
Quantitative Assessment Methods of Early Enamel Caries with Optical Coherence Tomography: A Review

Abstract
:1. Introduction
2. Optical Properties of Teeth
- (1)
- Refractive Index
- (2)
- Scattering Properties
- (3)
- Absorption Properties
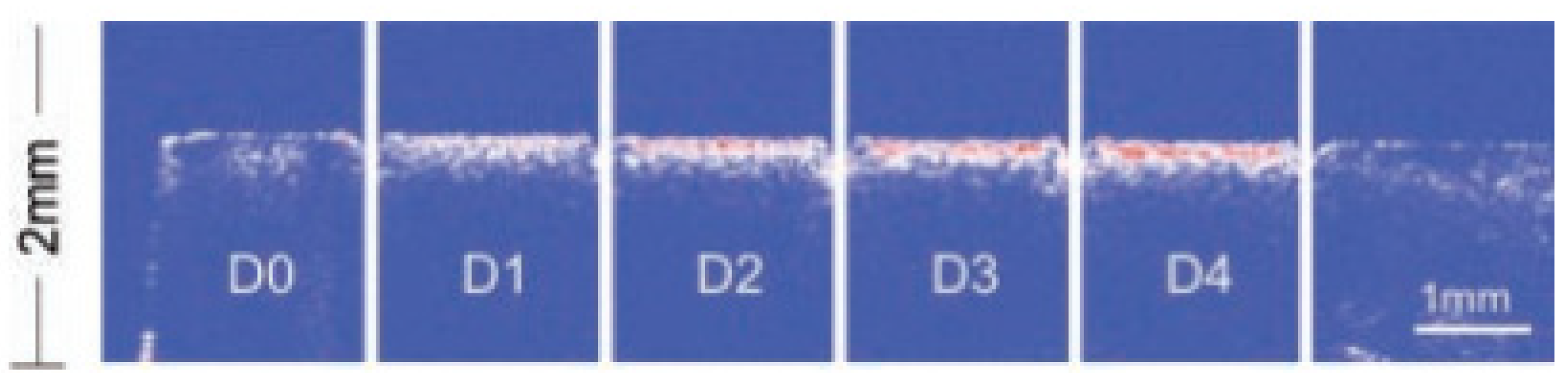
3. Preparation of Artificial Carious Lesions
4. Quantitative Assessment Methods of Early Enamel Caries with OCT
4.1. Quantitative Assessment Based on Lesion Depths
4.2. Quantitative Assessment Based on Reflectivity
4.3. Quantitative Assessment Based on Attenuation Coefficient
4.4. Quantitative Assessment Based on Degree of Polarization
4.5. Quantitative Assessment Based on Refractive Index
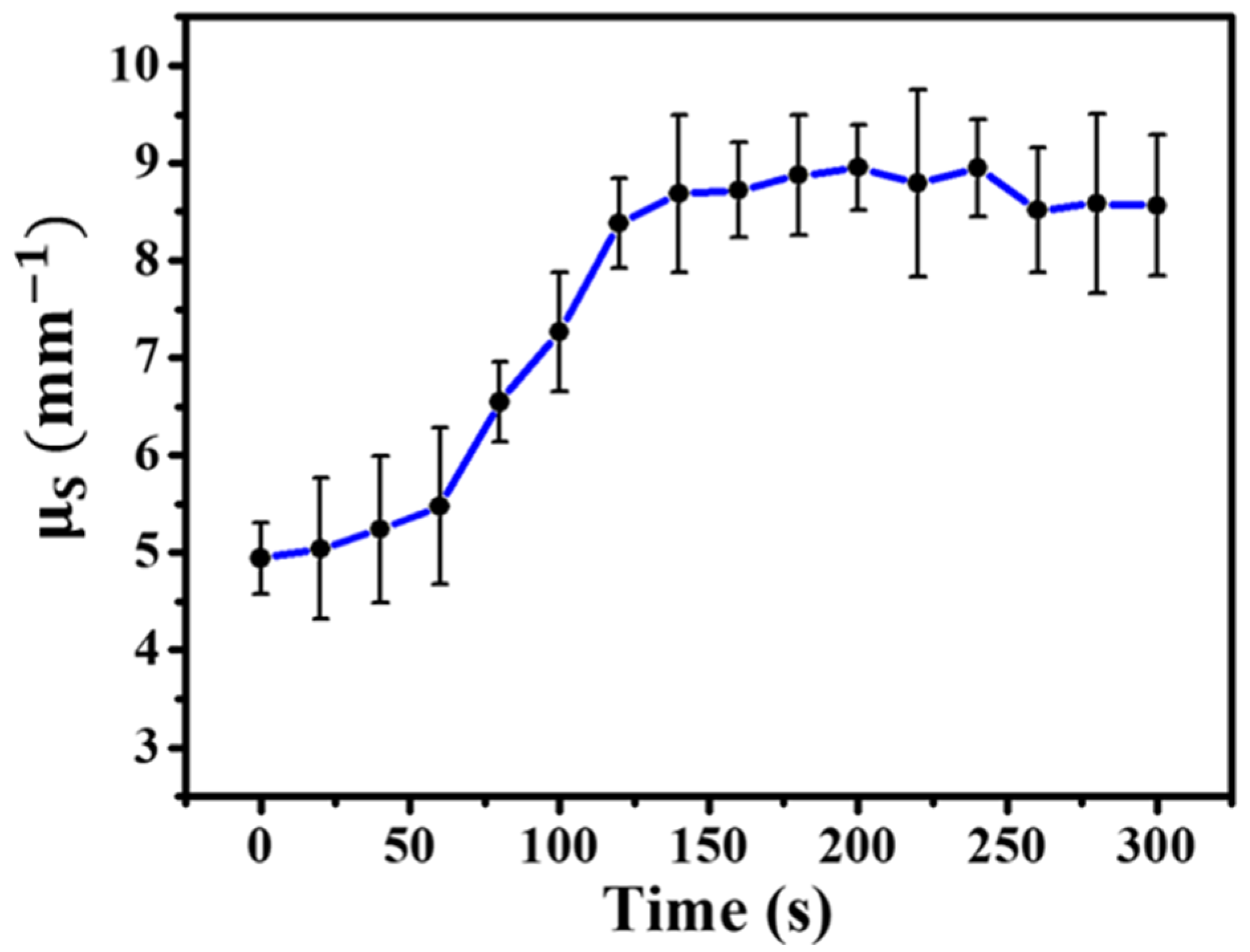
4.6. Quantitative Assessment Based on Scattering Coefficient
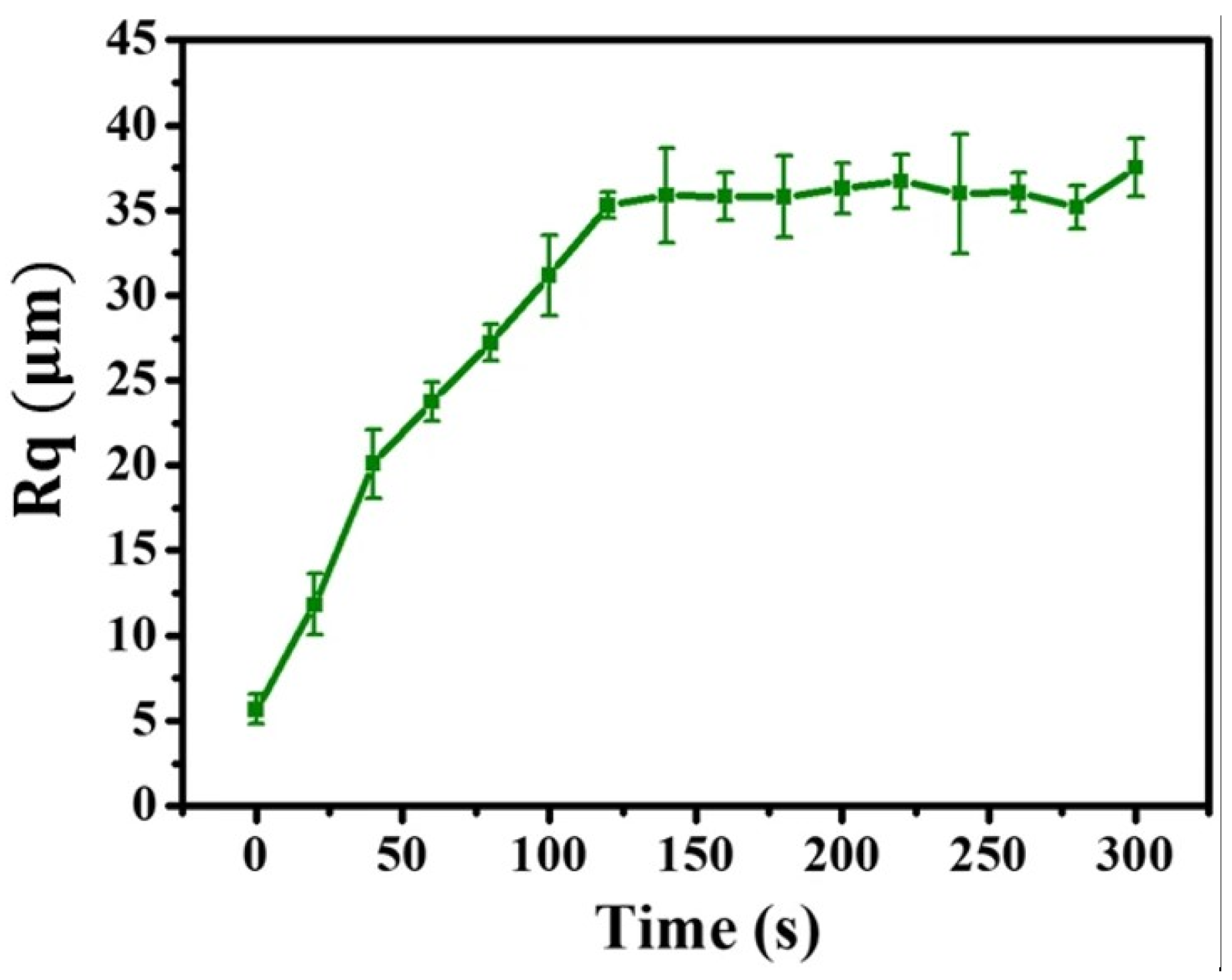
4.7. Quantitative Assessment Based on the Surface Roughness of Enamel
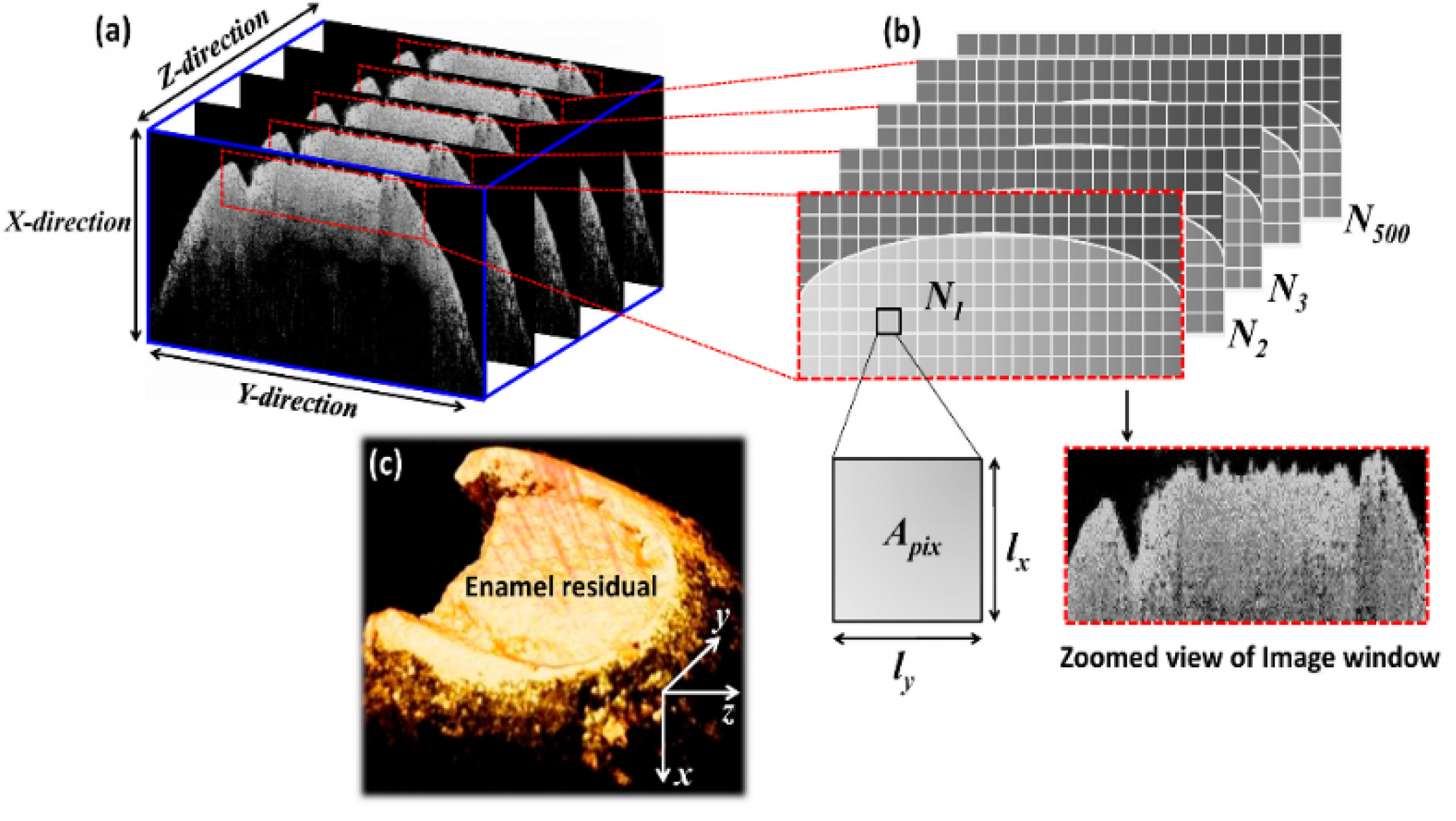
4.8. Quantitative Assessment Based on the Volume of Residual Enamel
4.9. Quantitative Assessment Based on the Dehydration Parameter
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baelum, V.; Fejerskov, O. Caries diagnosis: A mental resting place on the way to intervention. In Dental Caries–The Disease and Its Clinical Management; Blackwell Munksgaard: London, UK, 2003; pp. 101–110. [Google Scholar]
- Dirks, O.B. Posteruptive Changes in Dental Enamel. J. Dent. Res. 1966, 45, 503–511. [Google Scholar] [CrossRef]
- Tenbosch, J.J.; Verdonschot, E.H.; Vaarkamp. Light propagation through teeth containing simulated caries lesions. Phys. Med. Biol. 1995, 40, 1375–1387. [Google Scholar]
- Schneider, H.; Ahrens, M.; Strumpski, M.; Rüger, C.; Häfer, M.; Hüttmann, G.; Theisen-Kunde, D.; Schulz-Hildebrandt, H.; Haak, R. An Intraoral OCT Probe to Enhanced Detection of Approximal Carious Lesions and Assessment of Restorations. J. Clin. Med. 2020, 9, 3257. [Google Scholar] [CrossRef] [PubMed]
- Schneider, H.; Park, K.J.; Häfer, M.; Rüger, C.; Schmalz, G.; Krause, F.; Schmidt, J.; Ziebolz, D.; Haak, R. Dental Applications of Optical Coherence Tomography (OCT) in Cariology. Appl. Sci. 2017, 7, 472. [Google Scholar] [CrossRef]
- Brouwer, F.; Askar, H.; Paris, S.; Schwendicke, F. Detecting Secondary Caries Lesions: A Systematic Review and Meta-analysis. J. Dent. Res. 2016, 95, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.S.; Huynh, G.D.; Jones, G.C.; Fried, D. Near-infrared transillumination at 1310-nm for the imaging of early dental decay. Opt. Exp. 2003, 11, 2259–2265. [Google Scholar] [CrossRef]
- Schaefer, G.; Pitchika, V.; Litzenburger, L.; Hickel, R.; Kühnisch, J. Evaluation of occlusal caries detection and assessment by visual inspection, digital bitewing radiography and near-infrared light transillumination. Clin. Oral Investig. 2018, 22, 2431–2438. [Google Scholar] [CrossRef]
- Alammari, M.R.; Smith, P.W.; De Josselin De Jong, E.; Higham, S.M. Quantitative light-induced fluorescence (QLF): A tool for early occlusal dental caries detection and supporting decision making in vivo. J. Dent. 2013, 41, 127–132. [Google Scholar] [CrossRef]
- Gomez, J. Detection and diagnosis of the early caries lesion. BMC Oral Health 2015, 15, 3. [Google Scholar] [CrossRef]
- Abogazalah, N.; Ando, M. Alternative methods to visual and radiographic examinations for approximal caries detection. J. Oral Sci. 2017, 59, 315–322. [Google Scholar] [CrossRef]
