
A Fast Method for Whole Liver- and Colorectal Liver Metastasis Segmentations from MRI Using 3D FCNN Networks

 , ,
, , 
Abstract
:1. Introduction
- Detection and segmentation of liver metastasis from T1 MRI in less than 7 s.
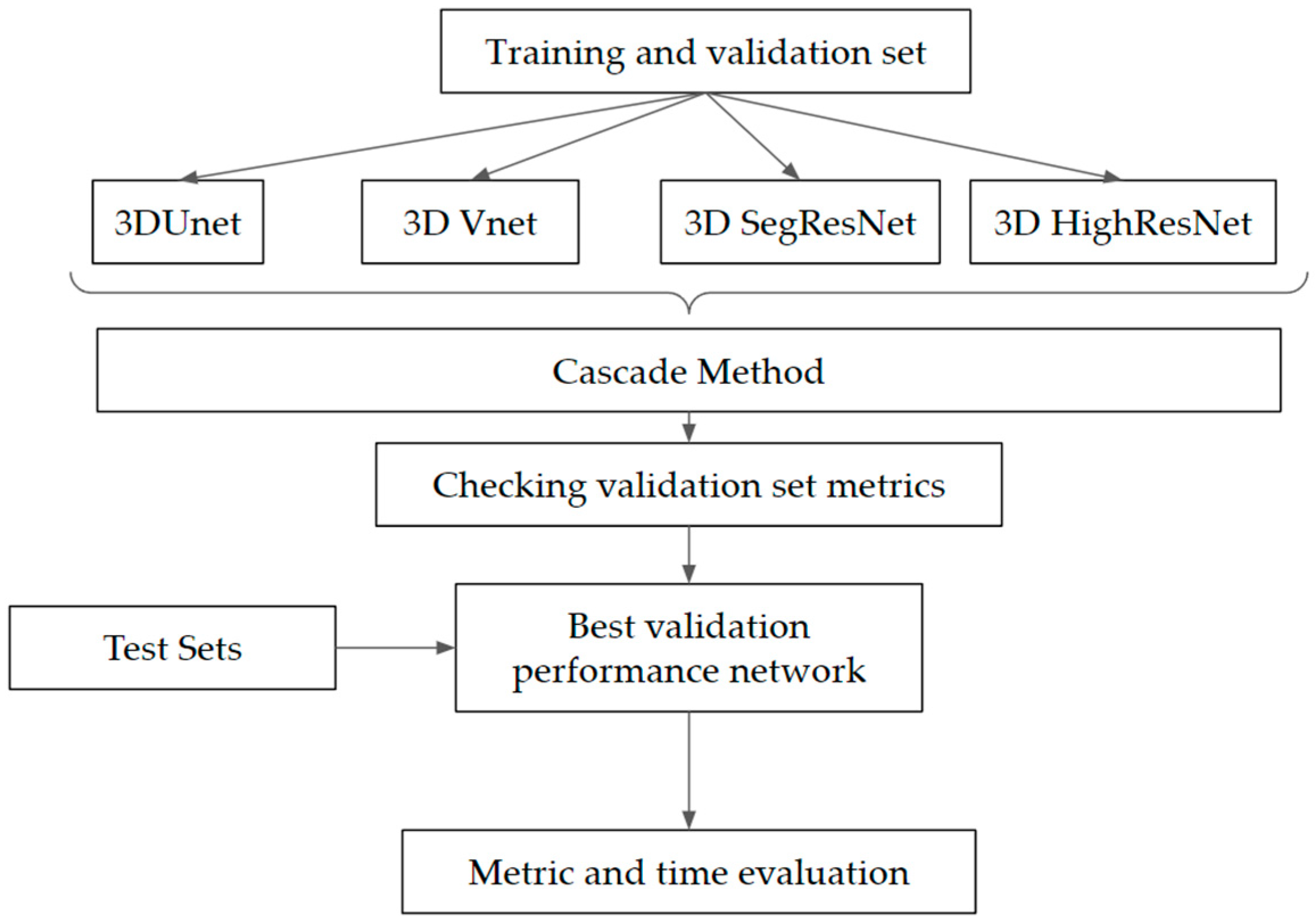
- Creation of a cascade deep learning segmentation method based on the 3D FCNN.
- Comparison of four FCNN segmentation networks on the inhomogeneous MRI dataset.
- HighResNet application for the liver and liver lesion segmentation.
- Creation of a GUI to simplify the integration of the AI tool into medical practice.
