
Technology Acceptance in Healthcare: A Systematic Review



Abstract
:1. Introduction
2. Literature Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Multiple Acceptance Models | Multiple Technologies | Databases | Coverage | Aim |
|---|---|---|---|---|---|
| [30] | - | ✓ | 16 datasets (names not reported) | Before July 2008 (not clearly reported) | Literature review of 20 articles to study the application of TAM in the healthcare domain. |
| [40] | - | - | PubMed, EMBASE, CINAHL, Business Source Premier, Science Citation Index, Social Sciences Citation Index, Cochrane Library, ABI/Inform, and PsychINFO | 1999–2009 | Systematic review for 60 studies to explore the barriers and facilitators to implementation. |
| [41] | - | ✓ | MEDLINE, EMBASE, CINAHL, Cochrane, Ovid, DARE, Biosis Previews, PsycINFO, HSTAT, ERIC, ProQuest, ISI Web of Knowledge, LILACS, and Ingenta | 19–0–2007 | Systematic review for 101 studies to explore the factors that facilitate or limit the implementation of ICTs in clinical settings. |
| [42] | - | ✓ | MEDLINE, EMBASE, CINAHL, PSYCINFO, and the Cochrane Library | 19–5–2009 | Systematic review for 37 review studies to identify the barriers and facilitators to e-health implementation and outstanding gaps in the literature. |
| [43] | - | ✓ | Science Direct, Springer, TÜBĐTAK EKUAL, Taylor and Francis, EBSCO Host, and Blackwell | 19–9–2010 | Qualitative review to analyze 50 articles to study the possible predictors of TAM. |
| [33] | ✓ | ✓ | ACM Digital Library, CINAHL, IEEE Xplore, MEDLINE, PsycINFO, Scopus, and Web of Science | Not specified | Systematic review for 16 studies provides an overview of factors that influence the acceptance of electronic technologies that support older adults. |
| [44] | - | - | PubMed, EMBASE, CINAHL, and PsychINFO | 20–0–2014 | Systematic review for 33 studies to explore the factors influencing healthcare professionals’ adoption of mobile health applications. |
| [45] | - | - | Google Scholar | 20–0–2015 | Systematic review for 44 studies to review the main barriers to adopt assistive technologies by older adults. |
| Med-line, Embase, CINAHL, PsycINFO, and Scopus | 19–6–2015 | ||||
| [6] | - | ✓ | Web of Science, PubMed, and Scopus | 19–9–2017 | Systematic review to analyze 134 TAM-based studies in health information systems. The study aims to understand the existing research and debates as is relevant to TAM in the healthcare domain. |
| [34] | ✓ | ✓ | Medline, Embase, CINAHL, Cochrane, Scopus, and Web of Science | 19–8–2018 | Systematic review for 13 studies to identify the methods utilized to assess the users’ acceptance of rehabilitation technologies for adults with moderate to severe traumatic brain injury. |
| This study | ✓ | ✓ | PubMed, IEEE Xplore, Springer, ACM, Science Direct, and Google Scholar | 20–0–2019 | Systematic review that includes 142 studies for technology acceptance in healthcare to classify the studies based on the technology acceptance models, the studied information technologies, participants, and countries of implementation. The study also aims to identify the prevailing acceptance models, most utilized factors, and the most confirmed relationships to address the literature gaps and help to build integrated models for technology acceptance in the healthcare domain. |
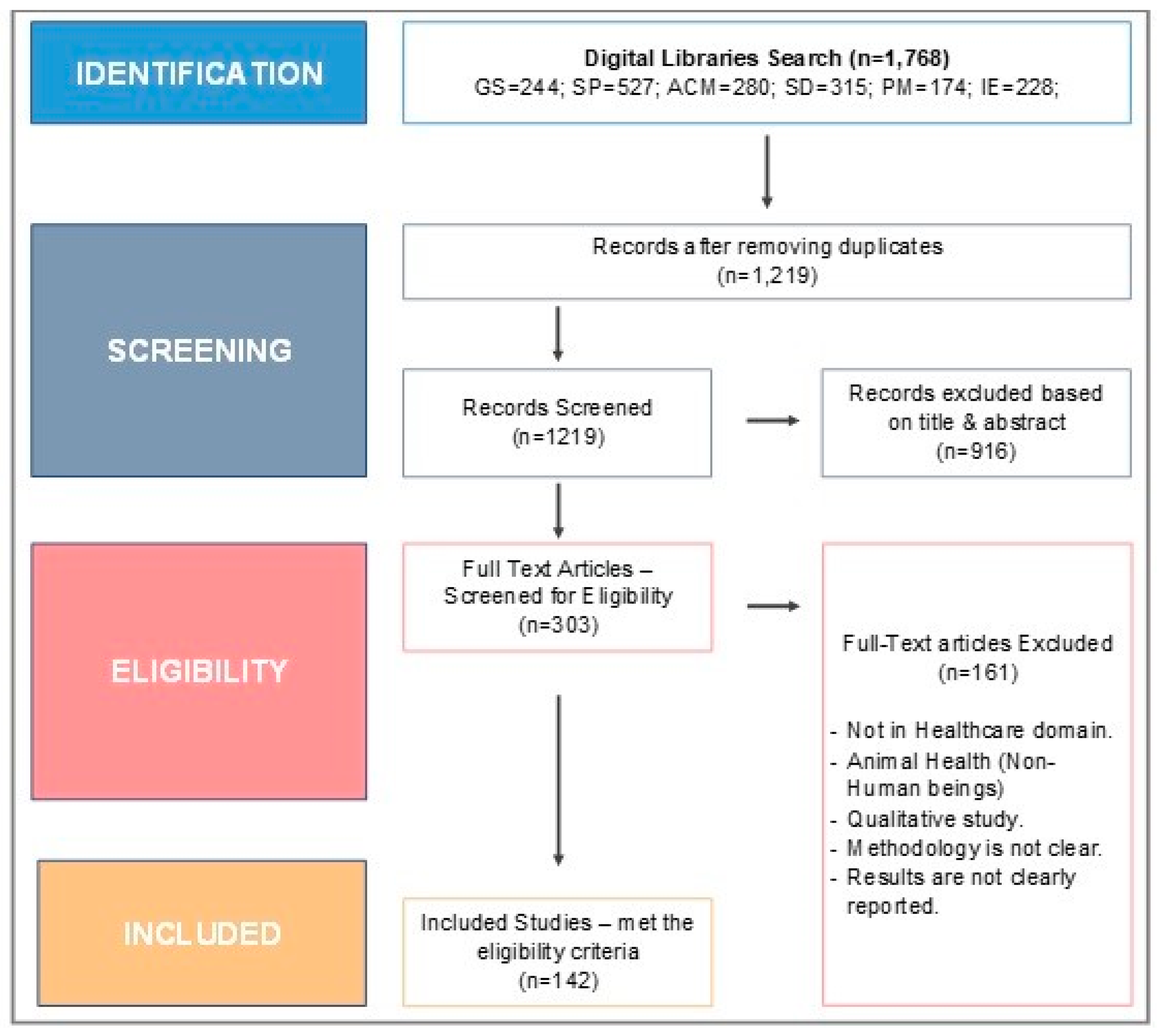
3. Materials and Methods
3.1. Inclusion/Exclusion Criteria
3.2. Data Sources and Search Strategy
3.3. Data Abstraction and Analysis
3.4. Quality Assessment
4. Results
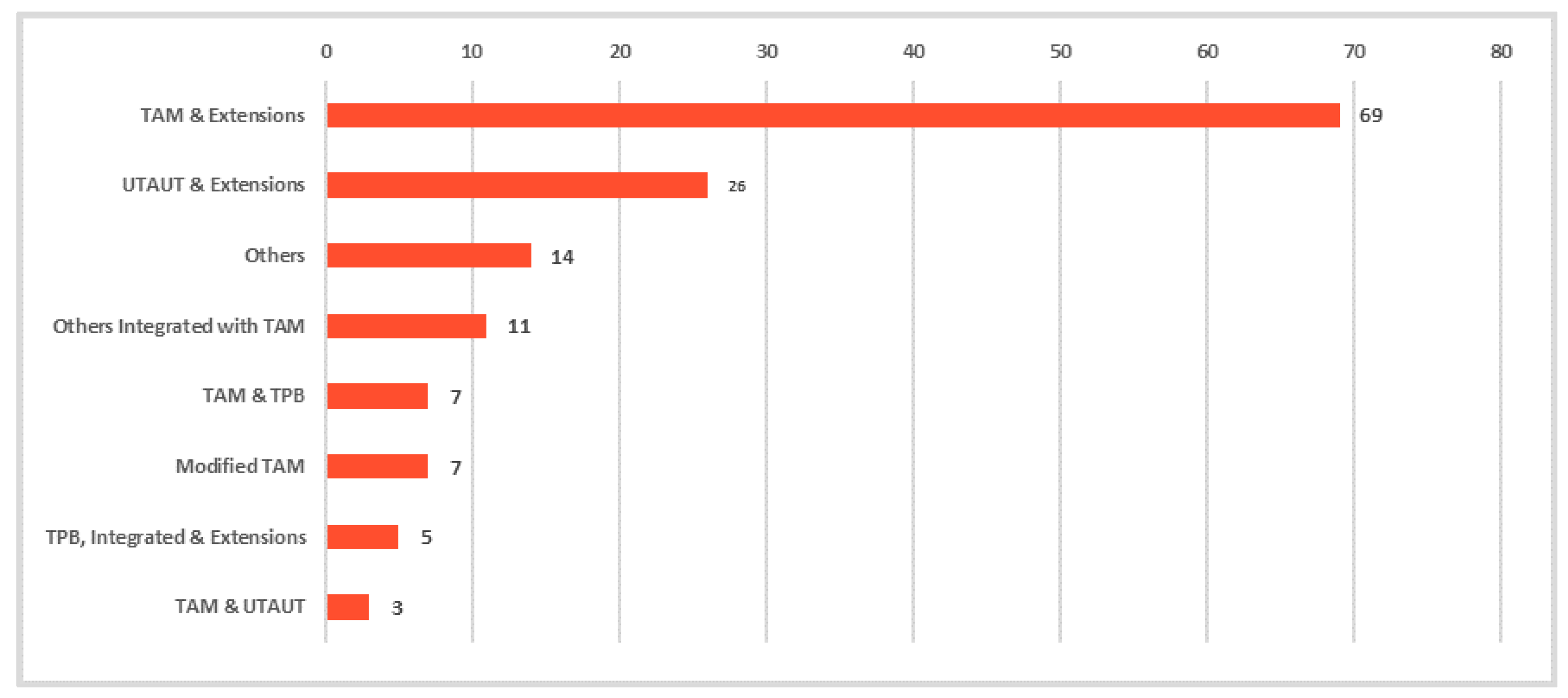
4.1. Prevailing Technology Acceptance Models and Theories in the Healthcare Domain
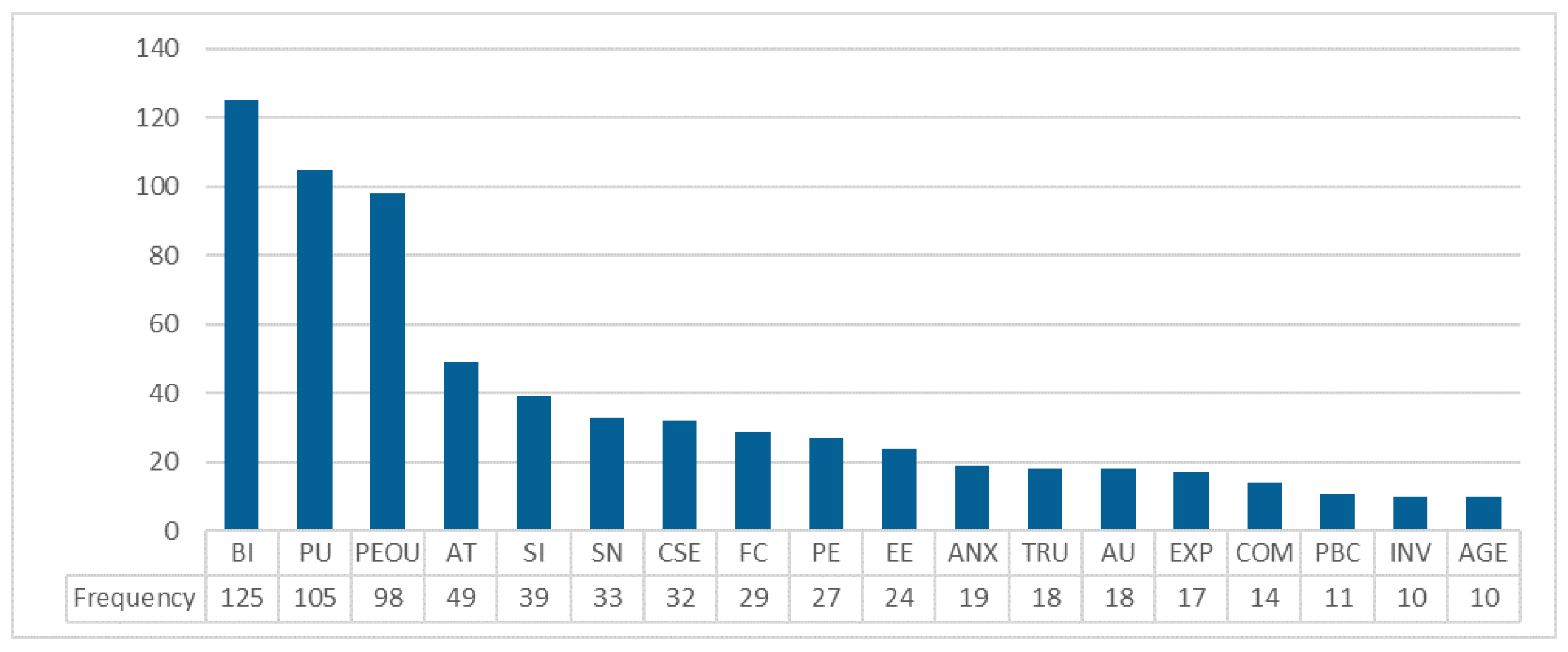
4.2. Key Factors Affecting Technology Acceptance in the Healthcare Domain
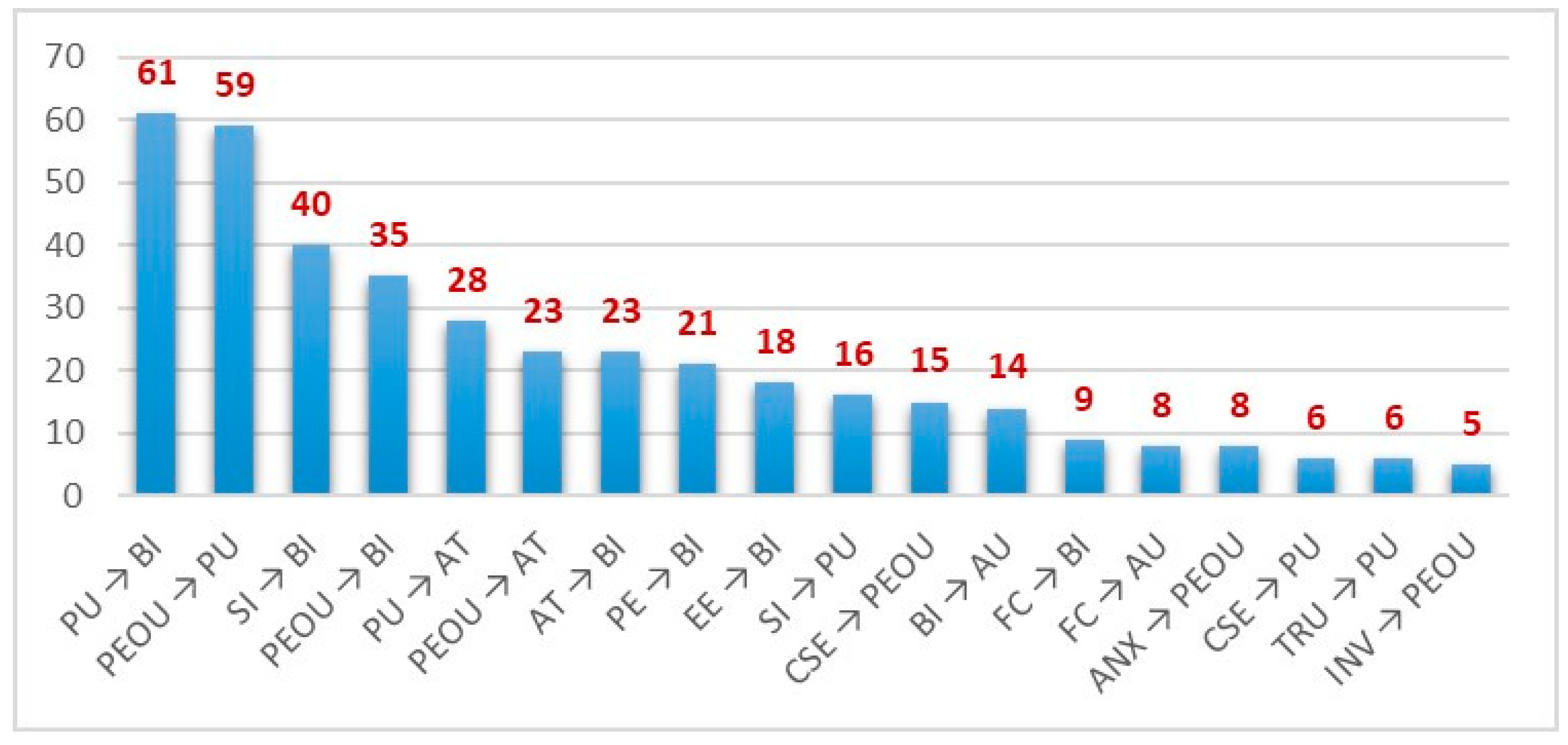
4.3. Main Confirmed Relationships among the Influential Factors
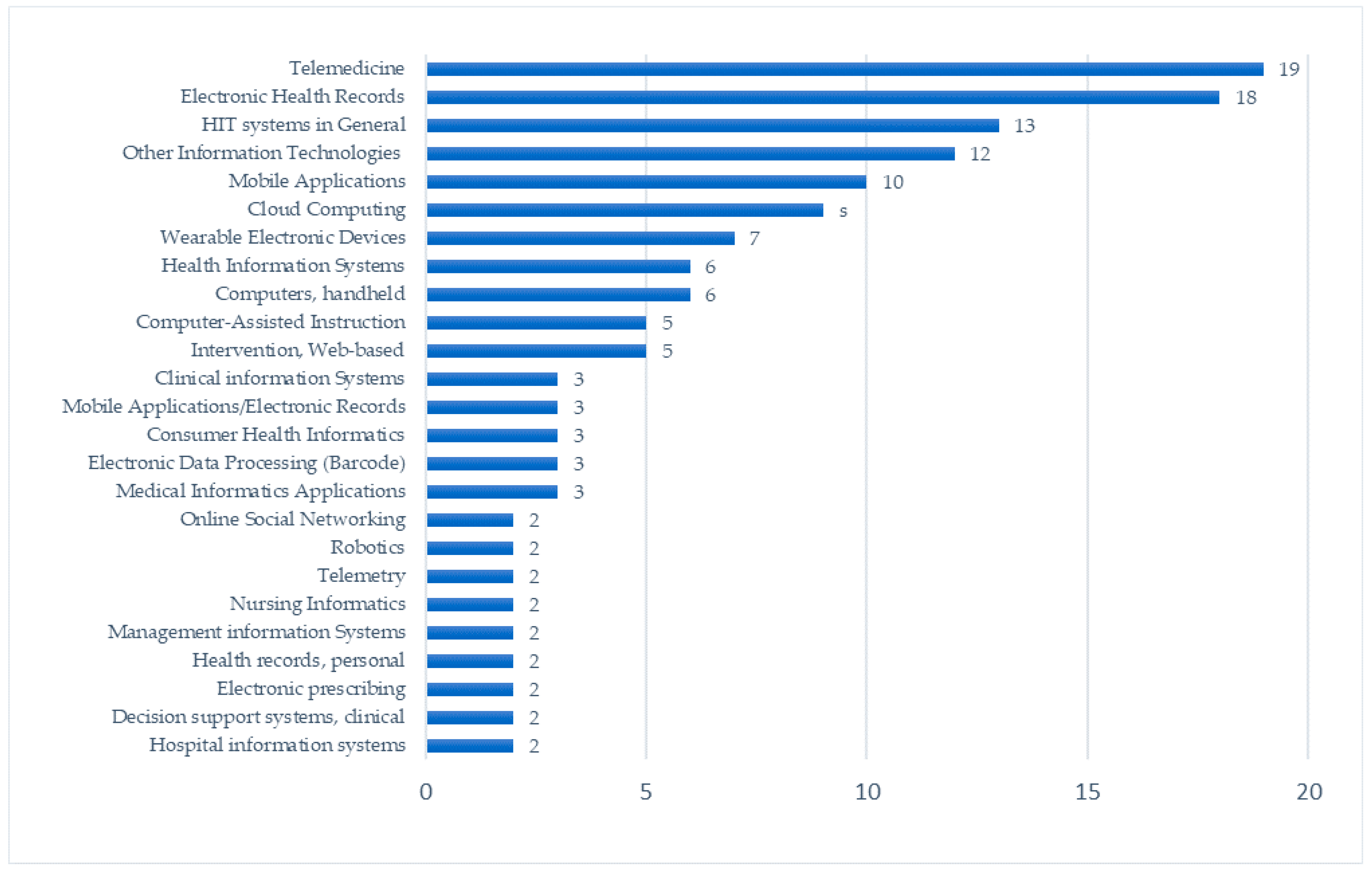
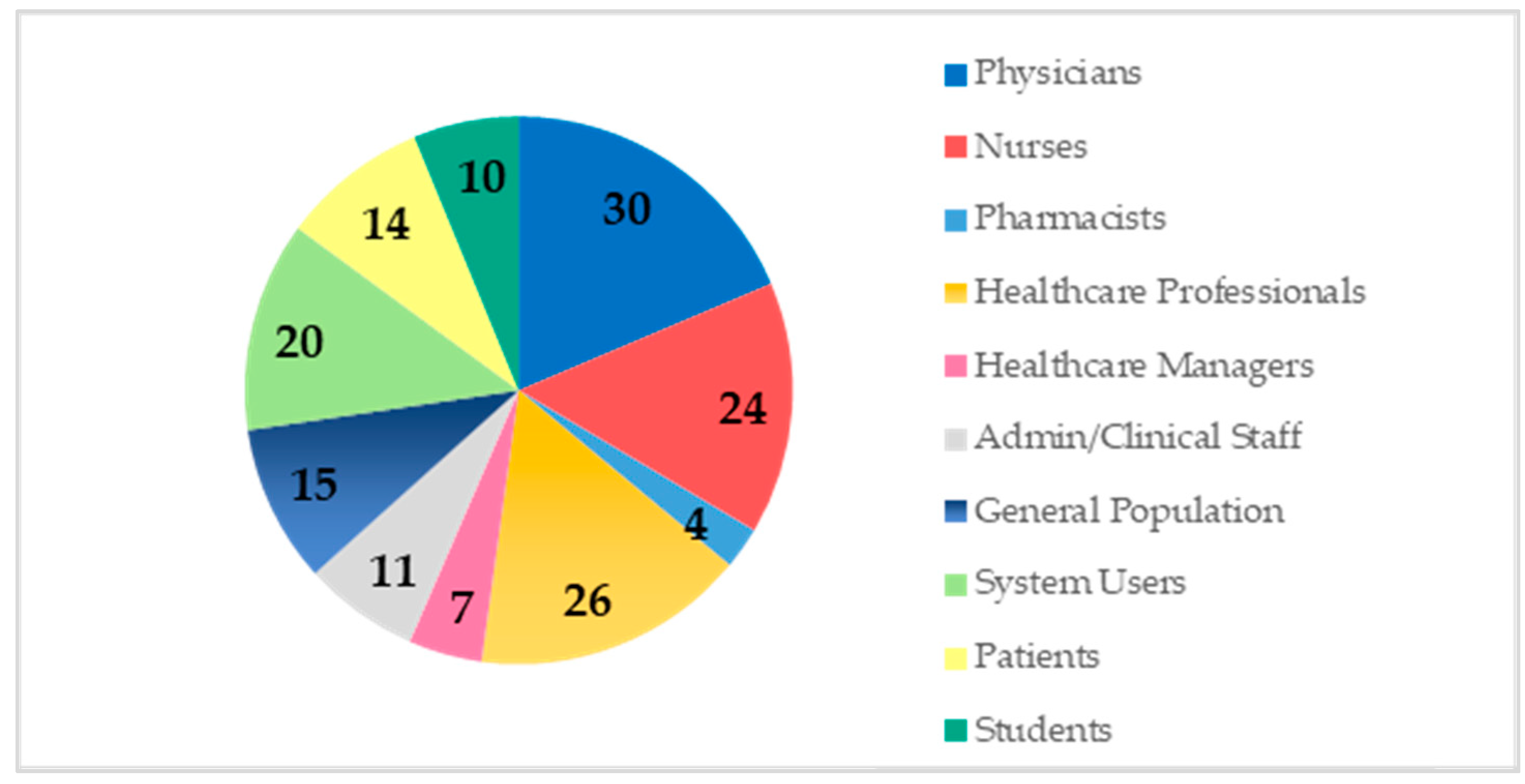
4.4. Main Information Technologies and Their Relationships with Countries and Participants
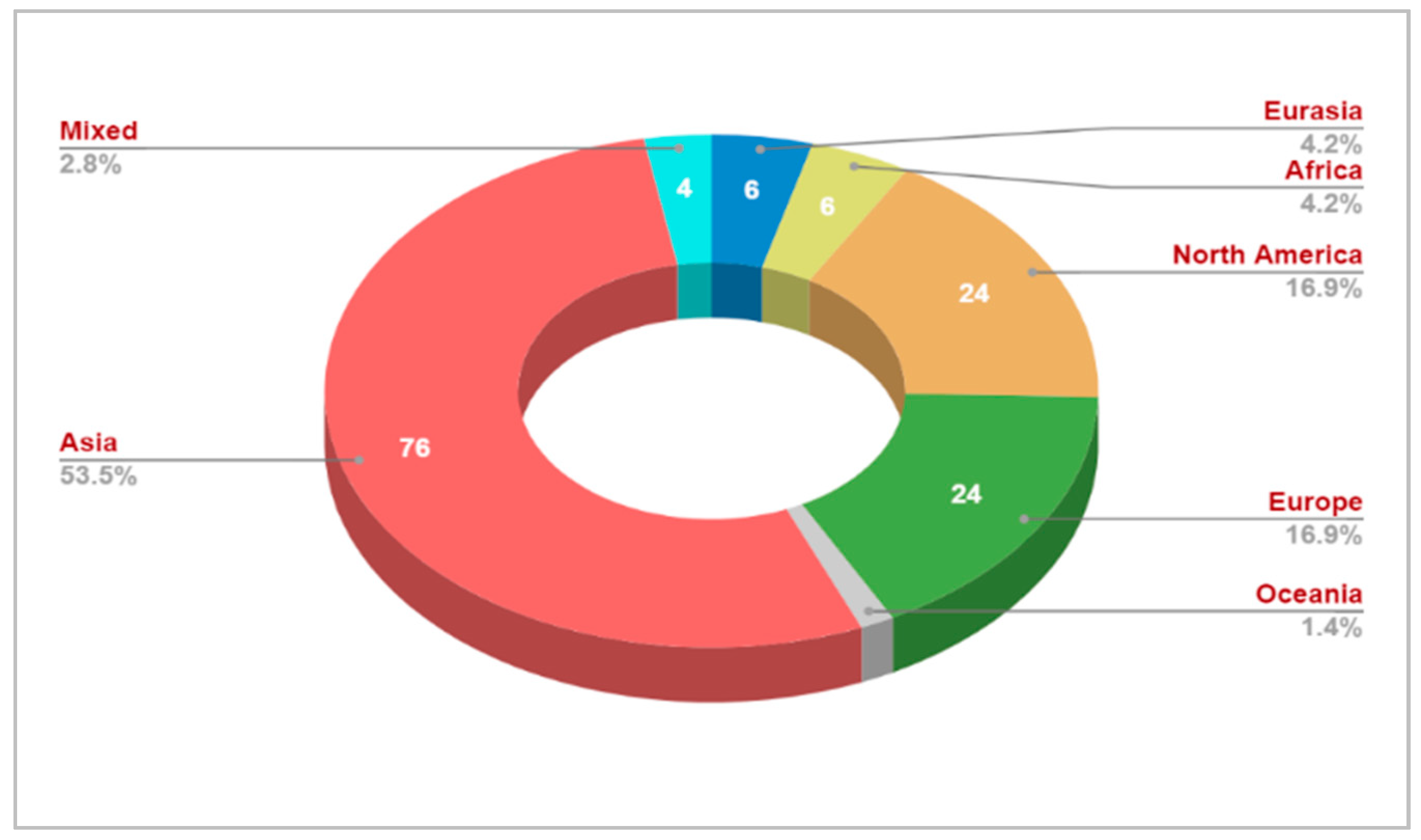
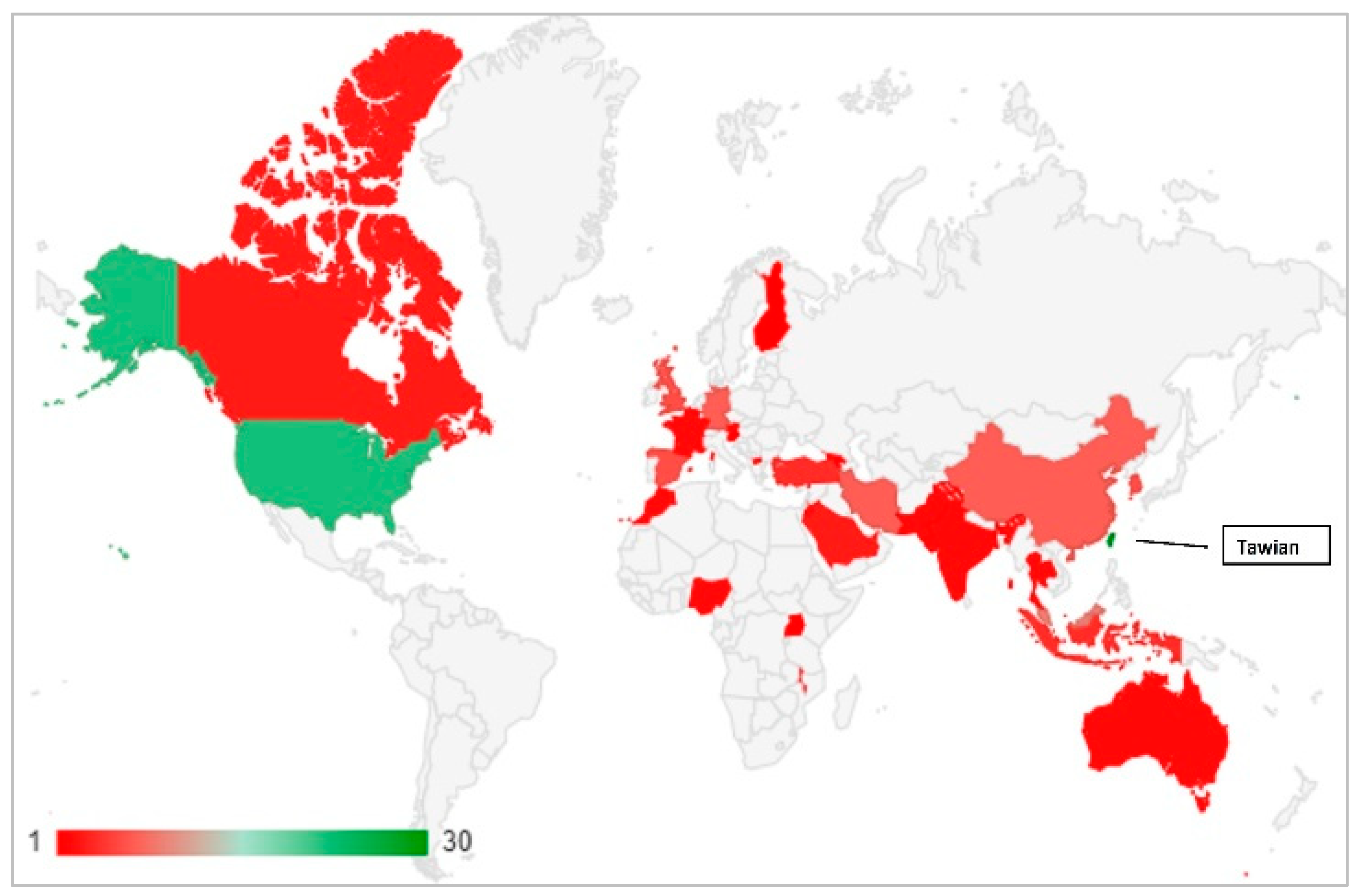
4.5. Distribution of Studies across Regions and Countries
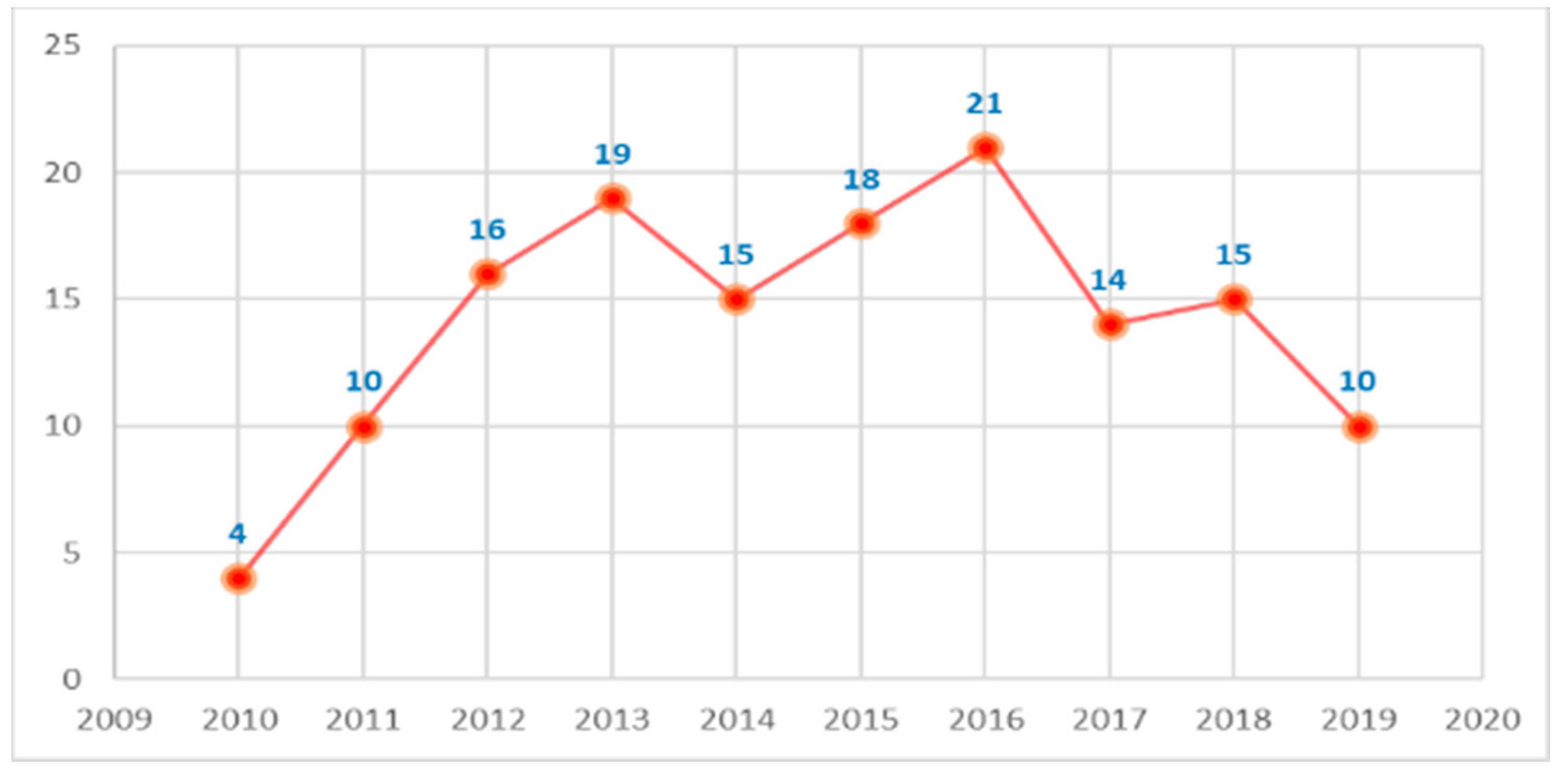
4.6. Progress of Technology Acceptance Studies in Healthcare
5. Discussion
6. Conclusions
6.1. Theoretical Contributions
6.2. Practical Implications
6.3. Limitations and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Total | Percentage | Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Total | Percentage |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S1 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% | S72 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S2 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% | S73 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% |
| S3 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% | S74 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S4 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S75 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S5 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S76 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% |
| S6 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% | S77 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S7 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% | S78 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% |
| S8 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% | S79 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S9 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 0.5 | 5.5 | 78.6% | S80 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S10 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S81 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S11 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S82 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S12 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S83 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S13 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 0.5 | 5.5 | 78.6% | S84 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S14 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S85 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S15 | 1 | 1 | 0.5 | 0 | 0.5 | 1 | 1 | 5 | 71.4% | S86 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S16 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% | S87 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% |
| S17 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 6.5 | 92.9% | S88 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S18 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S89 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S19 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S90 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% |
| S20 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% | S91 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S21 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% | S92 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 6.5 | 92.9% |
| S22 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% | S93 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S23 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S94 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S24 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S95 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S25 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S96 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S26 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S97 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S27 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S98 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S28 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% | S99 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S29 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% | S100 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S30 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% | S101 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% |
| S31 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% | S102 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S32 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S103 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S33 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S104 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% |
| S34 | 1 | 1 | 0.5 | 0 | 0.5 | 1 | 1 | 5 | 71.4% | S105 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S35 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% | S106 | 1 | 1 | 0.5 | 0.5 | 1 | 1 | 0.5 | 5.5 | 78.6% |
