1. Introduction
The aging index is the ratio of the elderly (economically inactive and aged 65 and over) to young people (aged 0 to 14). Statistics in Taiwan show that the aging index has spiraled from 49.3 (2005) to 107.9 (2018) (see Ministry of the Interior, Department of Statistics,
https://www.moi.gov.tw/stat/chart.aspx, accessed on 1 November 2022), which is higher than it is in many other developed countries. In addition, though some elderly people with a chronic disease living in Taiwan have doctor or caregiver support in a nursing home. However, in times of the COVID-19 epidemic, most sub-healthy elderly people (ShEP) live alone and frequently go outside to keep their distance from others in their daily activities, exposing themselves to a high level of risk for falls, sudden illness, and accidents [
1]. During the COVID-19 pandemic, new risk environment variables for falls have emerged. The first environmental variable may be that the pandemic could increase the risk of caregivers. For example, if the family members of caregivers test positive for COVID-19, they have to remain at home, leading the elderly they care for to be lonely at home. The second variable needed to be taken into consideration could be whether the family members of elderly people themselves test positive or whether the infection of colleagues leads to family members staying at home, which also increases the length of isolation for the elderly. The third aspect is that elderly people themselves increase the risk of infection because their resistance is weak, so they become more seriously ill or take longer to recover than the average person. The existing protection process of government regulations for the home isolation system never considered the issues mentioned above, it only took into account the spread of the virus and did not consider that these isolation measures would cause these elderly individuals to fall prey to higher levels of risk. Based on the new risk factors created by the pandemic, these past methods of preventing falls in elderly people have produced significant changes that cannot be easily dealt with.
Falls are among the biggest dangers to ShEP and encompass any instance in which an elderly person loses their balance or trips over something, especially during outside activities. In Asia, over half of the injuries to senior citizens (over the age of 65) come from falls and can have serious consequences [
2,
3]. For example, a fall can result in a bump to the head that, if left untreated, can lead to permanent brain damage [
1,
4]. Therefore, detecting accidents and reacting quickly is very important.
ShEP are an especially vulnerable group since they may not demonstrate typical pathologic symptoms or may express discomfort without any diagnosable or obvious illnesses. These common occurrences demonstrate that traditional standard medical observation methods are not suitable for ShEP [
4]. Consequently, more needs to be undertaken for this vulnerable group. Research on fall detection for ShEP care is still rare. Family members and caregivers can call and ask questions regarding an elderly person’s activities, but it is difficult to know the risk for falls without being physically present [
5]. Important context, such as location, has to be gathered in order to determine the risk level [
6].
Although some technologies, such as an activity calendar, can provide us some information about whether or not ShEP are undertaking dangerous activities; however, those tools require caregivers and family members to maintain constant contact with ShEP and guess whether or not they are in danger. The methods could be ineffective and do not address the problem of dynamic human variability. The first research question: in times of the COVID-19 epidemic, what is the relationship between dynamic risk factors and falls? In order to better support an effective healthcare mechanism, we need to first understand the relationship between risk factors and falls. The second research question: how can we build an effective system based on the factors we found? To solve the second research question, we need to develop an effective system based on all relevant factors, since existing studies only focus on retrieving context information from limited methods and are ineffective in examining many factors related to fall detection. The third research question: Can we build a system with the personal learning pattern based on the second question? To overcome the third research question, we need to fine-tune the system to handle human variability and personal matters. Everyone has different behavioral patterns, and ShEP are no exception.
This study will provide an alternative to addressing these problems and is organized as follows: In
Section 2, the literature review is presented in detail. In
Section 3 and
Section 4, a proposed method and the research model are introduced. In
Section 5, the evaluated method is introduced and then followed by the conclusion, including the expected contributions and limitations.
2. Literature Review
Some studies [
4,
7] state that medical records can help predict problems with falls, and using additional data is critical to detecting dynamic status changes within a user’s daily activities. In this section, some existing methods can be summarized as three categories: personal information management (PIM), collaborative filtering (CF), and wearable devices (WD). PIM in the ShEP area means the current physical conditions of the elderly. It includes chronic diseases, nursing interventions, counseling experience, and fall accidents [
8,
9]. In order to find out what context factors of a healthcare system could be relevant to fall detection, it is necessary to conduct a literature review in PIM. CF in the ShEP area represents the sharing of real-time information between an elderly person, family member, and caregivers and can be scaled up for a healthcare system or used through social media application systems (e.g., Facebook) to let caregivers know whether or not the elderly person is at risk [
10]. WD is a good method for identifying patterns in the elderly individual’s behavior and using big data analysis to help with fall detection [
11,
12].
PIM is an important research area in information systems. PIM can be applied to a healthcare system to allow for personalized features [
8]. For example, patients can have an inspection scheduled in their appointment based on the current state of their illness. PIM is an important clue as to the current physical condition of an elderly person. Among its varied advantages, PIM can provide relevant factors for falls and allow sub-healthy patients and their caregivers to interactively and constructively participate in their own care. PIM also provides information about altered behaviors that can impact fall detection, including smoking, exercise, diet, and alcohol consumption [
9].
