


Topology Optimization of Patient-Specific Custom-Fit Distal Tibia Plate: A Spiral Distal Tibia Bone Fracture


Abstract
:1. Introduction
2. Materials and Methods
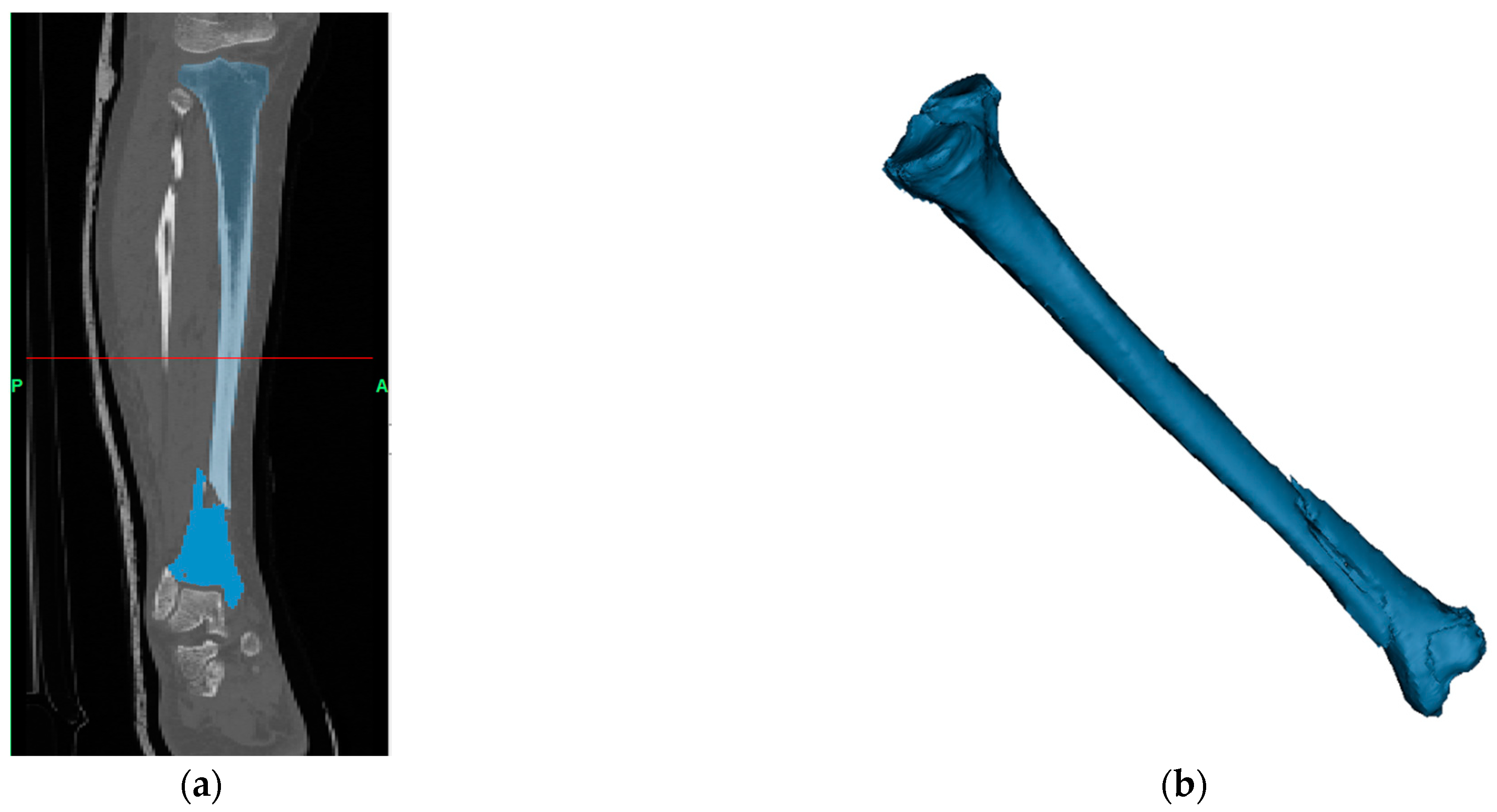
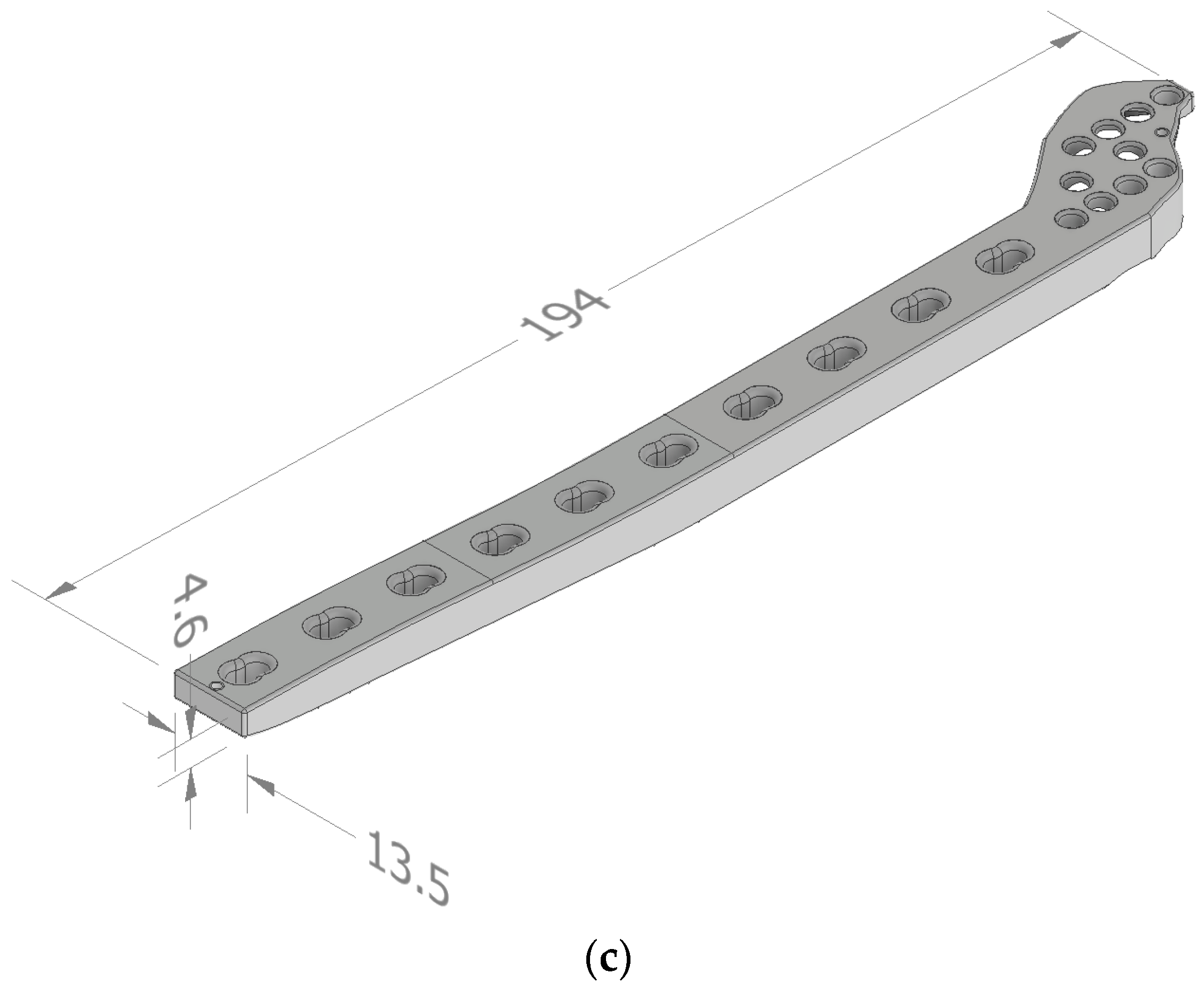
2.1. Patient Bone Fracture Model and Plate Design
2.2. Plate Topology Optimization
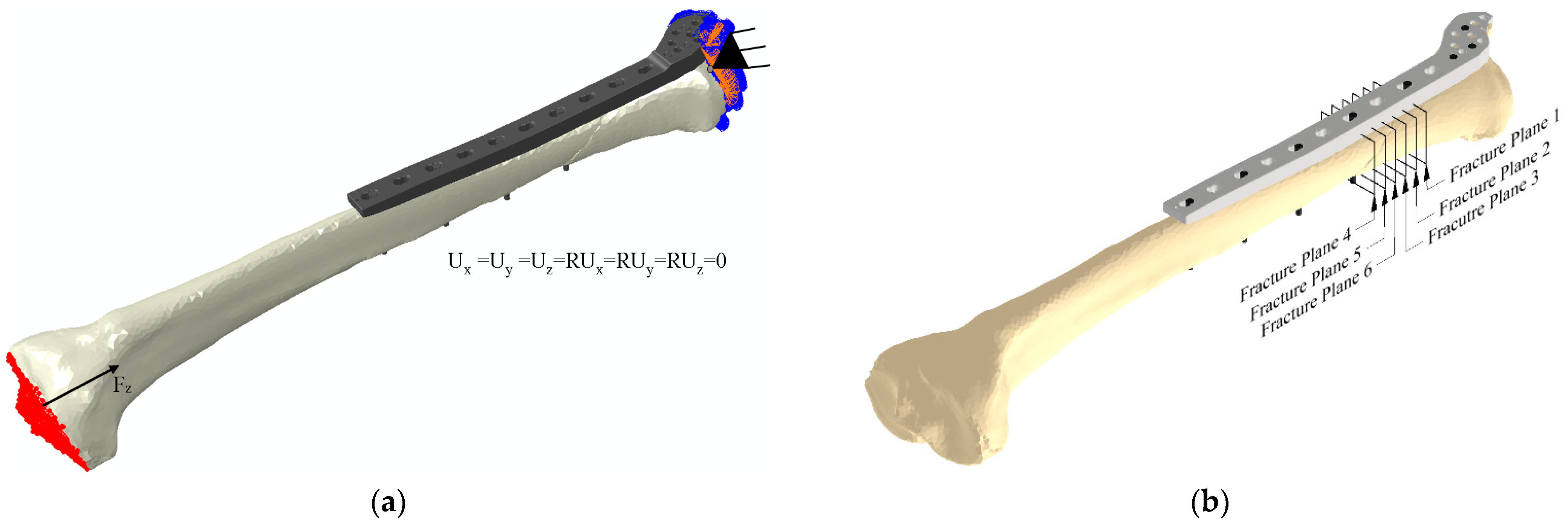
2.2.1. Finite Element Procedure
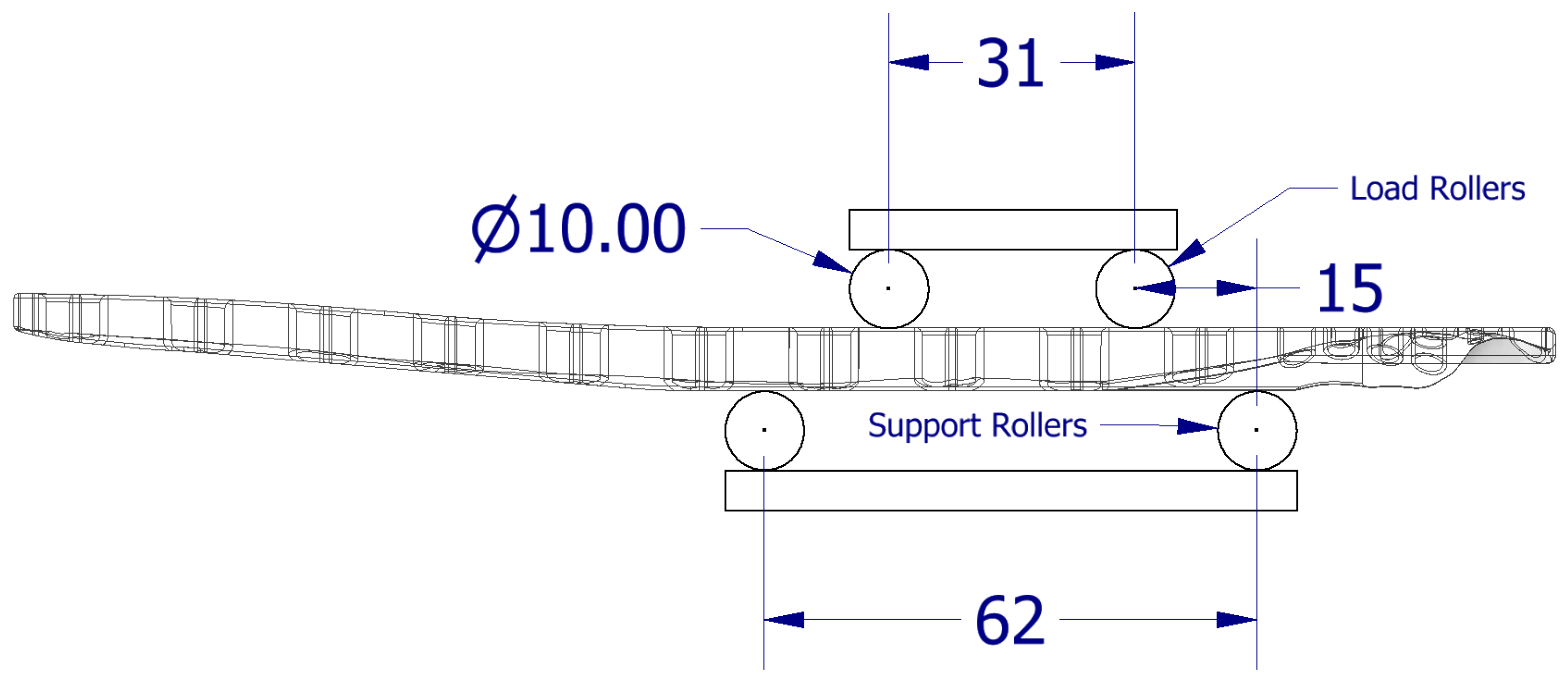
2.3. Bone Plate Stiffness Analysis
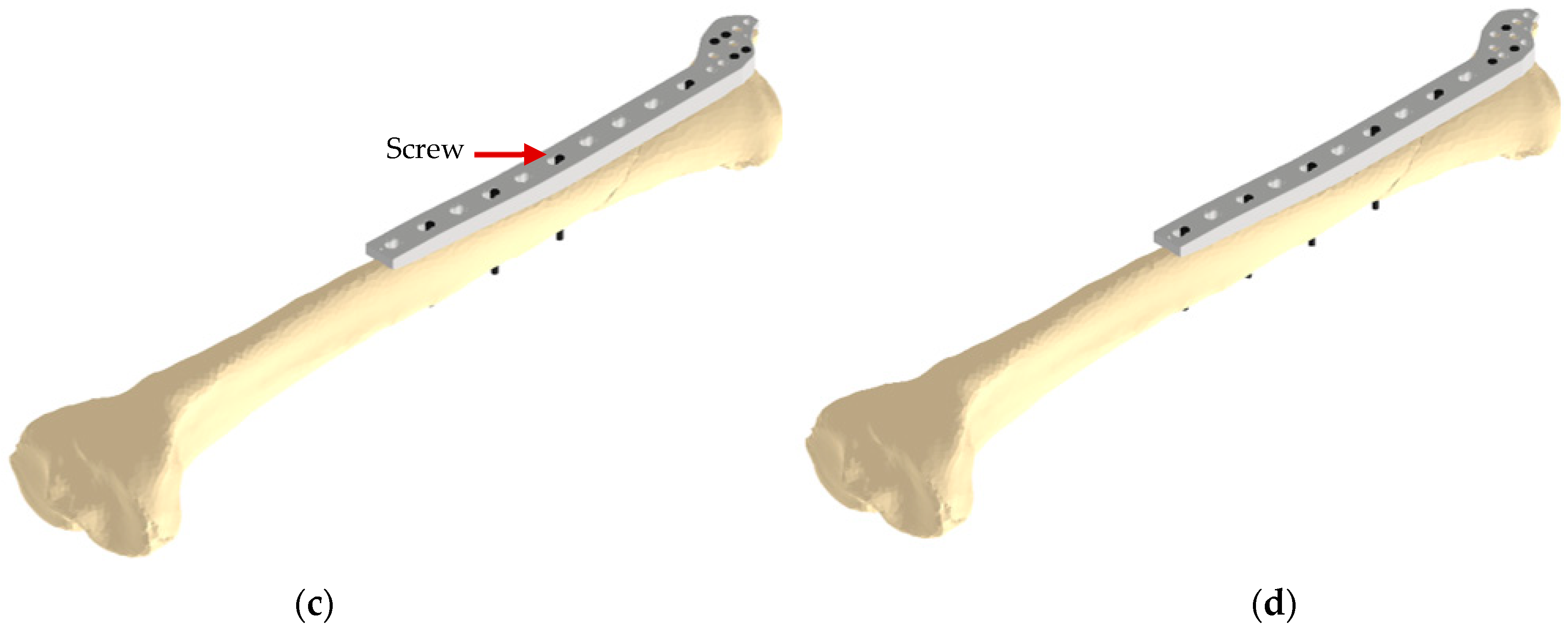
2.4. Stress Analysis of a Bone-Implant Model
2.5. The 3D Printing of the Plate Prototype
3. Results and Discussion
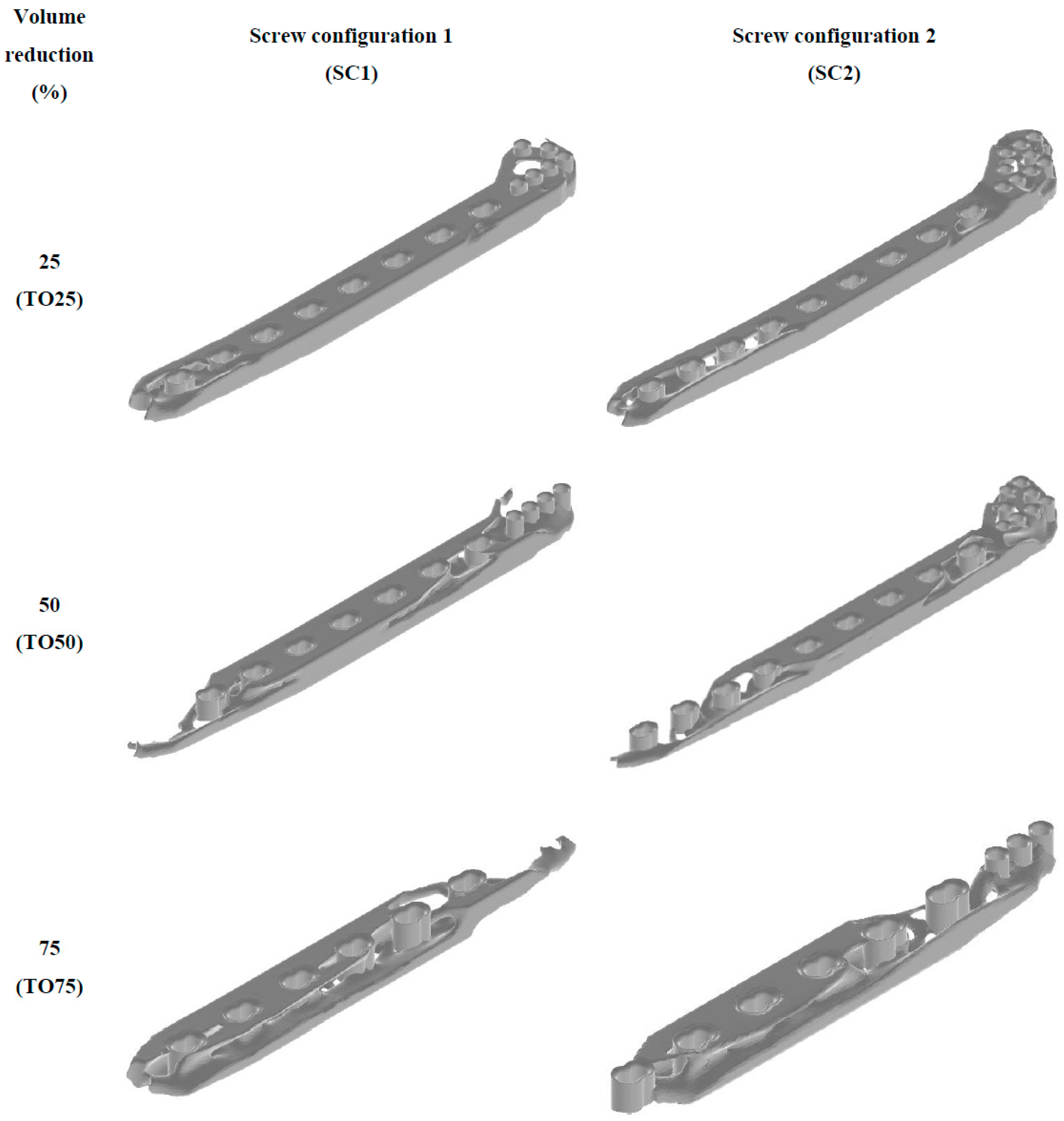
3.1. Topology Optimization of Bone Plate
3.2. Plate Mechanical Stiffness
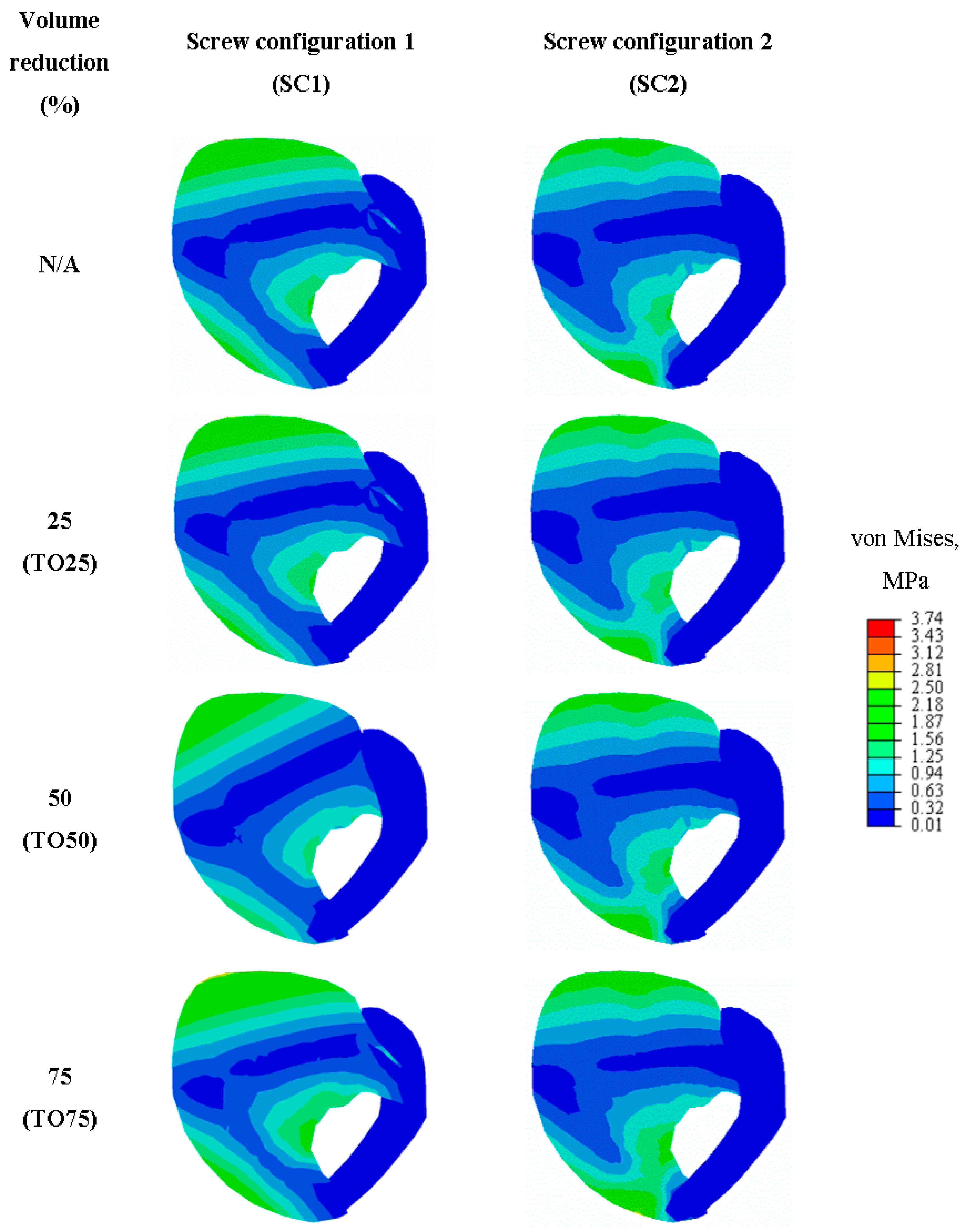
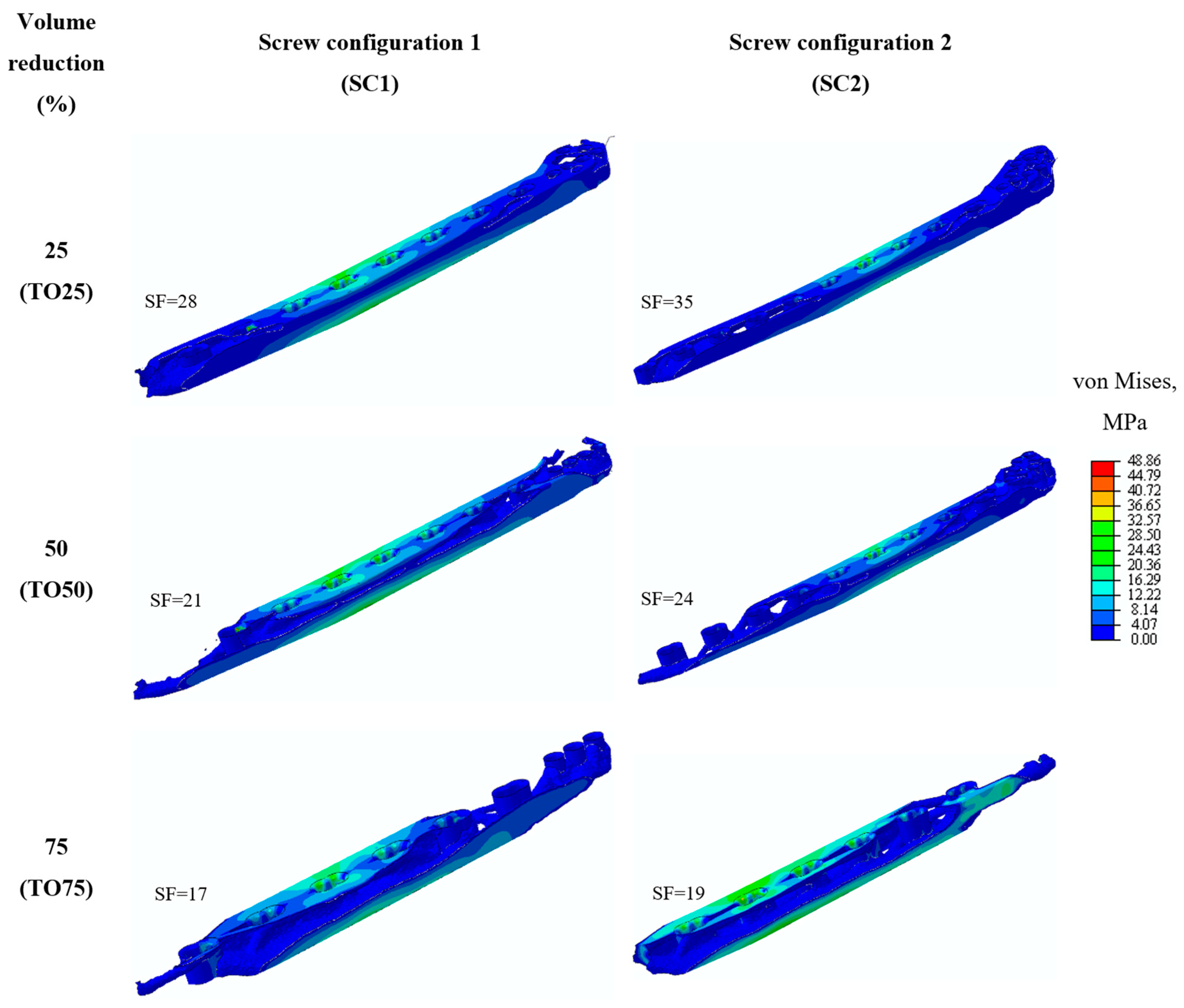
3.3. Biomechanical Stress Analysis
3.4. Plate Mechanical Stability
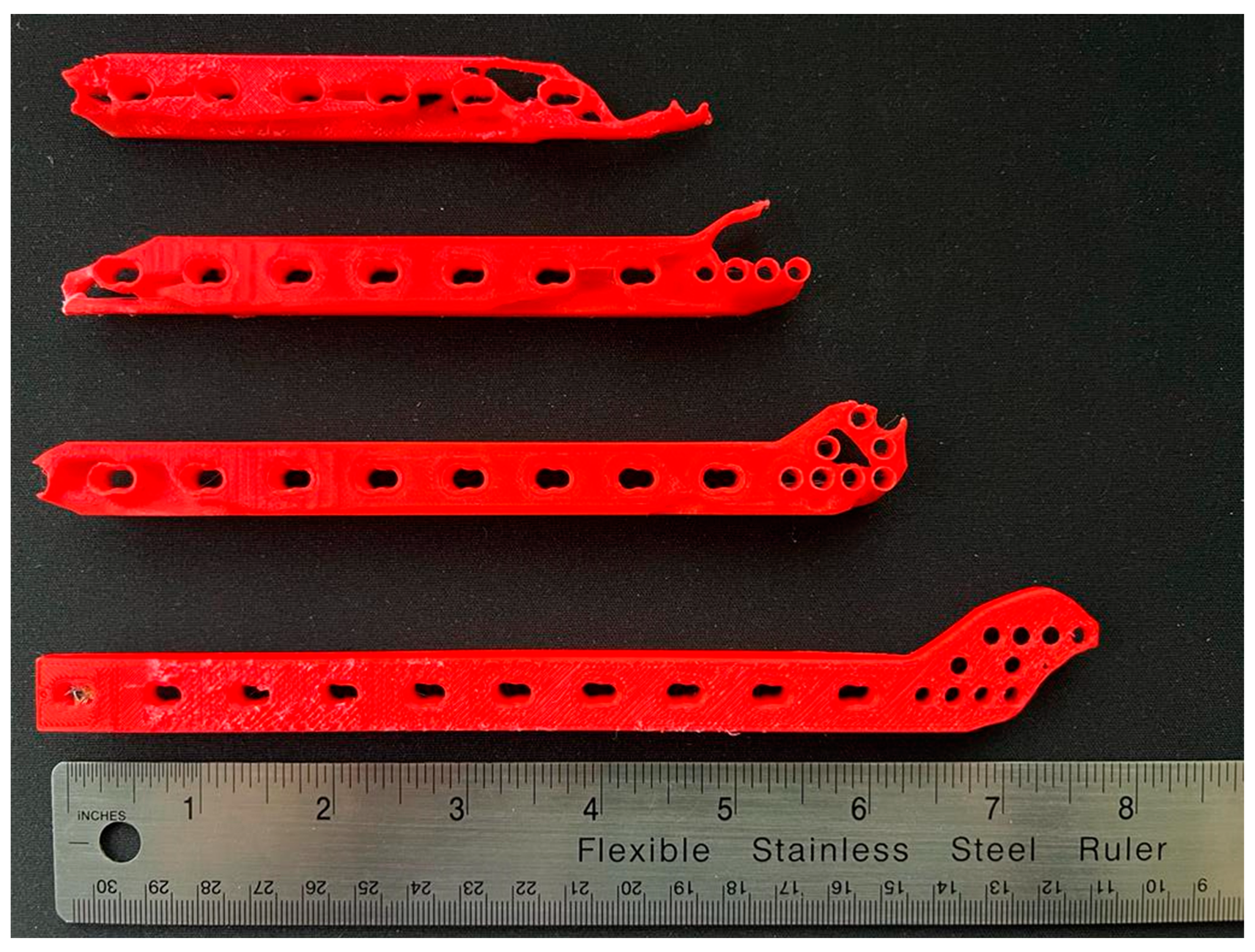
3.5. Plate Prototyping
4. Conclusions
- Topology optimization is a popular technique to target the stress shielding problem in many different types of implants and has been shown to be a suitable tool. Moreover, topology optimization minimizes the drawbacks of manual iterative design procedures through the use of computer aided design and finite element analysis.
- Topology optimization is capable of redistributing the elemental material of a custom-fit distal tibia plate and results in lightweight plates with less equivalent bending stiffness and, consequently, a more flexible plate design.