2. Literature Review
3. Materials and Methods
3.1. Dataset
3.2. The Method
3.2.1. The Network and Hyperparameters Choice
3.2.2. The Method Implementation Details
3.3. Evaluation
3.3.1. Evaluation Metrics
3.3.2. Evaluation of the Tool by a Medical Expert
4. Results
4.1. Network and Method Validation Results
4.2. Application on the Test Subsets
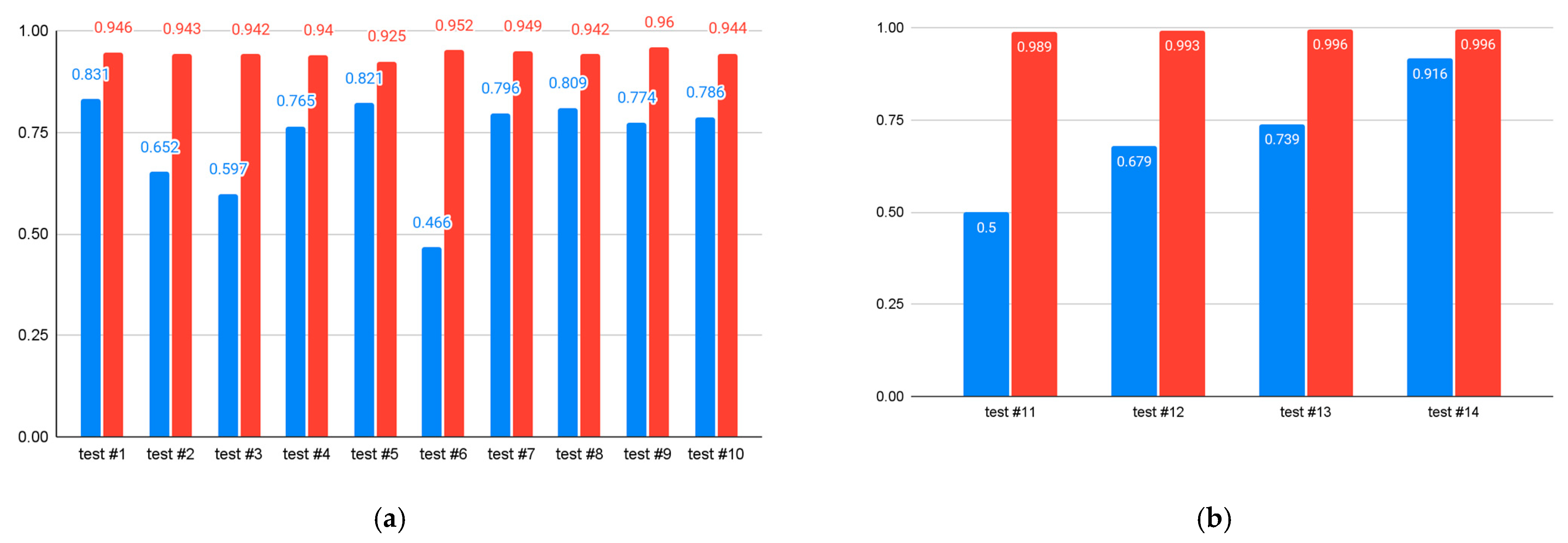
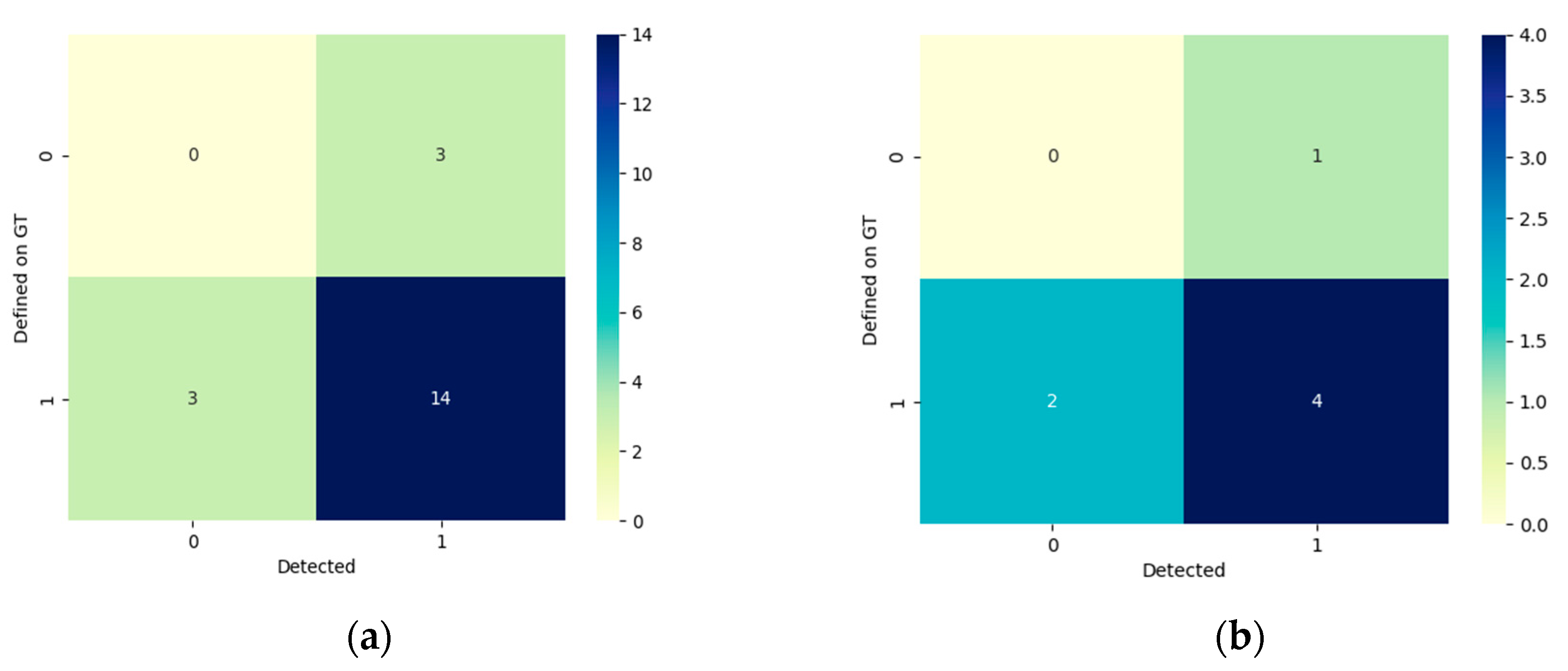
4.2.1. Quantitative Results
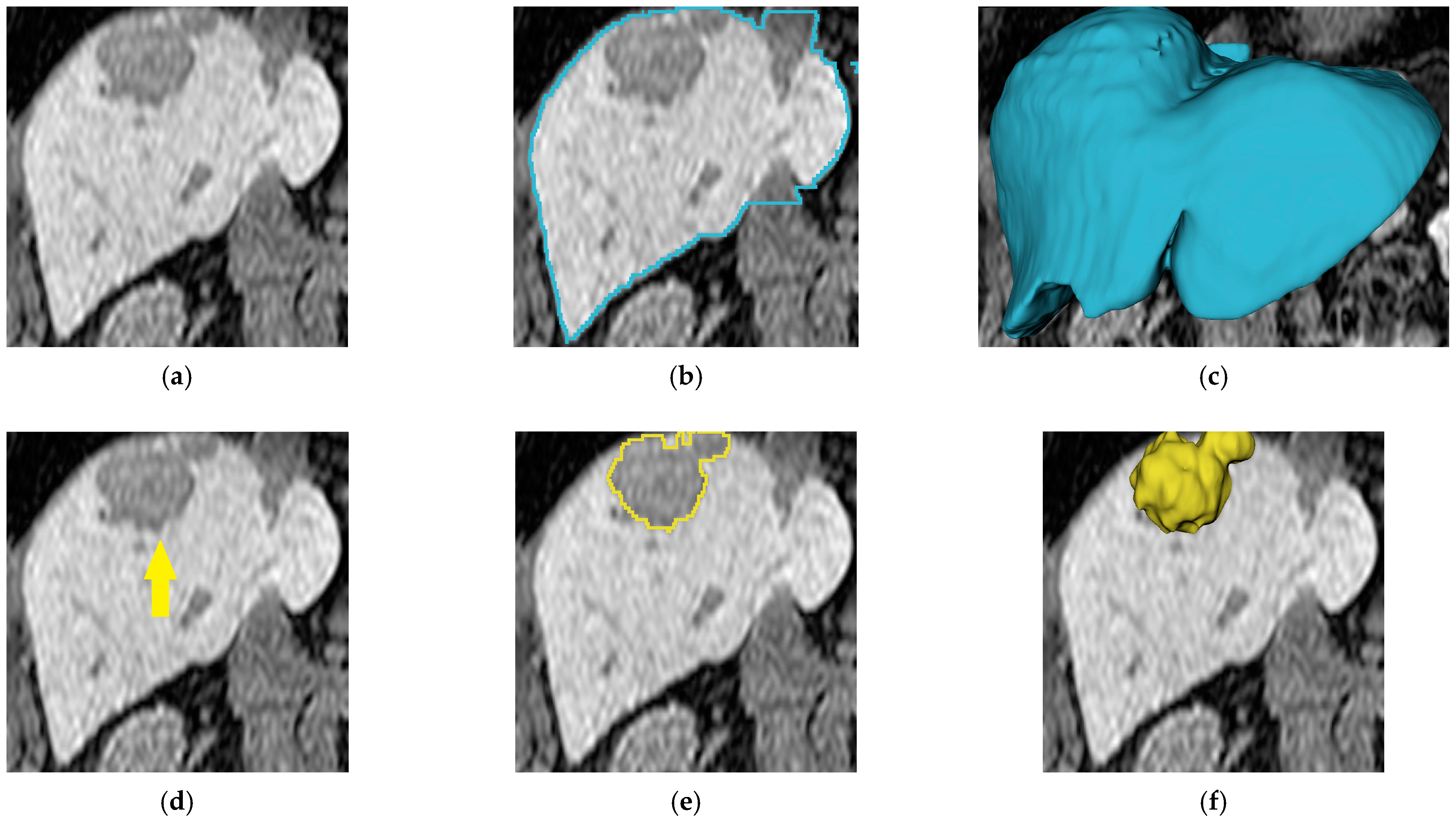
4.2.2. Qualitative Results
5. Discussion
5.1. Principal Findings
5.2. Comparison with Other Studies
5.3. Strength, Limitation, and Potential Future Application of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Correia, M.M.; Choti, M.A.; Rocha, F.G.; Wakabayashi, G. Colorectal Cancer Liver Metastases: A Comprehensive Guide to Management. 2019. Available online: https://sciarium.com/file/463066/ (accessed on 21 October 2021).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cancer in Norway. 2020. Available online: https://www.kreftregisteret.no/Generelt/Rapporter/Cancer-in-Norway/cancer-in-norway-2020/ (accessed on 7 October 2021).
- Gavriilidis, P.; Edwin, B.; Pelanis, E.; Hidalgo, E.; de’Angelis, N.; Memeo, R.; Aldrighetti, L.; Sutcliffe, R.P. Navigated liver surgery: State of the art and future perspectives. Hepatobiliary Pancreat. Dis. Int 2022, 21, 226–233. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Wu, J.; Holtorf, A.P.; Rinde, H.; Xie, S.; Shen, W.; Hou, J.; Li, X.; Li, Z.; Lai, J.; et al. Health economic assessment of Gd-EOB-DTPA MRI versus ECCM-MRI and multi-detector CT for diagnosis of hepatocellular carcinoma in China. PLoS ONE 2018, 13, e0191095. