
FLASH Irradiation with Proton Beams: Beam Characteristics and Their Implications for Beam Diagnostics



Abstract
:1. Clinical Treatments and FLASH Modifications
2. Beam Characteristics
2.1. Beam Currents
2.2. Beam Structure
2.3. Beam Energy
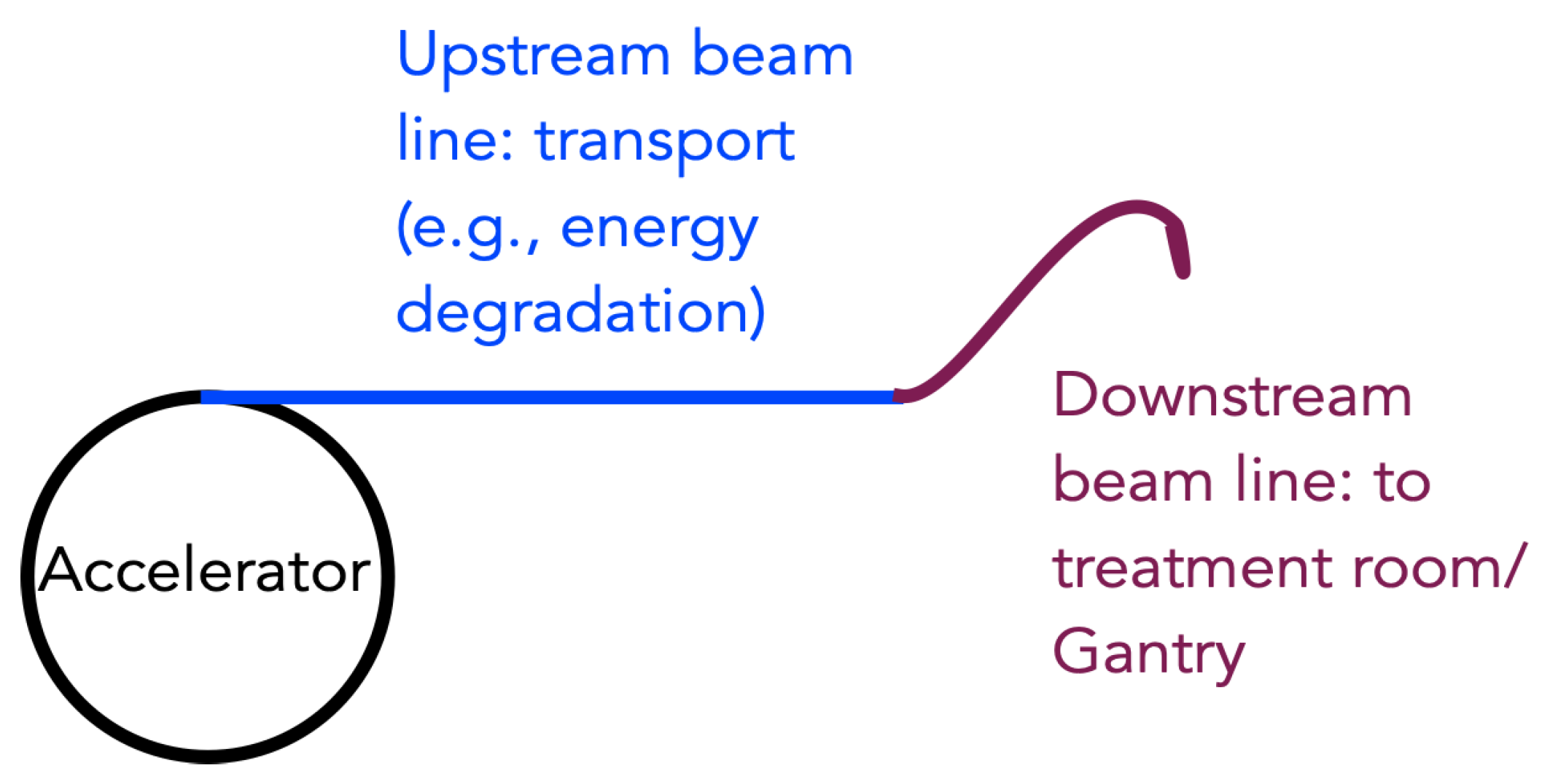
3. Control and Monitoring
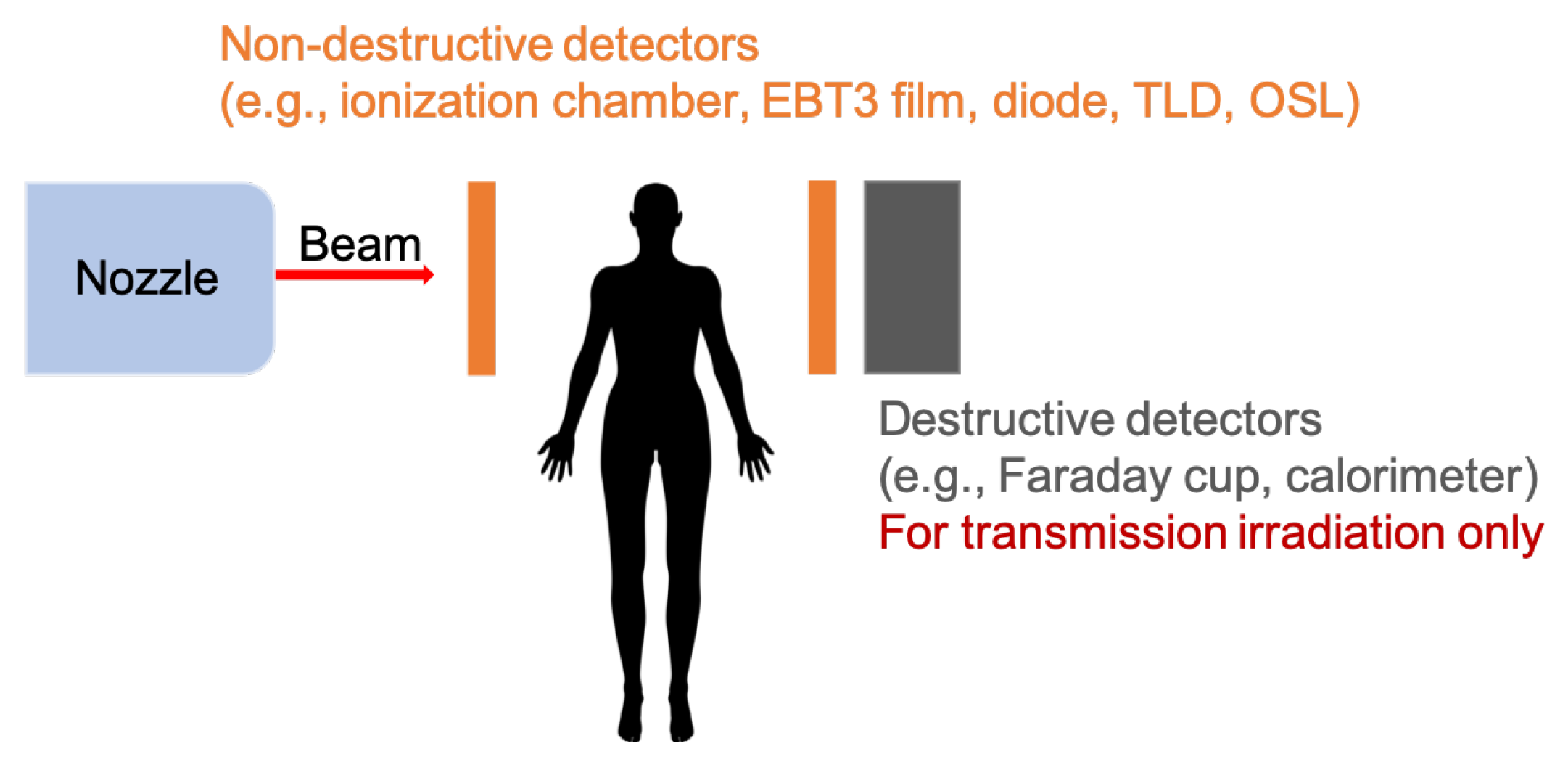
4. Absolute Dose Measurement
4.1. Active Detectors
4.2. Passive Detectors
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Foote, R.L.; Stafford, S.L.; Petersen, I.A.; Pulido, J.S.; Clarke, M.J.; Schild, S.E.; Garces, Y.I.; Olivier, K.R.; Miller, R.C.; Haddock, M.G.; et al. The clinical case for proton beam therapy. Radiat. Oncol. 2012, 7, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vozenin, M.C.; Hendry, J.; Limoli, C. Biological Benefits of Ultra-high Dose Rate FLASH Radiotherapy: Sleeping Beauty Awoken. Clin. Oncol. 2019, 31, 407–415. [Google Scholar] [CrossRef]
- Wilson, P.; Jones, B.; Yokoi, T.; Hill, M.; Vojnovic, B. Revisiting the ultra-high dose rate effect: Implications for charged particle radiotherapy using protons and light ions. Br. J. Radiol. 2012, 85, e933. [Google Scholar] [CrossRef] [Green Version]
