

Gamification of Upper Limb Rehabilitation in Mixed-Reality Environment
 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Related Works
3. Development
3.1. Concept
3.2. Components
3.2.1. HoloLens 2
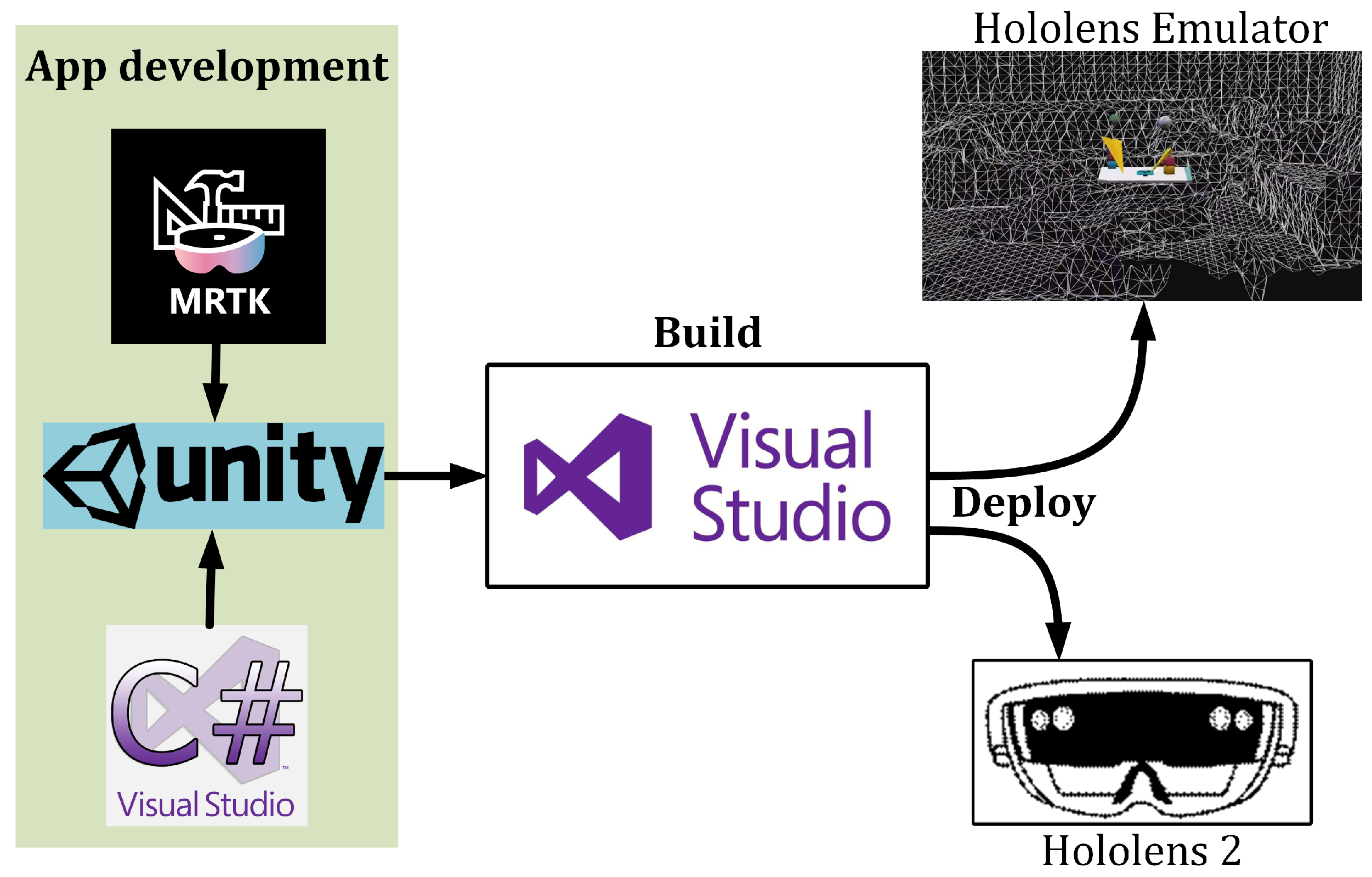
3.2.2. Unity and Visual Studio
3.2.3. Mixed Reality ToolKit (MRTK)
3.3. Gamification
4. Event Sequence