Despite these advantages, however, PIM has some limitations. For example, a user may need to guess whether or not a current activity corresponds to their PIM, but in a real situation there is the possibility that risk activities may suddenly occur beyond their PIM. Therefore, only using PIM is insufficient to protect against all variations and exceptions to ShEP activities. In addition, PIM does not record every symptom experienced by a user (e.g., a mild sprain), and many caregivers do not know the details of patients’ chronic diseases due to privacy issues. This possibility of misrepresentation limits its effectiveness in fall detection and makes it insufficient as a sole source of information for healthcare systems.
CF is widely used in e-commerce applications, mobile applications, and recommender systems [
13,
14,
15,
16,
17,
18], particularly in healthcare through a “Neighborhood-based” approach [
13,
14,
16], which provides a possible option for predicting the behavioral patterns of the elderly based on their preferences [
17]. In addition, CF can incorporate an elderly person’s nearest neighbors or relevant members into clustering algorithms [
14] for predicting the probability of a fall. Therefore, the clinical applications of fall detection can appropriately include CF (e.g., through social media or a decision support system) in the hopes of identifying potential risks to the elderly.
Existing methods using CF techniques share the context information of an elderly person with others to avoid possible risks. For example, the elderly can share their location to their friends or family members when they are exercising in a park [
19]. Therefore, that information can be useful to caregivers when deciding whether or not there is a risk. If such a system were applied accurately and effectively, a healthcare system based on CF techniques could be more scalable than a system based on PIM, because CF can respond to real-time situations dynamically.
However, CF requires the elderly person to send their current context information to the system constantly and caregivers need to check the system frequently, which is tedious. In addition, the context information may be misleading. For example, the elderly person may walk to a park for exercise but may only be sitting on a chair without any risk. As a result, CF is also insufficient for a healthcare system’s needs. In sum, it is not suitable to use CF in times of the COVID-19 epidemic.
Wearable devices monitor the physiological characteristics of users [
11,
20,
21] (e.g., weight and blood pressure) to know whether or not they are in danger. Some of the factors it monitors could trigger chronic diseases, such as an unhealthy diet, a lack of physical exercise, and irregular sleeping [
20]. These unhealthy living habits could also cause death or disability in the elderly. To address the challenges of monitoring chronic diseases in real time, many researchers have designed these wearable devices to monitor characteristics, such as blood pressure, and provide basic healthcare services with the internet of things (IoTs) cloud architecture [
11,
12,
21]. Some researchers use the WD method to replace mobile sensors, such as accelerometers, in order to obtain fixed body placement for ShEP [
22]. However, this method is usually not accepted widespread because these wearable devices could reveal the weaknesses of ShEP and they may also forget to wear such external devices.
WDs still have many limitations. First, although a WD can measure the physical health state of the elderly dynamically, it is not sufficient for identifying fall risks in real time. Second, a WD cannot measure many human behaviors that may be relevant to fall risks, only physiological characteristics. For example, a WD cannot tell whether elderly people are sitting or running in a park or in a room. However, those activities could be risk factors for a fall. Third, many elderly people do not use a WD, so it could be less useful for ShEP who undertake many activities.
Although existing studies reveal that PIM, CF, and WD could be relevant to fall detection, there are still many limitations. The strengths and weaknesses of each approach are summarized in
Table 1. One of the common limitations across these systems is a lack of sufficient context information to improve user performance and the awareness of fall risks. In addition, the majority of studies on healthcare systems do not consider the serious problem of human variability. Even some researchers use mobile sensors, but they mainly focus on using the accelerometer as a sensor, which has insufficient context information to lead to the low performance of fall detection [
23,
24]. This paper will try to address the existing problems of user performance and human variability by using context information and AI technologies. The proposed methods are described in the following sections.
Most existing studies on the identification of risk context factors affecting the elderly are designed and optimized for personal information management (PIM) only. This system includes information, such as physical symptoms, impairment records, and demographics [
7,
25]. However, PIM is a highly personal and burdensome task because the information is stored in multiple hierarchies [
25]. Another existing method is called collaborative filtering (CF). Users can share their current context information (e.g., interest or location) with family members or caregivers to let them know whether they are safe or in danger. CF is usually used through social network domains, such as Facebook. CF has been proven to be beneficial in improving healthcare performance by alleviating the problems of context information loss, disconnection, and redundant contacts [
15,
16,
18,
26], but it is not enough for detecting sudden risks immediately and effectively. In summary, most studies focus on developing a system of fall detection through static risk factors, and there are few empirical studies that systematically examine the impact of those factors on elderly care [
27]. Using PIM (e.g., medical records) and CF systems to detect abnormalities without a much wider variety of real-time context information and predictive algorithms (e.g., through AI technologies) creates obstacles to alerting ShEP of risk factors immediately and accurately [
28,
29].