- Favaudon, V.; Caplier, L.; Monceau, V.; Pouzoulet, F.; Sayarath, M.; Fouillade, C.; Poupon, M.F.; Brito, I.; Hupé, P.; Bourhis, J.; et al. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumor tissue in mice. Sci. Transl. Med. 2014, 6, 245ra93–245ra93. [Google Scholar] [CrossRef] [PubMed]
- Montay-Gruel, P.; Petersson, K.; Jaccard, M.; Boivin, G.; Germond, J.F.; Petit, B.; Doenlen, R.; Favaudon, V.; Bochud, F.; Bailat, C.; et al. Irradiation in a flash: Unique sparing of memory in mice after whole brain irradiation with dose rates above 100 Gy/s. Radiother. Oncol. 2017, 124, 365–369. [Google Scholar] [CrossRef]
- Citrin, D.E.; Mitchell, J.B. Mechanisms of Normal Tissue Injury From Irradiation. Semin. Radiat. Oncol. 2017, 27, 316–324. [Google Scholar] [CrossRef]
- Schüler, E.; Trovati, S.; King, G.; Lartey, F.; Rafat, M.; Villegas, M.; Praxel, A.J.; Loo, B.W.; Maxim, P.G. Experimental Platform for Ultra-high Dose Rate FLASH Irradiation of Small Animals Using a Clinical Linear Accelerator. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 195–203. [Google Scholar] [CrossRef]
- Lempart, M.; Blad, B.; Adrian, G.; Bäck, S.; Knöös, T.; Ceberg, C.; Petersson, K. Modifying a clinical linear accelerator for delivery of ultra-high dose rate irradiation. Radiother. Oncol. 2019, 139, 40–45. [Google Scholar] [CrossRef]