| S36 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% | S107 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S37 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S108 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S38 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S109 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S39 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S110 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S40 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S111 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S41 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S112 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S42 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S113 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S43 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 5 | 71.4% | S114 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | 100.0% |
| S44 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% | S115 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% |
| S45 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% | S116 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S46 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S117 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S47 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S118 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% |
| S48 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% | S119 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S49 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% | S120 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% |
| S50 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% | S121 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S51 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S122 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S52 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S123 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 5.5 | 78.6% |
| S53 | 1 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 5.5 | 78.6% | S124 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S54 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 0.5 | 5 | 71.4% | S125 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S55 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S126 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S56 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% | S127 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S57 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S128 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% |
| S58 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% | S129 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% |
| S59 | 1 | 1 | 0.5 | 0.5 | 0.5 | 1 | 1 | 5.5 | 78.6% | S130 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 6.5 | 92.9% |
| S60 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S131 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S61 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S132 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | 100.0% |
| S62 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 6 | 85.7% | S133 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S63 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% | S134 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% |
| S64 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% | S135 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S65 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S136 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% |
| S66 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6 | 85.7% | S137 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S67 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S138 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% |
| S68 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% | S139 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% |
| S69 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S140 | 1 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.5 | 78.6% |
| S70 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 5 | 71.4% | S141 | 1 | 1 | 1 | 0 | 0.5 | 0.5 | 0.5 | 4.5 | 64.3% |
| S71 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 5.5 | 78.6% | S142 | 1 | 1 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 5 | 71.4% |
Appendix B
| Sr. | Source | Year | Article Type | Studied Technology | Sample Size | Sample Type | Country | Acceptance Model |
|---|---|---|---|---|---|---|---|---|
| 1 | Bennani and Oumlil [84] | 2010 | Conference | ICT Appropriation | 111 | Physicians and Nurses | Morocco | TAM |
| 2 | Lai and Li [85] | 2010 | Conference | Computer Assistance Orthopedic Surgery System | 115 | Healthcare Professionals | Taiwan | Integrated Model: TAM and TPB |
| 3 | Kim et al. [86] | 2010 | Journal Article | Tele-Homecare Technology (Telemedicine) | 40 | Physicians | USA | Compare Two Models: TAM and TPB |
| 4 | Holtz [87] | 2010 | PHD Dissertation | Electronic Medical Records | 113 | Nurses | USA | UTAUT |
| 5 | Pai and Huang [88] | 2011 | Journal Article | Healthcare Information Systems | 366 | Nurses, Head Directors, and Other Related Personnel | Taiwan | Integrated Model: TAM and IS Success Model |
| 6 | Orruño et al. [89] | 2011 | Journal Article | Tele-Dermatology System | 171 | Physicians | Spain | Modified TAM |
| 7 | Maarop et al. [90] | 2011 | Conference | Teleconsultation Technology | 72 | Healthcare Providers | Malaysia | Extended TAM |
| 8 | Schnall and Bakken [91] | 2011 | Journal Article | Continuity of Care Record (CCR) with Context-Specific Links | 94 | HIV Case Managers | USA | Extended TAM |
| 9 | Kowitlawakul [92] | 2011 | Journal Article | eICU Telemedicine Technology | 117 | Registered Nurses | USA | Telemedicine TAM (TTAM)—Extended TAM |
| 10 | Damanhoori et al. [93] | 2011 | Conference | Breast Self-Examination Teleconsultation | 279 | Female Citizens | Malaysia | TAM |
| 11 | Lim et al. [94] | 2011 | Journal Article | Mobile Phones to Seek Health Information | 175 | Female Citizens 21+ | Singapore | Extended TAM |
| 12 | Mohamed, Tawfik, and Norton [95] | 2011 | Conference | Electronic Health Technologies | 50 | Participants—Not Specified | UAE and UK | E-Health Technology Acceptance Model (E-HTAM)—Extended TAM |
| 13 | Ortega Egea and Román González [96] | 2011 | Journal Article | Electronic Health Care Records (EHCR) | 254 | Physicians | Spain | Extended TAM |
| 14 | Mohamed, Tawfik, and Al-Jumeily [97] | 2011 | Conference | Smart Mobile Phone in the Medical Domain | 229 | Students Medical Practitioners, Ministry of Health Staff and Universities Staff | UAE and UK | Mobile Technology Acceptance Model (Mo-HTAM)—Extended TAM |
| 15 | Ketikidis et al. [7] | 2012 | Journal Article | Health Information Technology (HIT) | 133 | Healthcare Professionals: Doctors and Nurses | North Macedonia | Modified TAM2 |
| 16 | Chong and Chan [98] | 2012 | Book Chapter | Radio Frequency Identification (RFID) | 183 | Managers, Heads of Departments, IT Managers, or Logistic Mangers of the Healthcare Companies and Hospitals | Malaysia | Extended TAM |
| 17 | Kim and Park [99] | 2012 | Journal Article | Health Information Technology (HIT) | 728 | Users of Online Health Information | South Korea | Integrated Model-Health Information Technology Acceptance Model (HITAM): HBM, TPB, and TAM |
| 18 | Terrizzi et al. [100] | 2012 | Conference | Integrated Electronic Health Records (IEHR) | 31 | Physicians and Office Staff | USA | Extended TAM |
| 19 | Chow et al. [101] | 2012 | Journal Article | Online Virtual Health Learning: Rapid Sequence Intubation (RSI) | 206 | Nursing Students | Hong Kong | Extended TAM |
| 20 | Asua et al. [102] | 2012 | Journal Article | Telemonitoring System | 268 | Nurses, General Practitioners, and Pediatricians | Spain | Extended TAM |
| 21 | Khalika Banda and Gombachika [103] | 2012 | Conference | Mobile Health Services | 38 | Health Surveillance Assistants | Malawi | Extended TAM |
| 22 | Holden et al. [104] | 2012 | Journal Article | Bar-coded medication -dispensing and administration technology | 39 | Pharmacists and Pharmacy Technicians | USA | Extended TAM |
| 23 | Chang and Hsu [105] | 2012 | Journal Article | Online Patient-Safety Reporting System | 183 | Healthcare Professionals | Taiwan | Modified UTAUT |
| 24 | Ifinedo [106] | 2012 | Conference | Information Systems | 227 | Health Professionals | Canada | Modified UTAUT |
| 25 | Moores [107] | 2012 | Journal Article | Clinical Management System | 346 | Clinical Staff | France | Extended TAM—Integrated Model |
| 26 | Guo et al. [108] | 2012 | Conference | Mobile Health Services | 492 | Service Participants | Taiwan | Extended TAM |
| 27 | Sarlan et al. [109] | 2012 | Conference | Clinic Information System | 252 | Doctors and Staff | Malaysia | Integrated Model: TAM and TPB |
| 28 | Gagnon et al. [110] | 2012 | Journal Article | Home Telemonitoring System | 93 | Doctors and Nurses | Spain | Modified TAM |
| 29 | Chua et al. [111] | 2012 | Conference | Home-based Pill Dispensers | 21 | Patients | Singapore | TAM |
