
Multi-Shape Free-Form Deformation Framework for Efficient Data Transmission in AR-Based Medical Training Simulators


Abstract
:1. Introduction
2. Materials and Methods
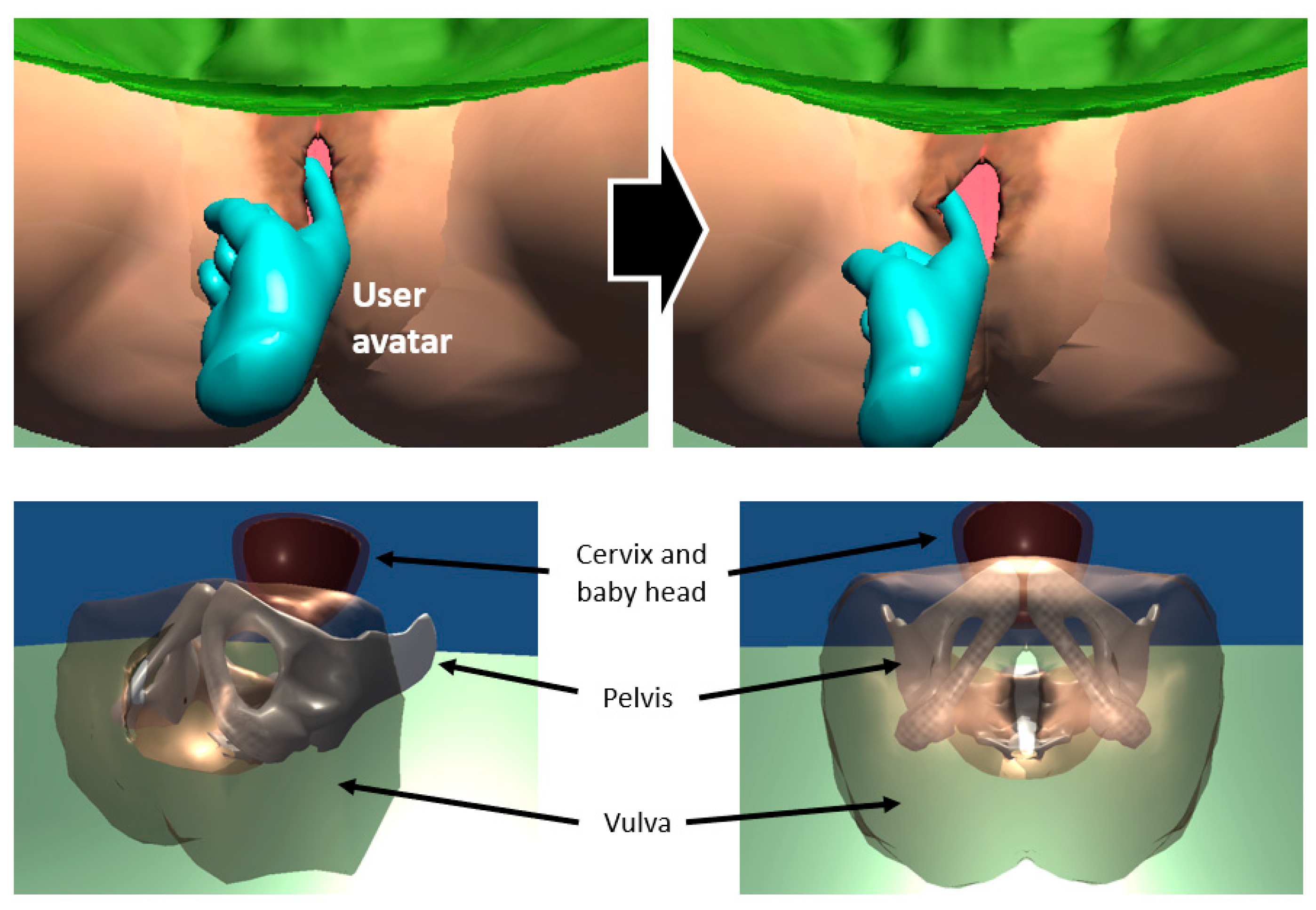
2.1. Use Case-Simulation of Vaginal Examination During Labour
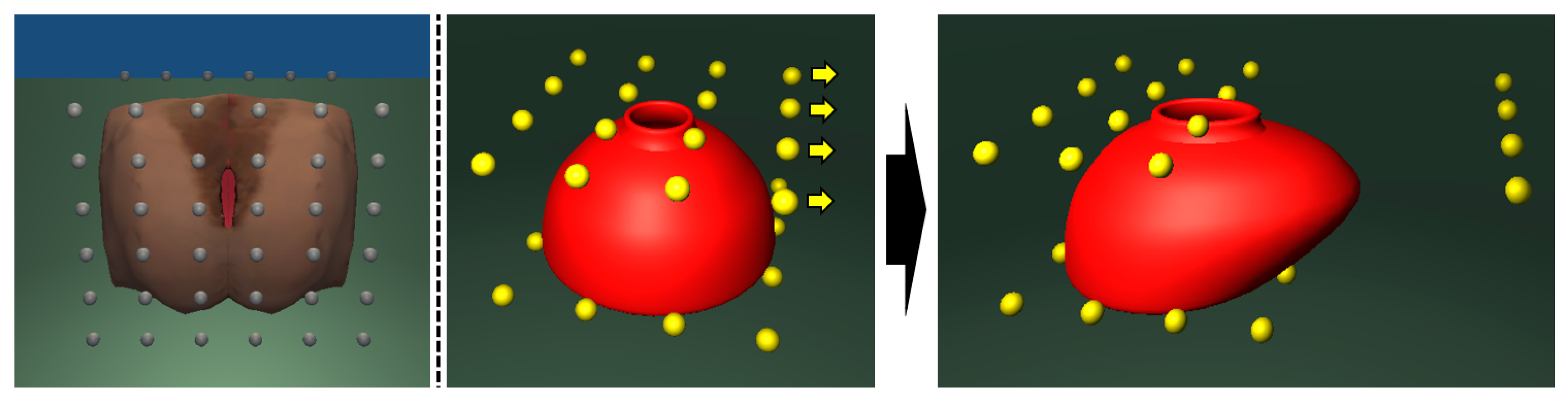
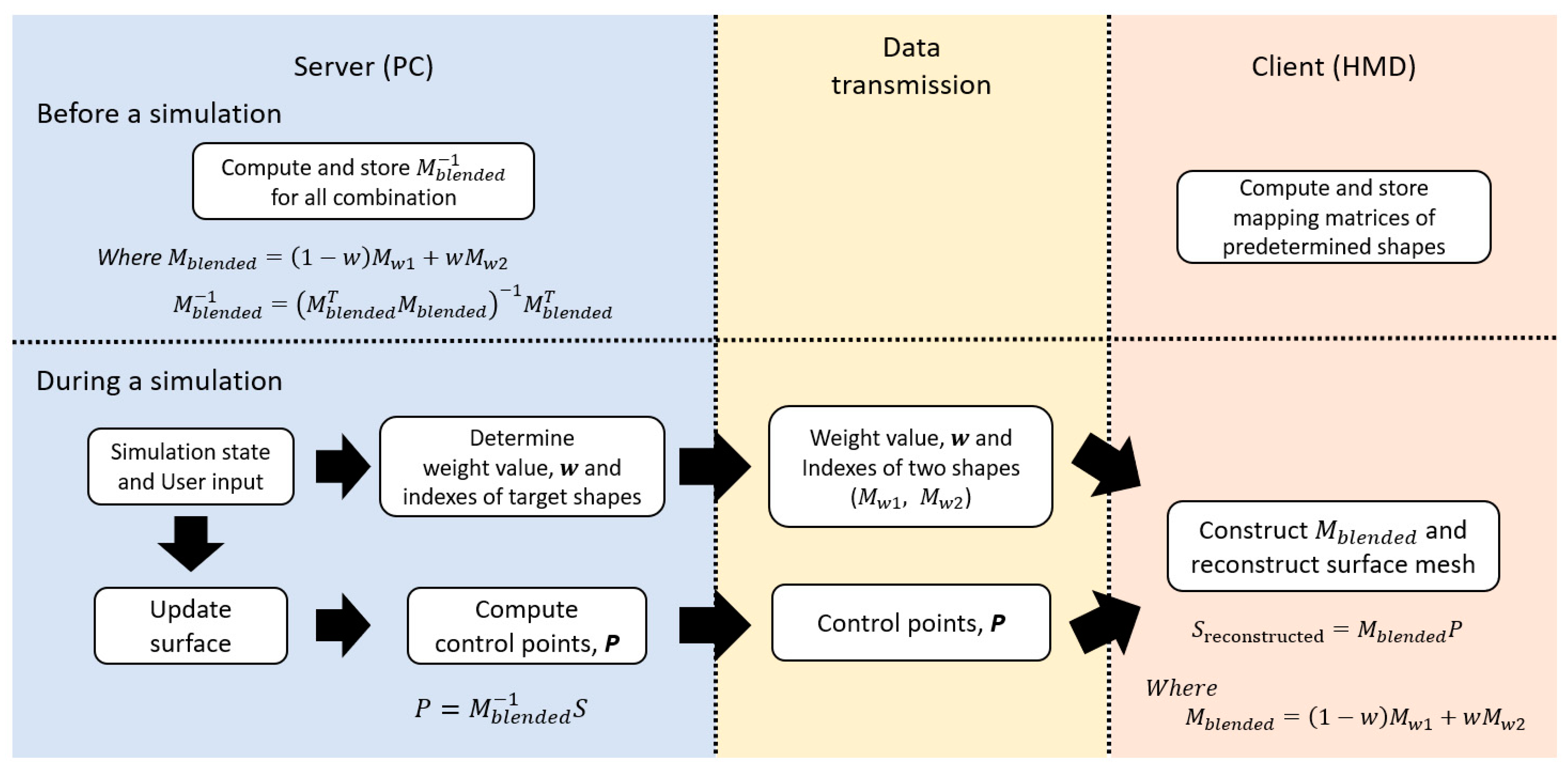
2.2. Multi-Shape Free-Form Deformation (MSFFD)
2.3. Framework Using MSFFD
3. Results
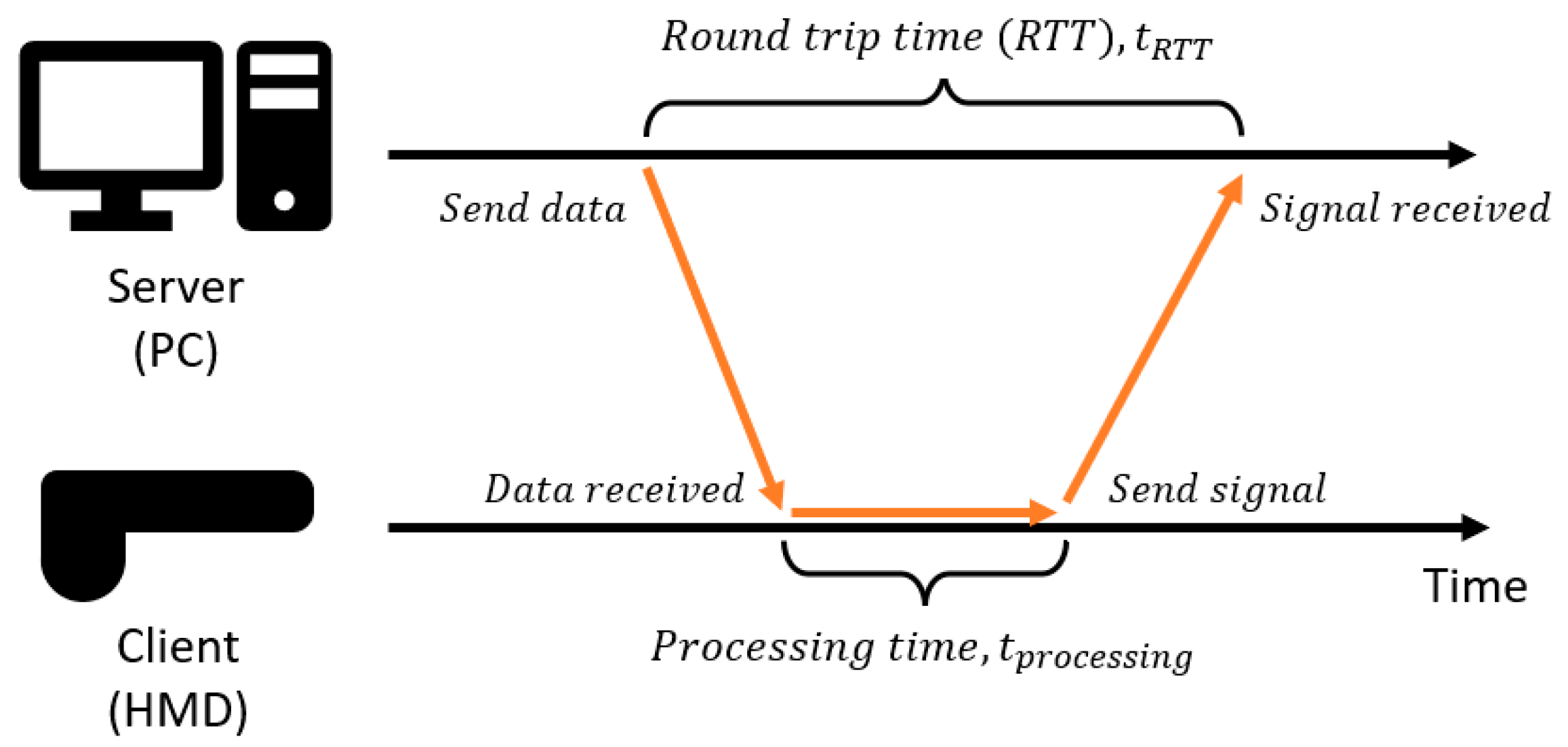
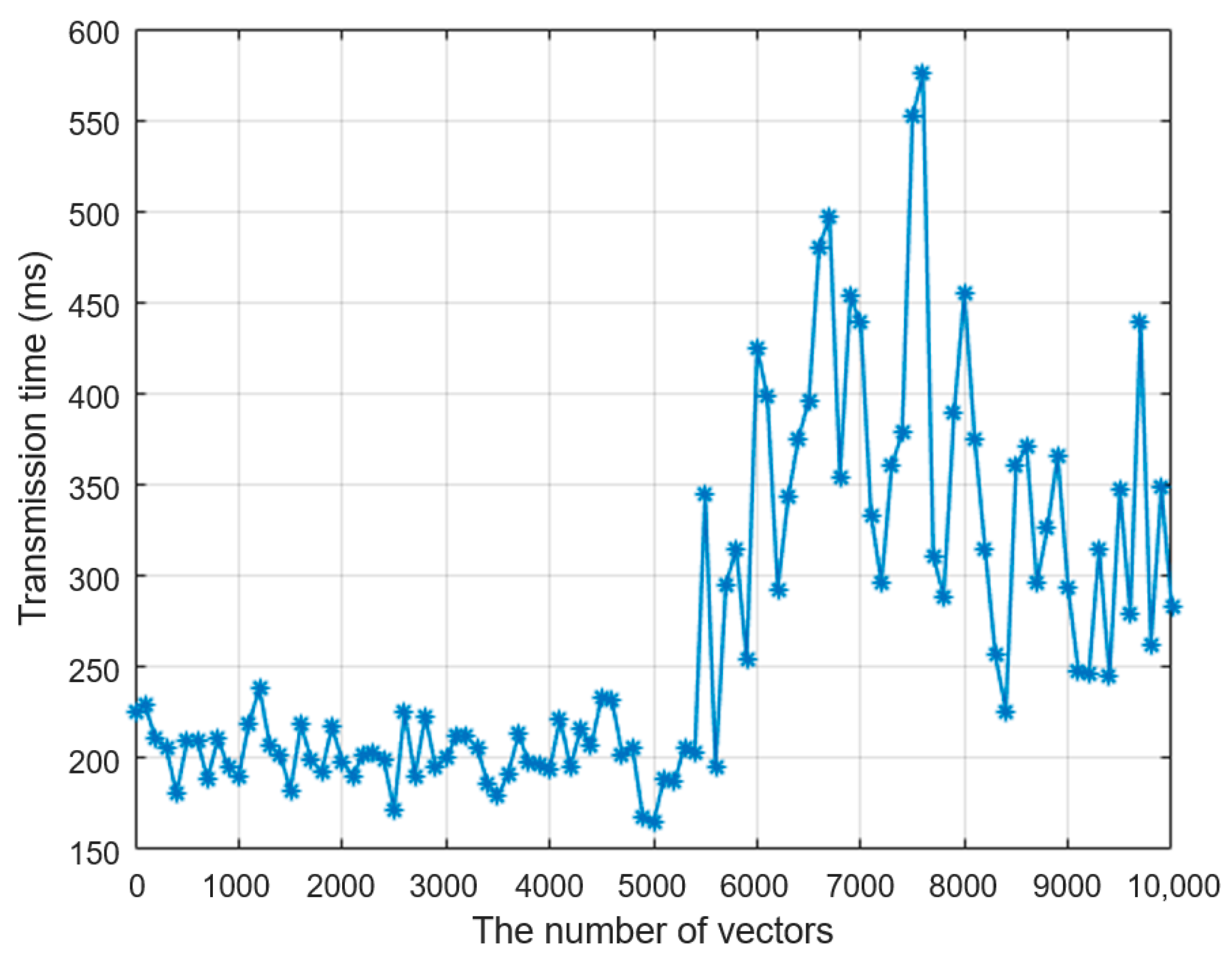
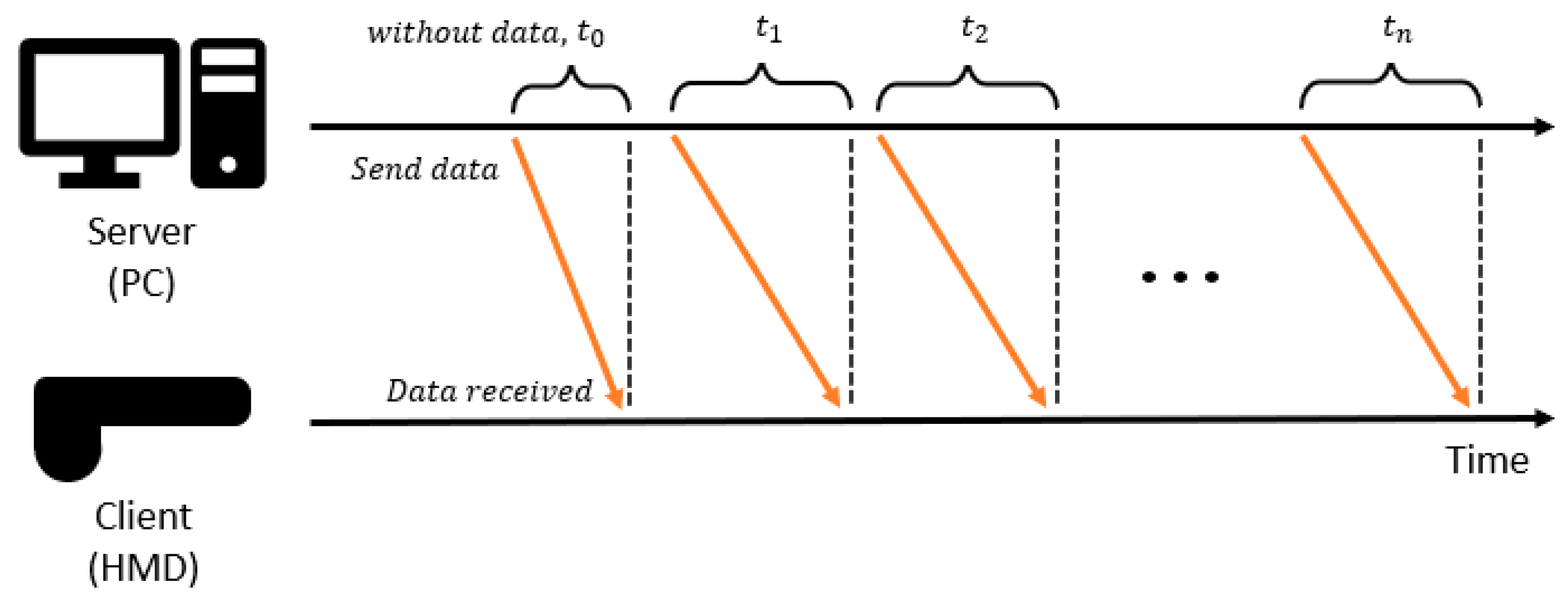
3.1. Round-Trip Time and Processing Time
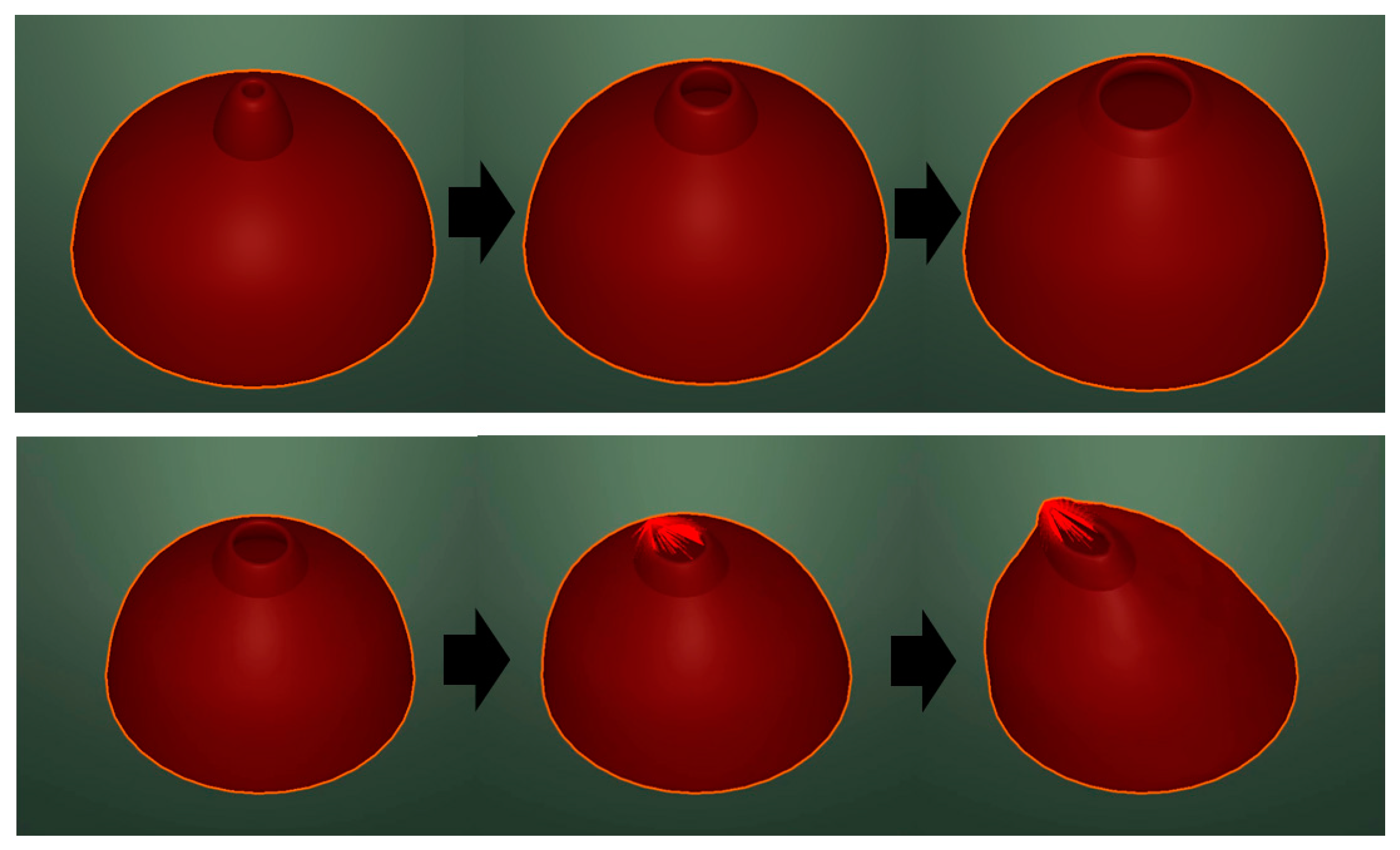
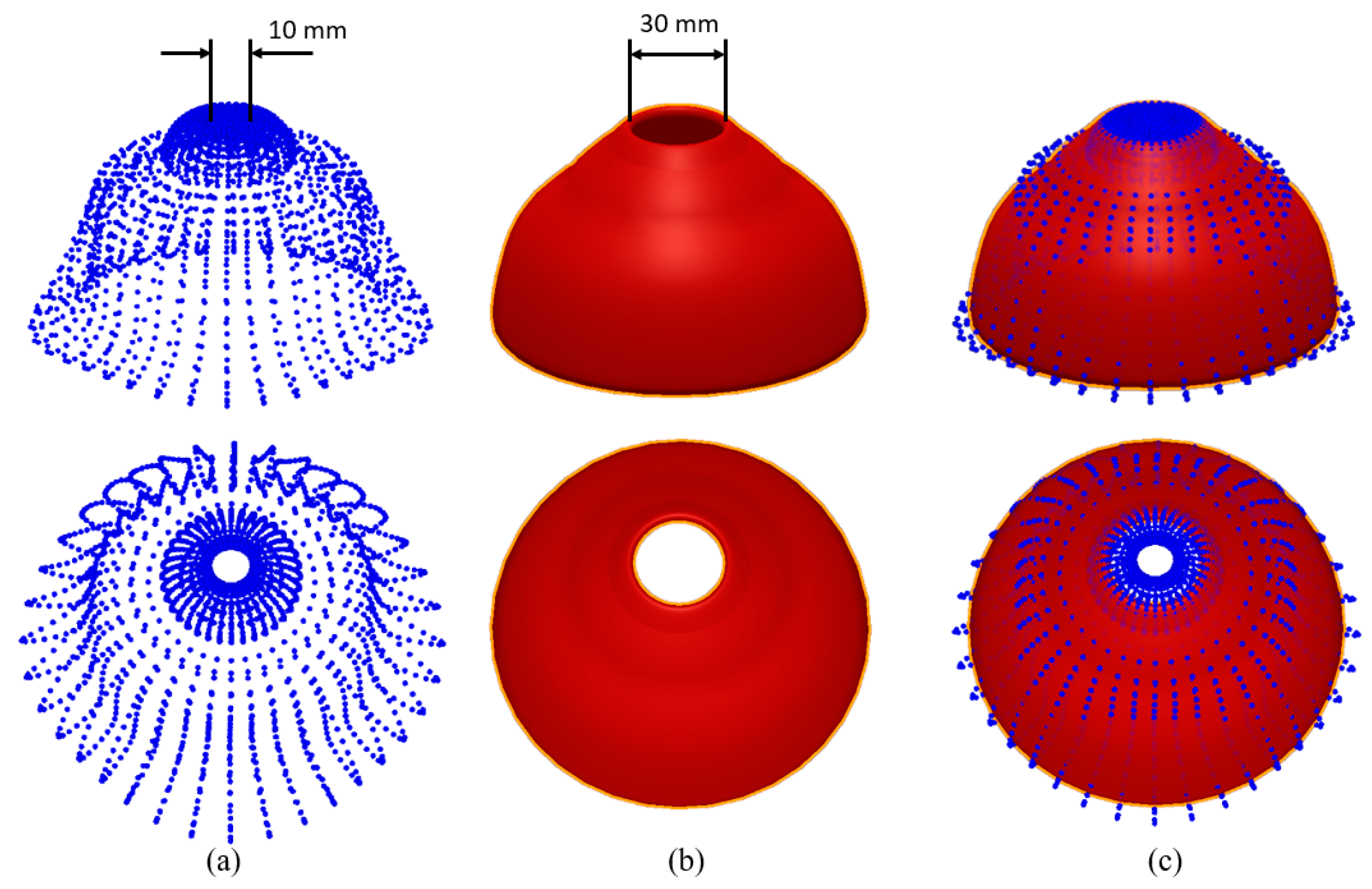
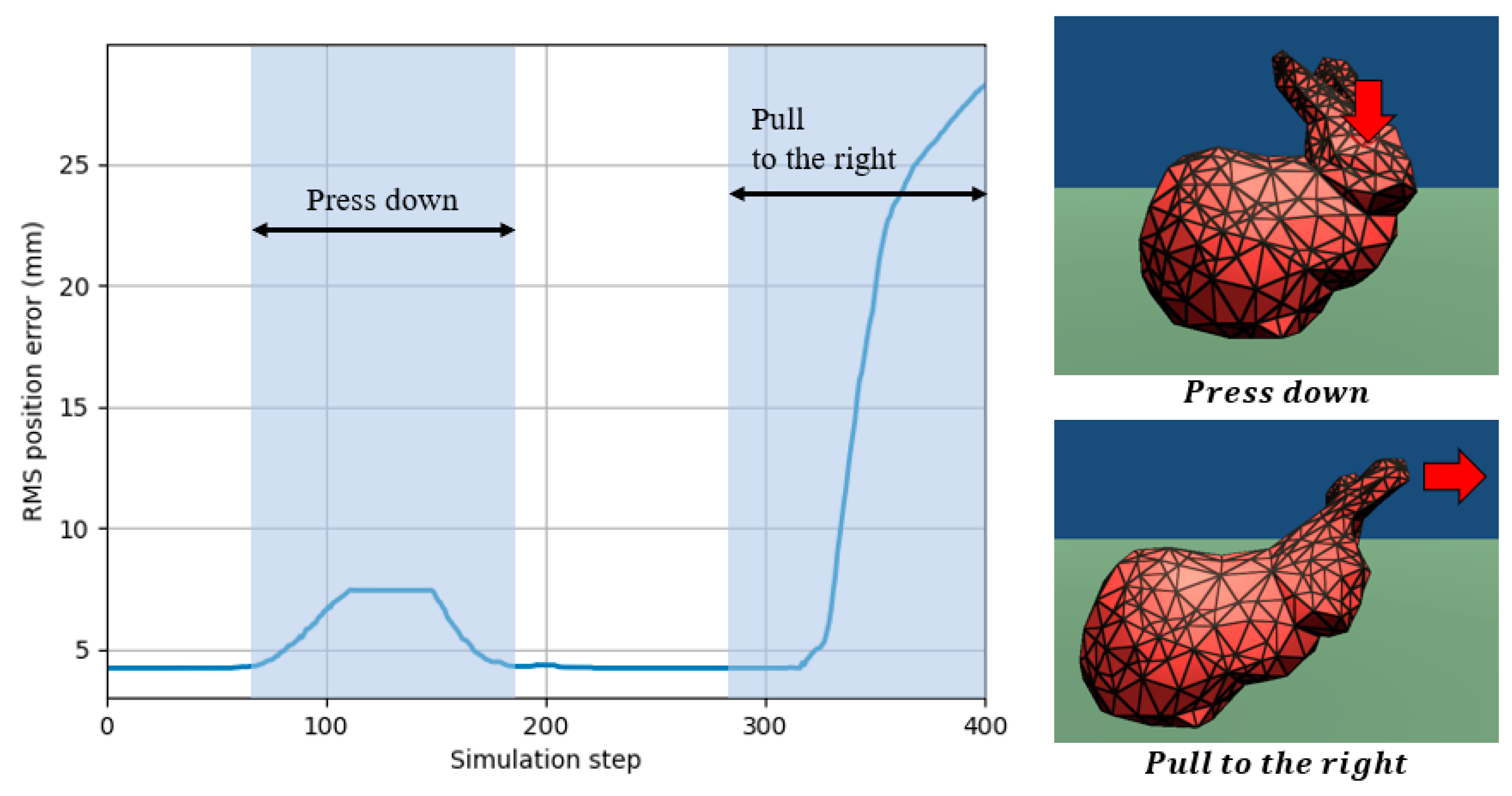
3.2. Verification on Stanford Bunny Simulation
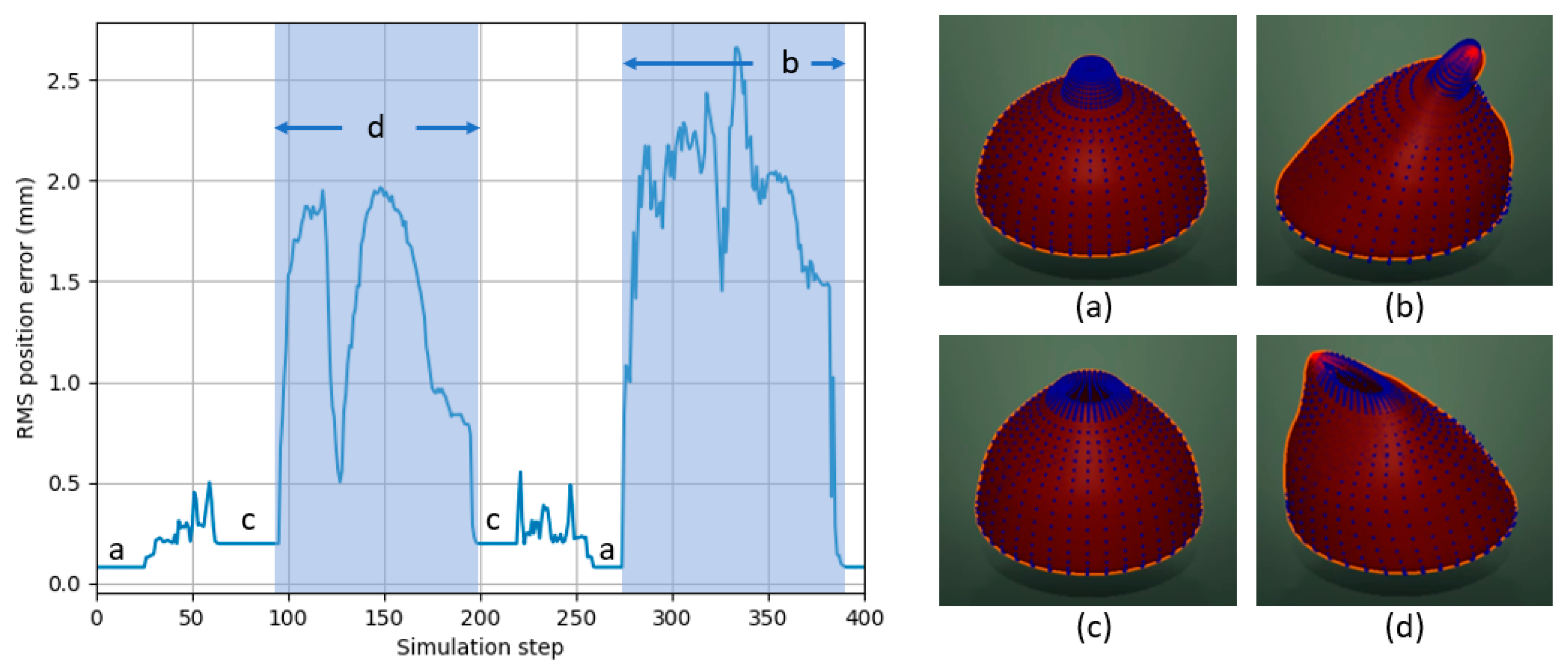
3.3. Verification on Vaginal Examination Simulation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kwon, H.-B.; Park, Y.-S.; Han, J.-S. Augmented Reality in Dentistry: A Current Perspective. Acta Odontol. Scand. 