
qEEG Analysis in the Diagnosis of Alzheimer’s Disease: A Comparison of Functional Connectivity and Spectral Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset and Preprocessing
2.2. Spectral Analysis
2.3. Functional Connectivity Analysis
2.3.1. Global Connectivity
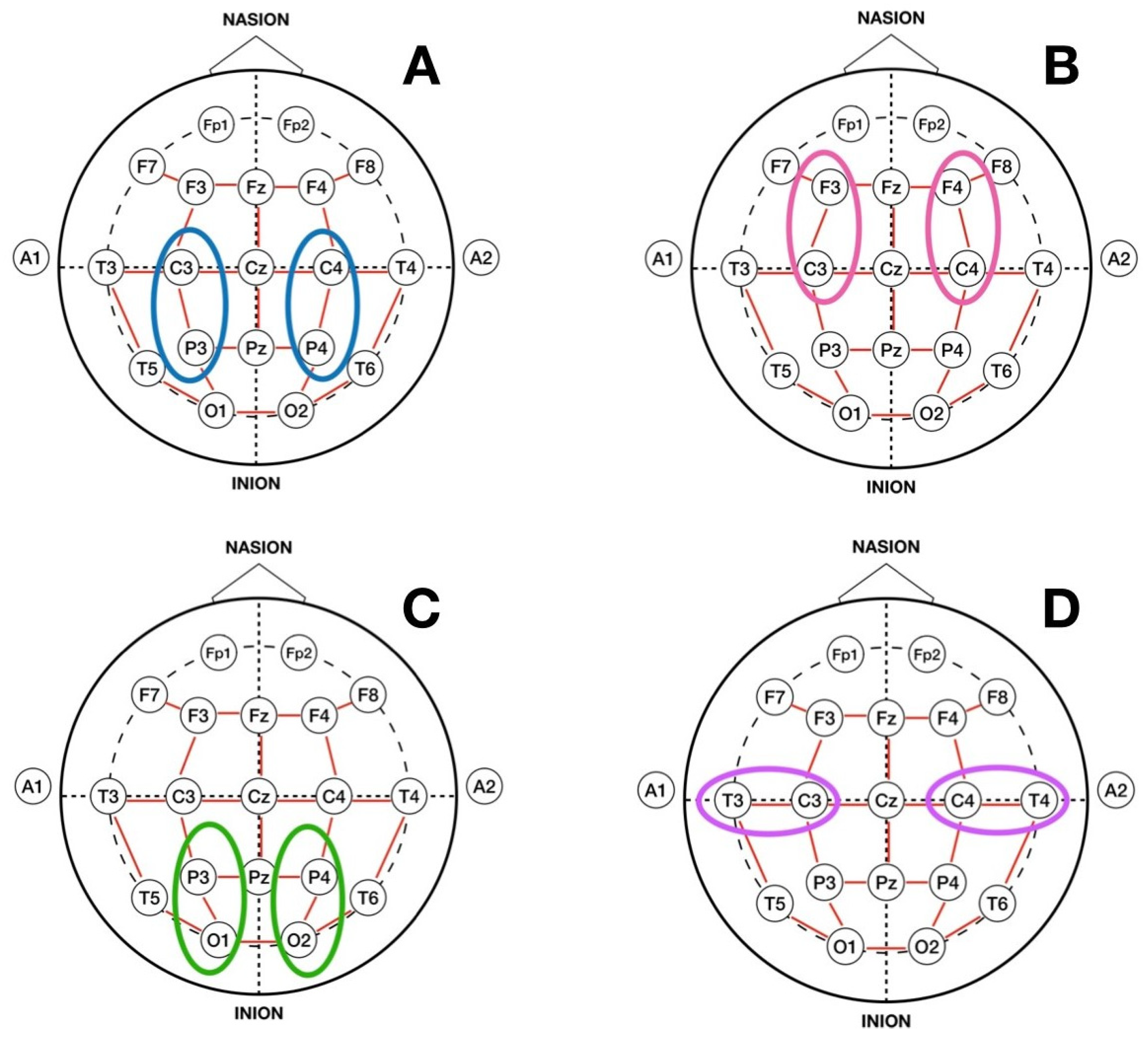
2.3.2. Homotopic Pair Connectivity
2.3.3. Localization of AD Using Homotopic Pair Connectivity
3. Results
3.1. Spectral Analysis
3.2. Functional Connectivity Analysis
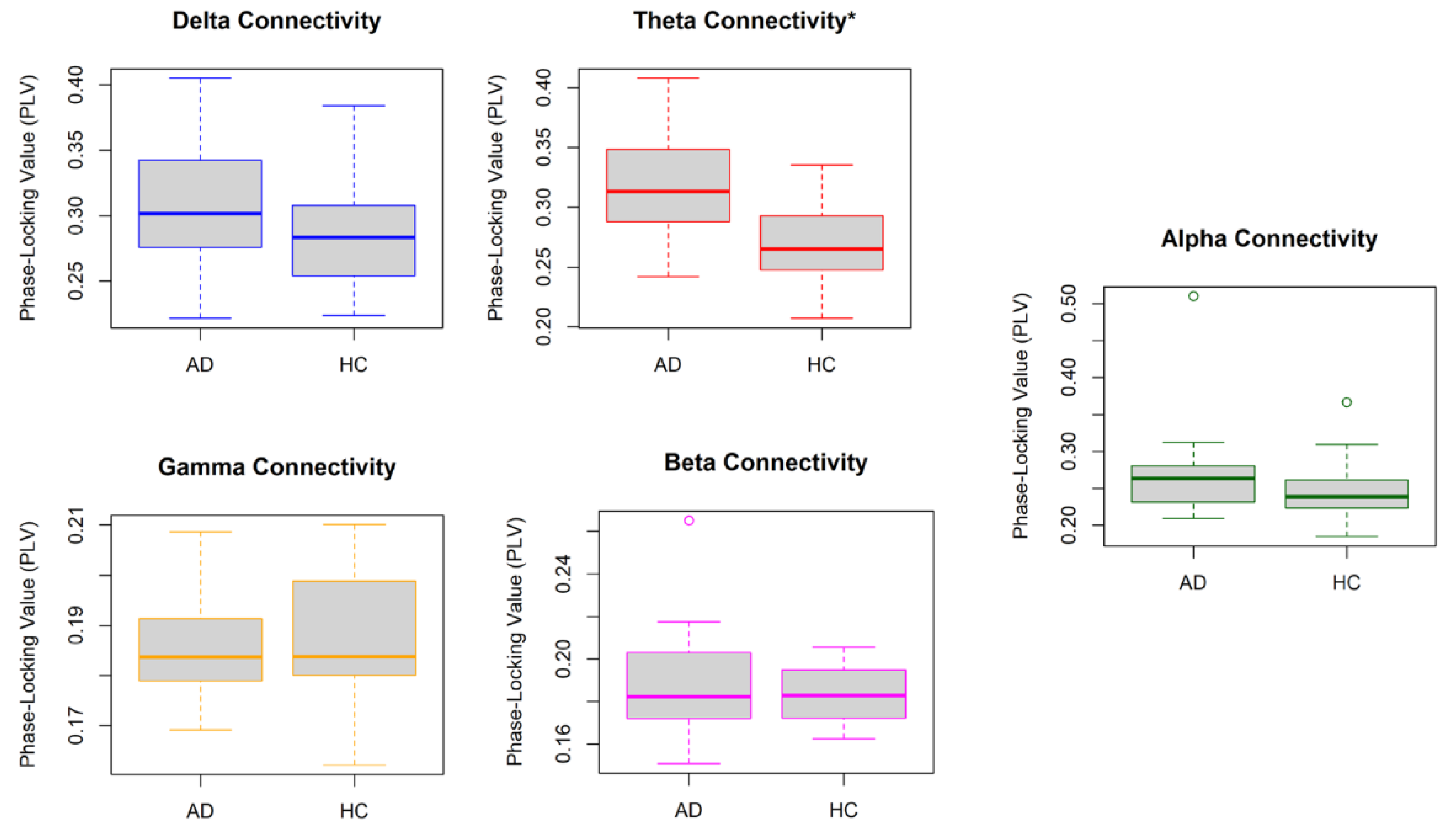
3.2.1. Global Connectivity
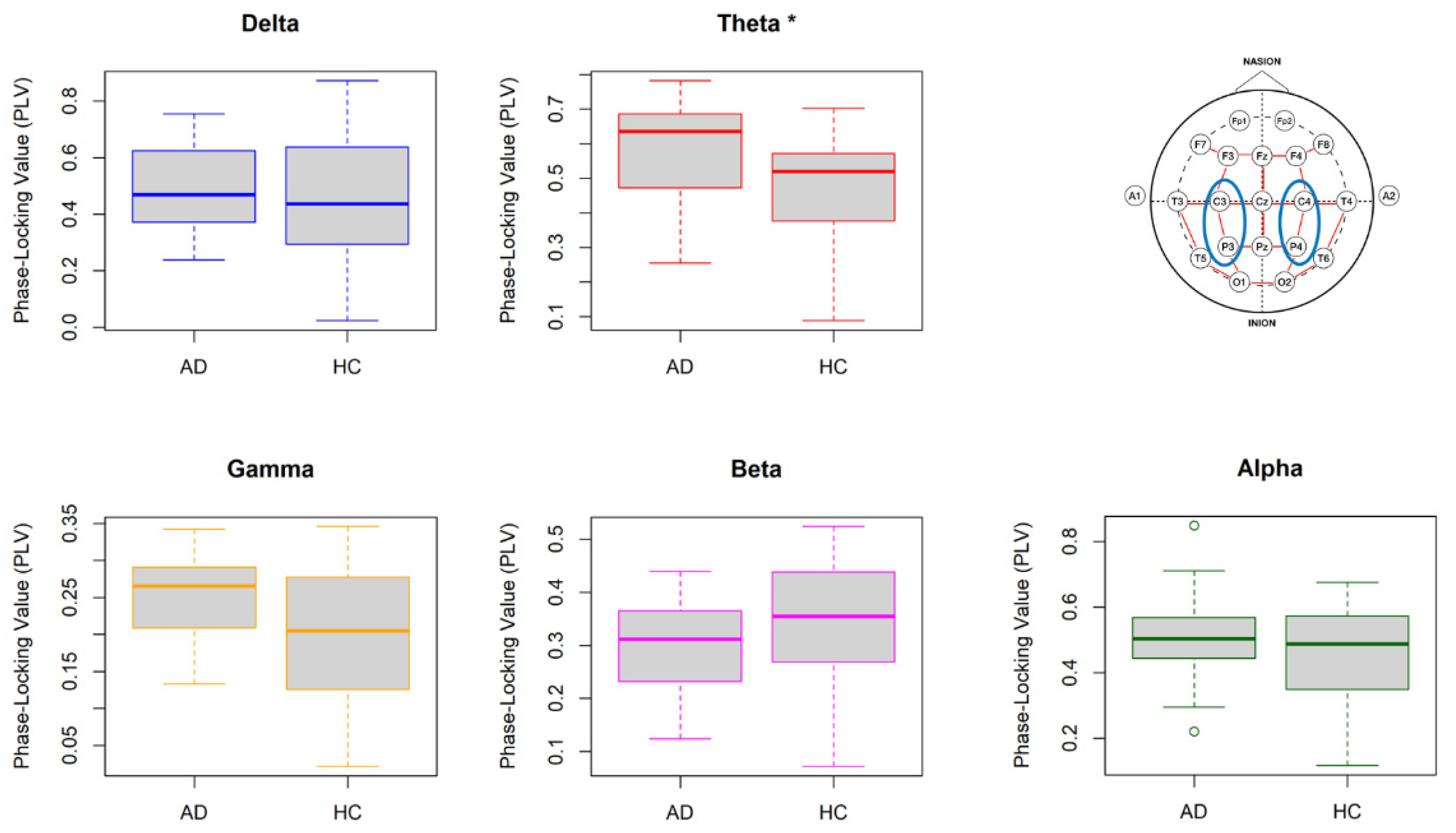
3.2.2. Homotopic Pair Connectivity
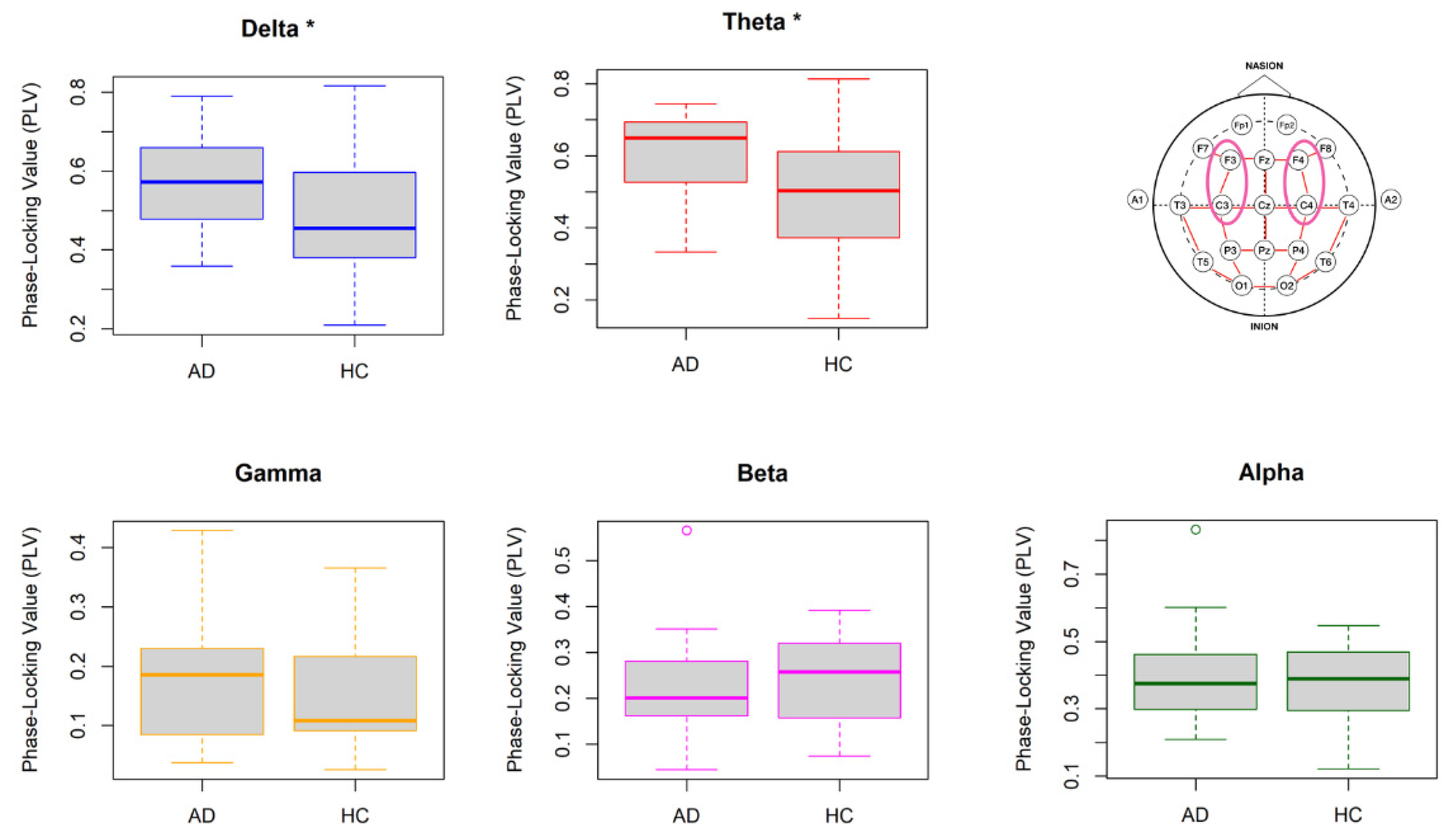
3.2.3. Localization of AD Using Homotopic Pair Connectivity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neto, E.; Allen, E.A.; Aurlien, H.; Nordby, H.; Eichele, T. EEG Spectral Features Discriminate between Alzheimer’s and Vascular Dementia. Front. Neurol. 2015, 6, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smailovic, U.; Jelic, V. Neurophysiological Markers of Alzheimer’s Disease: Quantitative EEG Approach. Neurol. Ther. 2019, 8 (Suppl. 2), 37–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Wang, J.; Yu, H.; Wei, X.; Yang, C.; Deng, B. Power Spectral Density and Coherence Analysis of Alzheimer’s EEG. Cogn. Neurodyn. 2015, 9, 291–304. [Google Scholar] [CrossRef]
- Heideman, M.; Johnson, D.; Burrus, C. Gauss and the History of the Fast Fourier Transform. IEEE ASSP Mag. 1984, 1, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Fraga, F.J.; Falk, T.H.; Kanda, P.A.M.; Anghinah, R. Characterizing Alzheimer’s Disease Severity via Resting-Awake EEG Amplitude Modulation Analysis. PLoS ONE 2013, 8, e72240. [Google Scholar] [CrossRef]