- Patriarca, A.; Fouillade, C.; Auger, M.; Martin, F.; Pouzoulet, F.; Nauraye, C.; Heinrich, S.; Favaudon, V.; Meyroneinc, S.; Dendale, R.; et al. Experimental Set-up for FLASH Proton Irradiation of Small Animals Using a Clinical System. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Bourhis, J.; Montay-Gruel, P.; Gonçalves Jorge, P.; Bailat, C.; Petit, B.; Ollivier, J.; Jeanneret-Sozzi, W.; Ozsahin, M.; Bochud, F.; Moeckli, R.; et al. Clinical translation of FLASH radiotherapy: Why and how? Radiother. Oncol. 2019, 139, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Esplen, N.M.; Mendonca, M.S.; Bazalova-Carter, M. Physics and biology of ultrahigh dose-rate (FLASH) radiotherapy: A topical review. Phys. Med. Biol. 2020, 65, 23TR03. [Google Scholar] [CrossRef]
- Bourhis, J.; Sozzi, W.J.; Jorge, P.G.; Gaide, O.; Bailat, C.; Duclos, F.; Patin, D.; Ozsahin, M.; Bochud, F.; Germond, J.F.; et al. Treatment of a first patient with FLASH-radiotherapy. Radiother. Oncol. 2019, 139, 18–22. [Google Scholar] [CrossRef]
- ClinicalTrials.gov [Internet]. Identifier NCT04592887, Feasibility Study of FLASH Radiotherapy for the Treatment of Symptomatic Bone Metastases (FAST-01); National Library of Medicine (US): Bethesda, MD, USA, 2020. Available online: clinicaltrials.gov/ct2/show/NCT04592887 (accessed on 15 January 2021).