3. The Proposed Method
According to International Data Corporation (IDC) reports, the worldwide mobile device market could reach 1.76 billion units shipped in 2020 (see Worldwide Smartphone Forecast Update,
https://www.idc.com/, accessed on 1 November 2022). Many studies show that ShEP widely uses smartphones in their everyday lives [
30,
31,
32]. Yet, their mobile technology needs with regard to healthcare application systems have received too little attention from academic researchers or practitioners so far. One of the purposes of this study is to find out the risk factors of fall detection among ShEP who still participate in numerous daily activities and regularly use mobile phones for their social communications. This study proposes a novel method using smartphones with mobile sensors to detect and monitor the dynamic context information of ShEP. The proposed method is suitable for people who did not need body contact during the COVID-19 epidemic.
The first proposed method is an indoor and outdoor (IO) approach. Smartphones can be used in fall detection to alert caregivers immediately after an accident, which can help lower the possibility of further consequences, such as permanent brain damage or sudden death. However, existing studies only focus on technologies, such as three-axis accelerometers or gyroscopes [
5,
33], which only detect some phenomena. Most ShEP participate in activities in different locations with varying fall risks [
4]. For example, forest trails and bedrooms present different risk probabilities for falls; thus, it is difficult to accurately assess risk factors only using PIM or CF. For these reasons, the first proposed method is an indoor and outdoor (IO) approach to fall detection.
Light intensity could be one of environment contexts for detecting whether a ShEP is indoors or not. Mobile light sensors can help dynamically capture light intensity. For example, if the value of illumination is greater than 5000 lux, which indicates in a sunny environment, it could suggest a lower probability of falling. Therefore, to decrease the probability of falls, illumination should be one of the more significant factors, such as changing our visualization to a bright level. Mobile light sensors could detect indoor or outdoor environments because we can use the illumination value as an emergency number in a dark room. If the value breaks through a certain threshold, we can conclude that a fall is occurring. The IO algorithm is presented below (Algorithm 1). The algorithm initializes the light dataset values with R programming and sets up the logic functions by the IES (the Illuminating Engineering Society of North America (
https://www.ies.org/, accessed on 1 November 2022)) based on initial dataset, computes the categories to enable the dynamic overall detection on the light shift to measure whether the individual is in an indoor environment or not.
| Algorithm 1 Indoor and Outdoor (IO) Approach |
| 1. Initialization of parameters: |
| dataset1 <- maml.mapInputPort (1) # class: data.framen <- nrow (dataset1) Categories <- c () |
| 2. Set up logic functions: |
for (i in 1:n){
light <- dataset1 [i,1]
if (light >= 0 & light < 120) cm 1 = Dark room
if (light >= 120 & light < 250) cm 1 = Dimmed room
if (light >= 250 & light < 1000) cm 1 = Bright room
if (light >= 1000 & light < 5000) cm 1 = Cloudy
if (light >= 5000) cm 1 = Sunny
Categories <- c (Categories, cm 1)} |
| 3. Compute the indoor and outdoor (IO): |
data.set <-c bind (dataset1, Categories)
maml.mapOutputPort ("data.set"); |
The IO algorithm approach takes into account a variety of contextual environments and categorizes them according to their risk factors. Consequently, all environments are labeled as “indoor” or “outdoor” in order to determine whether the elderly person will be at risk of a fall because noise, lights, and temperature could be important cues for their healthcare, mobile devices with an embedded light sensor can also be used to identify the environment surrounding the user [
34].
The second proposed method is a standing and lying (SL) approach. According to the multitasking theory [
35], a user is more at risk of falling when performing a secondary task in addition to a primary task. Those behaviors include when elderly people use mobile phones, although the risk is varied depending on whether the user performs the second action while holding the phone or while in the act of putting it down [
34,
35]. Consequently, it is important to know whether a user is holding onto or putting down their mobile device.
Although a few studies propose mobile sensors for fall detection using gyroscopes, tri-axis accelerometers, and magnetic sensors [
5,
33,
36], none of these technologies focus on standing and lying (SL) for multitasking detection [
22,
37]. Moreover, to the best of our knowledge, no literature has mentioned SL-based fall detection or usage within a fall detection system. The accelerometer z-axis sensor could be used for detecting standing or lying because we can use the surface of the earth by 9.8 m/s
2 as G (that is, 1 G = 9.8 m/s
2) when lying. I If the barycenter breaks through a certain threshold, such as θ, we can conclude that a fall is occurring. Conversely, if the inclination is supported by devices such as crutches, we can measure the value of the acceleration if it is lower than the θ, which is back to the horizontal plane to avoid the falling. The SL algorithm is presented below (Algorithm 2). The algorithm initializes the accelerometer X, Y, and Z values and sets up the logic functions by the dynamic angle based on initial AccX0, AccX1 and AccX2 and computes the falling points (FP) to enable the dynamic overall detection on the barycenter shift to measuring whether the FP is sufficient or not.
| Algorithm 2 Standing and Lying (SL) Approach |
| 1. Initialization of parameters: |
| AccX0, AccX1, AccX2, AccY0, AccY1, AccY2, AccZ0, AccZ1, AccZ2 |
| 2. Set up logic functions: |
| Fall_X012 (AccX0, AccX1, AccX2) |
| Fall_Y012 (AccY0, AccY1, AccY2) |
| Fall_Z012 (AccZ0, AccZ1, AccZ2) |
| 3. Compute the falling points (FP): |
If Fall_X012 && Fall_Y012 && Fall_Z012 >= FP then Fall = yes
Else Fall = no |
| End if |
Because elderly people use smartphones, an effective healthcare system should be able to detect their risk level and notify them to protect against falls until their tasks are completed. For these reasons, this SL algorithm approach is an important and novel method in our goal to solve fall accident issues.