- Pretty, I.A. Caries detection and diagnosis: Novel technologies. J. Dent. 2006, 34, 727–739. [Google Scholar] [CrossRef]
- Patil, C.A.; Bosschaart, N.; Keller, M.D.; Leeuwen, T.G.; Mahadevan-Jansen, A. Combined Raman spectroscopy and optical coherence tomography device for tissue characterization. Opt. Lett. 2008, 33, 1135–1137. [Google Scholar] [CrossRef] [PubMed]
- Qiao, W.; Chen, Z. All-optically integrated photoacoustic and optical coherence tomography: A review. J. Innov. Opt. Health Sci. 2017, 10, 1730006. [Google Scholar] [CrossRef]
- Tearney, G.J.; Brezinski, M.E.; Bouma, B.E.; Boppart, S.A.; Pitvis, C.; Southern, J.F.; Fujimoto, J.G. In vivo endoscopic optical biopsy with optical coherence tomography. Science 1997, 276, 2037–2039. [Google Scholar] [CrossRef]
- Hangai, M.; Ojima, Y.; Gotoh, N.; Inoue, R.; Yasuno, Y.; Makita, S.; Yamanari, M.; Yatagai, T.; Kita, M.; Yoshimura, N. Three-dimensional Imaging of Macular Holes with High-speed Optical Coherence Tomography. Ophthalmology 2007, 114, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Yasuno, Y.; Hong, Y.; Makita, S. In vivo high-contrast imaging of deep posterior eye by 1-μm swept source optical coherence tomography and scattering optical coherence angiography. Opt. Exp. 2007, 15, 6121–6139. [Google Scholar] [CrossRef]
- Baumgartner, A.; Dichtl, S.; Hitzenberger, C.K.; Sattmann, H.; Robl, B.; Moritz, A.; Fercher, A.F.; Sperr, W. Polarization–Sensitive Optical Coherence Tomography of Dental Structures. Caries Res. 2000, 14, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Colston, B.W.; Sathyam, U.S.; DaSilva, L.B.; Everett, M.J.; Stroeve, P.; Otis, L.L. Dental OCT. Opt. Exp. 1998, 3, 230–238. [Google Scholar] [CrossRef]
- Pagnoni, A.; Knuettel, A.; Welker, P.; Rist, M.; Stoudemayer, T.; Kolbe, L.; Sadiq, I.; Kligman, A.M. Optical coherence tomography in dermatology. Skin Res. Technol. 1999, 5, 83–87. [Google Scholar] [CrossRef]
- Pierce, M.C.; Strasswimmer, J.; Park, H.; Cense, B.; Boer, J.F. Birefringence measurements in human skin using polarization-sensitive optical coherence tomography. J. Biomed. Opt. 2004, 9, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.A.; Poneros, J.M.; Bouma, B.E.; Bressner, J.; Halpern, E.F.; Shishkov, M.; Lauwers, G.Y.; Kenudson, M.M.; Nishioka, N.S.; Tearney, G.J. Optical coherence tomography to identify intramucosal carcinoma and high-grade dysplasia in Barrett’s esophagus. Clin. Gastroenterol. Hepatol. 2006, 4, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Poneros, J.M.; Brand, S.; Bouma, B.E.; Tearney, G.J.; Compton, C.C.; Nishioka, N.S. Diagnosis of Specialized Intestinal Metaplasia by Optical Coherence Tomography. Gastroenterology 2001, 51, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Shang, J.; Liu, C.; Zhang, J.; Hou, F.; Liang, Y. Intraoperative imaging of oral-maxillofacial lesions using optical coherence tomography. J. Innov. Opt. Health Sci. 2020, 13, 2050011. [Google Scholar] [CrossRef]
- Na, J.; Baek, J.H.; Choi, E.S.; Ryu, S.Y.; Chang, J.; Lee, C.S.; Lee, B.H. Assessment of dental-caries using optical coherence tomography. Int. Soc. Opt. Eng. SPIE 2006, 6137, 18–27. [Google Scholar]
- Na, J.; Baek, J.H.; Ryu, S.Y.; Lee, C.; Lee, B.H. Tomographic imaging of incipient dental-caries using optical coherence tomography and comparison with various modalities. Opt. Rev. 2009, 16, 426–431. [Google Scholar] [CrossRef]
- Holtzman, J.S.; Osann, K.; Pharar, J. Ability of Optical Coherence Tomography to Detect Caries Beneath Commonly Used Dental Sealants. Lasers Surg. Med. 2010, 42, 752–759. [Google Scholar] [CrossRef]