| 30 | Su, Tsai, and Chen [112] | 2012 | Conference | Telecare System | 365 | Older Resident | Taiwan | TAM |
| 31 | Chow et al. [113] | 2013 | Journal Article | Clinical Imaging Portal | 128 | Nursing Students | Hong Kong | Extended TAM |
| 32 | Cheng [114] | 2013 | Journal Article | E-Learning System | 218 | Nurses | Taiwan | Integrated Model: TAM and Flow Theory |
| 33 | Bennani and Oumlil [28] | 2013 | Conference | IT in Healthcare | 250 | Nurses | Morocco | Extended UTAUT |
| 34 | Vanneste, Vermeulen, and Declercq [115] | 2013 | Journal Article | BelRAI Web Application: Web-Based System Enabling Person-Centered Recording and Data Sharing | 282 | Healthcare Professionals | Belgium | Extended UTAUT |
| 35 | Huang [116] | 2013 | Journal Article | Telecare | 369 | Residents 15+ | Taiwan | Extended TAM |
| 36 | Escobar-Rodríguez and Romero-Alonso [117] | 2013 | Journal Article | Automated Unit-Based Medication Storage and Distribution Systems | 118 | Nurse | Spain | Extended TAM |
| 37 | Arning, Kowalewski, and Ziefle [118] | 2013 | Conference | Wireless Medical Technologies (WMT) | 305 | Users/Non-Users | Germany | Innovation Diffusion Theory |
| 38 | Sarlan, Ahmad, and Fatimah [119] | 2013 | Conference | Health Information System (HIS) | 252 | Staff in Private Healthcare Organizations | Malaysia | Integrated Model: TAM and TPB |
| 39 | Cocosila [120] | 2013 | Journal Article | Mobile Health Applications | 170 | Smokers (18+) | United Kingdom | Attitude-Perceived Risk-Motivation Model |
| 40 | Gajanayake, Sahama, and Iannella [58] | 2013 | Journal Article | Electronic Health Record (EHR) | 334 | Medical, Nursing, and Health Students | Australia | TAM |
| 41 | Chen et al. [121] | 2013 | Journal Article | E-Appointment System | 334 | Citizens | Taiwan | Extended TAM |
| 42 | Kummer, Schäfer, and Todorova [122] | 2013 | Journal Article | Sensor-Based Medication Systems | 579 | Nurses | Australia | Extended TAM2 |
| 43 | Kuo, Liu, and Ma [123] | 2013 | Journal Article | Mobile Electronic Medical Record (MEMR) | 665 | Nurses | Taiwan | Extended TAM |
| 44 | Krueklai, Kiattisin, and Leelasantitham [124] | 2013 | Journal Article | E-Health Solutions | 200 | Participants from Government Hospitals | Thailand | UTAUT |
| 45 | Manimaran and Lakshmi [125] | 2013 | Journal Article | Health Management Information System (HMIS) | 960 | Healthcare Professionals: Doctors, Pharmacists, Nurses, etc. | India | Extended TAM |
| 46 | Tavakoli et al. [126] | 2013 | Journal Article | Electronic Medical Record (EMR) | 62 | System Users | Iran | Extended TAM |
| 47 | Jackson, Yi, and Park [127] | 2013 | Journal Article | Personal Digital Assistant (PDA) | 222 | Physicians | USA | TAM, TPB, and IDT |
| 48 | Mohamed et al. [128] | 2013 | Conference | Electronic Health Technologies | 129 | Participants—Not Specified | UAE and UK | E-Health Technology Acceptance Model (E-HTAM2)—Extended TAM |
| 49 | Sarlan, Ahmad, and Ahmad [62] | 2013 | Journal Article | Clinic Information System (CIS) | 252 | Doctors and Staff | Malaysia | Extended Hybrid Model: TAM and TPB |
| 50 | Ford [129] | 2014 | Master’s Thesis | Over-the-Counter Blood Pressure Monitor | 26 | Individuals in 2 age groups: (18–28) and (60–85) | USA | Extended UTAUT |
| 51 | Alaiad, Zhou, and Koru [130] | 2014 | Journal Article | Home Healthcare Robots | 64 | Patients and Healthcare Professionals | USA | Extended UTAUT |
| 52 | Lin [131] | 2014 | Journal Article | Knowledge Management Systems | 361 | Physicians | USA and Taiwan | Technology Acceptance View of Knowledge Management Systems in Healthcare Organizations (TAV-KMSHO) |
| 53 | Hsieh, Lai, and Ye [132] | 2014 | Conference | Health Cloud Services | 443 | Patients | Taiwan | Integrated Model: TAM and SQB |
| 54 | Gagnon et al. [133] | 2014 | Journal Article | Electronic Health Record (EHR) | 150 | Physicians | Canada | 4 Models: TAM, Extended TAM, Psychosocial Model, and Integrated Model |
| 55 | Fleming et al. [134] | 2014 | Journal Article | Prescription Monitoring: Prescription Access | 76 | Emergency Physicians | USA | TAM |
| 56 | Corneille et al. [135] | 2014 | Conference | Text-Message-Based Health Intervention | 120 | Undergraduate Psychology Students | USA | Innovation Diffusion Theory |
| 57 | Steininger et al. [136] | 2014 | Conference | Electronic Health Record (EHR) | 204 | Physicians | Austria | Modified TAM |
| 58 | Hwang, Kim, and Lee [137] | 2014 | Journal Article | Ambulance Telemetry Technology | 136 | Emergency Medical Technicians | S. Korea | Extended TAM |
| 59 | Hung, Tsai, and Chuang [138] | 2014 | Journal Article | Primary Health Information System (PHIS) | 768 | Nurses | Taiwan | Theory of Reasoned Action (TRA) |
| 60 | Rho, Choi, and Lee [139] | 2014 | Journal Article | Telemedicine Technology | 183 | Physicians | S. Korea | Extended TAM |
| 61 | Moon and Chang [140] | 2014 | Journal Article | Innovative Smartphone | 122 | Hospital Professionals | S. Korea | Integrated Model: TRA, TAM, and IS Success Model |
| 62 | Tsai [141] | 2014 | Journal Article | Telehealth System | 365 | Patients | Taiwan | Integrated Model: Extended TAM and HBM |
| 63 | Yallah [142] | 2014 | PhD Dissertation | Telemedicine | 190 | Physicians | Georgia | Extended TAM |
| 64 | Cleveland [143] | 2014 | PhD Dissertation | Educational Technology | 57 | Nurse Educators | USA | Extended TAM |
| 65 | Devine [144] | 2015 | PhD Dissertation | Social Media in Healthcare | 137 | Nurses | USA | UTAUT2 |
| 66 | Ebie and Njoku [145] | 2015 | Journal Article | Performance Appraisal System | 80 | Line Managers | United Kingdom | Extended TAM |
| 67 | Krishnan, Dhillon, and Lutteroth [146] | 2015 | Conference | Consumer Health Informatics Applications | 105 | Health Consumers | Malaysia | Integrated Model: TAM, TRA, and UTAUT2 |
| 68 | Basak, Gumussoy, and Calisir [147] | 2015 | Journal Article | Personal Digital Assistant (PDA) | 339 | Physicians | Turkey | Extended TAM |
| 69 | Briz-Ponce and García-Peñalvo [148] | 2015 | Journal Article | Mobile Technology and “Apps” in Medical Education | 124 | Students and Medical Professionals | Spain | Extended TAM |
| 70 | Song, Park, and Oh [149] | 2015 | Journal Article | Bar Code Medication Administration Technology | 163 | Nurses | USA | Extended TAM |
| 71 | Holahan et al. [150] | 2015 | Journal Article | Medication Reconciliation Technology | 53 | Primary Care Providers | USA | Effective Technology Use Model (ETUM) |
| 72 | Ahadzadeh et al. [151] | 2015 | Journal Article | Health-Related Internet Use | 293 | Female Users | Malaysia | Integrated Model: HBM and TAM |
| 73 | Kowitlawakul et al. [152] | 2015 | Journal Article | Electronic Health Records for Nursing Education (EHRNE) | 212 | Undergraduate Nurses | Singapore | Extended TAM |
| 74 | Elaklouk, Mat Zin, and Shapii [153] | 2015 | Journal Article | Serious Games for Cognitive Rehabilitation | 41 | Therapists | Saudi Arabia | Extended TAM |
| 75 | Chang et al. [154] | 2015 | Journal Article | E-Hospital Service: Web-Based Appointment System | 140 | Patients | Taiwan | Extended TAM |
| 76 | Hsieh [155] | 2015 | Journal Article | Health Cloud Services | 209 | Healthcare Professionals | Taiwan | Integrated Model: TPB and SQB |
| 77 | Steininger and Stiglbauer [156] | 2015 | Journal Article | Electronic Health Records (EHR) | 204 | Physicians | Austria | Modified TAM |
| 78 | De Veer et al. [157] | 2015 | Journal Article | E-Health Applications | 1014 | Older People | Germany | UTAUT |
| 79 | Ku and Hsieh [158] | 2015 | Conference | Health Cloud Services | 105 | Patients | Taiwan | Integrated Model: TPB and SQB |
| 80 | Liu and Cheng [159] | 2015 | Journal Article | Mobile Electronic Medical Records | 158 | Physicians | Taiwan | Integrated Model: TAM and Dual-Factor Model |
| 81 | Miiro and Maiga [160] | 2015 | Book Chapter | Social Networks For E-Health | 278 | Graduate Students | Uganda | E-Health Social Networked Model |
| 82 | Zaman [161] | 2015 | Master’s Thesis | Electronic Documentation Systems (her, EMR, EPR) | 248 | Nurses | USA | Extended TAM |
| 83 | Sezgin and Özkan-Yıldırım [162] | 2016 | Journal Article | Health Information Technology: Pharmaceutical Service Systems | 1420 | Pharmacists/ Pharmaceutical Assistants | Turkey | Integrated Model (P-TAM): TAM, UTAUT, and TPB |
| 84 | Mansur, Fatma [163] | 2016 | Journal Article | Information and Communication Technologies | 303 | Health Managers | Turkey | Extended TAM |
| 85 | Moon and Hwang [164] | 2016 | Book Chapter | Smart Health Care System | 126 | Students | S. Korea | Extended UTAUT |
| 86 | Ku and Hsieh [165] | 2016 | Conference | Cloud-Based Healthcare Services | 178 | Elderly Citizens | Taiwan | Extended TPB |
| 87 | Made Dhanar et al. [166] | 2016 | Conference | Hospital Information Systems | 100 | Hospital Staff and Doctors | Indonesia | Integrated Model: TAM and DeLone and McLean IS Success |