2018, 76, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, H.; Kim, Y.O. Virtual Reality and Augmented Reality in Plastic Surgery: A Review. Arch. Plast. Surg. 2017, 44, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayoub, A.; Pulijala, Y. The Application of Virtual Reality and Augmented Reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 238. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.; Bang, K.; Wetzstein, G.; Lee, B.; Gao, L. Toward the Next-Generation VR/AR Optics: A Review of Holographic near-Eye Displays from a Human-Centric Perspective. Optica 2020, 7, 1563–1578. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.B.; Tang, K.S.; Cheng, D.L.; Mi, E. Augmented Reality in Medical Education: A Systematic Review. Can. Med. Educ. J. 2020, 11, 81–96. [Google Scholar] [CrossRef]
- Barbieri, L.; Bruno, F.; Cosco, F.; Muzzupappa, M. Effects of Device Obtrusion and Tool-Hand Misalignment on User Performance and Stiffness Perception in Visuo-Haptic Mixed Reality. Int. J. Hum. Comput. Stud. 2014, 72, 846–859. [Google Scholar] [CrossRef]
- Nabiyouni, M.; Scerbo, S.; Bowman, D.A.; Höllerer, T. Relative Effects of Real-World and Virtual-World Latency on an Augmented Reality Training Task: An AR Simulation Experiment. Front. ICT 2016, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Gaffary, Y.; Le Gouis, B.; Marchal, M.; Argelaguet, F.; Arnaldi, B.; Lecuyer, A. AR Feels “Softer” than VR: Haptic Perception of Stiffness in Augmented versus Virtual Reality. IEEE Trans. Vis. Comput. Graph. 2017, 23, 2372–2377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, G.; Murray, D. Parallel Tracking and Mapping for Small AR Workspaces. In Proceedings of the 2007 6th IEEE and ACM International Symposium on Mixed and Augmented Reality (ISMAR), Nara, Japan, 13–16 November 2007; pp. 225–234. [Google Scholar] [CrossRef]