- Cassani, R.; Estarellas, M.; San-Martin, R.; Fraga, F.J.; Falk, T.H. Systematic Review on Resting-State EEG for Alzheimer’s Disease Diagnosis and Progression Assessment. Dis. Markers 2018, 2018, e5174815. [Google Scholar] [CrossRef] [Green Version]
- Hampel, H.; Lista, S.; Teipel, S.; Garaci, F.; Nisticò, R.; Blennow, K.; Zetterberg, H.; Bertram, L.; Duyckaerts, C.; Bakardjian, H.; et al. Perspective on Future Role of Biological Markers in Clinical Therapy Trials of Alzheimer’s Disease: A Long-Range Point of View beyond 2020. Biochem. Pharmacol. 2014, 88, 426–429. [Google Scholar] [CrossRef] [Green Version]
- Sperling, R.A.; Dickerson, B.C.; Pihlajamaki, M.; Vannini, P.; LaViolette, P.S.; Vitolo, O.V.; Hedden, T.; Becker, J.A.; Rentz, D.M.; Selkoe, D.J.; et al. Functional Alterations in Memory Networks in Early Alzheimer’s Disease. Neuromol. Med. 2010, 12, 27–43. [Google Scholar] [CrossRef] [Green Version]
- Al-Fahoum, A.S.; Al-Fraihat, A.A. Methods of EEG Signal Features Extraction Using Linear Analysis in Frequency and Time-Frequency Domains. ISRN Neurosci. 2014, 2014, 730218. [Google Scholar] [CrossRef] [Green Version]
- Arrufat-Pié, E.; Estévez-Báez, M.; Estévez-Carreras, J.M.; Machado-Curbelo, C.; Leisman, G.; Beltrán, C. Comparison between Traditional Fast Fourier Transform and Marginal Spectra Using the Hilbert–Huang Transform Method for the Broadband Spectral Analysis of the Electroencephalogram in Healthy Humans. Eng. Rep. 2021, 3, e12367. [Google Scholar] [CrossRef]