| 88 | Kim, Seok, et al. [31] | 2016 | Journal Article | Mobile Electronic Medical Record (EMR) | 449 | Healthcare Professionals | S. Korea | Extended UTAUT |
| 89 | Cimperman, Makovec Brenčič, and Trkman [35] | 2016 | Journal Article | Home Telehealth Services (HTS) | 400 | Old Users 50+ | Slovenia | Extended UTAUT |
| 90 | Hadadgar et al. [39] | 2016 | Journal Article | E-Learning Continuing Medical Education (CME) | 146 | General Practitioners | Iran | TPB |
| 91 | Hsiao and Chen [167] | 2016 | Journal Article | Computerized Clinical Practice Guidelines | 238 | Physicians | Taiwan | Integrative Model of Activity Theory and TAM |
| 92 | Lazard et al. [168] | 2016 | Journal Article | Patient Portal | 333 | Portal Users | USA | Extended TAM |
| 93 | Lin et al. [169] | 2016 | Journal Article | Wearable Instrumented Vest | 50 | Elderly 60+ | Taiwan | Extended TAM |
| 94 | Al-Nassar, Rababah, and Al-Nsour [170] | 2016 | Journal Article | Computerized Physician Order Entry (CPOE) | 118 | Physicians | Jordan | Extended TAM |
| 95 | Lazuras and Dokou [171] | 2016 | Journal Article | Online Counseling Services | 63 | Mental Health Professionals | United Kingdom | Extended TAM |
| 96 | Ifinedo Princely, Odette Griscti, and Judy Bailey [172] | 2016 | Journal Article | Healthcare Information Systems (HIS) | 197 | Registered Nurses | Canada | Extended TAM |
| 97 | Holden et al. [173] | 2016 | Journal Article | In-Room Pediatric ICU Technology | 167 | Nurses | USA | Expanded TAM |
| 98 | Ducey and Coovert [174] | 2016 | Journal Article | Tablet Computer Use | 261 | Physicians | USA | Extended TAM |
| 99 | Chen, Chang, and Lai [175] | 2016 | Conference | Cloud Sphygmomanometer | 521 | System Users | Taiwan | Extended TAM |
| 100 | Guo, Zhang, and Sun [176] | 2016 | Journal Article | Mobile Health Services | 650 | Service Users | China | Attribute-Perception-Intention Model |
| 101 | Becker [177] | 2016 | Journal Article | Mobile Mental Health Applications | 125 | Young Adults | Germany | Extended TAM |
| 102 | Shujen Lee and Chen [178] | 2016 | Conference | 3D Bio-Printing | 249 | Adults | Taiwan | TAM |
| 103 | Hsieh [179] | 2016 | Journal Article | Health Cloud Services | 681 | Patients | Taiwan | Dual-Factor Model: UTAUT and SQB |
| 104 | Ahmadi et al. [9] | 2017 | Journal Article | Picture Archiving and Communication System (PACS) | 151 | Healthcare Employees | Iran | UTAUT |
| 105 | Jayusman and Setyohadi [180] | 2017 | Conference | E-Learning System | 188 | Students at School of Health Sciences | Indonesia | Extended TAM |
| 106 | Amin et al. [181] | 2017 | Journal Article | Cloud-Based Healthcare Services | 147 | Healthcare Professionals | Malaysia, Pakistan, and Saudi Arabia | UTAUT |
| 107 | [182] | 2017 | Journal Article | Barcode Technology | 9 | Users | Iran | Extended TAM |
| 108 | Ehteshami [183] | 2017 | Journal Article | Electronic Health Record (EHR) | 233 | Physicians | Armenia | Tripolar Model (TMTA)—Extended TAM |
| 109 | Rajanen and Weng [184] | 2017 | Conference | Wearable Devices for Personal Healthcare—Smart Bands | 158 | Consumers | China | Extended TAM |
| 110 | Wahyuni and Nurbojatmiko [185] | 2017 | Conference | E-Health Services Consumer Informatics | 91 | Citizens | Indonesia | Extended Model: TAM and HBM |
| 111 | Nematollahi et al. [186] | 2017 | Journal Article | Electronic Medical Records (EMR) | 235 | Hospital Managers | Iran | UTAUT |
| 112 | Hsu and Wu [59] | 2017 | Journal Article | Nursing Information Systems | 158 | Nurses | Taiwan | TAM |
| 113 | Horne [187] | 2017 | PhD Dissertation | Telemedicine | 46 | Healthcare Workers | USA | TAM |
| 114 | Hsieh et al. [188] | 2017 | Book Chapter | Personal Health Information System in Self-Health Management | 240 | Middle-Aged and Elderly Citizens | Taiwan | HBM |
| 115 | Lin [189] | 2017 | Journal Article | Nursing Information System | 531 | Nurses | Taiwan | Integrated Model: TAM and ISSM |
| 116 | Dou et al. [190] | 2017 | Journal Article | Smartphone Health Technology for Chronic Disease Management | 157 | Patients | China | Extended TAM |
| 117 | Zhang et al. [191] | 2017 | Journal Article | Mobile Health Services | 650 | Service Users | China | Extended TAM |
| 118 | Khan et al. [78] | 2018 | Journal Article | E-Prescribing | 295 | Physicians | Pakistan | Extended UTAUT |
| 119 | Kalavani, Kazerani, and Shekofteh [65] | 2018 | Journal Article | Evidence-Based Medicine (EBM) Databases | 192 | Medical Residents | Iran | UTAUT |
| 120 | Lin et al. [60] | 2018 | Journal Article | Wearable Cardiac Health Technologies | 48 | Patients | Taiwan | Extended TAM |
| 121 | Martins et al. [192] | 2018 | Journal Article | E-Health Technology | 210 | Hospital Employees | Nigeria | Extended UTAUT |
| 122 | Beldad and Hegner [67] | 2018 | Journal Article | Fitness Apps | 476 | Users of Fitness Apps | Germany | Extended TAM |
| 123 | Perlich, Meinel, and Zeis [29] | 2018 | Journal Article | Interactive Documentation System | 46 | Therapists and Patients | Germany | Extended UTAUT |
| 124 | Nadri et al. [69] | 2018 | Journal Article | Hospital Information Systems | 202 | Systems Users | Iran | Extended TAM |
| 125 | Tubaishat [38] | 2018 | Journal Article | Electronic Health Records (EHR) | 1539 | Nurse | Jordan | TAM |
| 126 | Özdemir-Güngör and Camgöz-Akdağ [61] | 2018 | Journal Article | Electronic Health Records (EHR) | 99 | Healthcare Professionals and Administrative Staff | Turkey | Modified TAM |
| 127 | Aldosari et al. [193] | 2018 | Journal Article | Electronic Medical Records (EMR) | 153 | Nurses | Saudi Arabia | Modified TAM |
| 128 | Ku and Hsieh [194] | 2018 | Conference | Health Management Mobile Services | 105 | Citizens | Taiwan | Integrated Model: TPB and HBM |
| 129 | Hennemann et al. [195] | 2018 | Journal Article | Occupational E-Mental-Health | 1829 | Employees with Long Sick Leaves | Germany | Extended UTAUT |
| 130 | Vitari and Ologeanu-Taddei [196] | 2018 | Journal Article | Electronic Health Records (EHR) | 1741 + 1119 | Physicians, Paraprofessionals, and Administrative Personnel | France | New Developed Model |
| 131 | Venugopal et al. [10] | 2018 | Conference | Telemedicine and Electronic Health Records (EHR) | 568 | Clinical Staff | India | UTAUT |
| 132 | Liu and Lee [68] | 2018 | Journal Article | Pharma-Cloud | 179 | Pharmacists | Taiwan | Extended TAM |
| 133 | Zhou et al. [197] | 2019 | Journal Article | Telehealth | 436 | 60+ Years Old Patients | China | Extended TAM |
| 134 | Francis [198] | 2019 | Journal Article | Self-Monitoring Devices | 258 | Healthcare Providers | USA | Expanded UTAUT2 |
| 135 | Li et al. [63] | 2019 | Journal Article | Smart Wearables | 146 | 60+ Years Old Adults | China | Extended Hybrid Model: TAM and UTAUT |
| 136 | Tao et al. [199] | 2019 | Journal Article | Health Information Portal | 201 | Adults | China | Extended TAM Model |
| 137 | Masyarakat et al. [200] | 2019 | Journal Article | Nutrition Information System | 50 | Nutrition Officers | Indonesia | UTAUT |
| 138 | Tsai et al. [64] | 2019 | Journal Article | Telehealth | 281 | Adults 40+ | Taiwan | Integrated Model: TAM and SQB |
| 139 | Turja et al. [80] | 2019 | Journal Article | Care Robots | 544 | Healthcare Professionals | Finland | Robot Acceptance Model for Care (RAM-care) |
| 140 | Idoga et al. [66] | 2019 | Journal Article | Cloud-Based Health Center (CBHC) | 300 | Healthcare Professionals | Nigeria | UTAUT2 |
| 141 | Boon-itt [8] | 2019 | Journal Article | Health Websites | 222 | Internet Consumers | Thailand | Extended TAM |
| 142 | Schomakers, Lidynia, and Ziefle [201] | 2019 | Conference | E-Health Technologies: Fitness Trackers and Remote Monitoring of Implanted Cardiac Devices | 253 | Patients with Chronic Health Conditions | Germany | Acceptance Model of E-Health Technologies |
References
- Taherdoost, H. A review of technology acceptance and adoption models and theories. Procedia Manuf. 2018, 22, 960–967. [Google Scholar] [CrossRef]
- Taherdoost, H. Importance of Technology Acceptance Assessment for Successful Implementation and Development of New Technologies. Glob. J. Eng. Sci. 2019, 1. [Google Scholar] [CrossRef] [Green Version]
- Chau, P.Y.K.; Hu, P.J.-H. Investigating healthcare professionals’ decisions to accept telemedicine technology: An empirical test of competing theories. Inf. Manag. 2002, 39, 297–311. [Google Scholar] [CrossRef]
- Al-Qaysi, N.; Mohamad-Nordin, N.; Al-Emran, M. Developing a comprehensive theoretical model for adopting social media in higher education. Interact. Learn. Environ. 2021, 1–22. [Google Scholar] [CrossRef]
- Al-Emran, M.; Arpaci, I. Intelligent Systems and Novel Coronavirus (COVID-19): A Bibliometric Analysis. In Emerging Technologies During the Era of COVID-19 Pandemic; Springer: Berlin/Heidelberg, Germany, 2021; pp. 59–67. [Google Scholar]
- Rahimi, B.; Nadri, H.; Lotfnezhad Afshar, H.; Timpka, T. A Systematic Review of the Technology Acceptance Model in Health Informatics. Appl. Clin. Inform. 2018, 9, 604–634. [Google Scholar] [CrossRef] [Green Version]