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Clemente, A.; Ierardi, A.M.; Pettinari, I.; Tovoli, F.; Brocchi, S.; Peta, G.; Cappabianca, S.; Carrafiello, G.; Golfieri, R. Imaging of Colorectal Liver Metastases: New Developments and Pending Issues. Cancers 2020, 12, 151. [Google Scholar] [CrossRef] [Green Version]
- Pelanis, E.; Kumar, R.P.; Aghayan, D.L.; Palomar, R.; Fretland, A.; Brun, H.; Elle, O.J.; Edwin, B. Use of mixed reality for improved spatial understanding of liver anatomy. Minim. Invasive Ther. Allied Technol. 2020, 29, 154–160. [Google Scholar] [CrossRef]
- Kumar, R.P.; Pelanis, E.; Bugge, R.; Brun, H.; Palomar, R.; Aghayan, D.L.; Fretland, A.; Edwin, B.; Elle, O.J. Use of mixed reality for surgery planning: Assessment and development workflow. J. Biomed. Inform. 2020, 112, 100077. [Google Scholar] [CrossRef]
- Numminen, K.; Sipilä, O.; Mäkisalo, H. Preoperative hepatic 3D models: Virtual liver resection using three-dimensional imaging technique. Eur. J. Radiol. 2005, 56, 179–184. [Google Scholar] [CrossRef]
- Witowski, J.S.; Coles-Black, J.; Zuzak, T.Z.; Pędziwiatr, M.; Chuen, J.; Major, P.; Budzyński, A. 3D Printing in Liver Surgery: A Systematic Review. Telemed. E-Health 2017, 23, 943–947. [Google Scholar] [CrossRef]