4.1. Game Creation and Launch
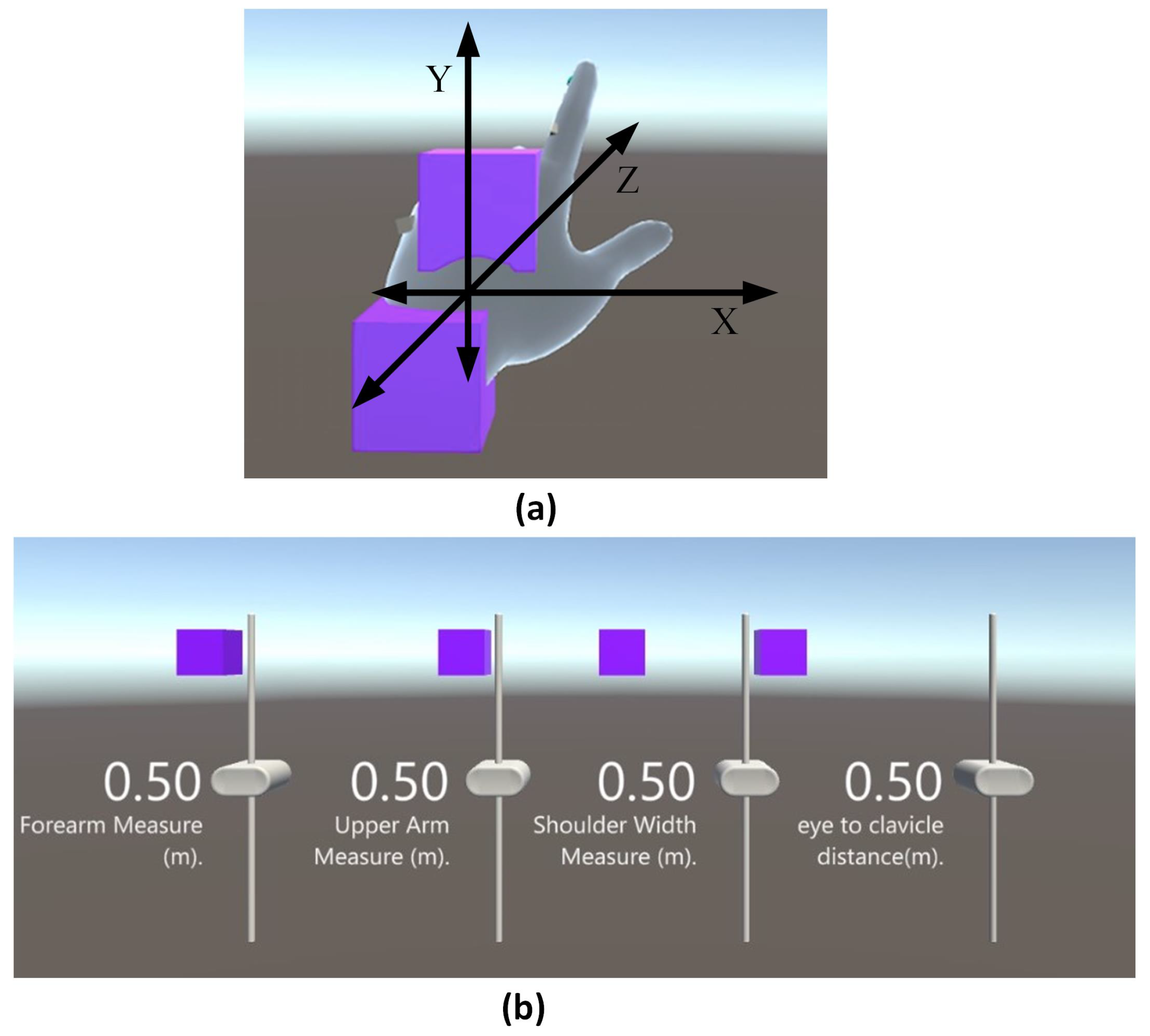
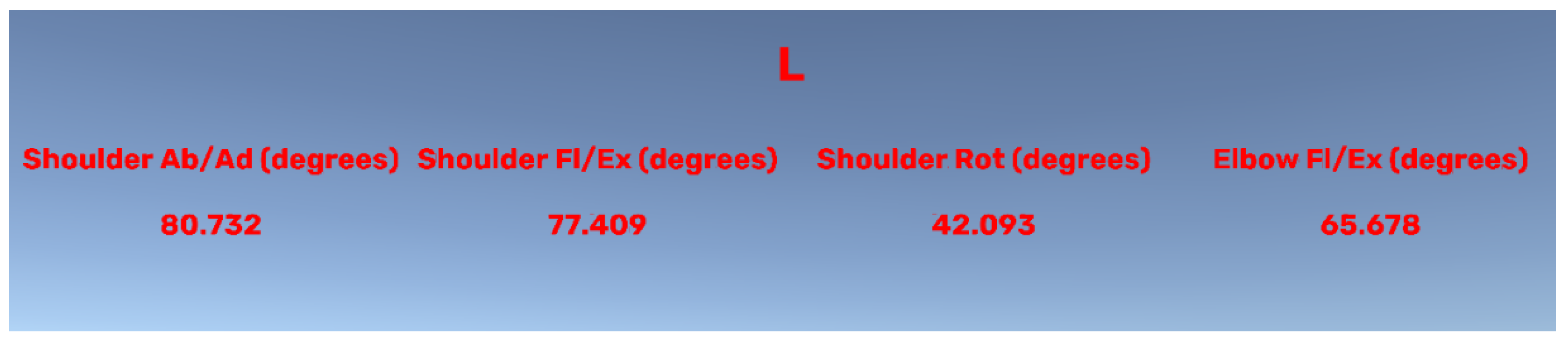
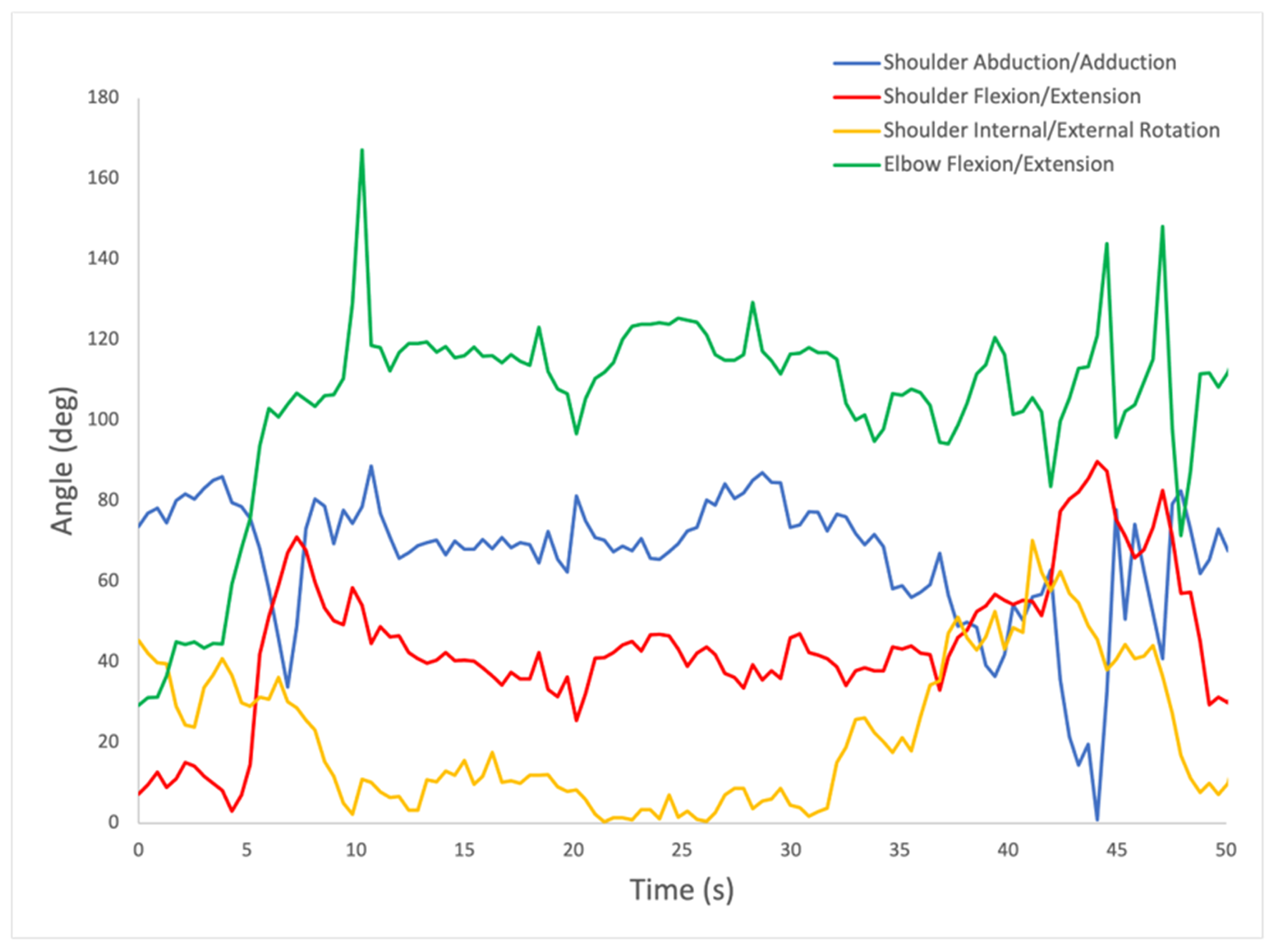
4.2. Upper Extremity Joint Measurement
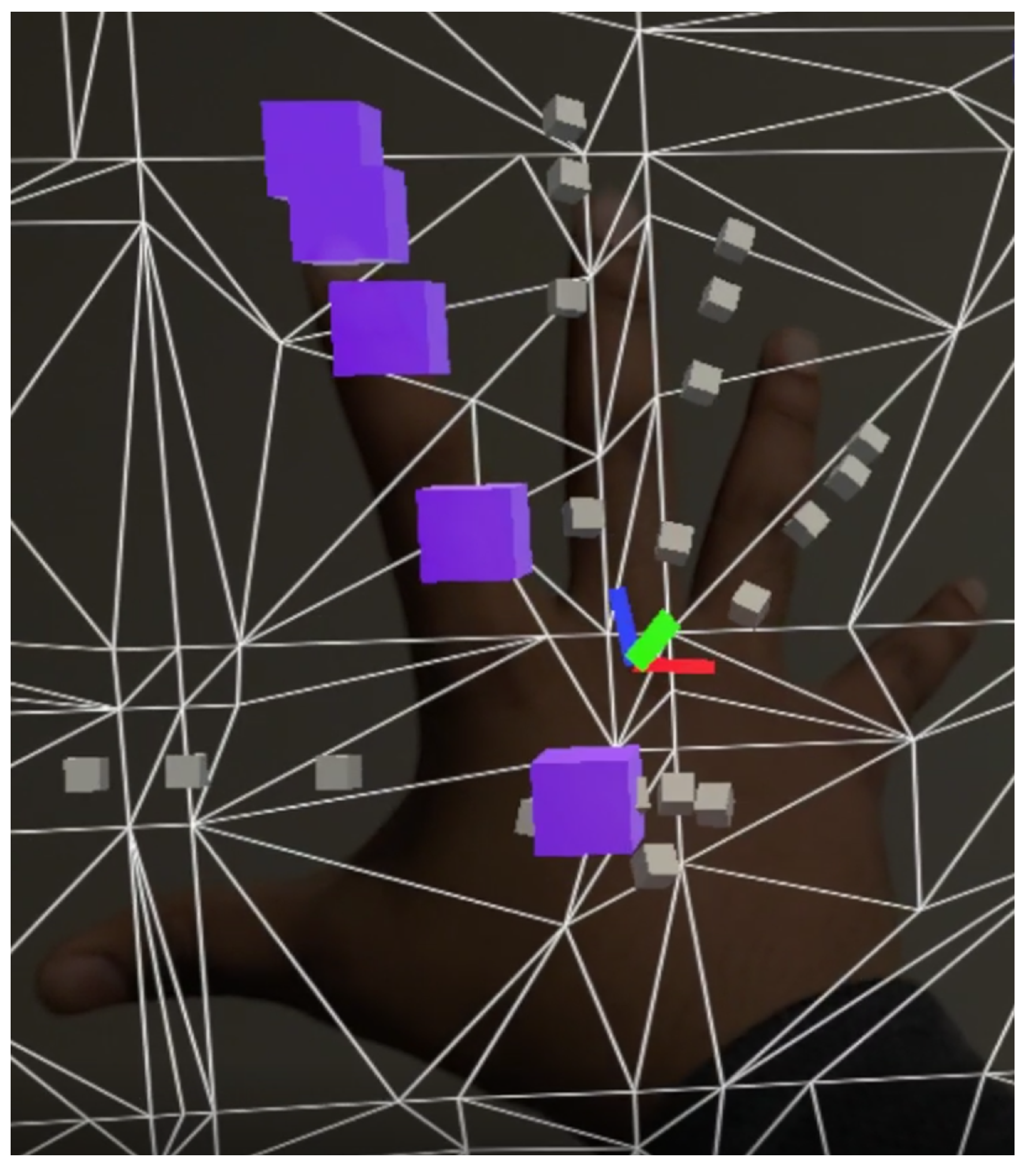
4.3. Finger and Wrist Joint Measurement
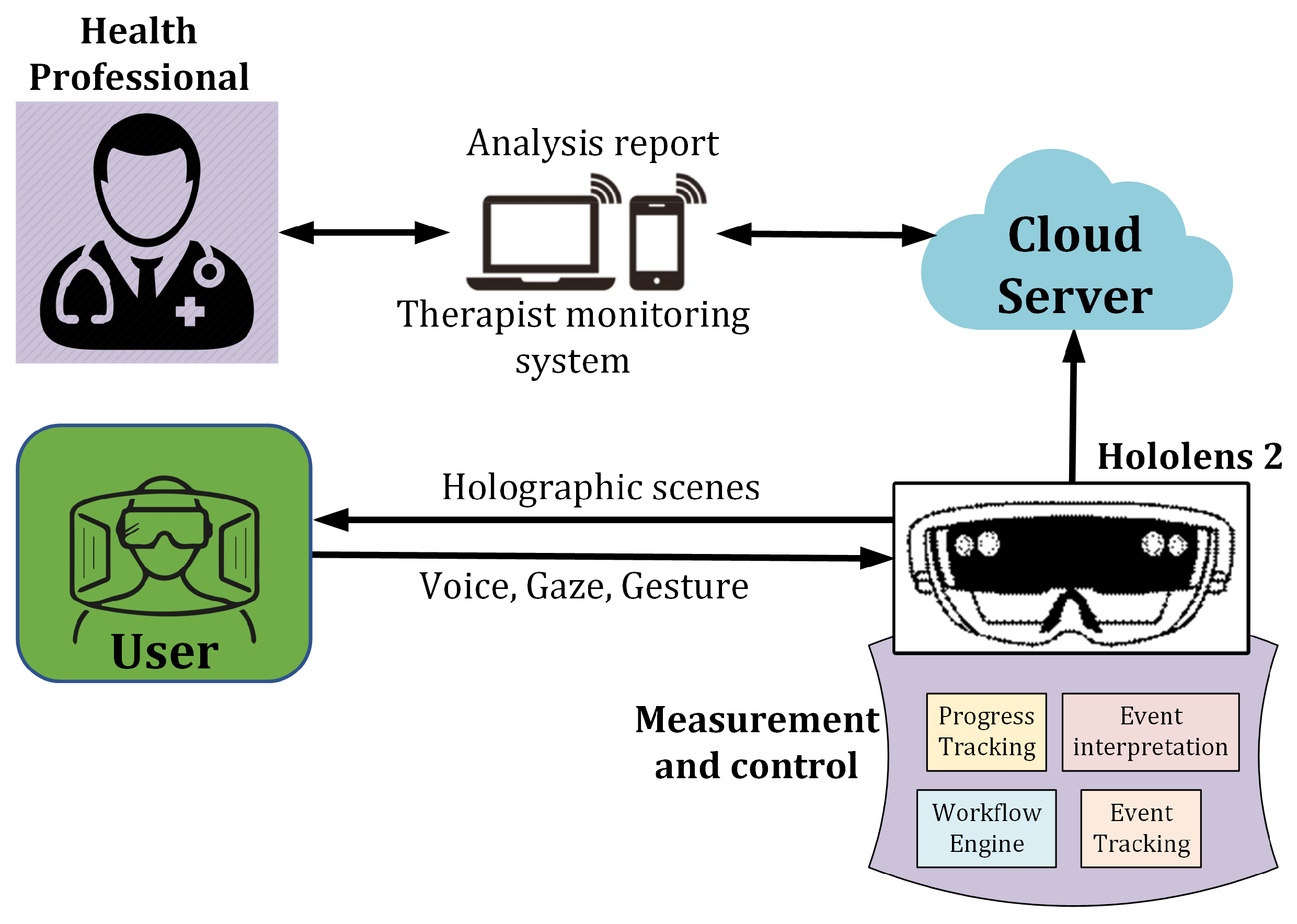
4.4. Data Transfer
5. Experiments and Results
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| UE | Upper Extremity |
| VR | Virtual Reality |
| AR | Augmented Reality |
| MR | Mixed Reality |
| OT | Occupational Therapists |
| IMUs | Inertial Measurement Units |
| sEMG | Surface Electromyography |
| RCT | Randomized Controlled Trial |
| ARAT | Action Research Arm Test |
| WMFT | Wolf Motor Function Test |
| LMC | Leap Motion Controller |
| FMA-UE | Fugl–Meyer Assessment-Upper Extremity |
| VRTE | VR-based Therapeutic Exercise |
| ADL | Activity of Daily Living |
| VT | Virtual Therapy |
| BRS | Brunnstrom Recovery Stage |
| BI | Barthel Index |
| UI | User Interface |
| ROM | Range of Motion |
| DoFs | Degrees of Freedom |
References
- Gideroğlu, K.; Sağlam, İ.; Çakıcı, H.; Özturan, K.; Güven, M.; Görgü, M. Epidemiology of the hand injuries in Bolu region: A retrospective clinical study. Abant. Med. J. 2012, 1, 13–15. [Google Scholar] [CrossRef]
- Upper Extremity Injury. 2022. Available online: https://www.jonathanohebmd.com/services/upper-extremity-injury (accessed on 23 October 2022).