The third proposed method is a resting and moving (RM) approach. ShEP are at an increased risk for falls during daily activities because they move all the time, and CF’s location tracking status has been shown to be insufficient for their protection. As previously described, the major concern using CF is its requirement for the elderly person to report their preference or location status and its lack of context about whether the elderly person is walking or running, which is important information for fall detection. Therefore, a new method that can detect whether they are resting or moving is necessary. In the RM approach, it is important for a real-time response to fall detection, so the instant speed (distance divided by instant time (m/s)) of the approach is used for measurement. We can use time sensors to measure instant time and GPS for the distance. As for transition speeds, they are 1 m/s, 2 m/s, and 3.5 m/s, corresponding to walking, running, or driving [
34,
38]. It indicates walking when the speed is less than 2 and greater than 1; a speed of less than 3.5 and greater than 2 represents running. If it is greater than 3.5, the RM changes to driving status. The RM algorithm is presented below (Algorithm 3). The first step of the algorithm initializes the instant speed dataset values with R programming. The second step is to set up the logic functions based on the previous research dataset. The final step is to output the categories, such as the walking, running, and driving statuses, in order to enable the dynamic overall detection of the RM approach for measuring whether an individual is moving or not.
| Algorithm 3 Resting and Moving (RM) Approach |
| 1. Initialization of parameters: |
Dataset2 <- mam1.mapInputPort (1) # class: data.frame
n <- nrow (dataset2)
Categories <- c () |
| 2. Set up logic functions: |
for (i in 1:n){
instant speed <- dataset2 (i,1]
if (instant speed >= 0 & instant speed < 1) is 1 = Staying
if (instant speed >= 1 & instant speed < 2) is 1 = Walking
if (instant speed >= 2 & instant speed < 3.5) is 1 = Running
if (instant speed >= 3.5) is 1 = Driving
Categories <- c (Categories, is 1)} |
3. Compute the resting and moving (RM):
data.set <- cbind (dataset2, Categories)
maml.mapOutputPort (“data.set”); |
The proposed system architecture (
Figure 1) defines the process for obtaining context awareness, including context interpretation and logical computing. To increase the accuracy, personalization, and learning orientation of healthcare systems, this study not only investigates the existing studies on fall detection to try to determine all possible context factors, but also uses artificial intelligence (AI) technologies to increase the performance of healthcare systems. With those context factors added, we developed a system called the Intelligent Healthcare Agent System (IHAS). A large variety of ShEP context information is retrieved via physical sensors, and it must be properly represented with a structured and interchangeable format. The adaptive service is activated only when ShEP are not available, and unexpected results regarding context awareness are sent back to cloud storage for further learning adjustments in order to improve the system’s response times. In this way, the proposed method can respond to real-time fall detection immediately after complex logical computing, which is of the highest importance.
The proposed system architecture, IHAS, can differentiate between indoor and outdoor environments by using tools such as mobile light sensors to detect the availability and intensity of lights (i.e., their illuminance). According to the rule of the Illuminating Engineering Society of North America (IES), which is the recognized technical authority on illumination and defines standard levels of lights based on the lux unit of lighting [
39], the value of illuminance should be transformed into understandable information. For example, if the value of illuminance is greater than 1000 lux, one can infer that the elderly person is outside. As with SL, if we want to overcome unstable human motions, we can also use the accelerometer z-axis sensor to detect the horizontal angle of the orientation of mobile devices [
34]. Therefore, if an absolute value of acceleration is greater than a certain threshold above 9.8 m/s
2 (i.e., 1 G), then we can say that the orientation is horizontally upward or downward [
34]. In addition, the technology separates body motion and movement into SL and RM in order to reduce possible errors from false detection. Further protections against errors are afforded by its use of multiple data points to detect speed. One cannot obtain user speed instantly from a single mobile sensor, such as an accelerometer sensor. Instead, the speed calculation should be equal to the distance (meters) per second and should measure the distance divided by instant time (m/s) [
34]. If the speed is greater than 1 m/s, we can say that the elderly person is moving [
40].
Many studies mention that elderly people desire to live at home when afflicted with chronic diseases [
8,
9]. However, ShEP are more active. Therefore, RM could be a meaningful aid for fall detection. We can detect the vertical acceleration and orientation of ShEP by using mobile sensors in order to determine whether they are lying or standing [
41,
42]. However, it is difficult when only using a single mobile sensor, such as an accelerometer, to detect RM because ShEP are often active outside, regularly transitioning from the lying to standing status. For that reason, adding this information context is important. In addition, ShEP usually keep their phones in their pockets when walking or running. As a result, significant errors are introduced from simply using accelerometers, gyroscopes, and magnetic sensors to detect RM. Unlike these other methods, IHAS can calculate instant speed without considering the average velocity because a fall can occur suddenly, and an effective system needs to be aware of the change of speed immediately.