- Gering, D.T.; Nabavi, A.; Kikinis, R.; Hata, N.; Bs, L.J.O.; Grimson, W.E.L.; Jolesz, F.A.; Black, P.M.; Wells, W.M. An integrated visualization system for surgical planning and guidance using image fusion and an open MR. J. Magn. Reson. Imaging 2001, 13, 967–975. [Google Scholar] [CrossRef]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Song, L.; Liu, S.; Zhang, Y. A Review of Deep-Learning-Based Medical Image Segmentation Methods. Sustainability 2021, 13, 1224. [Google Scholar] [CrossRef]
- Zhou, T.; Ruan, S.; Canu, S. A review: Deep learning for medical image segmentation using multi-modality fusion. Array 2019, 3–4, 100004. [Google Scholar] [CrossRef]
- Zhu, J.; Zhang, J.; Qiu, B.; Liu, Y.; Liu, X.; Chen, L. Comparison of the automatic segmentation of multiple organs at risk in CT images of lung cancer between deep convolutional neural network-based and atlas-based techniques. Acta Oncol. 2019, 58, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Çiçek, Ö.; Abdulkadir, A.; Lienkamp, S.S.; Brox, T.; Ronneberger, O. 3D U-Net: Learning Dense Volumetric Segmentation from Sparse Annotation. arXiv 2016, arXiv:160606650. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. arXiv 2015, arXiv:150504597. [Google Scholar]
- Milletari, F.; Navab, N.; Ahmadi, S.-A. V-Net: Fully Convolutional Neural Networks for Volumetric Medical Image Segmentation. arXiv 2021, arXiv:160604797. [Google Scholar]
- Myronenko, A. 3D MRI brain tumor segmentation using autoencoder regularization. arXiv 2019, arXiv:181011654. [Google Scholar]
- Li, W.; Wang, G.; Fidon, L.; Ourselin, S.; Cardoso, M.J.; Vercauteren, T. On the Compactness, Efficiency, and Representation of 3D Convolutional Networks: Brain Parcellation as a Pretext Task. In International Conference on Information Processing in Medical Imaging; Springer: Cham, Switzerland, 2017; Volume 10265, pp. 348–360. [Google Scholar] [CrossRef] [Green Version]