- Leuchter, A.F.; Cook, I.A.; Newton, T.F.; Dunkin, J.; Walter, D.O.; Rosenberg-Thompson, S.; Lachenbruch, P.A.; Weiner, H. Regional Differences in Brain Electrical Activity in Dementia: Use of Spectral Power and Spectral Ratio Measures. Electroencephalogr. Clin. Neurophysiol. 1993, 87, 385–393. [Google Scholar] [CrossRef]
- Hata, M.; Kazui, H.; Tanaka, T.; Ishii, R.; Canuet, L.; Pascual-Marqui, R.D.; Aoki, Y.; Ikeda, S.; Kanemoto, H.; Yoshiyama, K.; et al. Functional Connectivity Assessed by Resting State EEG Correlates with Cognitive Decline of Alzheimer’s Disease—An ELORETA Study. Clin. Neurophysiol. 2016, 127, 1269–1278. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, A.; Tangaro, S.; Bellotti, R.; Bertolino, A.; Blasi, G.; Pergola, G.; Taurisano, P.; Guaragnella, C. A Novel Synchronization-Based Approach for Functional Connectivity Analysis. Complexity 2017, 2017, e7190758. [Google Scholar] [CrossRef] [Green Version]
- Babiloni, C.; Lizio, R.; Marzano, N.; Capotosto, P.; Soricelli, A.; Triggiani, A.I.; Cordone, S.; Gesualdo, L.; Del Percio, C. Brain Neural Synchronization and Functional Coupling in Alzheimer’s Disease as Revealed by Resting State EEG Rhythms. Int. J. Psychophysiol. 2016, 103, 88–102. [Google Scholar] [CrossRef]
- Fell, J.; Axmacher, N. The Role of Phase Synchronization in Memory Processes. Nat. Rev. Neurosci. 2011, 12, 105–118. [Google Scholar] [CrossRef]
- Bastos, A.M.; Schoffelen, J.-M. A Tutorial Review of Functional Connectivity Analysis Methods and Their Interpretational Pitfalls. Front. Syst. Neurosci. 2015, 9, 175. [Google Scholar] [CrossRef] [Green Version]