- Increasing the effect of topology optimization by increasing the volume reduction led to increased stress stimuli transferred to the bone and reducing the risk of stress shielding, while being able to withstand the biomechanical environment and presenting mechanical stable bone plates for all given topology-optimized plates in both screw configurations.
- Topology optimization presented the ability to design for different screw configurations and enabling the alteration of the behavior of the bone fixation, with SC1 optimal designs providing absolute stability and minimal interfragmentary motion, whilst the SC2 optimal designs providing relative stability with interfragmentary motion. This shows that topology optimization is a suitable tool for pre-surgical planning.
- Rapid prototyping presented the ability to create visual prototypes of the intricate designs obtained from topology optimization and to assist with the planning of the surgical operation.
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Miller, D.L.; Goswami, T. A review of locking compression plate biomechanics and their advantages as internal fixators in fracture healing. Clin. Biomech. 2007, 22, 1049–1062. [Google Scholar] [CrossRef]
- Sommer, C.; Gautier, E.; Müller, M.; Helfet, D.L.; Wagner, M. First clinical results of the Locking Compression Plate (LCP). Injury 2003, 34 (Suppl. 2), B43–B54. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K.; Bazaka, O.; Chua, M.; Rochford, M.; Fedrick, L.; Spoor, J.; Symes, R.; Tieppo, M.; Collins, C.; Cao, A.; et al. Metallic Biomaterials: Current Challenges and Opportunities. Materials 2017, 10, 884. [Google Scholar] [CrossRef] [PubMed]
- Ridzwan, M.I.Z.; Shuib, S.; Hassan, A.Y.; Shokri, A.A.; Ibrahim, M.N.M. Problem of stress shielding and improvement to the hip implant designs: A review. J. Med. Sci. 2007, 7, 460–467. [Google Scholar] [CrossRef] [Green Version]
- Elias, C.N.; Lima, J.H.C.; Valiev, R.; Meyers, M.A. Biomedical applications of titanium and its alloys. JOM 2008, 60, 46–49. [Google Scholar] [CrossRef]
- Hanson, B.; van der Werken, C.; Stengel, D. Surgeons’ beliefs and perceptions about removal of orthopaedic implants. BMC Musculoskel. Disord. 2008, 9, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, G.O. Biodegradable implants in orthopaedic surgery—A review on the state-of-the-art. Clin. Mater. 1992, 10, 75–80. [Google Scholar] [CrossRef]
- Inion. Economic Benefit of Biodegradable Ankle Fracture Fixation; Inion OY: Tampere, Finland, 2015. [Google Scholar]
- Manavitehrani, I.; Fathi, A.; Badr, H.; Daly, S.; Negahi Shirazi, A.; Dehghani, F. Biomedical Applications of Biodegradable Polyesters. Polymers 2016, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Prakasam, M.; Locs, J.; Salma-Ancane, K.; Loca, D.; Largeteau, A.; Berzina-Cimdina, L. Biodegradable Materials and Metallic Implants—A Review. J. Funct. Biomater. 