- Vreugdenburg, T.D.; Ma, N.; Duncan, J.K.; Riitano, D.; Cameron, A.L.; Maddern, G.J. Comparative diagnostic accuracy of hepatocyte-specific gadoxetic acid (Gd-EOB-DTPA) enhanced MR imaging and contrast enhanced CT for the detection of liver metastases: A systematic review and meta-analysis. Int. J. Colorectal Dis. 2016, 31, 1739–1749. [Google Scholar] [CrossRef]
- Fretland, A.; Kazaryan, A.M.; Bjørnbeth, B.A.; Flatmark, K.; Andersen, M.H.; Tønnessen, T.I.; Bjørnelv, G.M.W.; Fagerland, M.W.; Kristiansen, R.; Øyri, K.; et al. Open versus laparoscopic liver resection for colorectal liver metastases (the Oslo-CoMet study): Study protocol for a randomized controlled trial. Trials 2015, 16, 73. [Google Scholar] [CrossRef]
- Bilic, P.; Christ, P.F.; Vorontsov, E.; Chlebus, G.; Chen, H.; Dou, Q.; Fu, C.; Han, X.; Heng, P.; Hesser, J.; et al. The Liver Tumor Segmentation Benchmark (LiTS). arXiv 2019, arXiv:190104056. [Google Scholar]
- Jiang, H.; Diao, Z.; Yao, Y.-D. Deep learning techniques for tumor segmentation: A review. J. Supercomput. 2022, 78, 1807–1851. [Google Scholar] [CrossRef]
- Siddique, N.; Sidike, P.; Elkin, C.; Devabhaktuni, V. U-Net and its variants for medical image segmentation: Theory and applications. arXiv 2020, arXiv:201101118. [Google Scholar] [CrossRef]
- Deep Learning. Available online: https://www.deeplearningbook.org/ (accessed on 1 September 2021).