- Ketikidis, P.; Dimitrovski, T.; Lazuras, L.; Bath, P.A. Acceptance of health information technology in health professionals: An application of the revised technology acceptance model. Health Inform. J. 2012, 18, 124–134. [Google Scholar] [CrossRef] [Green Version]
- Boon-itt, S. Quality of health websites and their influence on perceived usefulness, trust and intention to use: An analysis from Thailand. J. Innov. Entrep. 2019, 8, 4. [Google Scholar] [CrossRef]
- Ahmadi, M.; Mehrabi, N.; Sheikhtaheri, A.; Sadeghi, M. Acceptability of picture archiving and communication system (PACS) among hospital healthcare personnel based on a unified theory of acceptance and use of technology. Electron. Physician 2017, 9, 5325–5330. [Google Scholar] [CrossRef] [Green Version]
- Venugopal, P.; Priya, S.A.; Manupati, V.K.; Varela, M.L.R.; Machado, J.; Putnik, G.D. Impact of UTAUT Predictors on the Intention and Usage of Electronic Health Records and Telemedicine from the Perspective of Clinical Staffs. In Proceedings of the International Conference on Innovation, Engineering and Entrepreneurship, Guimarães, Portugal, 27–29 June 2018; Springer: Berlin/Heidelberg, Germany, 2018; Volume 505, pp. 172–177. [Google Scholar]
- Al-Maroof, R.; Al-Qaysi, N.; Salloum, S.A.; Al-Emran, M. Blended Learning Acceptance: A Systematic Review of Information Systems Models. Technol. Knowl. Learn. 2021, 1–36. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley Pub. Co.: Reading, MA, USA, 1975. [Google Scholar]
- Davis, F.D. A Technology Acceptance Model for Empirically Testing New End-User Information Systems; Theory and Results; Massachusetts Institute of Technology: Cambridge, MA, USA, 1986. [Google Scholar]
- Davis, F. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Bala, H. Technology acceptance model 3 and a research agenda on interventions. Decis. Sci. 2008, 39, 273–315. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Morris, M.; Davis, G.; Davis, F. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Triandis, H. Interpersonal Behavior; Brooks/Cole Pub. Co.: Monterey, CA, USA, 1977; ISBN 081850188X 9780818501883. [Google Scholar]
- Moore, G.C.; Benbasat, I. Development of an Instrument to Measure the Perceptions of Adopting an Information Technology Innovation. Inf. Syst. Res. 1991, 2, 192–222. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. From Intentions to Actions: A Theory of Planned Behavior. In Action Control; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. ISBN 978-3-642-69746-3. [Google Scholar]
- Thompson, R.L.; Higgins, C.A.; Howell, J.M. Personal Computing: Toward a Conceptual Model of Utilization. MIS Q. 1991, 15, 125–143. [Google Scholar] [CrossRef]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. Extrinsic and intrinsic motivation to use computers in the workplace. J. Appl. Soc. Psychol. 1992, 22, 1111–1132. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations, 4th ed.; Simon and Schuster (Free Press): New York, NY, USA, 1995; ISBN 1451602472. [Google Scholar]
- Igbaria, M.; Schiffman, S.J.; Wieckowski, T.J. The respective roles of perceived usefulness and perceived fun in the acceptance of microcomputer technology. Behav. Inf. Technol. 1994, 13, 349–361. [Google Scholar] [CrossRef]
- Bennani, A.E.; Oumlil, R. Factors fostering IT acceptance by nurses in Morocco: Short paper. In Proceedings of the Proceedings—International Conference on Research Challenges in Information Science, Paris, France, 29–31 May 2013. [Google Scholar]
- Perlich, A.; Meinel, C.; Zeis, D. Evaluation of the technology acceptance of a collaborative documentation system for addiction therapists and clients. Stud. Health Technol. Inform. 2018, 247, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Holden, R.J.; Karsh, B.-T. The Technology Acceptance Model: Its past and its future in health care. J. Biomed. Inform. 2010, 43, 159–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Lee, K.-H.; Hwang, H.; Yoo, S. Analysis of the factors influencing healthcare professionals’ adoption of mobile electronic medical record (EMR) using the unified theory of acceptance and use of technology (UTAUT) in a tertiary hospital. BMC Med. Inform. Decis. Mak. 2016, 16, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Emran, M.; Granić, A. Is It Still Valid or Outdated? A Bibliometric Analysis of the Technology Acceptance Model and Its Applications From 2010 to 2020. In Recent Advances in Technology Acceptance Models and Theories; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [Green Version]
- Vaezipour, A.; Whelan, B.M.; Wall, K.; Theodoros, D. Acceptance of Rehabilitation Technology in Adults with Moderate to Severe Traumatic Brain Injury, Their Caregivers, and Healthcare Professionals: A Systematic Review. J. Head Trauma Rehabil. 2019, 34, E67–E82. [Google Scholar] [CrossRef]
- Cimperman, M.; Makovec Brenčič, M.; Trkman, P. Analyzing older users’ home telehealth services acceptance behavior-applying an Extended UTAUT model. Int. J. Med. Inform. 2016, 90, 22–31. [Google Scholar] [CrossRef] [Green Version]
- Goodarzian, F.; Abraham, A.; Ghasemi, P.; Mascolo, M.D.; Nasseri, H. Designing a green home healthcare network using grey flexible linear programming: Heuristic approaches. J. Comput. Des. Eng. 2021, 8, 1468–1498. [Google Scholar] [CrossRef]
- Goodarzian, F.; Abraham, A.; Fathollahi-Fard, A.M. A biobjective home health care logistics considering the working time and route balancing: A self-adaptive social engineering optimizer. J. Comput. Des. Eng. 2021, 8, 452–474. [Google Scholar] [CrossRef]
- Tubaishat, A. Perceived usefulness and perceived ease of use of electronic health records among nurses: Application of Technology Acceptance Model. Inform. Health Soc. Care 2018, 43, 379–389. [Google Scholar] [CrossRef]
- Hadadgar, A.; Changiz, T.; Masiello, I.; Dehghani, Z.; Mirshahzadeh, N.; Zary, N. Applicability of the theory of planned behavior in explaining the general practitioners eLearning use in continuing medical education. BMC Med. Educ. 2016, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGinn, C.A.; Grenier, S.; Duplantie, J.; Shaw, N.; Sicotte, C.; Mathieu, L.; Leduc, Y.; Légaré, F.; Gagnon, M.-P. Comparison of user groups’ perspectives of barriers and facilitators to implementing electronic health records: A systematic review. BMC Med. 2011, 9, 46. [Google Scholar] [CrossRef] [Green Version]
- Gagnon, M.-P.; Desmartis, M.; Labrecque, M.; Car, J.; Pagliari, C.; Pluye, P.; Frémont, P.; Gagnon, J.; Tremblay, N.; Légaré, F. Systematic Review of Factors Influencing the Adoption of Information and Communication Technologies by Healthcare Professionals. J. Med. Syst. 2012, 36, 241–277. [Google Scholar] [CrossRef] [Green Version]
- Mair, F.S.; May, C.; O’Donnell, C.; Finch, T.; Sullivan, F.; Murray, E. Factors that promote or inhibit the implementation of e-health systems: An explanatory systematic review. Bull. World Health Organ. 2012, 90, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Yucel, A.; Gulbahar, U.; Yasemin, Y. Technology Acceptance Model: A Review of the Prior Predictors. Ankara Univ. Egit. Bilim. Fak. Derg. 2013, 46, 89–109. [Google Scholar] [CrossRef] [Green Version]
- Gagnon, M.-P.; Ngangue, P.; Payne-Gagnon, J.; Desmartis, M. m-Health adoption by healthcare professionals: A systematic review. J. Am. Med. Inform. Assoc. 2016, 23, 212–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusif, S.; Soar, J.; Hafeez-Baig, A. Older people, assistive technologies, and the barriers to adoption: A systematic review. Int. J. Med. Inform. 2016, 94, 112–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Saedi, K.; Al-Emran, M. A Systematic Review of Mobile Payment Studies from the Lens of the UTAUT Model. In Recent Advances in Technology Acceptance Models and Theories; Springer: Cham, Switzerland, 2021; Volume 335, pp. 79–106. [Google Scholar]
- Marangunić, N.; Granić, A. Technology acceptance model: A literature review from 1986 to 2013. Univers. Access Inf. Soc. 2015, 14, 81–95. [Google Scholar] [CrossRef]
- Fatehah, M.; Mezhuyev, V.; Al-Emran, M. A Systematic Review of Metamodelling in Software Engineering. In Recent Advances in Intelligent Systems and Smart Applications; Springer: Berlin/Heidelberg, Germany, 2021; pp. 3–27. [Google Scholar]
- Kitchenham, B.; Charters, S. Guidelines for performing systematic literature reviews in software engineering. Softw. Eng. Group Sch. Comput. Sci. Math. Keele Univ. 2007, 1–57. Available online: http://citeseerx.ist.psu.edu/viewdoc/summary?doi=10.1.1.117.471 (accessed on 2 November 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Al-Nuaimi, M.N.; Al-Emran, M. Learning management systems and technology acceptance models: A systematic review. Educ. Inf. Technol. 2021, 1–35. [Google Scholar] [CrossRef]
- Mendeley Ltd. Mendeley. Available online: https://www.mendeley.com/ (accessed on 14 March 2020).