2017, 8, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weisgrab, G.; Guillaume, O.; Guo, Z.; Heimel, P.; Slezak, P.; Poot, A.; Grijpma, D.; Ovsianikov, A. 3D Printing of large-scale and highly porous biodegradable tissue engineering scaffolds from poly(trimethylene-carbonate) using two-photon-polymerization. Biofabrication 2020, 12, 045036. [Google Scholar] [CrossRef]
- Hou, Y.; Wang, W.; Bartolo, P. Investigation of polycaprolactone for bone tissue engineering scaffolds: In vitro degradation and biological studies. Mater. Des. 2022, 216, 110582. [Google Scholar] [CrossRef]
- Rama Krishna, K.; Sridhar, I.; Sivashanker, S.; Khong, K.S.; Ghista, D.N. Design of Fracture Fixation Plate for Necessary and Sufficient Bone Stress Shielding. JSME Int. J. 2004, 47, 1086–1094. [Google Scholar] [CrossRef] [Green Version]
- Galbusera, F.; Bertolazzi, L.; Balossino, R.; Dubini, G. Combined computational study of mechanical behaviour and drug delivery from a porous, hydroxyapatite-based bone graft. Biomech. Model. Mechanobiol. 2009, 8, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Rendenbach, C.; Sellenschloh, K.; Gerbig, L.; Morlock, M.M.; Beck-Broichsitter, B.; Smeets, R.; Heiland, M.; Huber, G.; Hanken, H. CAD-CAM plates versus conventional fixation plates for primary mandibular reconstruction: A biomechanical in vitro analysis. J. Cranio-Maxillofac. Surg. 2017, 45, 1878–1883. [Google Scholar] [CrossRef] [PubMed]