- Jaggi, A.; Alexander, S. Suppl-6, M13: Rehabilitation for shoulder instability–current approaches. Open Orthop. J. 2017, 11, 957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenah, K.; Bernhardt, J.; Cumming, T.; Spratt, N.; Luker, J.; Janssen, H. Boredom in patients with acquired brain injuries during inpatient rehabilitation: A scoping review. Disabil. Rehabil. 2018, 40, 2713–2722. [Google Scholar] [CrossRef]
- Maceira-Elvira, P.; Popa, T.; Schmid, A.C.; Hummel, F.C. Wearable technology in stroke rehabilitation: Towards improved diagnosis and treatment of upper-limb motor impairment. J. Neuroeng. Rehabil. 2019, 16, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Smiderle, R.; Rigo, S.J.; Marques, L.B.; Peçanha de Miranda Coelho, J.A.; Jaques, P.A. The impact of gamification on students’ learning, engagement and behavior based on their personality traits. Smart Learn. Environ. 2020, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Held, J.P.O.; Yu, K.; Pyles, C.; Veerbeek, J.M.; Bork, F.; Heining, S.M.; Navab, N.; Luft, A.R. Augmented reality–based rehabilitation of gait impairments: Case report. JMIR mHealth uHealth 2020, 8, e17804. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Or, C.K.; Chen, T. Effectiveness of Using Virtual Reality–Supported Exercise Therapy for Upper Extremity Motor Rehabilitation in Patients with Stroke: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2022, 24, e24111. [Google Scholar] [CrossRef] [PubMed]
- Aguilera-Rubio, Á.; Cuesta-Gómez, A.; Mallo-López, A.; Jardón-Huete, A.; Oña-Simbaña, E.D.; Alguacil-Diego, I.M. Feasibility and Efficacy of a Virtual Reality Game-Based Upper Extremity Motor Function Rehabilitation Therapy in Patients with Chronic Stroke: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 3381. [Google Scholar] [CrossRef]
- Valentin, L.S.S. Can Digital Games Be a Way of Improving the Neuroplasticity in Stroke Damage? Can the Adult Brain Grow New Cells or Rewire Itself in Response to a New Experience? Open J. Med. Psychol. 2017, 6, 153–165. [Google Scholar] [CrossRef] [Green Version]
- Leong, S.C.; Tang, Y.M.; Toh, F.M.; Fong, K.N. Examining the effectiveness of virtual, augmented, and mixed reality (VAMR) therapy for upper limb recovery and activities of daily living in stroke patients: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2022, 19, 1–20. [Google Scholar] [CrossRef]
- Phan, H.L.; Le, T.H.; Lim, J.M.; Hwang, C.H.; Koo, K.i. Effectiveness of augmented reality in stroke rehabilitation: A Meta-Analysis. Appl. Sci. 2022, 12, 1848. [Google Scholar] [CrossRef]
- Fang, Z.; Wu, T.; Lv, M.; Chen, M.; Zeng, Z.; Qian, J.; Chen, W.; Jiang, S.; Zhang, J. Effect of traditional plus virtual reality rehabilitation on prognosis of stroke survivors: A systematic review and meta-analysis of randomized controlled trials. Am. J. Phys. Med. Rehabil. 2022, 101, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Faria, A.L.; Cameirão, M.S.; Couras, J.F.; Aguiar, J.R.; Costa, G.M.; Bermúdez i Badia, S. Combined cognitive-motor rehabilitation in virtual reality improves motor outcomes in chronic stroke–a pilot study. Front. Psychol. 2018, 9, 854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miclaus, R.; Roman, N.; Caloian, S.; Mitoiu, B.; Suciu, O.; Onofrei, R.R.; Pavel, E.; Neculau, A. Non-Immersive virtual reality for post-stroke upper extremity rehabilitation: A small cohort randomized trial. Brain Sci. 2020, 10, 655. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Bird, M.L.; Muthalib, M.; Teo, W.P. An innovative STRoke Interactive Virtual thErapy (STRIVE) online platform for community-dwelling stroke survivors: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2020, 101, 1131–1137. [Google Scholar] [CrossRef]
- Kim, W.S.; Cho, S.; Park, S.H.; Lee, J.Y.; Kwon, S.; Paik, N.J. A low cost kinect-based virtual rehabilitation system for inpatient rehabilitation of the upper limb in patients with subacute stroke: A randomized, double-blind, sham-controlled pilot trial. Medicine 2018, 97, e11173. [Google Scholar] [CrossRef]
- Thielbar, K.O.; Triandafilou, K.M.; Barry, A.J.; Yuan, N.; Nishimoto, A.; Johnson, J.; Stoykov, M.E.; Tsoupikova, D.; Kamper, D.G. Home-based upper extremity stroke therapy using a multiuser virtual reality environment: A randomized trial. Arch. Phys. Med. Rehabil. 2020, 101, 196–203. [Google Scholar] [CrossRef]
- KESKİN, Y.; Atci, A.; Urkmez, B.; Akgul, Y.; Ozaras, N.; Aydin, T. Efficacy of a video-based physical therapy and rehabilitation system in patients with post-stroke hemiplegia: A randomized, controlled, pilot study. Turkish J. Geriatr.-Turk Geriatr. Derg. 2020, 23, 118–128. [Google Scholar] [CrossRef]
- Fong, K.N.; Tang, Y.M.; Sie, K.; Yu, A.K.; Lo, C.C.; Ma, Y.W. Task-specific virtual reality training on hemiparetic upper extremity in patients with stroke. Virtual Real. 2022, 26, 453–464. [Google Scholar] [CrossRef]