- Al-Emran, M.; Mezhuyev, V.; Kamaludin, A. Technology Acceptance Model in M-learning context: A systematic review. Comput. Educ. 2018, 125, 389–412. [Google Scholar] [CrossRef]
- Al-Emran, M.; Mezhuyev, V.; Kamaludin, A.; Shaalan, K. The impact of knowledge management processes on information systems: A systematic review. Int. J. Inf. Manag. 2018, 43, 173–187. [Google Scholar] [CrossRef]
- Al-Qaysi, N.; Mohamad-Nordin, N.; Al-Emran, M. Employing the technology acceptance model in social media: A systematic review. Educ. Inf. Technol. 2020, 1–42. [Google Scholar] [CrossRef]
- AlQudah, A.A.; Salloum, S.A.; Shaalan, K. The Role of Technology Acceptance in Healthcare to Mitigate COVID-19 Outbreak. In Studies in Systems, Decision and Control; Springer: Berlin/Heidelberg, Germany, 2021; Volume 348, pp. 223–244. [Google Scholar]
- Gajanayake, R.; Sahama, T.; Iannella, R. The role of perceived usefulness and attitude on electronic health record acceptance. Int. J. E-Health Med. Commun. 2013, 5, 108–119. [Google Scholar] [CrossRef]
- Hsu, H.H.; Wu, Y.H. Investigation of the effects of a nursing information system by using the technology acceptance model. CIN—Comput. Inform. Nurs. 2017, 35, 315–322. [Google Scholar] [CrossRef]
- Lin, W.-Y.; Ke, H.-L.; Chou, W.-C.; Chang, P.-C.; Tsai, T.-H.; Lee, M.-Y. Realization and Technology Acceptance Test of a Wearable Cardiac Health Monitoring and Early Warning System with Multi-Channel MCGs and ECG. Sensors 2018, 18, 3538. [Google Scholar] [CrossRef] [Green Version]
- Özdemir-Güngör, D.; Camgöz-Akdağ, H. Examining the effects of technology anxiety and resistance to change on the acceptance of breast tumor registry system: Evidence from Turkey. Technol. Soc. 2018, 54, 66–73. [Google Scholar] [CrossRef]
- Sarlan, A.; Ahmad, R.; Ahmad, W.F.W.; Dominic, D.D. A study of SME private healthcare personnel acceptance of Clinic Information System in Malaysia. Int. J. Bus. Inf. Syst. 2013, 14, 238. [Google Scholar] [CrossRef]
- Li, J.; Ma, Q.; Chan, A.H.; Man, S.S. Health monitoring through wearable technologies for older adults: Smart wearables acceptance model. Appl. Ergon. 2019, 75, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Tsai, J.M.; Cheng, M.J.; Tsai, H.H.; Hung, S.W.; Chen, Y.L. Acceptance and resistance of telehealth: The perspective of dual-factor concepts in technology adoption. Int. J. Inf. Manag. 2019, 49, 34–44. [Google Scholar] [CrossRef]
- Kalavani, A.; Kazerani, M.; Shekofteh, M. Acceptance of evidence based medicine (EBM) databases by Iranian medical residents using unified theory of acceptance and use of technology (UTAUT). Health Policy Technol. 2018, 7, 287–292. [Google Scholar] [CrossRef]
- Idoga, P.E.; Toycan, M.; Nadiri, H.; Çelebi, E. Assessing factors militating against the acceptance and successful implementation of a cloud based health center from the healthcare professionals’ perspective: A survey of hospitals in Benue state, northcentral Nigeria. BMC Med. Inform. Decis. Mak. 2019, 19, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beldad, A.D.; Hegner, S.M. Expanding the Technology Acceptance Model with the Inclusion of Trust, Social Influence, and Health Valuation to Determine the Predictors of German Users’ Willingness to Continue using a Fitness App: A Structural Equation Modeling Approach. Int. J. Hum.-Comput. Interact. 2018, 34, 882–893. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.C.; Lee, C.C. An Investigation of Pharmacists’ Acceptance of NHI-PharmaCloud in Taiwan. J. Med. Syst. 2018, 42, 213. [Google Scholar] [CrossRef] [PubMed]
- Nadri, H.; Rahimi, B.; Afshar, H.L.; Samadbeik, M.; Garavand, A. Factors affecting acceptance of hospital information systems based on extended technology acceptance model: A case study in three paraclinical departments. Appl. Clin. Inform. 2018, 9, 238–247. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, R.; Prasad, J. A Conceptual and Operational Definition of Personal Innovativeness in the Domain of Information Technology. Inf. Syst. Res. 1998, 9, 204–215. [Google Scholar] [CrossRef]
- Gefen, D.; Karahanna, E.; Straub, D.W. Trust and TAM in Online Shopping: An Integrated Model. MIS Q. 2003, 27, 51. [Google Scholar] [CrossRef]
- Al-Qaysi, N.; Mohamad-Nordin, N.; Al-Emran, M. Factors Affecting the Adoption of Social Media in Higher Education: A Systematic Review of the Technology Acceptance Model. In Recent Advances in Intelligent Systems and Smart Applications; Springer: Berlin/Heidelberg, Germany, 2021; pp. 571–584. [Google Scholar]
- Medical Subject Headings—Home Page. Available online: http://www.nlm.nih.gov/mesh/ (accessed on 16 January 2021).
- Al-Saedi, K.; Al-Emran, M.; Abusham, E.; El-Rahman, S.A. Mobile Payment Adoption: A Systematic Review of the UTAUT Model. In Proceedings of the 2019 International Conference on Fourth Industrial Revolution, ICFIR 2019, Manama, Bahrain, 19–21 February 2019. [Google Scholar]
- King, W.R.; He, J. A meta-analysis of the technology acceptance model. Inf. Manag. 2006, 43, 740–755. [Google Scholar] [CrossRef]
- Legris, P.; Ingham, J.; Collerette, P. Why do people use information technology? A critical review of the technology acceptance model. Inf. Manag. 2003, 40, 191–204. [Google Scholar] [CrossRef]
- Alsharida, R.A.; Hammood, M.M.; Al-Emran, M. Mobile Learning Adoption: A Systematic Review of the Technology Acceptance Model from 2017 to 2020. Int. J. Emerg. Technol. Learn. 2021, 15. [Google Scholar] [CrossRef]
- Khan, I.U.; Yu, Y.; Hameed, Z.; Khan, S.U.; Waheed, A. Assessing the Physicians’ Acceptance of E-Prescribing in a Developing Country: An Extension of the UTAUT Model With Moderating Effect of Perceived Organizational Support. J. Glob. Inf. Manag. 2018, 26, 121–142. [Google Scholar] [CrossRef]
- Schaper, L.K.; Pervan, G.P. ICT and OTs: A model of information and communication technology acceptance and utilisation by occupational therapists. Int. J. Med. Inform. 2007, 76, S212–S221. [Google Scholar] [CrossRef] [PubMed]
- Turja, T.; Aaltonen, I.; Taipale, S.; Oksanen, A. Robot acceptance model for care (RAM-care): A principled approach to the intention to use care robots. Inf. Manag. 2019, 103220. [Google Scholar] [CrossRef]
- Wu, T.-Y.; Majeed, A.; Kuo, K.N. An overview of the healthcare system in Taiwan. Lond. J. Prim. Care 2010, 3, 115–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodarzian, F.; Ghasemi, P.; Gunasekaren, A.; Taleizadeh, A.A.; Abraham, A. A sustainable-resilience healthcare network for handling COVID-19 pandemic. Ann. Oper. Res. 2021, 1–65. [Google Scholar] [CrossRef]
- Arpaci, I.; Alshehabi, S.; Al-Emran, M.; Khasawneh, M.; Mahariq, I.; Abdeljawad, T.; Hassanien, A.E. Analysis of Twitter Data Using Evolutionary Clustering during the COVID-19 Pandemic. Comput. Mater. Contin. 2020, 65, 193–203. [Google Scholar] [CrossRef]
- Bennani, A.E.; Oumlil, R. Do constructs of technology acceptance model predict the ICT appropriation by physicians and nurses in healthcare public centres in Agadir, South of Morocco? In Proceedings of the HEALTHINF 2010—3rd International Conference on Health Informatics, Valencia, Spain, 20–23 January 2010; pp. 241–249. [Google Scholar]
- Lai, D.W.; Li, Y.P. Examining the technology acceptance model of the computer assistance orthopedic surgery system. In Proceedings of the 2010 7th International Conference on Service Systems and Service Management (ICSSSM’ 10), Tokyo, Japan, 28–30 June 2010; pp. 940–945. [Google Scholar]
- Kim, J.; DelliFraine, J.L.; Dansky, K.H.; McCleary, K.J. Physicians’ acceptance of telemedicine technology: An empirical test of competing theories. Int. J. Inf. Syst. Chang. Manag. 2010, 4, 210–225. [Google Scholar] [CrossRef]
- Holtz, B.E. An Examination of the Adoption of Electronic Medical Records by Rural Hospital Nurses through the Unified Theory of Acceptance and Use of Technology Lens; Michigan State University: East Lansing, MI, USA, 2010; Volume 72. [Google Scholar]
- Pai, F.Y.; Huang, K.I. Applying the Technology Acceptance Model to the introduction of healthcare information systems. Technol. Forecast. Soc. Chang. 2011, 78, 650–660. [Google Scholar] [CrossRef]
- Orruño, E.; Gagnon, M.P.; Asua, J.; Abdeljelil, A. Ben Evaluation of teledermatology adoption by health-care professionals using a modified Technology Acceptance Model. J. Telemed. Telecare 2011, 17, 303–307. [Google Scholar] [CrossRef]
- Maarop, N.; Win, K.T.; Masrom, M.; Hazara Singh, S.S. Exploring teleconsultation acceptance: A comparison study between emergency and non-emergency setting. In Proceedings of the 2011 International Conference on Research and Innovation in Information Systems (ICRIIS’11, IEEE), Kuala Lumpur, Malaysia, 23–24 November 2011; pp. 1–5. [Google Scholar]
- Schnall, R.; Bakken, S. Testing the Technology Acceptance Model: HIV case managers’ intention to use a continuity of care record with context-specific links. Inform. Health Soc. Care 2011, 36, 161–172. [Google Scholar] [CrossRef] [Green Version]
- Kowitlawakul, Y. The technology acceptance model: Predicting nurses’ intention to use telemedicine technology (eICU). CIN—Comput. Inform. Nurs. 2011, 29, 411–418. [Google Scholar] [CrossRef]
- Damanhoori, F.; Zakaria, N.; Hooi, L.Y.; Sultan, N.A.H.; Talib, N.A.; Ramadass, S. Understanding users’ Technology Acceptance on Breast Self Examination teleconsultation. In Proceedings of the 8th International Conference on High-capacity Optical Networks and Emerging Technologies (IEEE), Riyadh, Saudi Arabia, 19–21 December 2011; pp. 374–380. [Google Scholar]
- Lim, S.; Xue, L.; Yen, C.C.; Chang, L.; Chan, H.C.; Tai, B.C.; Duh, H.B.L.; Choolani, M. A study on Singaporean women’s acceptance of using mobile phones to seek health information. Int. J. Med. Inform. 2011, 80, e189–e202. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.H.H.M.; Tawfik, H.; Norton, L.; Al-Jumeily, D. e-HTAM: A Technology Acceptance Model for electronic health. In Proceedings of the 2011 International Conference on Innovations in Information Technology, Abu Dhabi, United Arab Emirates, 25–27 April 2011; pp. 134–138. [Google Scholar]
- Ortega Egea, J.M.; Román González, M.V. Explaining physicians’ acceptance of EHCR systems: An extension of TAM with trust and risk factors. Comput. Hum. Behav. 2011, 27, 319–332. [Google Scholar] [CrossRef]
- Mohamed, A.H.H.M.; Tawfik, H.; Al-Jumeily, D.; Norton, L. MoHTAM: A Technology Acceptance Model for Mobile Health Applications. In Proceedings of the 2011 Developments in E-systems Engineering (IEEE), Dubai, United Arab Emirates, 6–8 December 2011; pp. 13–18. [Google Scholar]
- Chong, A.Y.-L.; Chan, F.T.S. Understanding the Acceptance of RFID in the Healthcare Industry: Extending the TAM Model. In Decision-Making for Supply Chain Integration; Springer: Berlin/Heidelberg, Germany, 2012; pp. 105–122. [Google Scholar]
- Kim, J.; Park, H.A. Development of a health information technology acceptance model using consumers’ health behavior intention. J. Med. Internet Res. 2012, 14, e133. [Google Scholar] [CrossRef] [PubMed]
- Terrizzi, S.; Sherer, S.; Meyerhoefer, C.; Sheinberg, M.; Levick, D. Extending the technology acceptance model in healthcare: Identifying the role of trust and shared information. In Proceedings of the 18th Americas Conference on Information Systems 2012 (AMCIS 2012), Seattle, WA, USA, 9–11 August 2012; Volume 6, pp. 4518–4527. [Google Scholar]
- Chow, M.; Herold, D.K.; Choo, T.-M.; Chan, K. Extending the technology acceptance model to explore the intention to use Second Life for enhancing healthcare education. Comput. Educ. 2012, 59, 1136–1144. [Google Scholar] [CrossRef]
- Asua, J.; Orruño, E.; Reviriego, E.; Gagnon, M.P. Healthcare professional acceptance of telemonitoring for chronic care patients in primary care. BMC Med. Inform. Decis. Mak. 2012, 12, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalika Banda, C.; Gombachika, H. Mobile phone technology acceptance and usability in the delivery of health services among health surveillance assistants in rural areas of Malawi. In International Conference on e-Infrastructure and e-Services for Developing Countries (AFRICOMM 2012); Springer: Berlin/Heidelberg, Germany, 2013; Volume 119, pp. 249–258. [Google Scholar]
- Holden, R.J.; Brown, R.L.; Scanlon, M.C.; Karsh, B.T. Pharmacy workers’ perceptions and acceptance of bar-coded medication technology in a pediatric hospital. Res. Soc. Adm. Pharm. 2012, 8, 509–522. [Google Scholar] [CrossRef] [Green Version]
- Chang, I.C.; Hsu, H.M. Predicting medical staff intention to use an online reporting system with modified unified theory of acceptance and use of technology. Telemed. e-Health 2012, 18, 67–73. [Google Scholar] [CrossRef]
- Ifinedo, P. Technology acceptance by health professionals in Canada: An analysis with a modified UTAUT model. In Proceedings of the 45th Hawaii International Conference on System Sciences, Maui, HI, USA, 4–7 January 2012; pp. 2937–2946. [Google Scholar]
- Moores, T.T. Towards an integrated model of IT acceptance in healthcare. Decis. Support Syst. 2012, 53, 507–516. [Google Scholar] [CrossRef]
- Guo, X.; Yuan, J.; Cao, X.; Chen, X. Understanding the acceptance of mobile health services: A service participants analysis. In Proceedings of the 2012 International Conference on Management Science & Engineering 19th Annual Conference Proceedings, Dallas, TX, USA, 20–22 September 2012; pp. 1868–1873. [Google Scholar]
- Sarlan, A.; Ahmad, R.; Wan Ahmad, W.F.; Dominic, P.D.D. Users’ behavioral intention to use clinic information system: A survey. In Proceedings of the 2012 International Conference on Computer and Information Science, ICCIS 2012—A Conference of World Engineering, Science and Technology Congress, ESTCON 2012—Conference Proceedings, Kuala Lumpur, Malaysia, 12–14 June 2012; Volume 1, pp. 37–43. [Google Scholar]
- Gagnon, M.P.; Orruño, E.; Asua, J.; Abdeljelil, A.B.; Emparanza, J. Using a modified technology acceptance model to evaluate healthcare professionals’ adoption of a new telemonitoring system. Telemed. e-Health 2012, 18, 54–59. [Google Scholar] [CrossRef] [Green Version]
- Chua, J.C.; Foo, M.H.; Cheong, Y.L.; Ng, J.; Toh, C.K. Using paper prototyping to assess the perceived acceptance of MedMate: A home-based pill dispenser. In Proceedings of the 2012 Southeast Asian Network of Ergonomics Societies Conference: Ergonomics Innovations Leveraging User Experience and Sustainability (SEANES 2012), Langkawi, Malaysia, 9–12 July 2012. [Google Scholar]