- Gutwald, R.; Jaeger, R.; Lambers, F.M. Customized mandibular reconstruction plates improve mechanical performance in a mandibular reconstruction model. Comput. Methods Biomech. Biomed. Eng. 2017, 20, 426–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attard, A.; Tawy, G.F.; Simons, M.; Riches, P.; Rowe, P.; Biant, L.C. Health costs and efficiencies of patient-specific and single-use instrumentation in total knee arthroplasty: A randomised controlled trial. BMJ Open Qual. 2019, 8, e000493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yam, M.G.J.; Chao, J.Y.Y.; Leong, C.; Tan, C.H. 3D printed patient specific customised surgical jig for reverse shoulder arthroplasty, a cost effective and accurate solution. J. Clin. Orthop. Trauma 2021, 21, 101503. [Google Scholar] [CrossRef] [PubMed]
- Ridzwan, S.; Hassan, A.Y.; Shokri, A.A.; Ibrahim, M.N.M. Optimization in Implant Topology to Reduce Stress Shielding Problem. J. Appl. Sci. 2006, 6, 2768–2773. [Google Scholar]
- Park, S.-M.; Park, S.; Park, J.; Choi, M.; Kim, L.; Noh, G. Design process of patient-specific osteosynthesis plates using topology optimization. J. Comput. Des. Eng. 2021, 8, 1257–1266. [Google Scholar] [CrossRef]
- Zhang, A.; Chen, H.; Liu, Y.; Wu, N.; Chen, B.; Zhao, X.; Han, Q.; Wang, J. Customized reconstructive prosthesis design based on topological optimization to treat severe proximal tibia defect. Bio-Des. Manuf. 2021, 4, 87–99. [Google Scholar] [CrossRef]