- Ababsa, F.E.; Mallem, M. Robust Camera Pose Estimation Using 2D Fiducials Tracking for Real-Time Augmented Reality Systems. In Proceedings of the 2004 ACM SIGGRAPH International Conference on Virtual Reality Continuum and Its Applications in Industry, Singapore, 16–18 June 2004; pp. 431–435. [Google Scholar] [CrossRef] [Green Version]
- Koulieris, G.A.; Akşit, K.; Stengel, M.; Mantiuk, R.K.; Mania, K.; Richardt, C. Near-Eye Display and Tracking Technologies for Virtual and Augmented Reality. Comput. Graph. Forum 2019, 38, 493–519. [Google Scholar] [CrossRef]
- Lu, S.; Perdomo, Y.P.S.; Jiang, X.; Zheng, B. Integrating Eye-Tracking to Augmented Reality System for Surgical Training. J. Med. Syst. 2020, 44, 192. [Google Scholar] [CrossRef] [PubMed]
- Arias, T.; Tran, A.; Breaud, J.; Fournier, J.P.; Bongain, A.; Delotte, J. A Prospective Study into the Benefits of Simulation Training in Teaching Obstetric Vaginal Examination. Int. J. Gynecol. Obstet. 2016, 133, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Shea, K.L.; Rovera, E.J. Vaginal Examination Simulation Using Citrus Fruit to Simulate