- Dölling, R.; Lin, S.; Duperrex, P.; Gamma, G.; Keil, B. Beam diagnostics for the proton therapy facility PROSCAN. In Proceedings of the 8th International Topical Meeting on Nuclear Applications and Utilization of Accelerators, ACCAPP’07, Pocatello, ID, USA, 29 July–2 August 2007. [Google Scholar]
- Coutrakon, G.; Miller, D.; Kross, B.J.; Anderson, D.F.; DeLuca, P., Jr.; Siebers, J. A beam intensity monitor for the Loma Linda cancer therapy proton accelerator. Med. Phys. 1991, 18, 817–820. [Google Scholar] [CrossRef]
- Srinivasan, S.; Duperrex, P.A.; Schippers, J.M. Beamline characterization of a dielectric-filled reentrant cavity resonator as beam current monitor for a medical cyclotron facility. Phys. Med. 2020, 78, 101–108. [Google Scholar] [CrossRef]
- Auger, M.; Braccini, S.; Carzaniga, T.; Ereditato, A.; Nesteruk, K.; Scampoli, P. A detector based on silica fibers for ion beam monitoring in a wide current range. J. Instrum. 2016, 11, P03027. [Google Scholar] [CrossRef]
- Nesteruk, K.; Auger, M.; Braccini, S.; Carzaniga, T.; Ereditato, A.; Scampoli, P. A system for online beam emittance measurements and proton beam characterization. J. Instrum. 2018, 13, P01011. [Google Scholar] [CrossRef] [Green Version]
- Braccini, S. Compact Medical Cyclotrons and their use for Radioisotope Production and Multi-disciplinary Research. In Proceedings of the International Conference on Cyclotrons and Their Applications (Cyclotrons’16), Zurich, Switzerland, 11–16 September 2016; Number 21 in International Conference on Cyclotrons and Their Applications. JACoW: Geneva, Switzerland, 2017; pp. 229–234. [Google Scholar] [CrossRef]
- Farr, J.B.; Flanz, J.B.; Gerbershagen, A.; Moyers, M.F. New horizons in particle therapy systems. In Medical Physics; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2018; Volume 45, pp. e953–e983. [Google Scholar] [CrossRef] [Green Version]
- Darafsheh, A.; Hao, Y.; Zwart, T.; Wagner, M.; Catanzano, D.; Williamson, J.F.; Knutson, N.; Sun, B.; Mutic, S.; Zhao, T. Feasibility of proton FLASH irradiation using a synchrocyclotron for preclinical studies. Med. Phys. 2020, 47, 4348–4355. [Google Scholar] [CrossRef] [PubMed]
- Schippers, J.M. Chapter 3: Proton Accelerators. In Proton Therapy Physics; Paganetti, H., Ed.; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar]
- Jolly, S.; Owen, H.; Schippers, M.; Welsch, C. Technical challenges for FLASH proton therapy. Phys. Med. 2020, 78, 71–82. [Google Scholar] [CrossRef]
- Iwata, H.; Toshito, T.; Omachi, C.; Umezawa, M.; Shinozawa, Y.; Yamada, M.; Nakajima, K.; Nomura, K.; Ogino, H.; Shibamoto, Y. Scanning Proton FLASH Irradiation Using a Synchrotron Accelerator: Effects on Cultured Cells and Differences by Irradiation Positions. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, e522. [Google Scholar] [CrossRef]
- Diffenderfer, E.S.; Verginadis, I.I.; Kim, M.M.; Shoniyozov, K.; Velalopoulou, A.; Goia, D.; Putt, M.; Hagan, S.; Avery, S.; Teo, K.; et al. Design, Implementation, and in Vivo Validation of a Novel Proton FLASH Radiation Therapy System. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 440–448. [Google Scholar] [CrossRef] [Green Version]