- Iqbal, T.; Wang, L.; Li, D.; Dong, E.; Fan, H.; Fu, J.; Hu, C. A general multi-objective topology optimization methodology developed for customized design of pelvic prostheses. Med. Eng. Phys. 2019, 69, 8–16. [Google Scholar] [CrossRef]
- Fraldi, M.; Esposito, L.; Perrella, G.; Cutolo, A.; Cowin, S.C. Topological optimization in hip prosthesis design. Biomech. Model. Mechanobiol. 2010, 9, 389–402. [Google Scholar] [CrossRef] [PubMed]
- Al-Tamimi, A.A. 3D Topology Optimization and Mesh Dependency for Redesigning Locking Compression Plates Aiming to Reduce Stress Shielding. Int. J. Bioprinting 2021, 7, 339. [Google Scholar] [CrossRef]
- Chuah, H.G.; Rahim, I.A.; Yusof, M.I. Topology optimisation of spinal interbody cage for reducing stress shielding effect. Comput. Methods Biomech. Biomed. Eng. 2010, 13, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-F.; Fan, Y.-Y.; Jiang, X.-F.; Baur, D.A. A customized fixation plate with novel structure designed by topological optimization for mandibular angle fracture based on finite element analysis. BioMedical Eng. OnLine 2017, 16, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Tamimi, A.A.; Hernandez, M.A.; Omar, A.; Morales-Aldana, D.F.; Peach, C.; Bartolo, P. Mechanical, biological and tribological behaviour of fixation plates 3D printed by electron beam and selective laser melting. Int. J. Adv. Manuf. Technol. 2020, 109, 673–688. [Google Scholar] [CrossRef]
