ARRIVE guidelines. Br. J. Pharmacol. 2010, 160, 1577–1579. [Google Scholar] [CrossRef]
- Schwarz, F.; Iglhaut, G.; Becker, J. Quality assessment of reporting of animal studies on pathogenesis and treatment of peri-implant mucositis and peri-implantitis. A systematic review using the ARRIVE guidelines. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 63–72. [Google Scholar] [CrossRef]
- Alemán-Laporte, J.; Alvarado, G.; Sa Garcia-Gomes, M.; Fonseca Brasil Antiorio, A.T.; Zúñiga-Montero, M.; Cabrera Mori, C.M. Quality of Adherence to the ARRIVE Guidelines in the Material and Methods Section in Studies Where Swine Were Used as Surgical Biomodels: A Systematic Review (2013–2018). Animals (Basel) 2019, 9, 947. [Google Scholar] [CrossRef] [Green Version]
- Wei, D.; Tang, K.; Wang, Q.; Estill, J.; Yao, L.; Wang, X.; Chen, Y.; Yang, K. The use of GRADE approach in systematic reviews of animal studies. J. Evid. Based Med. 2016, 9, 98–104. [Google Scholar] [CrossRef]
- Schultz, C.L.; Poling, T.R.; Mint, J.O. A medical device/drug delivery system for treatment of glaucoma. Clin. Exp. Optom. 2009, 92, 343–348. [Google Scholar] [CrossRef] [PubMed]
- North, D.P. Treatment of acute glaucoma. Can. Med. Assoc. J. 1971, 105, 561. [Google Scholar]
- Asseff, C.F.; Weisman, R.L.; Podos, S.M.; Becker, B. Ocular penetration of pilocarpine in primates. Am. J. Ophthalmol. 1973, 75, 212–215. [Google Scholar] [CrossRef]
- Podos, S.M.; Becker, B.; Asseff, C.; Hartstein, J. Pilocarpine therapy with soft contact lenses. Am. J. Ophthalmol. 1972, 73, 336–341. [Google Scholar] [CrossRef]
- Hillman, J.S. Management of acute glaucoma with pilocarpine-soaked hydrophilic lens. Br. J. Ophthalmol. 1974, 58, 674–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruben, M.; Watkins, R. Pilocarpine dispensation for the soft hydrophilic contact lens. Br. J. Ophthalmol. 1975, 59, 455–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, C.C.; Ben-Shlomo, A.; Mackay, E.O.; Plummer, C.E.; Chauhan, A. Drug delivery by contact lens in spontaneously glaucomatous dogs. Curr. Eye Res. 2012, 37, 204–211. [Google Scholar] [CrossRef]
- Peng, C.C.; Burke, M.T.; Carbia, B.E.; Plummer, C.; Chauhan, A. Extended drug delivery by contact lenses for glaucoma therapy. J. Control. Release 2012, 162, 152–158. [Google Scholar] [CrossRef]
- Hsu, K.H.; Carbia, B.E.; Plummer, C.; Chauhan, A. Dual drug delivery from vitamin E loaded contact lenses for glaucoma therapy. Eur. J. Pharm. Biopharm. 2015, 94, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Hiratani, H.; Fujiwara, A.; Tamiya, Y.; Mizutani, Y.; Alvarez-Lorenzo, C. Ocular release of timolol from molecularly imprinted soft contact lenses. Biomaterials 2005, 26, 1293–1298. [Google Scholar] [CrossRef]
- Desai, A.R.; Maulvi, F.A.; Pandya, M.M.; Ranch, K.M.; Vyas, B.A.; Shah, S.A.; Shah, D.O. Co-delivery of timolol and hyaluronic acid from semi-circular ring-implanted contact lenses for the treatment of glaucoma: In vitro and in vivo evaluation. Biomater. Sci. 2018, 6, 1580–1591. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.R.; Maulvi, F.A.; Desai, D.M.; Shukla, M.R.; Ranch, K.M.; Vyas, B.A.; Shah, S.A.; Sandeman, S.; Shah, D.O. Multiple drug delivery from the drug-implants-laden silicone contact lens: Addressing the issue of burst drug release. Mater. Sci. Eng. C 2020, 112, 110885. [Google Scholar] [CrossRef]