- Shimada, Y.; Sadr, A.; Burrow, M.F.; Tagami, J.; Ozawa, N.; Sumi, Y. Validation of swept-source optical coherence tomography (SS-OCT) for the diagnosis of occlusal caries. J. Dent. 2010, 38, 655–665. [Google Scholar] [CrossRef]
- Darling, C.L.; Huynh, G.; Fried, D. Light scattering properties of natural and artificially demineralized dental enamel at 1310 nm. J. Biomed. Opt. 2006, 11, 034023. [Google Scholar] [CrossRef]
- Ohmi, M.; Ohnishi, Y.; Yoden, K.; Haruna, M. In vitro simultaneous measurement of refractive index and thickness of biological tissue by the low coherence interferometry. IEEE Trans. Biomed. Eng. 2000, 47, 1266–1270. [Google Scholar] [CrossRef]
- Wang, X.J.; Milner, T.E.; Boer, J.F.d.; Zhang, Y.; Pashley, D.H.; Nelson, J.S. Characterization of dentin and enamel by use of optical coherence tomography. Appl. Opt. 1999, 38, 2092–2096. [Google Scholar] [CrossRef]
- Besic, F.C.; Wiemann, M.R. Dispersion Staining, Dispersion, and Refractive Indices in Early Enamel Caries. J. Dent. Res. 1972, 51, 973–985. [Google Scholar] [CrossRef]
- Knuettel, A.R.; Bonev, S.M.; Knaak, W. New method for evaluation of in vivo scattering and refractive index properties obtained with optical coherence tomography. J. Biomed. Opt. 2004, 9, 265–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, D.; Glena, R.E.; Featherstone, J.D.B.; Seka, W. Nature of light scattering in dental enamel and dentin at visible and near-infrared wavelengths. Appl. Opt. 1995, 34, 1278–1285. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Fried, D. Attenuation of 1310-nm and 1550-nm laser light through sound dental enamel. Lasers Dent. VIII 2002, 4610, 187–190. [Google Scholar]
- Spitzer, D.; Bosch, J.T. The absorption and scattering of light in bovine and human dental enamel. Calcif. Tiss. Res. 1975, 17, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Chan, A.C.; Darling, C.L.; Fried, D. Methods for Monitoring Erosion Using Optical Coherence Tomography. Lasers Dent. XIX 2013, 8566, 35–40. [Google Scholar]
- Lee, C.; Darling, C.L.; Fried, D. Polarization-sensitive optical coherence tomographic imaging of artificial demineralization on exposed surfaces of tooth roots. Dent. Mater. 2009, 25, 721–728. [Google Scholar] [CrossRef]
- Şen, S.; Erber, R.; Deurer, N.; Orhan, G.; Lux, C.J.; Zingler, S. Demineralization Detection in Orthodontics Using an Ophthalmic Optical Coherence Tomography Device Equipped with a Multicolor Fluorescence Module. Clin. Oral Investig. 2020, 24, 2579–2590. [Google Scholar] [CrossRef]
- Azevedo, C.S.; Trung, L.C.E.; Simionato, M.R.L.; Freitas, A.Z.; Matos, A.B. Evaluation of caries-affected dentin with optical coherence tomography. Braz. Oral Res. 2011, 25, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.Z.; Zezell, D.M.; Mayer, M.P.A.; Ribeiro, A.C.; Gomes, A.S.L.; Jr., N.D.V. Determination of dental decay rates with optical coherence tomography. Laser Phys. Lett. 2009, 6, 896–900. [Google Scholar] [CrossRef]
- Espigares, J.; Sadr, A.; Hamba, H.; Shimada, Y.; Otsuki, M.; Tagami, J.; Sumi, Y. Assessment of natural enamel lesions with optical coherence tomography in comparison with microfocus X-ray computed tomography. J. Med. Imag. 2015, 2, 014001. [Google Scholar] [CrossRef] [PubMed]