4. The Research Model
An ideal healthcare system would have the ability to gather instant context information and promptly respond to ShEP and caregivers [
43]. Therefore, we propose a novel method including IO, SL, and RM sub-methods to increase the effectiveness of the system. We propose that healthcare systems also consider the methods of personalization and learning orientation. IHAS utilizes machine-learning algorithms to deal with the challenge of human variability [
44,
45]. The elderly can have different preferences and may change their behaviors based on their dynamic personal information (e.g., plasma glucose) even under the same context conditions [
46,
47,
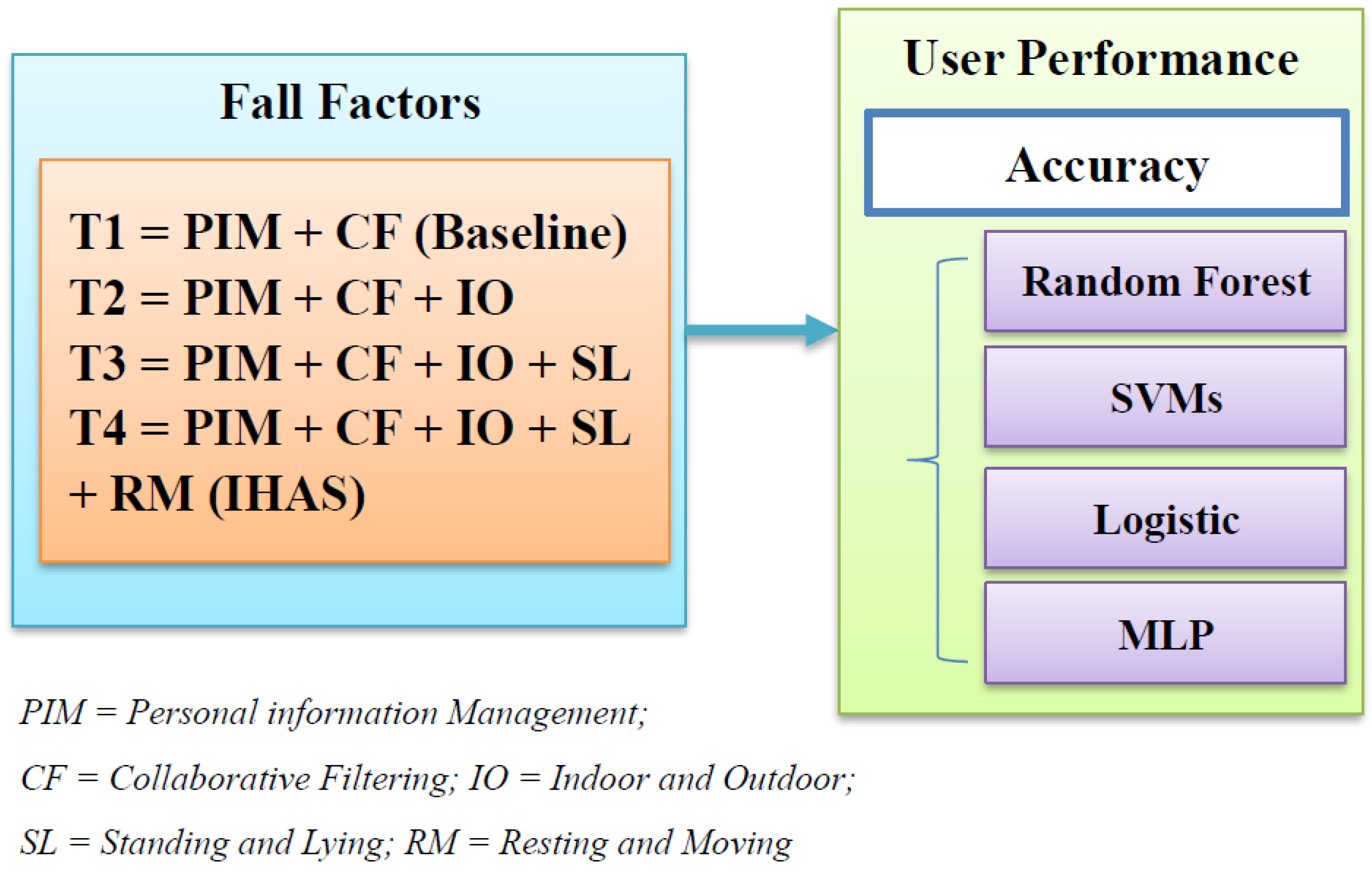
48]. Thus, the system automatically needs to learn information by itself. The research model for this system, which compares with existing methods, is shown in
Figure 2.