- Jung, H.J.; Abou-Jaoude, M.; Carbia, B.E.; Plummer, C.; Chauhan, A. Glaucoma therapy by extended release of timolol from nanoparticle loaded silicone-hydrogel contact lenses. J. Control Release 2013, 165, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Ciolino, J.B.; Stefanescu, C.F.; Ross, A.E.; Salvador-Culla, B.; Cortez, P.; Ford, E.M.; Wymbs, K.A.; Sprague, S.L.; Mascoop, D.R.; Rudina, S.S.; et al. In vivo performance of a drug-eluting contact lens to treat glaucoma for a month. Biomaterials 2014, 35, 432–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciolino, J.B.; Ross, A.E.; Tulsan, R.; Watts, A.C.; Wang, R.F.; Zurakowski, D.; Serle, J.B.; Kohane, D.S. Latanoprost-Eluting Contact Lenses in Glaucomatous Monkeys. Ophthalmology 2016, 123, 2085–2092. [Google Scholar] [CrossRef]
- Maulvi, F.A.; Lakdawala, D.H.; Shaikh, A.A.; Desai, A.R.; Choksi, H.H.; Vaidya, R.J.; Ranch, K.M.; Koli, A.R.; Vyas, B.A.; Shah, D.O. In vitro and in vivo evaluation of novel implantation technology in hydrogel contact lenses for controlled drug delivery. J. Control Release 2016, 226, 47–56. [Google Scholar] [CrossRef]
- Xu, J.; Li, X.; Sun, F. Preparation and evaluation of a contact lens vehicle for puerarin delivery. J. Biomater. Sci. Polym. Ed. 2010, 21, 271–288. [Google Scholar] [CrossRef] [PubMed]
- Maulvi, F.A.; Patil, R.J.; Desai, A.R.; Shukla, M.R.; Vaidya, R.J.; Ranch, K.M.; Vyas, B.A.; Shah, S.A.; Shah, D.O. Effect of gold nanoparticles on timolol uptake and its release kinetics from contact lenses: In vitro and in vivo evaluation. Acta Biomater. 2019, 86, 350–362. [Google Scholar] [CrossRef]
- Xu, J.; Ge, Y.; Bu, R.; Zhang, A.; Feng, S.; Wang, J.; Gou, J.; Yin, T.; He, H.; Zhang, Y.; et al. Co-delivery of latanoprost and timolol from micelles-laden contact lenses for the treatment of glaucoma. J. Control Release 2019, 305, 18–28. [Google Scholar] [CrossRef]
- Wichterle, O.; LÍM, D. Hydrophilic Gels for Biological Use. Nature 1960, 185, 117–118. [Google Scholar] [CrossRef]
- Marmion, V.J.; Yurdakul, S. Pilocarpine administration by contact lens. Trans Ophthalmol. Soc. UK 1977, 97, 162–163. [Google Scholar] [PubMed]
- Horne, R.R.; Rich, J.T.; Bradley, M.W.; Pitt, W.G. Latanoprost uptake and release from commercial contact lenses. J. Biomater. Sci. Polym. Ed. 2020, 31, 1–19. [Google Scholar] [CrossRef]
- Carvalho, I.M.; Marques, C.S.; Oliveira, R.S.; Coelho, P.B.; Costa, P.C.; Ferreira, D.C. Sustained drug release by contact lenses for glaucoma treatment-a review. J. Control Release 2015, 202, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Cho, S.; Park, H.S.; Kwon, I. Ocular Drug Delivery through pHEMA-Hydrogel Contact Lenses Co-Loaded with Lipophilic Vitamins. Sci. Rep. 2016, 6, 34194. [Google Scholar] [CrossRef]
- Alvarez-Lorenzo, C.; Hiratani, H.; Gomez-Amoza, J.L.; Martinez-Pacheco, R.; Souto, C.; Concheiro, A. Soft contact lenses capable of sustained delivery of timolol. J. Pharm. Sci. 2002, 91, 2182–2192. [Google Scholar] [CrossRef] [PubMed]
- White, C.J.; Byrne, M.E. Molecularly imprinted therapeutic contact lenses. Expert Opin. Drug Deliv. 2010, 7, 765–780. [Google Scholar] [CrossRef]
- Alvarez-Lorenzo, C.; Yanez, F.; Barreiro-Iglesias, R.; Concheiro, A. Imprinted soft contact lenses as norfloxacin delivery systems. J. Control Release 2006, 113, 236–244. [Google Scholar] [CrossRef]
- Vaughan, A.D.; Zhang, J.B.; Byrne, M.E. Enhancing therapeutic loading and delaying transport via molecular imprinting and living/controlled polymerization. AIChE J. 2010, 56, 268–279. [Google Scholar] [CrossRef]
- Ali, M.; Byrne, M.E. Controlled release of high molecular weight hyaluronic Acid from molecularly imprinted hydrogel contact lenses. Pharm. Res. 2009, 26, 714–726. [Google Scholar] [CrossRef]