- Hee, M.R. Optical Coherence Tomography of the Human Retina. Arch. Ophthalmol. 1995, 113, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, K.; Sasaki, K.; Makita, S.; Yamanari, M.; Cense, B.; Yasuno, Y. Simultaneous high-resolution retinal imaging and high-penetration choroidal imaging by one-micrometer adaptive optics optical coherence tomography. Opt. Exp. 2010, 18, 8515–8527. [Google Scholar] [CrossRef]
- Boer, J.F.; Milner, T.E.; Gemert, M.J.; Nelson, J.S. Two-dimensional birefringence imaging in biological tissue by polarization-sensitive optical coherence tomography. Opt. Lett. 1997, 22, 934–936. [Google Scholar] [CrossRef] [Green Version]
- Saxer, C.E.; Boer, J.F.; Hyle Park, B.H.; Zhao, Y.; Chen, Z.; Nelson, J.S. High-speed fiber-based polarization-sensitive optical coherence tomography of in vivo human skin. Opt. Lett. 2000, 25, 1355–1357. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Tom, H.; Lee, R.C.; Kang, H.; Simon, J.C.; Staninec, M.; Darling, C.L.; Pelzner, R.B.; Fried, D. Clinical monitoring of smooth surface enamel lesions using CP-OCT during nonsurgical intervention. Lasers Surg. Med. 2016, 48, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Otis, L.; Piao, D.; Zhu, Q. Characterization of dentin, enamel, and carious lesions by a polarization-sensitive optical coherence tomography system. Appl. Opt. 2005, 44, 2041–2048. [Google Scholar] [CrossRef]
- Le, M.H.; Darling, C.L.; Fried, D. Automated analysis of lesion depth and integrated reflectivity in PS-OCT scans of tooth demineralization. Lasers Surg. Med. 2010, 42, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.S.; Darling, C.L.; Featherstone, J.D.B.; Fried, D. Imaging Artificial Caries on the Occlusal Surfaces with Polarization-Sensitive Optical Coherence Tomography. Caries Res. 2006, 40, 81–89. [Google Scholar] [CrossRef]
- Meng, Z.; Yao, X.; Yao, H.; Liu, T.; Li, Y.; Wang, G. Detecting early artificial caries by using optical coherence tomography. Chin. J. Lasers 2010, 37, 2709–2713. [Google Scholar] [CrossRef]
- Yao, H.; Li, Y.; Wang, G.; Yao, X.; Meng, Z.; Jin, S.; Liang, Y.; Zhang, L.; Liu, T. Quantification detecting artificial early caries with an All-fiber-OCT system. Int. J. Biomed. Eng. 2009, 37, 65–69+66. [Google Scholar]
- Park, K.J.; Schneider, H.; Ziebolz, D.; Krause, F.; Haak, R. Optical coherence tomography to evaluate variance in the extent of carious lesions in depth. Lasers Med. Sci. 2018, 33, 1573–1579. [Google Scholar] [CrossRef]
- Yavuz, B.S.; Kargul, B. Comparative evaluation of the spectral-domain optical coherence tomography and microhardness for remineralization of enamel caries lesions. Dent. Mater. J. 2021, 40, 1115–1121. [Google Scholar] [CrossRef] [PubMed]
- Can, A.M.; Darling, C.L.; Ho, C.; Fried, D. Non-destructive assessment of inhibition of demineralization in dental enamel irradiated by a λ = 9.3-μm CO2 laser at ablative irradiation intensities with PS-OCT. Lasers Surg. Med. 2008, 40, 342–349. [Google Scholar] [CrossRef]
- Staninec, M.; Douglas, S.M.; Darling, C.L.; Chan, K.; Kang, H.; Lee, R.C.; Fried, D. Non-destructive clinical assessment of occlusal caries lesions using near-IR imaging methods. Lasers Surg. Med. 2011, 43, 951–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, R.S.; Fried, D. Remineralization of Enamel Caries Can Decrease Optical Reflectivity. J. Dent. Res. 2006, 85, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.S.; Darling, C.L.; Featherstone, J.D.B.; Fried, D. Remineralization of in vitro dental caries assessed with polarization-sensitive optical coherence tomography. J. Biomed. Opt. 2006, 11, 014016. [Google Scholar] [CrossRef] [PubMed]