- Su, S.P.; Tsai, C.H.; Chen, Y.K. Applying the technology acceptance model to explore intention to use telecare system in Taiwan. In Proceedings of the Proceedings—13th ACIS International Conference on Software Engineering, Artificial Intelligence, Networking, and Parallel/Distributed Computing (SNPD 2012), Kyoto, Japan, 8–10 August 2012; pp. 353–356. [Google Scholar]
- Chow, M.; Chan, L.; Lo, B.; Chu, W.P.; Chan, T.; Lai, Y.M. Exploring the intention to use a clinical imaging portal for enhancing healthcare education. Nurse Educ. Today 2013, 33, 655–662. [Google Scholar] [CrossRef]
- Cheng, Y.M. Exploring the roles of interaction and flow in explaining nurses’ e-learning acceptance. Nurse Educ. Today 2013, 33, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Vanneste, D.; Vermeulen, B.; Declercq, A. Healthcare professionals’ acceptance of BelRAI, a web-based system enabling person-centred recording and data sharing across care settings with interRAI instruments: A UTAUT analysis. BMC Med. Inform. Decis. Mak. 2013, 13, 129. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.C. Innovative health care delivery system-A questionnaire survey to evaluate the influence of behavioral factors on individuals’ acceptance of telecare. Comput. Biol. Med. 2013, 43, 281–286. [Google Scholar] [CrossRef]
- Escobar-Rodríguez, T.; Romero-Alonso, M.M. Modeling nurses’ attitude toward using automated unit-based medication storage and distribution systems: An extension of the technology acceptance model. CIN—Comput. Inform. Nurs. 2013, 31, 235–243. [Google Scholar] [CrossRef]
- Arning, K.; Kowalewski, S.; Ziefle, M. Modelling user acceptance of wireless medical technologies. In Proceedings of the Lecture Notes of the Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering (LNICST), Paris, France, 7–8 November 2013; Volume 61, pp. 146–153. [Google Scholar]
- Sarlan, A.; Ahmad, R.; Fatimah, W.; Ahmad, W.; Dominic, P.D.D. Private Healthcare in Malaysia: Investigation on Technology Profiles and Technology Acceptance Factors. In Proceedings of the Information Systems International Conference (ISICO), Bali, Indonesia, 2–4 December 2013; pp. 98–103. [Google Scholar]
- Cocosila, M. Role of user a priori attitude in the acceptance of mobile health: An empirical investigation. Electron. Mark. 2013, 23, 15–27. [Google Scholar] [CrossRef]
- Chen, S.C.; Liu, S.C.; Li, S.H.; Yen, D.C. Understanding the mediating effects of relationship quality on technology acceptance: An empirical study of E-appointment system. J. Med. Syst. 2013, 37. [Google Scholar] [CrossRef] [PubMed]
- Kummer, T.F.; Schäfer, K.; Todorova, N. Acceptance of hospital nurses toward sensor-based medication systems: A questionnaire survey. Int. J. Nurs. Stud. 2013, 50, 508–517. [Google Scholar] [CrossRef]
- Kuo, K.M.; Liu, C.F.; Ma, C.C. An investigation of the effect of nurses’ technology readiness on the acceptance of mobile electronic medical record systems. BMC Med. Inform. Decis. Mak. 2013, 13, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Krueklai, S.; Kiattisin, S.; Leelasantitham, A. Analysis of factor affecting in unified theory of acceptance and use of technology (UTAUT) e-healthcare of government hospitals in Thailand. Int. Conf. Inf. Soc. Sci. Int. Symp. Mark. Logist. Bus. 2013, 443–451. [Google Scholar]
- Manimaran, S.; Lakshmi, K.B. Development of model for assessing the acceptance level of users in rural healthcare system of Tamilnadu, India. Technol. Health Care 2013, 21, 479–492. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, N.; Jahanbakhsh, M.; Shahin, A.; Mokhtari, H.; Rafiei, M. Electronic medical record in central polyclinic of isfahan oil industry: A case study based on technology acceptance model. Acta Inform. Medica 2013, 21, 23–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, J.D.; Yi, M.Y.; Park, J.S. An empirical test of three mediation models for the relationship between personal innovativeness and user acceptance of technology. Inf. Manag. 2013, 50, 154–161. [Google Scholar] [CrossRef]
- Mohamed, A.H.H.M.; Tawfik, H.; Norton, L.; Al-Jumeily, D. A Technology Acceptance Model for a User-Centred Culturally-Aware E-Health Design. In Proceedings of the 2013 Sixth International Conference on Developments in eSystems Engineering (IEEE), Abu Dhabi, United Arab Emirates, 16–18 December 2013; pp. 121–125. [Google Scholar]
- Ford, S. “Drew” Age, Performance and Retention Interval Effects on Acceptance of a Consumer Health Information Technology System; Louisiana State University: Baton Rouge, LA, USA, 2014. [Google Scholar]
- Alaiad, A.; Zhou, L.; Koru, G. An exploratory study of home healthcare robots adoption applying the UTAUT model. Int. J. Healthc. Inf. Syst. Inform. 2014, 9, 44–59. [Google Scholar] [CrossRef]
- Lin, H.C. An investigation of the effects of cultural differences on physicians’ perceptions of information technology acceptance as they relate to knowledge management systems. Comput. Hum. Behav. 2014, 38, 368–380. [Google Scholar] [CrossRef]
- Hsieh, P.J.; Lai, H.M.; Ye, Y.S. Patients’ acceptance and resistance toward the health cloud: An integration of technology acceptance and status quo bias perspectives. In Proceedings of the Proceedings—Pacific Asia Conference on Information Systems (PACIS 2014), Chengdu, China, 24–28 June 2014. [Google Scholar]
- Gagnon, M.P.; Ghandour, E.K.; Talla, P.K.; Simonyan, D.; Godin, G.; Labrecque, M.; Ouimet, M.; Rousseau, M. Electronic health record acceptance by physicians: Testing an integrated theoretical model. J. Biomed. Inform. 2014, 48, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Fleming, M.L.; Hatfield, M.D.; Wattana, M.K.; Todd, K.H. Exploratory study of emergency physicians’ use of a prescription monitoring program using a framework of technology acceptance. J. Pain Palliat. Care Pharmacother. 2014, 28, 19–27. [Google Scholar] [CrossRef]
- Corneille, M.; Carter, L.; Hall-Byers, N.M.; Clark, T.; Younge, S. Exploring user acceptance of a text-message based health intervention. In Proceedings of the Annual Hawaii International Conference on System Sciences, Waikoloa, HI, USA, 6–9 January 2014; pp. 2759–2767. [Google Scholar]
- Steininger, K.; Stiglbauer, B.; Baumgartner, B.; Engleder, B. Factors explaining physicians’ acceptance of electronic health records. In Proceedings of the Annual Hawaii International Conference on System Sciences, Waikoloa, HI, USA, 6–9 January 2014; pp. 2768–2777. [Google Scholar]
- Hwang, J.Y.; Kim, K.Y.; Lee, K.H. Factors that influence the acceptance of telemetry by emergency medical technicians in ambulances: An application of the extended technology acceptance model. Telemed. e-Health 2014, 20, 1127–1134. [Google Scholar] [CrossRef] [Green Version]
- Hung, S.Y.; Tsai, J.C.A.; Chuang, C.C. Investigating primary health care nurses’ intention to use information technology: An empirical study in Taiwan. Decis. Support Syst. 2014, 57, 331–342. [Google Scholar] [CrossRef]
- Rho, M.J.; young Choi, I.; Lee, J. Predictive factors of telemedicine service acceptance and behavioral intention of physicians. Int. J. Med. Inform. 2014, 83, 559–571. [Google Scholar] [CrossRef]
- Moon, B.C.; Chang, H. Technology acceptance and adoption of innovative smartphone uses among hospital employees. Healthc. Inform. Res. 2014, 20, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.H. The adoption of a telehealth system: The integration of extended technology acceptance model and health belief model. J. Med. Imaging Health Inform. 2014, 4, 448–455. [Google Scholar] [CrossRef]
- Yallah, A. A Correlational Study of the Technology Acceptance Model and Georgia Behavioral Healthcare Provider Telemedicine Adoption; Northcentral University: Scottsdale, AZ, USA, 2014; Volume 3622519. [Google Scholar]
- Cleveland, S.D. Factors Predicting Nurse Educators’ Acceptance and Use of Educational Technology in Classroom Instruction. Ph.D. Thesis, Capella University, Minneapolis, MN, USA, 2014. [Google Scholar]
- Devine, D.A. Assessment of Nurse Faculty’s Acceptance and Intent to Use Social Media Using the Unified Theory of Acceptance and Use of Technology 2 Model; Villanova University: Villanova, PA, USA, 2015. [Google Scholar]
- Ebie, S.; Njoku, E. Extension of the technology acceptance model (TAM) to the adoption of the electronic knowledge and skills framework (E-KSF) in the national health service (NHS). J. Appl. Sci. Dev. 2015, 6, 19–50. [Google Scholar]
- Krishnan, S.B.; Dhillon, J.S.; Lutteroth, C. Factors influencing consumer intention to adopt Consumer Health Informatics applications an empirical study in Malaysia. In Proceedings of the 2015 IEEE Student Conference on Research and Development (SCOReD 2015), Kuala Lumpur, Malaysia, 13–14 December 2015; pp. 653–658. [Google Scholar]
- Basak, E.; Gumussoy, C.A.; Calisir, F. Examining the factors affecting PDA acceptance among physicians: An extended technology acceptance model. J. Healthc. Eng. 2015, 6, 399–418. [Google Scholar] [CrossRef]
- Briz-Ponce, L.; García-Peñalvo, F.J. An empirical assessment of a technology acceptance model for apps in medical education. J. Med. Syst. 2015, 39, 176. [Google Scholar] [CrossRef]
- Song, L.; Park, B.; Oh, K.M. Analysis of the Technology Acceptance Model in Examining Hospital Nurses’ Behavioral Intentions Toward the Use of Bar Code Medication Administration. CIN—Comput. Inform. Nurs. 2015, 33, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Holahan, P.J.; Lesselroth, B.J.; Adams, K.; Wang, K.; Church, V. Beyond technology acceptance to effective technology use: A parsimonious and actionable model. J. Am. Med. Inform. Assoc. 2015, 22, 718–729. [Google Scholar] [CrossRef] [PubMed]
- Ahadzadeh, A.S.; Pahlevan Sharif, S.; Ong, F.S.; Khong, K.W. Integrating Health Belief Model and Technology Acceptance Model: An investigation of health-related Internet use. J. Med. Internet Res. 2015, 17, e3564. [Google Scholar] [CrossRef] [PubMed]
- Kowitlawakul, Y.; Chan, S.W.C.; Pulcini, J.; Wang, W. Factors influencing nursing students’ acceptance of electronic health records for nursing education (EHRNE) software program. Nurse Educ. Today 2015, 35, 189–194. [Google Scholar] [CrossRef]
- Elaklouk, A.M.; Mat Zin, N.A.; Shapii, A. Investigating therapists’ intention to use serious games for acquired brain injury cognitive rehabilitation. J. King Saud Univ.—Comput. Inf. Sci. 2015, 27, 160–169. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.Y.; Pang, C.; Michael Tarn, J.; Liu, T.S.; Yen, D.C. Exploring user acceptance of an e-hospital service: An empirical study in Taiwan. Comput. Stand. Interfaces 2015, 38, 35–43. [Google Scholar] [CrossRef]
- Hsieh, P.J. Healthcare professionals’ use of health clouds: Integrating technology acceptance and status quo bias perspectives. Int. J. Med. Inform. 2015, 84, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Steininger, K.; Stiglbauer, B. EHR acceptance among Austrian resident doctors. Health Policy Technol. 2015, 4, 121–130. [Google Scholar] [CrossRef]
- De Veer, A.J.E.; Peeters, J.M.; Brabers, A.E.M.; Schellevis, F.G.; Rademakers, J.J.D.J.M.; Francke, A.L. Determinants of the intention to use e-health by community dwelling older people. BMC Health Serv. Res. 2015, 15, 103. [Google Scholar] [CrossRef] [Green Version]
- Ku, W.T.; Hsieh, P.J. Taiwanese middle-aged and elderly patients’ acceptance and resistance toward the health cloud. In Proceedings of the International Conference on Human Aspects of IT for the Aged Population, Los Angeles, CA, USA, 2–7 August 2015; Springer: Berlin/Heidelberg, Germany; Volume 9194, pp. 89–100. [Google Scholar]
- Liu, C.F.; Cheng, T.J. Exploring critical factors influencing physicians’ acceptance of mobile electronic medical records based on the dual-factor model: A validation in Taiwan. BMC Med. Inform. Decis. Mak. 2015, 15, 4. [Google Scholar] [CrossRef] [Green Version]
- Miiro, E.; Maiga, G. A model of e-health acceptance and usage in uganda: The perspective of online social networks. In Proceedings of the International Conference on e-Infrastructure and e-Services for Developing Countries, Kampala, Uganda, 24–25 November 2015; Springer: Berlin/Heidelberg, Germany; Volume 147, pp. 115–126. [Google Scholar]
- Zaman, N. An Investigation of Nurse Technology Training and Acceptance of Electronic Documentation Systems (e.g., EHR, EMR, EPR); North Carolina A&T State University: Greensboro, NC, USA, 2015. [Google Scholar]
- Sezgin, E.; Özkan-Yıldırım, S. A cross-sectional investigation of acceptance of health information technology: A nationwide survey of community pharmacists in Turkey. Res. Soc. Adm. Pharm. 2016, 12, 949–965. [Google Scholar] [CrossRef]
- Mansur, F.; Cakmak, E.K. A Study for determining the variables having impact on health manager’s acceptance and use of technology: Example of ankara province. Int. J. Health Manag. Tour. 2016, 1, 37–55. [Google Scholar]
- Moon, Y.J.; Hwang, Y.H. A study of effects of UTAUT-based factors on acceptance of smart health care services. In Advanced Multimedia and Ubiquitous Engineering; Springer: Berlin/Heidelberg, Germany, 2016; Volume 354, pp. 317–324. ISBN 9783662478943. [Google Scholar]
- Ku, W.T.; Hsieh, P.J. Acceptance of cloud-based healthcare services by elderly Taiwanese people. In Proceedings of the International Conference on Human Aspects of IT for the Aged Population, Toronto, ON, Canada, 17–22 July 2016; Springer: Berlin/Heidelberg, Germany; Volume 9754, pp. 186–195. [Google Scholar]
- Made Dhanar, I.Y.; Reza, M.; Meyliana; Widjaja, H.A.E.; Hidayanto, A.N. Acceptance of HIS usage level in hospital with SEM-PLS as analysis methodology: Case study of a private hospital in Indonesia. In Proceedings of the 2016 International Conference on Information Management and Technology (ICIMTech 2016), Bandung, Indonesia, 16–18 November 2016; pp. 112–117. [Google Scholar]
- Hsiao, J.L.; Chen, R.F. Critical factors influencing physicians’ intention to use computerized clinical practice guidelines: An integrative model of activity theory and the technology acceptance model. BMC Med. Inform. Decis. Mak. 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Lazard, A.J.; Watkins, I.; Mackert, M.S.; Xie, B.; Stephens, K.K.; Shalev, H. Design simplicity influences patient portal use: The role of aesthetic evaluations for technology acceptance. J. Am. Med. Inform. Assoc. 2016, 23, e157–e161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.Y.; Chou, W.C.; Tsai, T.H.; Lin, C.C.; Lee, M.Y. Development of a wearable instrumented vest for posture monitoring and system usability verification based on the technology acceptance model. Sensors 2016, 16, 2172. [Google Scholar] [CrossRef] [Green Version]
- Al-Nassar, B.A.Y.; Rababah, K.A.; Al-Nsour, S.N. Impact of computerised physician order entry in Jordanian hospitals by using technology acceptance model. Int. J. Inf. Syst. Chang. Manag. 2016, 8, 191–210. [Google Scholar] [CrossRef]