- Lee, M.M.; Lee, K.J.; Song, C.H. Game-based virtual reality canoe paddling training to improve postural balance and upper extremity function: A preliminary randomized controlled study of 30 patients with subacute stroke. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 2590. [Google Scholar] [CrossRef]
- Choi, D.; Choi, W.; Lee, S. Influence of Nintendo Wii Fit balance game on visual perception, postural balance, and walking in stroke survivors: A pilot randomized clinical trial. Games Health J. 2018, 7, 377–384. [Google Scholar] [CrossRef]
- Kim, J.H. Effects of a virtual reality video game exercise program on upper extremity function and daily living activities in stroke patients. J. Phys. Ther. Sci. 2018, 30, 1408–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.y.; Song, E.; Moon, J.H.; Hahm, S.C. Effects of Virtual Reality Based Therapeutic Exercise on the Upper Extremity Function and Activities of Daily Living in Patients with Acute Stroke: A Pilot Randomized Controlled Trial. Med.-Leg. Update 2021, 21, 676–682. [Google Scholar]
- Oh, Y.B.; Kim, G.W.; Han, K.S.; Won, Y.H.; Park, S.H.; Seo, J.H.; Ko, M.H. Efficacy of virtual reality combined with real instrument training for patients with stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2019, 100, 1400–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, M.A.; Singh, D.K.A.; Mohd Nordin, N.A.; Hooi Nee, K.; Ibrahim, N. Virtual reality games as an adjunct in improving upper limb function and general health among stroke survivors. Int. J. Environ. Res. Public Health 2019, 16, 5144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiper, P.; Szczudlik, A.; Agostini, M.; Opara, J.; Nowobilski, R.; Ventura, L.; Tonin, P.; Turolla, A. Virtual reality for upper limb rehabilitation in subacute and chronic stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2018, 99, 834–842. [Google Scholar] [CrossRef]
- Abd El-Kafy, E.M.; Alshehri, M.A.; El-Fiky, A.A.R.; Guermazi, M.A. The effect of virtual reality-based therapy on improving upper limb functions in individuals with stroke: A randomized control trial. Front. Aging Neurosci. 2021, 13, 731343. [Google Scholar] [CrossRef]
- Cuesta-Gómez, A.; Sánchez-Herrera-Baeza, P.; Oña-Simbaña, E.D.; Martínez-Medina, A.; Ortiz-Comino, C.; Balaguer-Bernaldo-de Quirós, C.; Jardón-Huete, A.; Cano-de-la Cuerda, R. Effects of virtual reality associated with serious games for upper limb rehabilitation in patients with multiple sclerosis: Randomized controlled trial. J. Neuroeng. Rehabil. 2020, 17, 1–10. [Google Scholar] [CrossRef]
- Afsar, S.I.; Mirzayev, I.; Yemisci, O.U.; Saracgil, S.N.C. Virtual reality in upper extremity rehabilitation of stroke patients: A randomized controlled trial. J. Stroke Cerebrovasc. Dis. 2018, 27, 3473–3478. [Google Scholar] [CrossRef]
- Aşkın, A.; Atar, E.; Koçyiğit, H.; Tosun, A. Effects of Kinect-based virtual reality game training on upper extremity motor recovery in chronic stroke. Somatosens. Mot. Res. 2018, 35, 25–32. [Google Scholar] [CrossRef]
- Ain, Q.U.; Khan, S.; Ilyas, S.; Yaseen, A.; Tariq, I.; Liu, T.; Wang, J. Additional effects of Xbox kinect training on upper limb function in chronic stroke patients: A randomized control trial. Healthcare 2021, 9, 242. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Peris, C.; Fuertes-Kenneally, L.; Vetrovsky, T.; Sarabia, J.M.; Climent-Paya, V.; Manresa-Rocamora, A. Effects of Exergaming in Patients with Cardiovascular Disease Compared to Conventional Cardiac Rehabilitation: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 3492. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, L.V.; Nichols-Larsen, D.S.; Uswatte, G.; Strahl, N.; Simeo, M.; Proffitt, R.; Kelly, K.; Crawfis, R.; Taub, E.; Morris, D.; et al. Video game rehabilitation for outpatient stroke (VIGoROUS): A multi-site randomized controlled trial of in-home, self-managed, upper-extremity therapy. EClinicalMedicine 2022, 43, 101239. [Google Scholar] [CrossRef]
- Malick, W.H.; Butt, R.; Awan, W.A.; Ashfaq, M.; Mahmood, Q. Effects of Augmented Reality Interventions on the Function of Upper Extremity and Balance in Children with Spastic Hemiplegic Cerebral Palsy: A Randomized Clinical Trial. Front. Neurol. 2022, 13, 895055. [Google Scholar] [CrossRef] [PubMed]
- HoloLens 2—Overview, Features, and Specs|Microsoft HoloLens. 2022. Available online: https://www.microsoft.com/en-us/hololens/hardware] (accessed on 23 October 2022).
- Technologies. Unity. 2022. Available online: https://unity.com (accessed on 23 October 2022).
- Visual Studio: IDE and Code Editor for Software Developers and Teams. 2022. Available online: https://visualstudio.microsoft.com (accessed on 23 October 2022).
- Microsoft. MRTK2-Unity Developer Documentation—MRTK 2. 2022. Available online: https://learn.microsoft.com/en-us/windows/mixed-reality/mrtk-unity/mrtk2/?view=mrtkunity-2022-05 (accessed on 23 October 2022).