- Nee, A.; Chan, K.; Kang, H.; Staninec, M.; Darling, C.L.; Fried, D. Longitudinal monitoring of demineralization peripheral to orthodontic brackets using cross polarization optical coherence tomography. J. Dent. 2014, 42, 547–555. [Google Scholar] [CrossRef]
- Kang, H.; Darling, C.L.; Fried, D. Nondestructive monitoring of the repair of enamel artificial lesions by an acidic remineralization model using polarization-sensitive optical coherence tomography. Dent. Mater. 2012, 28, 488–494. [Google Scholar] [CrossRef]
- Amaechi, B.T.; Higham, S.M.; Podoleanu, A.G.; Rogers, J.A.; Jackson, D.A. Use of optical coherence tomography for assessment of dental caries: Quantitative procedure. J. Oral Rehabil. 2001, 28, 1092–1093. [Google Scholar] [CrossRef]
- Amaechi, B.T.; Podoleanu, A.; Komarov, G.; Higham, S.M.; Jackson, D.A. Optical coherence tomography for dental caries detection and analysis. Lasers Dent. VIII 2002, 4610, 100–108. [Google Scholar]
- Amaechi, B.T.; Podoleanu, A.G.; Higham, S.M.; Jackson, D.A. Correlation of quantitative light-induced fluorescence and optical coherence tomography applied for detection and quantification of early dental caries. J. Biomed. Opt. 2003, 8, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Jones, R.S. Evaluating a novel fissure caries model using swept source optical coherence tomography. Dent. Mater. J. 2013, 32, 906–912. [Google Scholar] [CrossRef]
- Sowa, M.G.; Popescu, D.P.; Werner, J.; Hewko, M.; Ko, A.C.T.; Payette, J.; Dong, C.C.S.; Cleghorn, B.; Choo-Smith, L.P. Precision of Raman depolarization and optical attenuation measurements of sound tooth enamel. Anal. Bioanal. Chem. 2007, 387, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Mandurah, M.; Sadr, A.; Shimada, Y.; Kitasako, Y.; Nakashima, S.; Bakhsh, T.A.; Tagami, J.; Sumi, Y. Monitoring remineralization of enamel subsurface lesions by optical coherence tomography. J. Biomed. Opt. 2013, 18, 046006. [Google Scholar] [CrossRef]
- Featherstone, J.D.B.; Cate, J.M.; Shariati, M.; Arends, J. Comparison of artificial caries-like lesions by quantitative microradiography and microhardness profiles. Caries Res. 1983, 17, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Maia, A.M.A.; Freitas, A.Z.; Campello, S.; Gomes, A.S.L.; Karlsson, L. Evaluation of dental enamel caries assessment using quantitative light induced fluorescence and optical coherence tomography. J. Biophotonics 2016, 9, 596–602. [Google Scholar] [CrossRef]
- Cara, A.C.B.; Zezell, D.M.; Ana, P.A.; Maldonado, E.P.; Freitas, A.Z. Evaluation of two quantitative analysis methods of optical coherence tomography for detection of enamel demineralization and comparison with microhardness. Lasers Surg. Med. 2014, 46, 666–671. [Google Scholar] [CrossRef]
- Popescu, D.P.; Sowa, M.G.; Hewko, M.D.; Choo-Smith, L.P. Assessment of early demineralization in teeth using the signal attenuation in optical coherence tomography images. J. Biomed. Opt. 2008, 13, 054053. [Google Scholar] [CrossRef]
- Sowa, M.G.; Popescu, D.P.; Friesen, J.R.; Hewko, M.D.; Choo-Smith, L.-P. A comparison of methods using optical coherence tomography to detect demineralized regions in teeth. J. Biophotonics 2011, 4, 814–823. [Google Scholar] [CrossRef]
- Darling, C.L.; Fried, D. Polarized light propagation through sound and carious enamel at 1310-nm. Proc. SPIE–Int. Soc. Opt. Eng. 2006, 6137, 151–158. [Google Scholar]