- Nie, D.; Cao, X.; Gao, Y.; Wang, L.; Shen, D. Estimating CT Image From MRI Data Using 3D Fully Convolutional Networks. In Deep Learning and Data Labeling for Medical Applications; Springer: Cham, Switzerland, 2016; pp. 170–178. [Google Scholar] [CrossRef] [Green Version]
- Hatamizadeh, A.; Tang, Y.; Nath, V.; Yang, D.; Myronenko, A.; Landman, B.; Roth, H.R.; Xu, D. UNETR: Transformers for 3D Medical Image Segmentation. arXiv 2021, arXiv:2103.10504. [Google Scholar]
- Meng, L.; Zhang, Q.; Bu, S. Two-Stage Liver and Tumor Segmentation Algorithm Based on Convolutional Neural Network. Diagnostics 2021, 11, 1806. [Google Scholar] [CrossRef] [PubMed]
- Oktay, O.; Schlemper, J.; Folgoc, L.L.; Lee, M.; Heinrich, M.; Misawa, K.; Mori, K.; McDonagh, S.; Hammerla, N.Y.; Kainz, B.; et al. Attention U-Net: Learning Where to Look for the Pancreas. arXiv 2018, arXiv:1804.03999. [Google Scholar]
- Loizou, C.P.; Pantziaris, M.; Seimenis, I.; Pattichis, C.S. Brain MR image normalization in texture analysis of multiple sclerosis. In Proceedings of the 2009 9th International Conference on Information Technology and Applications in Biomedicine, Larnaka, Cyprus, 4–7 November 2009; pp. 1–5. [Google Scholar] [CrossRef]
- Isensee, F.; Petersen, J.; Klein, A.; Zimmerer, D.; Jaeger, P.F.; Kohl, S.; Wasserthal, J.; Koehler, G.; Norajitra, T.; Wirkert, S.; et al. nnU-Net: Self-adapting Framework for U-Net-Based Medical Image Segmentation. arXiv 2018, arXiv:180910486. [Google Scholar]
- Arabi, H.; Shiri, I.; Jenabi, E.; Becker, M.; Zaidi, H. Deep Learning-based Automated Delineation of Head and Neck Malignant Lesions from PET Images. In Proceedings of the 2020 IEEE Nuclear Science Symposium and Medical Imaging Conference (NSS/MIC), Boston, MA, USA, 31 October–7 November 2020; pp. 1–3. [Google Scholar] [CrossRef]
- Deudon, M.; Kalaitzis, A.; Goytom, I.; Arefin, M.R.; Lin, Z.; Sankaran, K.; Michalski, V.; Kahou, S.E.; Cornebise, J.; Bengio, Y. HighRes-net: Recursive Fusion for Multi-Frame Super-Resolution of Satellite Imagery. arXiv 2020, arXiv:2002.06460. [Google Scholar]
- Roy, S.S.; Rodrigues, N.; Taguchi, Y.-H. Incremental Dilations Using CNN for Brain Tumor Classification. Appl. Sci. 2020, 10, 4915. [Google Scholar] [CrossRef]
- Christ, P.F.; Ettlinger, F.; Grün, F.; Elshaera, M.E.A.; Lipkova, J.; Schlecht, S.; Ahmaddy, F.; Tatavarty, S.; Bickel, M.; Bilic, P.; et al. Automatic Liver and Tumor Segmentation of CT and MRI Volumes using Cascaded Fully Convolutional Neural Networks. arXiv 2017, arXiv:1702.05970. [Google Scholar]
- Xi, X.-F.; Wang, L.; Sheng, V.S.; Cui, Z.; Fu, B.; Hu, F. Cascade U-ResNets for Simultaneous Liver and Lesion Segmentation. IEEE Access 2020, 8, 68944–68952. [Google Scholar] [CrossRef]
- Mourya, G.K.; Bhatia, D.; Gogoi, M.; Handique, A. CT Guided Diagnosis: Cascaded U-Net for 3D Segmentation of Liver and Tumor. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1128, 012049. [Google Scholar] [CrossRef]
- Feng, X.; Wang, C.; Cheng, S.; Guo, L. Automatic Liver And Tumor Segmentation Of CT Based On Cascaded U-Net. In Proceedings of the 2018 Chinese Intelligent Systems Conference; Jia, Y., Du, J., Zhang, W., Eds.; Springer: Singapore, 2019; Volume 529, pp. 155–164. [Google Scholar] [CrossRef]
- Bousabarah, K.; Letzen, B.; Tefera, J.; Savic, L.; Schobert, I.; Schlachter, T.; Staib, L.H.; Kocher, M.; Chapiro, J.; Lin, M. Automated detection and delineation of hepatocellular carcinoma on multiphasic contrast-enhanced MRI using deep learning. Abdom. Radiol. 2020, 46, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, D.; Xiao, X.; Accorsi, F.; Marshall, H.; Cossetto, T.; Kim, D.; McCarthy, D.; Dawson, C.; Knezevic, S.; et al. United adversarial learning for liver tumor segmentation and detection of multi-modality non-contrast MRI. Med. Image. Anal. 2021, 73, 102154. [Google Scholar] [CrossRef] [PubMed]
- Sakinis, T.; Milletari, F.; Roth, H.; Korfiatis, P.; Kostandy, P.; Philbrick, K.; Akkus, Z.; Xu, Z.; Xu, D.; Erickson, B.J. Interactive segmentation of medical images through fully convolutional neural networks. arXiv 2019, arXiv:190308205. [Google Scholar]
- Kerfoot, E.; Clough, J.; Oksuz, I.; Lee, J.; King, A.P.; Schnabel, J.A. Left-Ventricle Quantification Using Residual U-Net. In Statistical Atlases and Computational Models of the Heart. Atrial Segmentation and LV Quantification Challenges; Springer: Cham, Switzerland, 2019; pp. 371–380. [Google Scholar] [CrossRef]
- Ioffe, S.; Szegedy, C. Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift. arXiv 2015, arXiv:1502.03167. [Google Scholar]
- Ulyanov, D.; Vedaldi, A.; Lempitsky, V. Instance Normalization: The Missing Ingredient for Fast Stylization. arXiv 2017, arXiv:1607.08022. [Google Scholar]
- Wu, Y.; He, K. Group Normalization. arXiv 2018, arXiv:1803.08494. [Google Scholar]
- Ma, J.; Chen, J.; Ng, M.; Huang, R.; Li, Y.; Li, C.; Yang, X.; Martel, A.L. Loss odyssey in medical image segmentation. Med. Image Anal. 2021, 71, 102035. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Van der Walt, S.; Schönberger, J.L.; Nunez-Iglesias, J.D.; Boulogne, F.; Warner, J.; Yager, N.; Gouillart, E.; Yu, T. scikit-image: Image processing in Python. PeerJ 2014, 2, e453. [Google Scholar] [CrossRef]
- Schwier, M.; Moltz, J.H.; Peitgen, H.-O. Object-based analysis of CT images for automatic detection and segmentation of hypodense liver lesions. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 737–747. [Google Scholar] [CrossRef]
- PySimpleGUI. Available online: https://pysimplegui.readthedocs.io/en/latest/#legal (accessed on 5 January 2022).