- Psoroulas, S.; Bula, C.; Actis, O.; Weber, D.C.; Meer, D. A predictive algorithm for spot position corrections after fast energy switching in proton pencil beam scanning. Med. Phys. 2018, 45, 4806–4815. [Google Scholar] [CrossRef] [PubMed]
- Nesteruk, K.P.; Calzolaio, C.; Meer, D.; Rizzoglio, V.; Seidel, M.; Schippers, J.M. Large energy acceptance gantry for proton therapy utilizing superconducting technology. Phys. Med. Biol. 2019, 64, 175007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedroni, E.; Bacher, R.; Blattmann, H.; Böhringer, T.; Coray, A.; Lomax, A.; Lin, S.; Munkel, G.; Scheib, S.; Schneider, U. The 200-MeV proton therapy project at the Paul Scherrer Institute: conceptual design and practical realization. Med. Phys. 1995, 22, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Haberer, T.; Becher, W.; Schardt, D.; Kraft, G. Magnetic scanning system for heavy ion therapy. Nucl. Inst. Methods Phys. Res. A 1993, 330, 296–305. [Google Scholar] [CrossRef]
- Lin, S.; Boehringer, T.; Coray, A.; Grossmann, M.; Pedroni, E. More than 10 years experience of beam monitoring with the Gantry 1 spot scanning proton therapy facility at PSI. Med. Phys. 2009, 36, 5331. [Google Scholar] [CrossRef]
- Liszka, M.; Stolarczyk, L.; Kłodowska, M.; Kozera, A.; Krzempek, D.; Mojżeszek, N.; Pędracka, A.; Waligórski, M.P.R.; Olko, P. Ion recombination and polarity correction factors for a plane–parallel ionization chamber in a proton scanning beam. Med. Phys. 2018, 45, 391–401. [Google Scholar] [CrossRef] [Green Version]
- Nesteruk, K.P.; Togno, M.; Grossmann, M.; Lomax, A.J.; Weber, D.C.; Schippers, J.M.; Safai, S.; Meer, D.; Psoroulas, S. Commissioning of a clinical pencil beam scanning proton therapy unit for ultrahigh dose rates (FLASH). arXiv 2021, arXiv:2101.01770. [Google Scholar]
- Winterhalter, C.; Togno, M.; Nesteruk, K.P.; Emert, F.; Psoroulas, S.; Vidal, M.; Meer, D.; Weber, D.C.; Lomax, A.; Safai, S. Faraday cup for commissioning and quality assurance for proton pencil beam scanning beams at conventional and ultra-high dose rates. Phys. Med. Biol. 2020. Submitted. [Google Scholar]
- Boag, J.W.; Hochhäuser, E.; Balk, O.A. The effect of free-electron collection on the recombination correction to ionization measurements of pulsed radiation. Phys. Med. Biol. 1996, 41, 885–897. [Google Scholar] [CrossRef]
- Bruggmoser, G.; Saum, R.; Schmachtenberg, A.; Schmid, F.; Schüle, E. Determination of the recombination correction factorkSfor some specific plane-parallel and cylindrical ionization chambers in pulsed photon and electron beams. Phys. Med. Biol. 2006, 52, N35–N50. [Google Scholar] [CrossRef]
- Dölling, R. Ionisation Chambers and Secondary Emission Monitors at the PROSCAN Beam Lines. AIP Conf. Proc. 2006, 868, 271–280. [Google Scholar] [CrossRef]
- Schippers, M.; Duppich, J.; Goitein, G.; Hug, E.; Jermann, M.; Mezger, A. First Year of Operation of Psi’s New Sc Cyclotron and Beam Lines for Proton Therapy. Proc. Cyclotrons 2007, 2007, 15–17. [Google Scholar]
- Gomà, C.; Lorentini, S.; Meer, D.; Safai, S. Proton beam monitor chamber calibration. Phys. Med. Biol. 2014, 59, 4961–4971. [Google Scholar] [CrossRef] [PubMed]