- Cai, L.; Wei, X.; Wang, J.; Yu, H.; Deng, B.; Wang, R. Reconstruction of Functional Brain Network in Alzheimer’s Disease via Cross-Frequency Phase Synchronization. Neurocomputing 2018, 314, 490–500. [Google Scholar] [CrossRef]
- Lachaux, J.P.; Rodriguez, E.; Martinerie, J.; Varela, F.J. Measuring Phase Synchrony in Brain Signals. Hum. Brain Mapp. 1999, 8, 194–208. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; Gouw, A.A.; Hillebrand, A.; Tijms, B.M.; Stam, C.J.; van Straaten, E.C.W.; Pijnenburg, Y.A.L. Different Functional Connectivity and Network Topology in Behavioral Variant of Frontotemporal Dementia and Alzheimer’s Disease: An EEG Study. Neurobiol. Aging 2016, 42, 150–162. [Google Scholar] [CrossRef]
- Engels, M.M.A.; Stam, C.J.; van der Flier, W.M.; Scheltens, P.; de Waal, H.; van Straaten, E.C.W. Declining Functional Connectivity and Changing Hub Locations in Alzheimer’s Disease: An EEG Study. BMC Neurol. 2015, 15, 145. [Google Scholar] [CrossRef] [Green Version]
- Bruña, R.; Maestú, F.; Pereda, E. Phase Locking Value Revisited: Teaching New Tricks to an Old Dog. J. Neural Eng. 2018, 15, 056011. [Google Scholar] [CrossRef]
- Poza, J.; Bachiller, A.; Gomez, C.; Garcia, M.; Nunez, P.; Gomez-Pilar, J.; Tola-Arribas, M.A.; Cano, M.; Hornero, R. Phase-Amplitude Coupling Analysis of Spontaneous EEG Activity in Alzheimer’s Disease. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; Volume 2017, pp. 2259–2262. [Google Scholar] [CrossRef] [Green Version]