- Xu, J.; Li, X.; Sun, F. In vitro and in vivo evaluation of ketotifen fumarate-loaded silicone hydrogel contact lenses for ocular drug delivery. Drug Deliv. 2011, 18, 150–158. [Google Scholar] [CrossRef] [Green Version]
- Malaekeh-Nikouei, B.; Ghaeni, F.A.; Motamedshariaty, V.S.; Mohajeri, S.A. Controlled release of prednisolone acetate from molecularly imprinted hydrogel contact lenses. J. Appl. Polym. Sci. 2012, 126, 387–394. [Google Scholar] [CrossRef]
- Varela-Garcia, A.; Gomez-Amoza, J.L.; Concheiro, A.; Alvarez-Lorenzo, C. Imprinted Contact Lenses for Ocular Administration of Antiviral Drugs. Polymers (Basel) 2020, 12, 2026. [Google Scholar] [CrossRef] [PubMed]
- De Jong, W.H.; Borm, P.J. Drug delivery and nanoparticles:applications and hazards. Int. J. Nanomed. 2008, 3, 133–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, J.F.; Couceiro, R.; Concheiro, A.; Torres-Labandeira, J.J.; Alvarez-Lorenzo, C. Poly(hydroxyethyl methacrylate-co-methacrylated-beta-cyclodextrin) hydrogels: Synthesis, cytocompatibility, mechanical properties and drug loading/release properties. Acta Biomater. 2008, 4, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Kim, S.H.; Khang, D.; Lee, J.Y. Potential Therapeutic Usage of Nanomedicine for Glaucoma Treatment. Int. J. Nanomed. 2020, 15, 5745–5765. [Google Scholar] [CrossRef] [PubMed]
- Kowing, D.; Messer, D.; Slagle, S.; Wasik, A.; Group, V.P.S. Programs to optimize adherence in glaucoma. Optometry 2010, 81, 339–350. [Google Scholar] [CrossRef]
- Nardi, M.; Casini, G.; Guidi, G.; Figus, M. Emerging surgical therapy in the treatment of glaucoma. Prog. Brain Res. 2015, 221, 341–357. [Google Scholar] [CrossRef]
- Fea, A.M.; Bron, A.M.; Economou, M.A.; Laffi, G.; Martini, E.; Figus, M.; Oddone, F. European study of the efficacy of a cross-linked gel stent for the treatment of glaucoma. J. Cataract Refract. Surg. 2020, 46, 441–450. [Google Scholar] [CrossRef]
- Wang, B.B.; Lin, M.M.; Nguyen, T.; Turalba, A.V. Patient attitudes toward novel glaucoma drug delivery approaches. Digit. J. Ophthalmol. 2018, 24, 16–23. [Google Scholar] [CrossRef]
- Agency, E.M. Emea/622721/2009. Available online: https://www.ema.europa.eu/en/documents/public-statement/emea-public-statement-antimicrobial-preservatives-ophthalmic-preparations-human-use_en.pdf (accessed on 27 May 2020).
- Varadaraj, V.; Kahook, M.Y.; Ramulu, P.Y.; Pitha, I.F. Patient Acceptance of Sustained Glaucoma Treatment Strategies. J. Glaucoma 2018, 27, 328–335. [Google Scholar] [CrossRef]
- Lim, C.H.L.; Stapleton, F.; Mehta, J.S. Review of Contact Lens-Related Complications. Eye Contact Lens. 2018, 44 (Suppl. 2), S1–S10. [Google Scholar] [CrossRef] [PubMed]
- Dart, J.K.; Stapleton, F.; Minassian, D. Contact lenses and other risk factors in microbial keratitis. Lancet 1991, 338, 650–653. [Google Scholar] [CrossRef]
- Schein, O.D.; Buehler, P.O.; Stamler, J.F.; Verdier, D.D.; Katz, J. The impact of overnight wear on the risk of contact lens-associated ulcerative keratitis. Arch. Ophthalmol. 1994, 112, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Holden, B.A.; Sweeney, D.F.; Swarbrick, H.A.; Vannas, A.; Nilsson, K.T.; Efron, N. The vascular response to long-term extended contact lens wear. Clin. Exp. Optom. 1986, 69, 112–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holden, B.A.; Sweeney, D.F.; Vannas, A.; Nilsson, K.T.; Efron, N. Effects of long-term extended contact lens wear on the human cornea. Investig. Ophthalmol. Vis. Sci. 1985, 26, 1489–1501. [Google Scholar]