- Harasimowicz, J.; Welsch, C.P. Faraday cup for low-energy, low-intensity beam measurements at the USR. In Proceedings of the 2010 Beam Instrumentation Workshop, BIW 2010, Newport News, VA, USA, 15–19 April 2010; pp. 257–259. [Google Scholar]
- Auger, M.; Braccini, S.; Ereditato, A.; Nesteruk, K.P.; Scampoli, P. Low current performance of the Bern medical cyclotron down to the pA range. Meas. Sci. Technol. 2015, 26, 94006. [Google Scholar] [CrossRef]
- Palmans, H.; Thomas, R.; Simon, M.; Duane, S.; Kacperek, A.; DuSautoy, A.; Verhaegen, F. A small-body portable graphite calorimeter for dosimetry in low-energy clinical proton beams. Phys. Med. Biol. 2004, 49, 3737–3749. [Google Scholar] [CrossRef]
- Christensen, J.B.; Vestergaard, A.; Andersen, C.E. Using a small-core graphite calorimeter for dosimetry and scintillator quenching corrections in a therapeutic proton beam. Phys. Med. Biol. 2020, 65, 215023. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, A.B. Electronic dosimetry in radiation therapy. Radiat. Meas. 2006, 41, S134–S153. [Google Scholar] [CrossRef]
- Petasecca, M.; Cullen, A.; Fuduli, I.; Espinoza, A.; Porumb, C.; Stanton, C.; Aldosari, A.H.; Bräuer-Krisch, E.; Requardt, H.; Bravin, A.; et al. X-tream: A novel dosimetry system for synchrotron microbeam radiation therapy. J. Instrum. 2012, 7, P07022. [Google Scholar] [CrossRef] [Green Version]
- Fournier, P.; Cornelius, I.; Dipuglia, A.; Cameron, M.; Davis, J.A.; Cullen, A.; Petasecca, M.; Rosenfeld, A.B.; Bräuer-Krisch, E.; Häusermann, D.; et al. X-Tream dosimetry of highly brilliant X-ray microbeams in the MRT hutch of the Australian Synchrotron. Radiat. Meas. 2017, 106, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.A.; Paino, J.R.; Dipuglia, A.; Cameron, M.; Siegele, R.; Pastuovic, Z.; Petasecca, M.; Perevertaylo, V.L.; Rosenfeld, A.B.; Lerch, M.L. Characterisation and evaluation of a PNP strip detector for synchrotron microbeam radiation therapy. Biomed. Phys. Eng. Express 2018, 4, 044002. [Google Scholar] [CrossRef] [Green Version]
- Cirrone, G.; Cuttone, G.; Lo Nigro, S.; Mongelli, V.; Raffaele, L.; Sabini, M.; Valastro, L.; Bucciolini, M.; Onori, S. Dosimetric characterization of CVD diamonds irradiated with 62MeV proton beams. In Nuclear Instruments and Methods in Physics Research Section A: Accelerators, Spectrometers, Detectors and Associated Equipment, Proceedings of the 5th International Conference on Radiation Effects on Semiconductor Materials Detectors and Devices, Florence, Italy, 10–13 October 2004; Elsevier: Amsterdam, The Netherlands, 2005; Volume 552, pp. 197–202. [Google Scholar] [CrossRef]
- Dieterich, S.; Ford, E.; Pavord, D.; Zeng, J. Chapter 3—In-Vivo Dosimetry. In Practical Radiation Oncology Physics; Dieterich, S., Ford, E., Pavord, D., Zeng, J., Eds.; Elsevier: Philadelphia, PA, USA, 2016; pp. 30–39. [Google Scholar] [CrossRef]
- Gomà, C.; Marinelli, M.; Safai, S.; Verona-Rinati, G.; WÃŒrfel, J. The role of a microDiamond detector in the dosimetry of proton pencil beams. Z. Fuer Med. Phys. 2016, 26, 88–94. [Google Scholar] [CrossRef]