- Gallego-Jutgla, E.; Elgendi, M.; Vialatte, F.; Sole-Casals, J.; Cichocki, A.; Latchoumane, C.; Jeong, J.; Dauwels, J. Diagnosis of Alzheimer’s Disease from EEG by Means of Synchrony Measures in Optimized Frequency Bands. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 4266–4270. [Google Scholar] [CrossRef] [Green Version]
- Elgendi, M.; Vialatte, F.; Cichocki, A.; Latchoumane, C.; Jeong, J.; Dauwels, J. Optimization of EEG Frequency Bands for Improved Diagnosis of Alzheimer Disease. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 6087–6091. [Google Scholar] [CrossRef] [Green Version]
- Jasper, H. The Ten-Twenty Electrode System of the International Federation. Electroencephalogr. Clin. Neurophysiol. 1958, 10, 370–375. [Google Scholar]
- Rutkove, S.B. Introduction to Volume Conduction. In The Clinical Neurophysiology Primer; Humana Press: Totowa, NJ, USA, 2007; pp. 44–53. [Google Scholar]
- Blackburn, D.; Zhao, Y.; De Marco, M.; Bell, S.; He, F.; Wei, H.-L.; Lawrence, S.; Unwin, Z.; Blyth, M.; Angel, J.; et al. A Pilot Study Investigating a Novel Non-Linear Measure of Eyes Open versus Eyes Closed EEG Synchronization in People with Alzheimer’s Disease and Healthy Controls. Brain Sci. 2018, 8, 134. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.; Alimardani, M.; Hiraki, K. The Effect of Robot-Guided Meditation on Intra-Brain EEG Phase Synchronization. In Proceedings of the Companion of the 2021 ACM/IEEE International Conference on Human-Robot Interaction, Boulder, CO, USA, 8–11 March 2021; ACM: New York, NY, USA, 2021; pp. 318–322. [Google Scholar] [CrossRef]