- Hugen, N.; van de Velde, C.J.H.; de Wilt, J.H.W.; Nagtegaal, I.D. Metastatic pattern in colorectal cancer is strongly influenced by histological subtype. Ann. Oncol. 2014, 25, 651–657. [Google Scholar] [CrossRef]
- Owler, J.; Irving, B.; Ridgeway, G.; Wojciechowska, M.; Mcgonigle, J.; Brady, S.M. Comparison of Multi-Atlas Segmentation and U-Net Approaches for Automated 3D Liver Delineation in MRI. In Medical Image Understanding and Analysis; Springer: Cham, Switzerland, 2020; pp. 478–488. [Google Scholar] [CrossRef]
- Winther, H.; Hundt, C.; Ringe, K.I.; Wacker, F.K.; Schmidt, B.; Jürgens, J.; Haimerl, M.; Beyer, L.P.; Stroszczynski, C.; Wiggermann, P.; et al. A 3D Deep Neural Network for Liver Volumetry in 3T Contrast-Enhanced MRI. ROFO. Fortschr. Geb. Rontgenstr. Nuklearmed. 2021, 193, 305–314. [Google Scholar] [CrossRef]
- Fabijańska, A.; Vacavant, A.; Lebre, M.-A.; Pavan, A.L.M.; de Pina, D.R.; Abergel, A.; Chabrot, P.; Magnin, B. U-Catchcc: An Accurate HCC Detector In Hepatic DCE-MRI Sequences Based On An U-Net Framework. In Computer Vision and Graphics; Chmielewski, L.J., Kozera, R., Orłowski, A., Wojciechowski, K., Bruckstein, A.M., Petkov, N., Eds.; Springer International Publishing: Cham, Switzerland, 2018; Volume 11114, pp. 319–328. [Google Scholar] [CrossRef]
- Jansen, M.J.A.; Kuijf, H.J.; Niekel, M.; Veldhuis, W.B.; Wessels, F.J.; Viergever, M.A.; Pluim, J.P.W. Liver segmentation and metastases detection in MR images using convolutional neural networks. J. Med. Imaging Bellingham Wash 2019, 6, 044003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NVIDIA Clara AI-Assisted Annotation Extension—Development. 3D Slicer Community. 14 July 2019. Available online: https://discourse.slicer.org/t/nvidia-clara-ai-assisted-annotation-extension/7570 (accessed on 21 October 2021).
- Project MONAI. Available online: https://monai.io/ (accessed on 21 October 2021).