- Sorriaux, J.; Kacperek, A.; Rossomme, S.; Lee, J.; Bertrand, D.; Vynckier, S.; Sterpin, E. Evaluation of Gafchromic EBT3 films characteristics in therapy photon, electron and proton beams. Phys. Med. 2013, 29, 599–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buonanno, M.; Grilj, V.; Brenner, D.J. Biological effects in normal cells exposed to FLASH dose rate protons. Radiother. Oncol. 2019, 139, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Desrosiers, M.F.; Puhl, J.M.; Cooper, S.L. An absorbed-dose/dose-rate dependence for the alanine-EPR dosimetry system and its implications in high-dose ionizing radiation metrology. J. Res. Natl. Inst. Stand. Technol. 2008, 113, 79–95. [Google Scholar] [CrossRef] [PubMed]
- Tochilin, E.; Goldstein, N. Dose rate and spectral measurements from pulsed x-ray generators. Health Phys. 1966, 12, 1705–1714. [Google Scholar] [CrossRef]
- Karsch, L.; Beyreuther, E.; Burris-Mog, T.; Kraft, S.; Richter, C.; Zeil, K.; Pawelke, J. Dose rate dependence for different dosimeters and detectors: TLD, OSL, EBT films, and diamond detectors. Med. Phys. 2012, 39, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Jorge, P.G.; Jaccard, M.; Petersson, K.; Gondré, M.; Durán, M.T.; Desorgher, L.; Germond, J.F.; Liger, P.; Vozenin, M.C.; Bourhis, J.; et al. Dosimetric and preparation procedures for irradiating biological models with pulsed electron beam at ultra-high dose-rate. Radiother. Oncol. 2019, 139, 34–39. [Google Scholar] [CrossRef]
- Jaccard, M.; Petersson, K.; Buchillier, T.; Germond, J.F.; Durán, M.T.; Vozenin, M.C.; Bouhris, J.; Bochud, F.O.; Bailat, C. High dose-per-pulse electron beam dosimetry: usability and dose-rate independence of EBT3 Gafchromic films. Med. Phys. 2017, 44, 725–735. [Google Scholar] [CrossRef]
- Christensen, J.B.; Togno, M.; Nesteruk, K.P.; Psoroulas, S.; Meer, D.; Weber, D.C.; Lomax, T.; Yukihara, E.G.; Safai, S. Al2O3:C optically stimulated luminescence dosimeters (OSLDs) for ultra-high dose-rate proton dosimetry. Phys. Med. Biol. 2021, in press. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Accelerator Type | Isochronous Cyclotron | Synchrocyclotron | Synchrotron |
|---|---|---|---|
| RF Frequency (MHz) | 50–100 | 50–100 | 1–10 |
| Bunch Length (ns) | 1–2 | 1–2 | 25–200 |
| Treatment Pulse Width (s) | - | (1–20) | 0.5–5 |
| Pulse Repetition Rate (Hz) | continuous | ∼ | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nesteruk, K.P.; Psoroulas, S. FLASH Irradiation with Proton Beams: Beam Characteristics and Their Implications for Beam Diagnostics. Appl. Sci. 2021, 11, 2170. https://doi.org/10.3390/app11052170
Nesteruk KP, Psoroulas S. FLASH Irradiation with Proton Beams: Beam Characteristics and Their Implications for Beam Diagnostics. Applied Sciences. 2021; 11(5):2170. https://doi.org/10.3390/app11052170
Chicago/Turabian StyleNesteruk, Konrad P., and Serena Psoroulas. 2021. "FLASH Irradiation with Proton Beams: Beam Characteristics and Their Implications for Beam Diagnostics" Applied Sciences 11, no. 5: 2170. https://doi.org/10.3390/app11052170
APA StyleNesteruk, K. P., & Psoroulas, S. (2021). FLASH Irradiation with Proton Beams: Beam Characteristics and Their Implications for Beam Diagnostics. Applied Sciences, 11(5), 2170. https://doi.org/10.3390/app11052170