- Leeuwis, N.; Yoon, S.; Alimardani, M. Functional Connectivity Analysis in Motor-Imagery Brain Computer Interfaces. Front. Hum. Neurosci. 2021, 15, 732946. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhao, Y.; Durongbhan, P.; Chen, L.; Liu, J.; Billings, S.A.; Zis, P.; Unwin, Z.C.; De Marco, M.; Venneri, A.; et al. Imaging of Nonlinear and Dynamic Functional Brain Connectivity Based on EEG Recordings With the Application on the Diagnosis of Alzheimer’s Disease. IEEE Trans. Med. Imaging 2020, 39, 1571–1581. [Google Scholar] [CrossRef]
- Durongbhan, P.; Zhao, Y.; Chen, L.; Zis, P.; De Marco, M.; Unwin, Z.C.; Venneri, A.; He, X.; Li, S.; Zhao, Y.; et al. A Dementia Classification Framework Using Frequency and Time-Frequency Features Based on EEG Signals. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 826–835. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using Lme4. J. Stat. Soft. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Acharya, J.N.; Acharya, V.J. Overview of EEG Montages and Principles of Localization. J. Clin. Neurophysiol. 2019, 36, 325–329. [Google Scholar] [CrossRef]
- Trongnetrpunya, A.; Nandi, B.; Kang, D.; Kocsis, B.; Schroeder, C.E.; Ding, M. Assessing Granger Causality in Electrophysiological Data: Removing the Adverse Effects of Common Signals via Bipolar Derivations. Front. Syst. Neurosci. 2016, 9, 189. [Google Scholar] [CrossRef] [Green Version]
- Rossini, P.M.; Di Iorio, R.; Vecchio, F.; Anfossi, M.; Babiloni, C.; Bozzali, M.; Bruni, A.C.; Cappa, S.F.; Escudero, J.; Fraga, F.J.; et al. Early Diagnosis of Alzheimer’s Disease: The Role of Biomarkers Including Advanced EEG Signal Analysis. Report from the IFCN-Sponsored Panel of Experts. Clin. Neurophysiol. 2020, 131, 1287–1310. [Google Scholar] [CrossRef]