In this research model, Treatment 1 with PIM and CF is treated as the baseline to compare against IHAS and other sub-methods. Although WD can also reveal the real-time context information, many ShEP are not willing to use it all day if it performs some of the same functions as a mobile phone. Therefore, this study removes it from the baseline for reacting to a real situation. IHAS is Treatment 4, incorporating all of the above relevant factors. Because this study focuses on the interaction between the elderly and mobile devices during their daily activities, the reporting time and accuracy are appropriate for measuring user performance. AI technologies utilize a substantial amount of context information for training, so user performance may also be affected. There is no existing work on incorporating IO, SL, and RM into a system. However, as previously described, these methods could significantly improve the accuracy of fall detection. Therefore, this study contends that PIM, CF, IO, SL, and RM are all relevant to fall detection. The first hypothesis is the following:
H1. Incorporating the risk factors (a) PIM, (b) CF, (c) IO, (d) SL, and (e) RM into the system will have a positive impact on the performance of fall detection.
The main purpose of this study is to prove that Treatment 4 (IHAS) is more effective in fall detection than the existing methods, including Treatments 1, 2, and 3. Therefore, IHAS should be compared with these existing methods to determine the accuracy of each approach in fall detection. The rest of the hypotheses are proposed using the following:
H2. In fall detection, IHAS will lead to the best performance when compared to the baseline (Treatment 1), followed by Treatment 2 (H3) and Treatment 3 (H4).
As previously described, we utilize AI technologies in IHAS to handle human variability, because AI can adapt to different user patterns through training and build personalization and self-learning mechanisms. From this perspective, IHAS offers more benefits to ShEP with integrated AI technologies.
5. Experiment Design
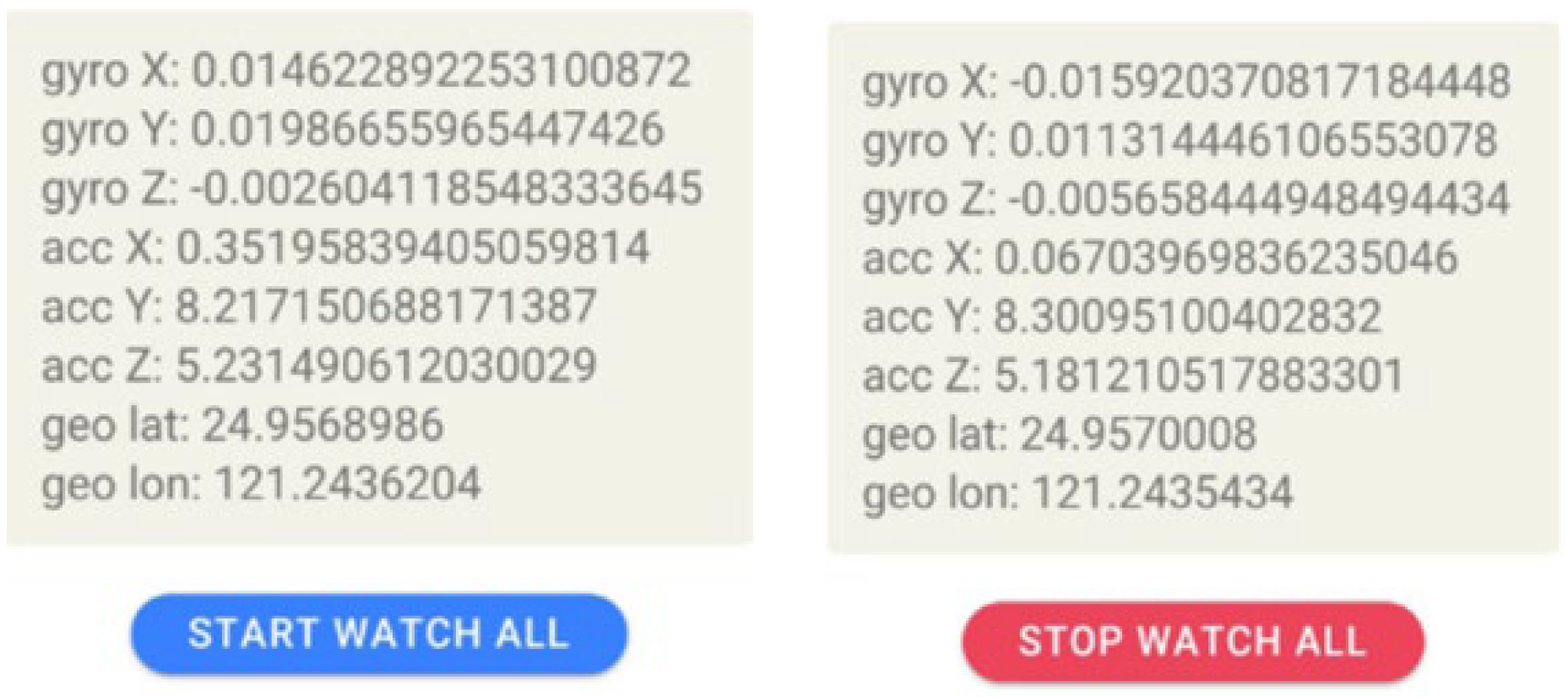
The prototype system was built based on IHAS. The prototype system can collect the ground truth data through a questionnaire regarding IO, SL, and RM context information coupled with AI technologies collecting quantitative measures of user performance. A prototype system (
Figure 3) was developed using Android Studio software, which is built on Java programming and Android SDK. This mobile application services (APPs) type is suitable for running on smartphones in order to automatically detect real-time context information.