- Siva Rama Krishna, L.; Mahesh, N.; Sateesh, N. Topology optimization using solid isotropic material with penalization technique for additive manufacturing. Mater. Today Proc. 2017, 4, 1414–1422. [Google Scholar] [CrossRef]
- Klahn, C.; Leutenecker, B.; Meboldt, M. Design Strategies for the Process of Additive Manufacturing. Procedia CIRP 2015, 36, 230–235. [Google Scholar] [CrossRef] [Green Version]
- Parthasarathy, J. Additive manufacturing of medical devices. In Additive Manufacturing Innovations, Advances, and Applications; Sudarshan, T.S., Ed.; CRC Press: Boca Raton, FL, USA, 2015; pp. 369–388. [Google Scholar]
- Murr, L.E. Frontiers of 3D Printing/Additive Manufacturing: From Human Organs to Aircraft Fabrication†. J. Mater. Sci. Technol. 2016, 32, 987–995. [Google Scholar] [CrossRef]
- Tilton, M.; Lewis, G.S.; Bok Wee, H.; Armstrong, A.; Hast, M.W.; Manogharan, G. Additive manufacturing of fracture fixation implants: Design, material characterization, biomechanical modeling and experimentation. Additiv. Manuf. 2020, 33, 101137. [Google Scholar] [CrossRef]
- Meinberg, E.G.; Agel, J.; Roberts, C.S.; Karam, M.D.; Kellam, J.F. Fracture and Dislocation Classification Compendium-2018. J. Orthop. Trauma 2018, 32 (Suppl. 1), S1–S170. [Google Scholar] [CrossRef] [PubMed]
- LCP Distal Tibia Plate. Available online: https://www.jnjmedtech.com/en-US/product/35mm-lcp-medial-distal-tibia-plate (accessed on 23 August 2022).