- Weissman, B.A.; Mondino, B.J. Risk factors for contact lens associated microbial keratitis. Cont. Lens Anterior Eye 2002, 25, 3–9. [Google Scholar] [CrossRef]
- Doughty, M.J.; Aakre, B.M.; Ystenaes, A.E.; Svarverud, E. Short-term adaptation of the human corneal endothelium to continuous wear of silicone hydrogel (lotrafilcon A) contact lenses after daily hydrogel lens wear. Optom. Vis. Sci. 2005, 82, 473–480. [Google Scholar] [CrossRef] [Green Version]
- Willcox, M.D.P.; Argüeso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- Pisella, P.J.; Malet, F.; Lejeune, S.; Brignole, F.; Debbasch, C.; Bara, J.; Rat, P.; Colin, J.; Baudouin, C. Ocular surface changes induced by contact lens wear. Cornea 2001, 20, 820–825. [Google Scholar] [CrossRef]
- Tseng, S.S.; Hsiao, J.C.; Chang, D.C. Mistaken diagnosis of keratoconus because of corneal warpage induced by hydrogel lens wear. Cornea 2007, 26, 1153–1155. [Google Scholar] [CrossRef]
- Schornack, M. Hydrogel contact lens-induced corneal warpage. Cont. Lens Anterior Eye 2003, 26, 153–159. [Google Scholar] [CrossRef]
- Costa, V.P.; Braga, M.E.M.; Duarte, C.M.M.; Alvarez-Lorenzo, C.; Concheiro, A.; Gil, M.H.; de Sousa, H.C. Anti-glaucoma drug-loaded contact lenses prepared using supercritical solvent impregnation. J. Supercrit. Fluids 2010, 53, 165–173. [Google Scholar] [CrossRef]
- Sharma, M.; Bhowmick, R.; Gappa-Fahlenkamp, H. Drug-Loaded Nanoparticles Embedded in a Biomembrane Provide a Dual-Release Mechanism for Drug Delivery to the Eye. J. Ocul. Pharmacol. Ther. 2016, 32, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kim, H.J.; Kim, D.H.; Chang, W.S.; Vales, T.P.; Kim, J.W.; Kim, K.H.; Kim, J.K. Thermo-sensitive nanogel-laden bicontinuous microemulsion drug-eluting contact lenses. J. Biomed. Mater. Res. B Appl. Biomater. 2019, 107, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Shin, K.S.; Kim, J.W.; Kang, J.Y.; Kim, J.K. Stimulus-Responsive Contact Lens for IOP Measurement or Temperature-Triggered Drug Release. Transl. Vis. Sci. Technol. 2020, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uchida, R.; Sato, T.; Tanigawa, H.; Uno, K. Azulene incorporation and release by hydrogel containing methacrylamide propyltrimenthylammonium chloride, and its application to soft contact lens. J. Control Release 2003, 92, 259–264. [Google Scholar] [CrossRef]
- Sato, T.; Uchida, R.; Tanigawa, H.; Uno, K.; Murakami, A. Application of polymer gels containing side-chain phosphate groups to drug-delivery contact lenses. J. Appl. Polym. Sci. 2005, 98, 731–735. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sartini, F.; Menchini, M.; Posarelli, C.; Casini, G.; Figus, M. In Vivo Efficacy of Contact Lens Drug-Delivery Systems in Glaucoma Management. A Systematic Review. Appl. Sci. 2021, 11, 724. https://doi.org/10.3390/app11020724
Sartini F, Menchini M, Posarelli C, Casini G, Figus M. In Vivo Efficacy of Contact Lens Drug-Delivery Systems in Glaucoma Management. A Systematic Review. Applied Sciences. 2021; 11(2):724. https://doi.org/10.3390/app11020724
Chicago/Turabian StyleSartini, Francesco, Martina Menchini, Chiara Posarelli, Giamberto Casini, and Michele Figus. 2021. "In Vivo Efficacy of Contact Lens Drug-Delivery Systems in Glaucoma Management. A Systematic Review" Applied Sciences 11, no. 2: 724. https://doi.org/10.3390/app11020724
APA StyleSartini, F., Menchini, M., Posarelli, C., Casini, G., & Figus, M. (2021). In Vivo Efficacy of Contact Lens Drug-Delivery Systems in Glaucoma Management. A Systematic Review. Applied Sciences, 11(2), 724. https://doi.org/10.3390/app11020724