- Lazuras, L.; Dokou, A. Mental health professionals’ acceptance of online counseling. Technol. Soc. 2016, 44, 10–14. [Google Scholar] [CrossRef]
- Ifinedo, P.; Griscti, O.; Bailey, J.; Profit, S. Nova Scotia Nurses’ Acceptance of Healthcare Information Systems: Focus on Technology Characteristics and Related Factors. Can. J. Nurs. Inform. 2016, 11, 1–13. [Google Scholar]
- Holden, R.J.; Asan, O.; Wozniak, E.M.; Flynn, K.E.; Scanlon, M.C. Nurses’ perceptions, acceptance, and use of a novel in-room pediatric ICU technology: Testing an expanded technology acceptance model. BMC Med. Inform. Decis. Mak. 2016, 16, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducey, A.J.; Coovert, M.D. Predicting tablet computer use: An extended Technology Acceptance Model for physicians. Health Policy Technol. 2016, 5, 268–284. [Google Scholar] [CrossRef]
- Chen, M.S.; Chang, S.W.; Lai, Y.H. The intention to use the cloud sphygmomanometer-demonstrated by Taiwan medical center. In Proceedings of the Proceedings—2016 9th International Congress on Image and Signal Processing, BioMedical Engineering and Informatics (CISP-BMEI 2016), Datong, China, 15–17 October 2016; pp. 1843–1848. [Google Scholar]
- Guo, X.; Zhang, X.; Sun, Y. The privacy-personalization paradox in mHealth services acceptance of different age groups. Electron. Commer. Res. Appl. 2016, 16, 55–65. [Google Scholar] [CrossRef]
- Becker, D. Acceptance of Mobile Mental Health Treatment Applications. Procedia Comput. Sci. 2016, 58, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Shujen Lee, C.; Chen, J.K. 3D bio-printing in medical treatment: A technology acceptance model. In Proceedings of the PICMET 2016—Portland International Conference on Management of Engineering and Technology: Technology Management for Social Innovation, Honolulu, HI, USA, 4–8 September 2016; pp. 3149–3154. [Google Scholar]
- Hsieh, P.J. An empirical investigation of patients’ acceptance and resistance toward the health cloud: The dual factor perspective. Comput. Hum. Behav. 2016, 63, 959–969. [Google Scholar] [CrossRef]
- Jayusman, H.; Setyohadi, D.B. An empirical investigations of user acceptance of “Scalsa” e-learning in stikes Harapan Bangsa Purwokerto. In Proceedings of the 2017 5th International Conference on Cyber and IT Service Management (CITSM 2017), Denpasar, Indonesia, 8–10 August 2017. [Google Scholar]
- Ul Amin, R.; Inayat, I.; Shahzad, B.; Saleem, K.; Aijun, L. An empirical study on acceptance of secure healthcare service in Malaysia, Pakistan, and Saudi Arabia: A mobile cloud computing perspective. Ann. Telecommun. 2017, 72, 253–264. [Google Scholar] [CrossRef]
- Ehteshami, A. Barcode Technology Acceptance and Utilization in Health Information Management Department at Academic Hospitals According to Technology Acceptance Model. Acta Inform. Medica 2017, 25, 4. [Google Scholar] [CrossRef] [Green Version]
- Beglaryan, M.; Petrosyan, V.; Bunker, E. Development of a tripolar model of technology acceptance: Hospital-based physicians’ perspective on EHR. Int. J. Med. Inform. 2017, 102, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Rajanen, D.; Weng, M. Digitization for fun or reward? A study of acceptance of wearable devices for personal healthcare. In Proceedings of the 21st International Academic Mindtrek Conference, Tampere, Finland, 20–21 September 2017; AcademicMindtrek 2017. Association for Computing Machinery, Inc.: New York, NY, USA, 2017; Volume 2017-Janua. [Google Scholar]
- Wahyuni, R. Nurbojatmiko Explaining acceptance of e-health services: An extension of TAM and health belief model approach. In Proceedings of the 2017 5th International Conference on Cyber and IT Service Management (CITSM 2017), Denpasar, Indonesia, 8–10 August 2017. [Google Scholar]
- Nematollahi, M.; Moosavi, A.; Lazem, M.; Aslani, N.; Kafashi, M.; Garavand, A. Factors affecting in adoption and use of electronic medical record based on unified theory of acceptance and use of technology in Iran. Shiraz E Med. J. 2017, 18, 57582. [Google Scholar] [CrossRef] [Green Version]
- Horne, M.E.P. The Technology Acceptance Model and Telemedicine: Predicting Health Care Providers’ Intention to Use Telemedicine; University of Phoenix: Phoenix, AZ, USA, 2017. [Google Scholar]
- Hsieh, P.-J.; Lai, H.-M.; Ku, H.-C.; Ku, W.-T. Understanding Middle-Aged and Elderly Taiwanese People’s Acceptance of the Personal Health Information System for Self-health Management. In Human Aspects of IT for the Aged Population. Applications, Services and Contexts; Springer: Berlin/Heidelberg, Germany, 2017; Volume 10298, pp. 393–403. ISBN 9783319585352. [Google Scholar]
- Lin, H.C. Nurses’ satisfaction with using nursing information systems from technology acceptance model and information systems success model perspectives. CIN—Comput. Inform. Nurs. 2017, 35, 91–99. [Google Scholar] [CrossRef]
- Dou, K.; Yu, P.; Deng, N.; Liu, F.; Guan, Y.; Li, Z.; Ji, Y.; Du, N.; Lu, X.; Duan, H. Patients’ Acceptance of Smartphone Health Technology for Chronic Disease Management: A Theoretical Model and Empirical Test. JMIR mHealth uHealth 2017, 5, e177. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Han, X.; Dang, Y.; Meng, F.; Guo, X.; Lin, J. User acceptance of mobile health services from users’ perspectives: The role of self-efficacy and response-efficacy in technology acceptance. Inform. Health Soc. Care 2017, 42, 194–206. [Google Scholar] [CrossRef]
- Martins, O.; Oyedeji, A.; Abolade, R.; Folorunsho, O. An Empirical Study of Unified Theory of Acceptance and Use of Technology Model for E-Health Technology in Lagos, Nigeria. Futo J. Ser. 2018, 4, 117–126. [Google Scholar]
- Aldosari, B.; Al-Mansour, S.; Aldosari, H.; Alanazi, A. Assessment of factors influencing nurses acceptance of electronic medical record in a Saudi Arabia hospital. Inform. Med. Unlocked 2018, 10, 82–88. [Google Scholar] [CrossRef]
- Ku, W.T.; Hsieh, P.J. Understanding the acceptance of health management mobile services: Integrating theory of planned behavior and health belief model. In Proceedings of the International Conference on Human-Computer Interaction, Las Vegas, NV, USA, 15–20 July 2018; Springer: Berlin/Heidelberg, Germany; Volume 850, pp. 247–252. [Google Scholar]
- Hennemann, S.; Witthöft, M.; Bethge, M.; Spanier, K.; Beutel, M.E.; Zwerenz, R. Acceptance and barriers to access of occupational e-mental health: Cross-sectional findings from a health-risk population of employees. Int. Arch. Occup. Environ. Health 2018, 91, 305–316. [Google Scholar] [CrossRef]
- Vitari, C.; Ologeanu-Taddei, R. The intention to use an electronic health record and its antecedents among three different categories of clinical staff. BMC Health Serv. Res. 2018, 18, 194. [Google Scholar] [CrossRef]
- Zhou, M.; Zhao, L.; Kong, N.; Campy, K.S.; Qu, S.; Wang, S. Factors influencing behavior intentions to telehealth by Chinese elderly: An extended TAM model. Int. J. Med. Inform. 2019, 126, 118–127. [Google Scholar] [CrossRef]
- Francis, R.P. Examining healthcare providers’ acceptance of data from patient self-monitoring devices using structural equation modeling with the UTAUT2 model. Int. J. Healthc. Inf. Syst. Inform. 2019, 14, 44–60. [Google Scholar] [CrossRef]
- Tao, D.; Shao, F.; Wang, H.; Yan, M.; Qu, X. Integrating usability and social cognitive theories with the technology acceptance model to understand young users’ acceptance of a health information portal. Health Inform. J. 2019, 146045821987933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masyarakat, J.K.; Nurhayati1, S.; Anandari1, D.; Ekowati, W. Unified Theory of Acceptance and Usage of Technology (UTAUT) Model to Predict Health Information System Adoption. KEMAS J. Kesehat. Masy. 2019, 15, 89–97. [Google Scholar] [CrossRef]
- Schomakers, E.M.; Lidynia, C.; Ziefle, M. Listen to My Heart? How Privacy Concerns Shape Users’ Acceptance of e-Health Technologies. In Proceedings of the International Conference on Wireless and Mobile Computing, Networking and Communications, Barcelona, Spain, 21–23 October 2019; Volume 2019-Octob, pp. 306–311. [Google Scholar]










| ID | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| 1 | The objective of the study should be related to the application of technology acceptance theories in healthcare. | The study is related to applying technology acceptance or adoption but not in healthcare (e.g., banking). |
| 2 | The research model and its related hypotheses were empirically evaluated. | The research model was evaluated using a qualitative method or not even evaluated. |
| 3 | The study must be a journal article, conference paper, book chapter, Ph.D. dissertation, or master’s thesis. | The study is a review, position paper, editorial, etc. |
| 4 | The study must be published in the English language. | The study is published in languages other than English. |
| ID | Keywords |
|---|---|
| 1 | (“Technology Acceptance”) AND (Healthcare OR Health OR Medical OR Physician OR Nurse OR Patient) |
| 2 | (“Technology Adoption”) AND (Healthcare OR Health OR Medical OR Physician OR Nurse OR Patient) |
| 3 | (“Technology Acceptance”) AND (Healthcare OR Health OR Medical OR Physician OR Nurse OR Patient) AND (“Intention to use” OR “Actual use”) |
| 4 | (“Technology Adoption”) AND (Healthcare OR Health OR Medical OR Physician OR Nurse OR Patient) AND (“Intention to use” OR “Actual use”) |
| Sr. | Question |
|---|---|
| 1 | Does the research have clear aims and objectives? |
| 2 | Are the technology acceptance model and its hypotheses well specified? |
| 3 | Are the data collection methods appropriately detailed? |
| 4 | Does the study explain the reliability and validity of the measures? |
| 5 | Are the statistical techniques utilized to analyze the data well clarified? |
| 6 | Do the findings add to the literature? |
| 7 | Does the study add to the readers’ knowledge or understanding? |
| Technology | Frequency | Countries |
|---|---|---|
| Telemedicine | 19 | Taiwan (4), USA (3), Germany (2), Malaysia (2), South Korea (2), Spain, India, UK, Slovenia, China, Georgia |
| Electronic Health Records | 18 | USA (3), Austria (2), Iran (2), Jordan, India, Turkey, Taiwan, Spain, Saudi Arabia, Singapore, France, Canada, Armenia, Australia |
| HIT Systems in General | 13 | Morocco (2), South Korea (2), UK and UAE (2), Nigeria, Australia, Thailand, Canada, North Macedonia, Turkey, Germany |
| Mobile Applications | 10 | Germany (2), Taiwan (2), China (2), Malawi, Singapore, Spain, UK |
| Cloud Computing | 9 | Taiwan (7), Nigeria, one study conducted in: Malaysia, Pakistan, and Saudi Arabia |
| Wearable Electronic Devices | 7 | Germany (2), Taiwan (2), China (2), USA |
| Computers, Handheld | 6 | USA (2), China, Turkey, South Korea, one study conducted in: UAE and UK |
| Health Information Systems | 6 | Taiwan (3), Canada, Indonesia, Malaysia |
| Intervention, Web-Based | 5 | Taiwan (2), Belgium, Malaysia, Thailand |
| Computer-Assisted Instruction | 5 | Hong Kong (2), Taiwan, Iran, Indonesia |
| Medical Informatics Applications | 3 | USA (3) |
| Electronic Data Processing (Barcode) | 3 | USA (2), Iran |
| Consumer Health Informatics | 3 | USA, Malaysia, Indonesia |
| Mobile Applications/Electronic Records | 3 | Taiwan (2), South Korea |
| Clinical Information Systems | 3 | Malaysia (2), France |
| Hospital Information Systems | 2 | Iran, Indonesia |
| Decision Support Systems, Clinical | 2 | Taiwan, Iran |
| Electronic Prescribing | 2 | USA, Pakistan |
| Health Records, Personal | 2 | USA, China |
| Management Information Systems | 2 | India, one study conducted in: USA and Taiwan |
| Nursing Informatics | 2 | Taiwan (2) |
| Telemetry | 2 | Spain (2) |
| Robotics | 2 | USA, Finland |
| Online Social Networking | 2 | USA, Uganda |
| Other Information Technologies (One Study Each) | 12 | Taiwan (2), USA (2), Iran, Jordan, Spain, Saudi Arabia, Turkey, Malaysia, Singapore, UK |
| Participant Groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Technology | Physicians | Nurses | Pharmacists | Healthcare Professionals | Healthcare Managers | Admin/Clinical Staff | General Population | System Users | Patients | Students |
| Telemedicine | 4 | 1 | 5 | 1 | 4 | 1 | 4 | |||
| Electronic Health Records | 7 | 5 | 2 | 1 | 4 | 1 | 1 | 1 | ||
| HIT Systems in General | 2 | 4 | 1 | 2 | 2 | 1 | 1 | |||
| Mobile Applications | 2 | 4 | 3 | 1 | 1 | |||||
| Cloud Computing | 1 | 3 | 1 | 1 | 3 | |||||
| Wearable Electronic Devices | 1 | 3 | 1 | 2 | ||||||
| Handheld Computers | 3 | 2 | 1 | 1 | 1 | |||||
| Health Information Systems | 3 | 1 | 1 | 2 | 1 | |||||
| Web-Based Systems (Intervention) | 2 | 1 | 1 | 1 | ||||||
| Computer-Assisted Instruction | 1 | 1 | 3 | |||||||
| Medical Informatics Applications | 1 | 1 | 1 | |||||||
| Electronic Data Processing (Barcode) | 1 | 1 | 1 | |||||||
| Consumer Health Informatics | 3 | |||||||||
| Mobile Applications/Electronic Records | 1 | 1 | 1 | |||||||
| Clinical Information Systems | 2 | 3 | ||||||||
| Hospital Information systems | 1 | 1 | 1 | |||||||
| Decision Support Systems | 2 | |||||||||
| Electronic Prescribing | 2 | |||||||||
| Health Records (Personal) | 1 | 1 | ||||||||
| Management Information Systems | 2 | 1 | 1 | |||||||
| Nursing Informatics | 2 | |||||||||
| Telemetry | 2 | 2 | ||||||||
| Robotics | 2 | 1 | ||||||||
| Online Social Networking | 1 | 1 | ||||||||
| Other Technologies | 1 | 1 | 1 | 3 | 2 | 1 | 1 | 2 | ||
| Total | 30 | 24 | 4 | 26 | 7 | 11 | 15 | 20 | 14 | 10 |
| ID | Country | Frequency | Percentage (%) |
|---|---|---|---|
| 1 | China | 7 | 4.73 |
| 2 | Germany | 7 | 4.73 |
| 3 | Iran | 7 | 4.73 |
| 4 | Malaysia | 9 | 6.08 |
| 5 | South Korea | 6 | 4.05 |
| 6 | Spain | 6 | 4.05 |
| 7 | Taiwan | 30 | 20.27 |
| 8 | United Kingdom | 6 | 4.05 |
| 9 | USA | 22 | 14.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlQudah, A.A.; Al-Emran, M.; Shaalan, K. Technology Acceptance in Healthcare: A Systematic Review. Appl. Sci. 2021, 11, 10537. https://doi.org/10.3390/app112210537
AlQudah AA, Al-Emran M, Shaalan K. Technology Acceptance in Healthcare: A Systematic Review. Applied Sciences. 2021; 11(22):10537. https://doi.org/10.3390/app112210537
Chicago/Turabian StyleAlQudah, Adi A., Mostafa Al-Emran, and Khaled Shaalan. 2021. "Technology Acceptance in Healthcare: A Systematic Review" Applied Sciences 11, no. 22: 10537. https://doi.org/10.3390/app112210537
APA StyleAlQudah, A. A., Al-Emran, M., & Shaalan, K. (2021). Technology Acceptance in Healthcare: A Systematic Review. Applied Sciences, 11(22), 10537. https://doi.org/10.3390/app112210537