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Network | Subject | Sensitivity | Precision | Dice |
|---|---|---|---|---|
| 3D U-net (Stage1) | Liver | 0.940 ± 0.007 | 0.775 ± 0.110 | 0.834 ± 0.054 |
| Tumors | 0 | 0 | 0 | |
| 3D U-net (Full method) | Liver | 0.995 ± 0.007 | 0.873 ± 0.124 | 0.930 ± 0.077 |
| Tumors | 0.167 ± 0.421 | 0.051 ± 0.412 | 0.093 ± 0.365 | |
| V-net (Stage1) | Liver | 0.871 ± 0.079 | 0.589 ± 0.141 | 0.693 ± 0.099 |
| Tumors | 0 | 0 | 0 | |
| V-net (Stage2) | Liver | 0.975 ± 0.026 | 0.762 ± 0.147 | 0.848 ± 0.099 |
| Tumors | 0.3278 ± 0.460 | 0.385 ± 0.382 | 0.275 ± 0.358 | |
| SegResNet (Stage1) | Liver | 0.916 ± 0.062 | 0.746∓0.102 | 0.815 ± 0.046 |
| Tumors | 0 | 0 | 0 | |
| SegResNet (Stage2) | Liver | 0.992 ± 0.008 | 0.796 ± 0.112 | 0.879 ± 0.716 |
| Tumors | 0.663 ± 0.339 | 0.692 ± 0.226 | 0.655 ± 0.281 | |
| HighResNet (Stage 1) | Liver | 0.994 ± 0.003 | 0.859 ± 0.044 | 0.919 ± 0.026 |
| Tumors | 0.948 ± 0.209 | 0.351 ± 0.156 | 0.488 ± 0.153 | |
| HighResNet (Full method) | Liver | 0.988 ± 0.008 | 0.896 ± 0.035 | 0.942 ± 0.017 |
| Tumors | 0.915 ± 0.258 | 0.510 ± 0.165 | 0.626 ± 0.134 |
| Network | Subject | Sensitivity | Precision | Dice |
|---|---|---|---|---|
| Test set #1 compared to GT | Liver | 0.988 ± 0.003 | 0.903 ± 0.019 | 0.944 ± 0.009 |
| Tumors | 0.832 ± 0.163 | 0.699 ± 0.124 | 0.780 ± 0.119 | |
| Test set #2 compared to expert corrections | Liver | 0.996 ± 0.003 | 0.993 ± 0.006 | 0.994 ± 0.003 |
| Tumors | 0.667 ± 0.257 | 0.882 ± 0.146 | 0.709 ± 0.171 |
| Authors, Year | Study Goal and DL Method | Liver Dice | Tumor Dice |
|---|---|---|---|
| Owler et al., 2020 [53] | Liver segmentation using 3D U-net via T1 weighted dataset of 153 cases | 0.970 | n\a |
| Winther et al., 2021 [54] | Liver segmentation using V-net via T1 weighted MRI dataset of 100 patients | 96.0 ± 1.9 | n\a |
| Christ et al., 2017 [36] | Liver and HCC tumor segmentation via 2D U-net from DW-MRI T2-weighted dataset of 31 patients | 87 | 69.7 |
| Fabijańska et al., 2018 [55] | HCC tumor segmentation via 2D U-net from DCE-MRI dataset of 9 patients | n\a | 0.482 |
| Jansen et al., 2019 [56] | Liver segmentation via FCNN network from 6 SCE MR images and tumor detection via dual pathway FCNN from SCE and DW NRI images from 121 patients | 0.95 | n\a Sensitivity 99.8 |
| Bousabarahet al., 2020 [40] | Liver and HCC tumor segmentation via 3D U-net from multiphasic contrast-enhanced T1-weighted MRI dataset from 174 patients | 0.91 ± 0.01 | 0.68 ± 0.03 |
| Zhaoet al., 2021 [41] | HCC tumor and hemangioma segmentation via united adversarial learning framework UAL from multi modal contrast-enhances (T1-, T2-weighted and DWI) MRI images from 255 patients. | n\a | 83.63 ± 2.16 |
| Our method | Liver and CLRM tumor segmentation via HighResNet from a T1-weighted contrast-enhanced dataset of 80 MRI images | 0.958 ± 0.024 | 0.724 ± 0.130 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamkova, Y.; Pelanis, E.; Bjørnerud, A.; Edwin, B.; Elle, O.J.; Kumar, R.P. A Fast Method for Whole Liver- and Colorectal Liver Metastasis Segmentations from MRI Using 3D FCNN Networks. Appl. Sci. 2022, 12, 5145. https://doi.org/10.3390/app12105145
Kamkova Y, Pelanis E, Bjørnerud A, Edwin B, Elle OJ, Kumar RP. A Fast Method for Whole Liver- and Colorectal Liver Metastasis Segmentations from MRI Using 3D FCNN Networks. Applied Sciences. 2022; 12(10):5145. https://doi.org/10.3390/app12105145
Chicago/Turabian StyleKamkova, Yuliia, Egidijus Pelanis, Atle Bjørnerud, Bjørn Edwin, Ole Jakob Elle, and Rahul Prasanna Kumar. 2022. "A Fast Method for Whole Liver- and Colorectal Liver Metastasis Segmentations from MRI Using 3D FCNN Networks" Applied Sciences 12, no. 10: 5145. https://doi.org/10.3390/app12105145
APA StyleKamkova, Y., Pelanis, E., Bjørnerud, A., Edwin, B., Elle, O. J., & Kumar, R. P. (2022). A Fast Method for Whole Liver- and Colorectal Liver Metastasis Segmentations from MRI Using 3D FCNN Networks. Applied Sciences, 12(10), 5145. https://doi.org/10.3390/app12105145