The availability of ShEP data is checked through a context-aware process based on the system architecture of IHAS. There are 148 ground truth records (please see the Ground Truth of the Availability for Evaluation, the Excel data used to support the findings of this study have been deposited in the “The Ground Truth of the Availability for Evaluation.xlsx” repository in [
https://drive.google.com/file/d/1Nd3KXnmRZKhc9VgWsCe8qXxVBHMeJ9G7/view?usp=sharing, accessed on 1 November 2022].) collected from the questionnaire regarding the availability factors, which proves that the proposed method is better than the existing methods. We recruited 148 users, all over 18 years old, to fill the perceptions through the online survey (
https://www.surveycake.com/s/6o7VO, accessed on 1 November 2022), and all information concerning this questionnaire was given to participants before the survey, such as the meanings of the terms PIM and CF, the ability to interrupt the survey anytime, consent agreements of free will, no risk statements, etc. In order to evaluate IHAS, the independent variable is defined with the level of context used, which was operationalized on four levels: (1) a baseline of PIM and CF; (2) PIM, CF, and IO; (3) PIM, CF, IO, and SL; and (4) PIM, CF, IO, SL, and RM. The dependent variable is the accuracy rate of correct fall predictions, which is associated with the research questions as well as the hypotheses.
The experimental design of this paper is mainly based on the scope of the IHAS model to develop a smartphone prototype APPs software to collect real-time dynamic information about the elderly. At present, this prototype system is mainly used to collect environmental perceptions and use questionnaire feedback from the elderly. According to the prototype system, we can continue to analyze whether or not the elderly could be at risk (not availability) through machine learning algorithms in response to these four situations. In the future, the complete formal commercial ShEP system based on the IHAS architecture will emphasize the comfort of users and the ease of operation of mobile phones for the elderly. Dynamic adjustments will be made according to the feedback of the users, such as the expansion of the detecting information and the alerts function if they are at risk. The system will be combined with the different mobile phone interfaces of family members and caregivers to enable the instant messages function regarding prevention, which can generate personalized interfaces for different user groups.
For classification tasks, true positive (TP), true negative (TN), false positive (FP), and false negative (FN) rates assess the results of classifiers with observations. Positive or negative means a classifier’s prediction, and the terms “true” or “false” refer to whether or not the prediction could correspond to the observation [
49,
50]. Accuracy is the number of correct predictions divided by the total number of fall predictions (i.e., accuracy = (TP + TN)/(TP + TN + FP + FN)). Machine learning algorithms (including random forest, SVMs, logistic, and MLP) are used with 10-fold cross validation to obtain the accuracy of the fall predictions of IHAS with four levels of context used. A single subsample provides validation data for testing, and the remaining nine subsamples are training data. All observations can be used for both training and testing, and each observation for validation occurs exactly once. These algorithms are chosen because they are popular machine learning algorithms and have been widely used [
51].
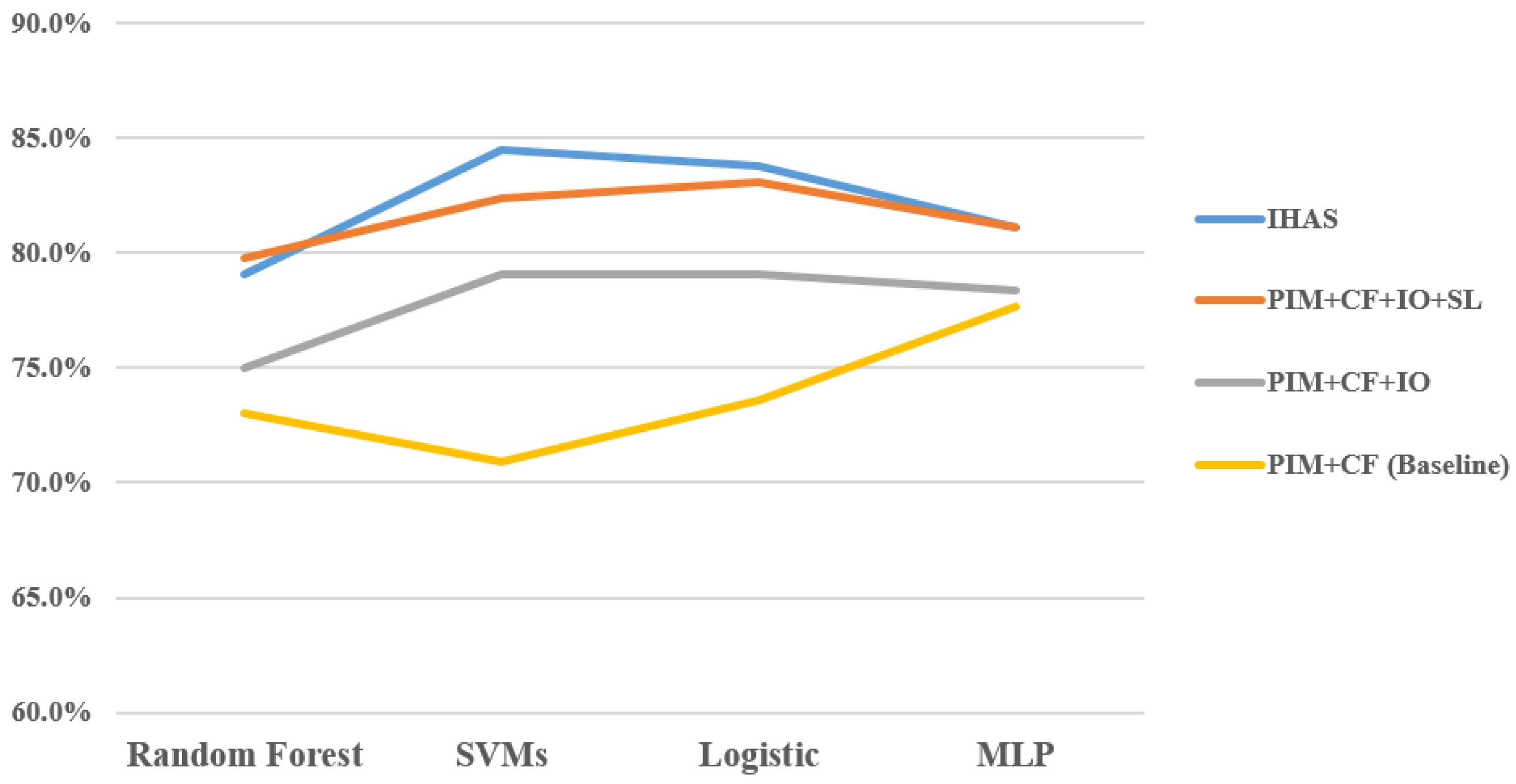
The accuracy of classification algorithms is shown in