- Sankari, Z.; Adeli, H.; Adeli, A. Intrahemispheric, Interhemispheric, and Distal EEG Coherence in Alzheimer’s Disease. Clin. Neurophysiol. 2011, 122, 897–906. [Google Scholar] [CrossRef]
- Yin, Z.; Li, J.; Zhang, Y.; Ren, A.; Von Meneen, K.M.; Huang, L. Functional Brain Network Analysis of Schizophrenic Patients with Positive and Negative Syndrome Based on Mutual Information of EEG Time Series. Biomed. Signal Process. Control 2017, 31, 331–338. [Google Scholar] [CrossRef]
- Quraan, M.A.; McCormick, C.; Cohn, M.; Valiante, T.A.; McAndrews, M.P. Altered Resting State Brain Dynamics in Temporal Lobe Epilepsy Can Be Observed in Spectral Power, Functional Connectivity and Graph Theory Metrics. PLoS ONE 2013, 8, e68609. [Google Scholar] [CrossRef] [Green Version]
- Adeli, H.; Ghosh-Dastidar, S.; Dadmehr, N. A Spatio-Temporal Wavelet-Chaos Methodology for EEG-Based Diagnosis of Alzheimer’s Disease. Neurosci. Lett. 2008, 444, 190–194. [Google Scholar] [CrossRef]
- Deng, B.; Cai, L.; Li, S.; Wang, R.; Yu, H.; Chen, Y.; Wang, J. Multivariate Multi-Scale Weighted Permutation Entropy Analysis of EEG Complexity for Alzheimer’s Disease. Cogn. Neurodyn. 2017, 11, 217–231. [Google Scholar] [CrossRef]
- Krajcovicova, L.; Marecek, R.; Mikl, M.; Rektorova, I. Disruption of Resting Functional Connectivity in Alzheimer’s Patients and At-Risk Subjects. Curr. Neurol. Neurosci. Rep. 2014, 14, 491. [Google Scholar] [CrossRef]