- Everett, M.J.; Colston, B.W.; Sathyam, U.S.; Silva, L.B.; Fried, D.; Featherstone, J.D. Noninvasive diagnosis of early caries with polarization-sensitive optical coherence tomography (PS-OCT). Lasers Dent. V SPIE 2022, 3593, 177–182. [Google Scholar]
- Golde, J.; Tetschke, F.; Walther, J.; Rosenauer, T.; Hempel, F.; Hannig, C.; Koch, E.; Kirsten, L. Detection of carious lesions utilizing depolarization imaging by polarization sensitive optical coherence tomography. J. Biomed. Opt. 2018, 23, 071201–071208. [Google Scholar] [CrossRef] [PubMed]
- Götzinger, E.; Pircher, M.; Geitzenauer, W.; Ahlers, C.; Baumann, B.; Michels, S.; Schmidt-Erfurth, U.; Hitzenberger, C.K. Retinal pigment epithelium segmentation by polarization sensitive optical coherence tomography. Opt. Exp. 2008, 16, 16410–16422. [Google Scholar] [CrossRef]
- Golde, J.; Tetschke, F.; Vosahlo, R.; Walther, J.; Hannig, C.; Koch, E.; Kirsten, L. Assessment of occlusal enamel alterations utilizing depolarization imaging based on PS-OCT. Biomed. Opt. Imag. SPIE 2019, 11078, 11078_24. [Google Scholar]
- Tetschke, F.; Golde, J.; Rosenauer, T.; Basche, S.; Walther, J.; Kirsten, L.; Koch, E.; Hannig, C. Correlation between Lesion Progression and Depolarization Assessed by Polarization-Sensitive Optical Coherence Tomography. Appl. Sci. 2020, 10, 2971. [Google Scholar] [CrossRef]
- Meng, Z.; Yao, X.; Yao, H.; Liang, Y.; Liu, T.; Li, Y.; Wang, G. Measurement of the refractive index of human teeth by optical coherence tomography. J. Biomed. Opt. 2009, 14, 034010. [Google Scholar] [CrossRef]
- Hariri, I.; Sadr, A.; Shimada, Y.; Nakashima, S.; Sumi, Y.; Tagami, J. Relationship between Refractive Index and Mineral Content of Enamel and Dentin Using SS-OCT and TMR. Lasers Dent. XVIII 2012, 8208, 117–122. [Google Scholar]
- Hariri, I.; Sadr, A.; Nakashima, S.; Shimada, Y.; Tagami, J.; Sumi, Y. Estimation of the Enamel and Dentin Mineral Content from the Refractive Index. Caries Res. 2013, 47, 18–26. [Google Scholar] [CrossRef]
- Tsai, M.T.; Wang, Y.L.; Yeh, T.W.; Lee, H.C.; Chen, W.J.; Ke, J.L.; Lee, Y.J. Early detection of enamel demineralization by optical coherence tomography. Sci. Rep. 2019, 9, 17154. [Google Scholar] [CrossRef] [Green Version]
- Wijesinghe, R.E.; Cho, N.H.; Park, K.; Jeon, M.; Kim, J. Bio-Photonic Detection and Quantitative Evaluation Method for the Progression of Dental Caries Using Optical Frequency-Domain Imaging Method. Sensors 2016, 16, 2076. [Google Scholar] [CrossRef] [PubMed]
- Natsume, Y.; Nakashima, S.; Sadr, A. Estimation of lesion progress in artificial root caries by swept source optical coherence tomography in comparison to transverse microradiography. J. Biomed. Opt. 2011, 16, 071408. [Google Scholar] [CrossRef] [PubMed]
- Shimamura, Y.; Murayama, R.; Kurokawa, H.; Miyazaki, M.; Mihata, Y.; Kmaguchi, S. Influence of tooth-surface hydration conditions on optical coherence-tomography imaging. J. Dent. 2011, 39, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Nazari, A.; Sadr, A.; Funollet, M.C.; Nakashima, S.; Shimada, Y.; Tagami, J.; Sumi, Y. Effect of hydration on assessment of early enamel lesion using swept-source optical coherence tomography. J. Biophotonics 2012, 6, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Won, J.; Huang, P.C.; Spillman, D.R.; Chaney, E.J.; Adam, R.; Klukowska, M.; Barkalifa, R.; Boppart, S.A. Handheld optical coherence tomography for clinical assessment of dental plaque and gingiva. J. Biomed. Opt. 2020, 25, 116011. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | OCT System | Sample Preparation | Lesion Depth Result |