Figure 4. For the baseline only, the accuracy of random forest is 73%, SVMs is 70.9%, logistic is 73.6%, and MLP is 77.7%. After adding IO, the accuracy of random forest is 75, SVMs is 79.1%, logistic is 79.1%, and MLP is 78.4%. If SL is continuously increased to the risk factor list, the accuracy of random forest is 79.8, SVMs is 82.4%, logistic is 83.1%, and MLP is 81.1%. As for IHAS, the accuracy of random forest is 79.1, SVMs is 84.5%, logistic is 83.8%, and MLP is 81.1%.
To test the first hypothesis, ANOVA was used to assess whether or not the effect of risk factors reveals significant differences between using the availability data on the fall detection model (including PIM, CF, IO, SL, and RM) and not using the availability data. The main effects of fall prediction (F (3, 15) = 11.75, p < 0.01) are significant. Therefore, the first hypothesis is supported. The LSD test was carried out for multiple comparisons. IHAS has significantly higher accuracy than the baseline (mean difference = 8.33, p < 0.05) and Treatment 2 (mean difference = 4.23, p < 0.05). Therefore, the second and third hypothesis are all supported. As for Treatment 3 (mean difference = 0.53, p > 0.05), the fourth hypothesis is not supported.
To give a comprehensive discussion of such results, regarding the relevant risk factors of availability based on sensor information, the results of the evaluation indicate that the risk factors had significant impacts on fall detection. IHAS (including all risk factors) performs better in fall detection than the existing methods using only PIM and CF (Treatment 1). There is a difference in the results between IHAS and other treatments. For example, Treatment 3 has an insignificant impact on increasing fall detection.
6. Conclusions
According to the evaluation in the previous section, IHAS is compared to the existing methods and functions significantly better than them. In addition, the proposed system can trigger a notification to caregivers to assist in reducing the risks of falls and their potential consequences. IHAS represents a better tool for ShEP than only relying on behavioral or medical histories, which may increase the error rate of fall predictions because of human variability in predicting the possible risk of falls.
IHAS utilizes classification algorithms, which are the most popular AI technologies, to calculate the accuracy of four different treatments. IHAS addresses several existing problems in fall detection systems: (1) a focus limited to one or two types of fall detection, (2) a lack of system architecture defining the process for context awareness, and (3) an oversight regarding human variability. This research led to several contributions: (1) incorporating all risk factors concerning fall detection, (2) examining the effect of the risk factors on fall detection, (3) separately examining the effects of PIM, CF, IO, SL, and RM, (4) overcoming the challenges of building a context-aware process in the system architecture, and (5) utilizing AI technologies to manage human variability.
This study contributes to both practical applications for fall detection, as well as future research on the topic. As more of the population ages, in times of the COVID-19 epidemic, falls will continue to be a huge problem, especially for ShEP. Although the issue is becoming more and more serious, this topic is still in an early stage of discussion, and ShEP are suffering. More needs to be done. This paper also has some limitations. For example, we will need to collect vast amounts of data through AI technologies in order to verify the performance of IHAS effectively. Nevertheless, this study offers a clear direction for further research and promising initial results in fall detection.








{kind=link}
{kind=link}
{kind=link}
{kind=link}