- Bari Antor, M.; Jamil, A.H.M.S.; Mamtaz, M.; Monirujjaman Khan, M.; Aljahdali, S.; Kaur, M.; Singh, P.; Masud, M. A Comparative Analysis of Machine Learning Algorithms to Predict Alzheimer’s Disease. J. Healthc. Eng. 2021, 2021, e9917919. [Google Scholar] [CrossRef]
- Liu, L.; Zhao, S.; Chen, H.; Wang, A. A New Machine Learning Method for Identifying Alzheimer’s Disease. Simul. Model. Pract. Theory 2020, 99, 102023. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AD | HC | |
|---|---|---|
| Size | N = 20 | N = 20 |
| Age | 60 (SD = 4.40) | 61 (SD = 6.67) |
| Gender (F/M) | 8/12 | 12/8 |
| Homotopic Pair | Delta Band (1–4 Hz) | Theta Band (4–8 Hz) |
|---|---|---|
| A | ✘ | √ |
| B | ✘ | ✘ |
| C | ✘ | ✘ |
| D | ✘ | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frangopoulou, M.S.; Alimardani, M. qEEG Analysis in the Diagnosis of Alzheimer’s Disease: A Comparison of Functional Connectivity and Spectral Analysis. Appl. Sci. 2022, 12, 5162. https://doi.org/10.3390/app12105162
Frangopoulou MS, Alimardani M. qEEG Analysis in the Diagnosis of Alzheimer’s Disease: A Comparison of Functional Connectivity and Spectral Analysis. Applied Sciences. 2022; 12(10):5162. https://doi.org/10.3390/app12105162
Chicago/Turabian StyleFrangopoulou, Maria Semeli, and Maryam Alimardani. 2022. "qEEG Analysis in the Diagnosis of Alzheimer’s Disease: A Comparison of Functional Connectivity and Spectral Analysis" Applied Sciences 12, no. 10: 5162. https://doi.org/10.3390/app12105162
APA StyleFrangopoulou, M. S., & Alimardani, M. (2022). qEEG Analysis in the Diagnosis of Alzheimer’s Disease: A Comparison of Functional Connectivity and Spectral Analysis. Applied Sciences, 12(10), 5162. https://doi.org/10.3390/app12105162