|---|---|---|---|
| Le et al. [49] | . | Sample number: 10 bovine enamel blocks for in vitro detection | |
| Solution: pH 4.8 demineralization solution | |||
| Method: 5 windows for each block, demineralization for 0–4 days, respectively. | |||
| Jones et al. [50] | . | Sample number: 15 human posterior teeth for in vitro detection | |
| Solution: pH 4.3 demineralization solution and pH 7.0 remineralization solution | |||
| Method: occlusal areas were exposed to 14-day pH cycling, which consisted of 6 h demineralization and 17 h remineralization a day. | |||
| Meng et al. [51] | . | Sample number: 6 human isolated teeth for in vitro detection | is demineralization time. |
| Method: demineralization for 12, 24, 48, 72, 96 and 120 h. | |||
| Yao et al. [52] | . | Sample number: 7 human permanent teeth for in vitro detection | is demineralization time. |
| Solution: PH 4.5 demineralization solution | |||
| Method: demineralization for 12, 24, 48, 72, 96, 120 h. | |||
| Park et al. [53] | , imaging speed 16 kHz. | 13 human molars, 25 human incisors, 11 premolars and 15 molars for ex vivo detection, 18 patients for in vivo detection. | Vary considerably within each ICDAS category using OCT. |
| , imaging speed 48–91 kHz, handheld scanning probe (Non-intraoral probe). | |||
| Yavuz et al. [54] | . | Sample number: 40 human enamel blocks | Reduction in lesion depth after remineralization for three remineralization agents: |
| Solution: PH 4.8 demineralization solution and PH 7.0 remineralization solution | |||
| Method: 3 windows for each block, with one window demineralized for 3 days and one window remineralized for 6 days by PH cycling. | |||
| Can et al. [55] | . | Sample number: 15 bovine enamel blocks for in vitro detection | |
| Solution: pH 4.9 demineralization solution | |||
| Method: 3 windows for each block, demineralization for 9 days | |||
| Jones et al. [57] | . | Sample number: 20 human posterior teeth for in vitro detection | . |
| Solution: pH 4.9 demineralization solution and pH 7.0 remineralization solution | |||
| Method: demineralization for 9 days and remineralization for 20 days. |
| Reference | OCT System | Sample Preparation | |
|---|---|---|---|
| Le et al. [49] | 1310-nm PS-OCT, axial/lateral. | Sample number: 10 bovine enamel blocks for in vitro detection | for the fixed depth algorithm: 100–770 for the edge detection algorithm: 20–500 |
| Solution: pH 4.8 demineralization solution | |||
| Method: 5 windows for each block, demineralization for 0–4 days, respectively. | |||
| Jones et al. [50] | . | Sample number: 15 human posterior teeth for in vitro detection | : 450 ± 110 |
| Solution: pH 4.3 demineralization solution and pH 7.0 remineralization solution | |||
| Method: occlusal areas were exposed to 14-day PH cycling, which consisted of 6 h demineralization and 17 h remineralization a day. | |||
| Nee et al. [59] | , body/imaging tip of the handpiece 7 × 18 cm/1.5 × 4 cm, 6 × 6 × 7 mm volume imaging time 3 s. | Sample number: Two teeth in 20 patients for in vivo detection | : 10.2 (10.5)–29.7 (9.4) |
| Solution: two types of adhesives | |||
| Method: The adhesives were used to bond the brackets. Demineralization around orthodontic brackets was detected every 3 months for one year. | |||