Cervical Dilation and Effacement. Cureus 2015, 7, e314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sederberg, T.W.; Parry, S.R. Free-Form Deformation of Solid Geometric Models. In SIGGRAPH ’86: Proceedings of the 13th Annual Conference on Computer Graphics and Interactive Techniques; Association for Computing Machinery: New York, NY, USA, 1986; Volume 20, pp. 151–160. [Google Scholar] [CrossRef]
- Coquillart, S. Extended Free-Form Deformation: A Sculpturing Tool for 3D Geometric Modeling. In SIGGRAPH ’90: Proceedings of the 17th Annual Conference on Computer Graphics and Interactive Techniques; Association for Computing Machinery: New York, NY, USA, 1990; Volume 24, pp. 187–196. [Google Scholar] [CrossRef] [Green Version]
- Peterlik, I.; Nouicer, M.; Duriez, C.; Cotin, S.; Kheddar, A. Constraint-Based Haptic Rendering of Multirate Compliant Mechanisms. IEEE Trans. Haptics 2011, 4, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Maskey, N.; Horsmanheimo, S.; Tuomimäki, L. Analysis of Latency for Cellular Networks for Smart Grid in Suburban Area. In Proceedings of the 2014 5th IEEE PES Innovative Smart Grid Technologies Europe (ISGT Europe), Istanbul, Turkey, 12–15 October 2014; pp. 1–4. [Google Scholar] [CrossRef]
- García, B.; Gortázar, F.; López-fernández, L.; Gallego, M.; París, M. WebRTC Testing: Challenges and Practical Solutions. IEEE Commun. Stand. Mag. 2017, 1, 36–42. [Google Scholar] [CrossRef]
- Müller, M.; Heidelberger, B.; Hennix, M.; Ratcliff, J. Position Based Dynamics. J. Vis. Commun. Image Represent. 2007, 18, 109–118. [Google Scholar] [CrossRef] [Green Version]
- di Luca, M. New Method to Measure End-to-End Delay of Virtual Reality. Presence Teleoperators Virtual Environ. 2010, 19, 569–584. [Google Scholar] [CrossRef]
- Elbamby, M.S.; Perfecto, C.; Bennis, M.; Doppler, K. Toward Low-Latency and Ultra-Reliable Virtual Reality. IEEE Netw. 2018, 32, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Ono, Y.; Chen, B.Y.; Nishita, T.; Feng, J. Free-Form