- Bendsøe, M.P.; Sigmund, O. Topology optimization by distribution of isotropic material. In Topology Optimization: Theory, Methods, and Applications; Springer: Berlin/Heidelberg, Germany, 2004; pp. 1–69. [Google Scholar]
- Ferro, N.; Perotto, S.; Bianchi, D.; Ferrante, R.; Mannisi, M. Design of cellular materials for multiscale topology optimization: Application to patient-specific orthopedic devices. Struct. Multidiscip. Optim. 2022, 65, 79. [Google Scholar] [CrossRef]
- Al-Tamimi, A.; Fernandes, P.R.A.; Peach, C.; Cooper, G.; Diver, C.; Bartolo, P.J. Metallic bone fixation implants: A novel design approach for reducing the stress shielding phenomenon. Virtual Phys. Prototyp. 2017, 12, 141–151. [Google Scholar] [CrossRef]
- Kim, S.-H.; Chang, S.-H.; Son, D.-S. Finite element analysis of the effect of bending stiffness and contact condition of composite bone plates with simple rectangular cross-section on the bio-mechanical behaviour of fractured long bones. Compos. Part B Eng. 2011, 42, 1731–1738. [Google Scholar] [CrossRef]
- Wang, S.-P.; Lin, K.-J.; Hsu, C.-E.; Chen, C.-P.; Shih, C.-M.; Lin, K.-P. Biomechanical Comparison of a Novel Implant and Commercial Fixation Devices for AO/OTA 43-C1 Type Distal Tibial Fracture. Appl. Sci. 2021, 11, 4395. [Google Scholar] [CrossRef]
- AO Foundation. Available online: https://www.aofoundation.org/trauma/clinical-library-and-tools/journals-and-publications/classification (accessed on 23 August 2022).
- Al-Tamimi, A.A.; Quental, C.; Folgado, J.; Peach, C.; Bartolo, P. Stress analysis in a bone fracture fixed with topology-optimised plates. Biomech. Model. Mechanobiol. 2020, 19, 693–699. [Google Scholar] [CrossRef] [Green Version]
- BS 3531-23.1:1991; Implants for Osteosynthesis. Bone Plates Method for Determination of Bending Strength and Stiffness. British Standards Institution: London, UK, 1991.
- Minns, R.J.; Bremble, G.R.; Campbell, J. A biomechanical study of internal fixation of the tibial shaft. J. Biomech. 1977, 10, 569–579. [Google Scholar] [CrossRef]
- Ganesh, V.K.; Ramakrishna, K.; Ghista, D.N. Biomechanics of bone-fracture fixation by stiffness-graded plates in comparison with stainless-steel plates. BioMedical Eng. OnLine 2005, 4, 46. [Google Scholar] [CrossRef] [Green Version]
- Wippert, P.-M.; Rector, M.; Kuhn, G.; Wuertz-Kozak, K. Stress and Alterations in Bones: An Interdisciplinary Perspective. Front. Endocrinol. 2017, 8, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, N.; Li, S.; Zhang, B.; Wang, C.; Chen, B.; Han, Q.; Wang, J. The advances of topology optimization techniques in orthopedic implants: A review. Med. Bio.l Eng. Comput. 2021, 59, 1673–1689. [Google Scholar] [CrossRef]
- Lang, J.J.; Bastian, M.; Foehr, P.; Seebach, M.; Weitz, J.; von Deimling, C.; Schwaiger, B.J.; Micheler, C.M.; Wilhelm, N.J.; Grosse, C.U.; et al. Improving mandibular reconstruction by using topology optimization, patient specific design and additive manufacturing?-A biomechanical comparison against miniplates on human specimen. PLoS ONE 2021, 16, e0253002. [Google Scholar] [CrossRef] [PubMed]
- Ruedi, T.; Buckley, R.E.; Moran, C.G. AO Principles of Fracture Management-Vol. 1: Principles-Vol. 2: Specific Fractures, 3rd ed.; Thieme: Stuttgart, Germany, 2018. [Google Scholar]
- Liao, B.; Sun, J.; Xu, C.; Xia, R.; Li, W.; Lu, D.; Jin, Z. A mechanical study of personalised Ti6Al4V tibial fracture fixation plates with grooved surface by finite element analysis. Biosurface Biotribology 2021, 7, 142–153. [Google Scholar] [CrossRef]
- Gibson, I.; Rosen, D.; Stucker, B.; Khorasani, M. Additive Manufacturing Technologies, 3rd ed.; Springer Nature: Cham, Switzerland, 2021; p. 675. [Google Scholar]
- Al-Tamimi, A.; Huang, B.; Vyas, C.; Hernandez, M.; Peach, C.; Bartolo, P. Topology optimised metallic bone plates produced by electron beam melting: A mechanical and biological study. Int. J. Adv. Manuf. Technol. 2019, 104, 195–210. [Google Scholar] [CrossRef] [Green Version]
- Segaran, N.; Saini, G.; Mayer, J.L.; Naidu, S.; Patel, I.; Alzubaidi, S.; Oklu, R. Application of 3D Printing in Preoperative Planning. J. Clin. Med. 2021, 10, 917. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Number of Elements |
|---|---|
| Bone plate | 400,000 |
| Screws | 500 |
| Tibia bone–Proximal | 87,000 |
| Tibia bone–Distal | 29,000 |
| Equivalent Bending Stiffness Change (%) | ||
|---|---|---|
| Initial Design | 14.13 ± 1.7 N.m2 | |
| Volume Reduction, % | Plates SC1 | Plates SC2 |
| 25 | −22.29% | −20.99% |
| 50 | −32.74% | −27.83% |
| 75 | −76.24% | −73.38% |
| Plate | Von Misses Stress Change (%) | |
|---|---|---|
| SC1 | SC2 | |
| TO25-BP | 0.16 | 0.09 |
| TO50-BP | 2 | 5 |
| TO75-BP | 13 | 13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Tamimi, A.A. Topology Optimization of Patient-Specific Custom-Fit Distal Tibia Plate: A Spiral Distal Tibia Bone Fracture. Appl. Sci. 2022, 12, 10569. https://doi.org/10.3390/app122010569
Al-Tamimi AA. Topology Optimization of Patient-Specific Custom-Fit Distal Tibia Plate: A Spiral Distal Tibia Bone Fracture. Applied Sciences. 2022; 12(20):10569. https://doi.org/10.3390/app122010569
Chicago/Turabian StyleAl-Tamimi, Abdulsalam A. 2022. "Topology Optimization of Patient-Specific Custom-Fit Distal Tibia Plate: A Spiral Distal Tibia Bone Fracture" Applied Sciences 12, no. 20: 10569. https://doi.org/10.3390/app122010569
APA StyleAl-Tamimi, A. A. (2022). Topology Optimization of Patient-Specific Custom-Fit Distal Tibia Plate: A Spiral Distal Tibia Bone Fracture. Applied Sciences, 12(20), 10569. https://doi.org/10.3390/app122010569