| Kang et al. [60] | . | Sample number: 10 bovine enamel blocks for in vitro detection | for 8 days demineralization: 257 ± 60.2 for 4, 8, 12 days remineralization: 236 ± 73.8, 206 ± 96.0, 168 ± 58.5 |
| Solution: pH 4.6 demineralization solution and pH 4.8 remineralization solution | |||
| Method: 6 windows for each block, demineralization for 8 days and remineralization for three 4-day periods | |||
| Amaechi et al. [61] | 850-nm TD-OCT. | Sample number: 15 bovine teeth for in vitro detection | for 1 to 3 days: 54.0 ± 11.27, 71.87 ± 4.79, 86.64 ± 7.57 |
| Solution: pH 4.5 demineralization solution | |||
| Method: demineralization for 3 days | |||
| Amaechi et al. [63] | . | Sample number: 15 bovine incisor teeth for in vitro detection | Reflectivity of demineralization for 0, 24, 48, 72 h: 31.86 ± 9.30, 14.45 ± 5.47, 8.66 ± 1.96, 4.32 ± 2.72 |
| Solution: pH 4.5 demineralization solution | |||
| Method: 3 windows for each teeth. Demineralization for 24, 48, 72 h, respectively. |
| Reference | OCT System | Sample Preparation | Attenuation Coefficient Result |
|---|---|---|---|
| Mandurah et al. [66] | , sweep rate 20 kHz. | Sample number: 24 bovine enamel blocks for in vitro detection | (mean). |
| Solution: pH 4.6 demineralization solution and two types of remineralization solution | |||
| Method: 3 windows for each block, demineralization for 14 days and remineralization for 14 days. | |||
| Maia et al. [68] | . | Sample number: 5 human premolar teeth for in vitro detection | Attenuation coefficient increase: 27.8–62.5% |
| Solution: pH 5.0 demineralization solution | |||
| Method: demineralization for 9 days. | |||
| Cara et al. [69] | . | Sample number: 40 third molars for in vitro detection | 0.93 sensitivity, 0.96 specificity |
| Solution: pH 4.3 demineralization solution and pH 7.4 remineralization solution | |||
| Method: four groups performed 0–21 days pH cycling, consisting of 3 h demineralization and 20 h remineralization a day. | |||
| Popescu et al. [70] | . | 21 human molars and premolars for in vitro detection |
| Reference | OCT System | Sample Preparation | DOPU Result |
|---|---|---|---|
| Golde et al. [74] | , sweep rate 50 kHz. | 3 human molar teeth with different proximal lesions | The significant DOPU contrast provided better identification of lesions in comparison with the reflectivity images. |
| Tetschke et al. [77] | , sweep rate 50 kHz. | Sample number: 18 bovine enamel blocks for in vitro detection | 0.6–0.97 |
| Solution: pH 4.95 demineralization solution | |||
| Method: demineralization for 49 days. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, B.; Niu, J.; Zhou, X.; Dong, X. Quantitative Assessment Methods of Early Enamel Caries with Optical Coherence Tomography: A Review. Appl. Sci. 2022, 12, 8780. https://doi.org/10.3390/app12178780
Shi B, Niu J, Zhou X, Dong X. Quantitative Assessment Methods of Early Enamel Caries with Optical Coherence Tomography: A Review. Applied Sciences. 2022; 12(17):8780. https://doi.org/10.3390/app12178780
Chicago/Turabian StyleShi, Boya, Jiaxin Niu, Xinyue Zhou, and Xiaoyang Dong. 2022. "Quantitative Assessment Methods of Early Enamel Caries with Optical Coherence Tomography: A Review" Applied Sciences 12, no. 17: 8780. https://doi.org/10.3390/app12178780
APA StyleShi, B., Niu, J., Zhou, X., & Dong, X. (2022). Quantitative Assessment Methods of Early Enamel Caries with Optical Coherence Tomography: A Review. Applied Sciences, 12(17), 8780. https://doi.org/10.3390/app12178780