Deformation with Automatically Generated Multiresolution Lattices. In Proceedings of the 2002 1st International Symposium on Cyber Worlds, Tokyo, Japan, 6–8 November 2002; pp. 472–479. [Google Scholar] [CrossRef]
- Feng, J.; Shao, J.; Jin, X.; Peng, Q.; Forrest, A.R. Multiresolution Free-Form Deformation with Subdivision Surface of Arbitrary Topology. Vis. Comput. 2006, 22, 28–42. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Required Information | The Number of Vectors | Average Latency | Maximum Latency | |
|---|---|---|---|---|
| w/o the proposed framework | 524 surface vertices 524 normals | 1048 | 281 ms | 315 ms |
| w/the proposed framework | 48 control points | 48 | 6 ms | 51 ms |
| Reduction rate | 95.4% | 97.9% | 83.8% |
| Required Information | The Number of Vectors | Average Latency | Maximum Latency | |
|---|---|---|---|---|
| w/o the proposed framework | 4560 surface vertices 4560 normals | 9160 | 18,969 ms | 40,092 ms |
| w/the proposed framework | 104 control points weight value | 104 | 7 ms | 33 ms |
| Reduction rate | 93.0% | 99.9% | 99.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Bello, F. Multi-Shape Free-Form Deformation Framework for Efficient Data Transmission in AR-Based Medical Training Simulators. Appl. Sci. 2021, 11, 9925. https://doi.org/10.3390/app11219925
Kim M, Bello F. Multi-Shape Free-Form Deformation Framework for Efficient Data Transmission in AR-Based Medical Training Simulators. Applied Sciences. 2021; 11(21):9925. https://doi.org/10.3390/app11219925
Chicago/Turabian StyleKim, Myeongjin, and Fernando Bello. 2021. "Multi-Shape Free-Form Deformation Framework for Efficient Data Transmission in AR-Based Medical Training Simulators" Applied Sciences 11, no. 21: 9925. https://doi.org/10.3390/app11219925
APA StyleKim, M., & Bello, F. (2021). Multi-Shape Free-Form Deformation Framework for Efficient Data Transmission in AR-Based Medical Training Simulators. Applied Sciences, 11(21), 9925. https://doi.org/10.3390/app11219925