- Technologies, U. Unity-Scripting API: Ray. 2022. Available online: https://docs.unity3d.com/ScriptReference/Ray.html (accessed on 22 October 2022).
- Faity, G.; Mottet, D.; Froger, J. Validity and reliability of Kinect v2 for quantifying upper body kinematics during seated reaching. Sensors 2022, 22, 2735. [Google Scholar] [CrossRef]
- Milosevic, B.; Leardini, A.; Farella, E. Kinect and wearable inertial sensors for motor rehabilitation programs at home: State of the art and an experimental comparison. Biomed. Eng. Online 2020, 19, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Ma, M.; Proffitt, R.; Skubic, M. Validation of a Kinect V2 based rehabilitation game. PLoS ONE 2018, 13, e0202338. [Google Scholar] [CrossRef]
- Assad-Uz-Zaman, M.; Islam, M.R.; Miah, S.; Rahman, M.H. NAO robot for cooperative rehabilitation training. J. Rehabil. Assist. Technol. Eng. 2019, 6, 2055668319862151. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
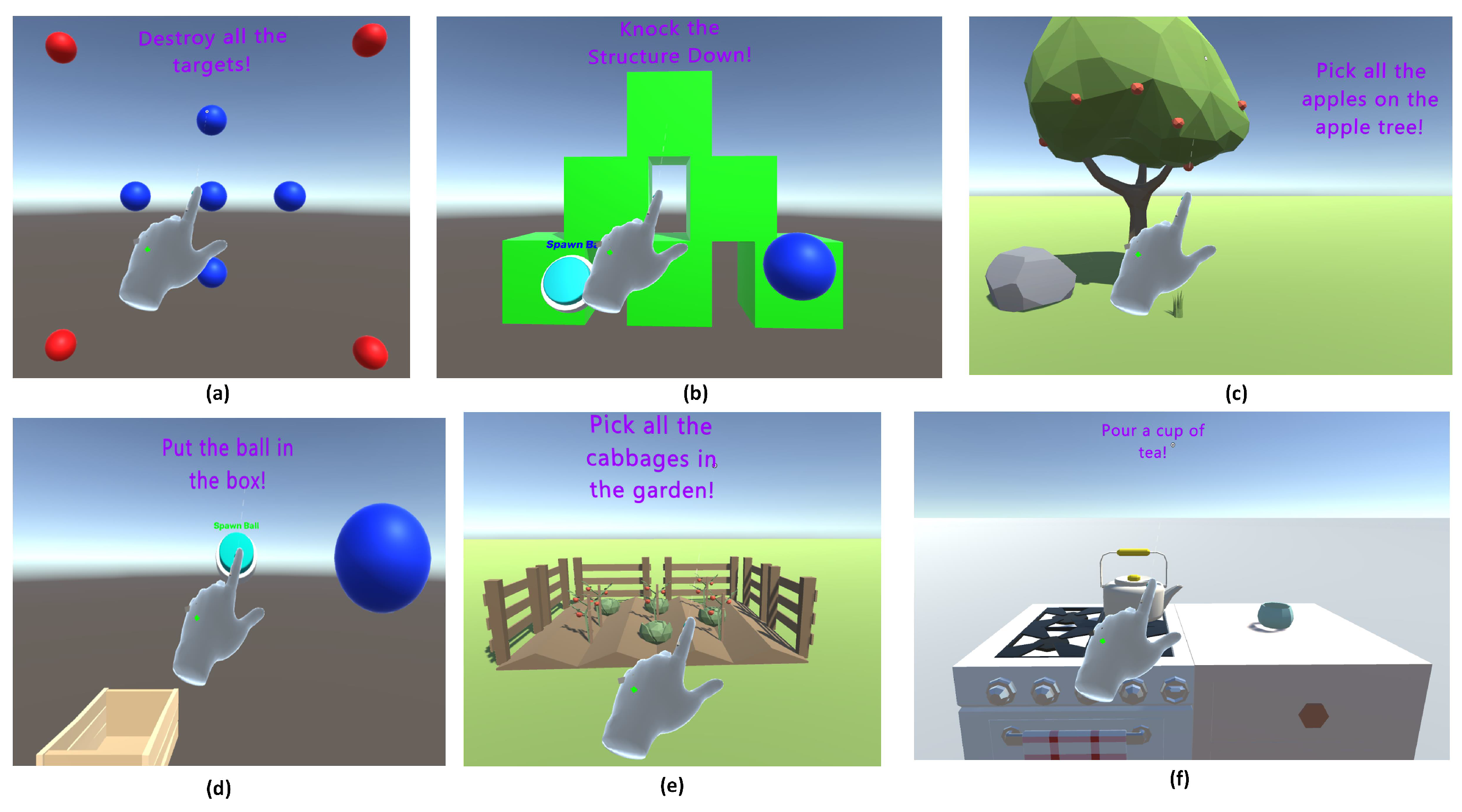
| Game Level | Main Focus Area | DoFs | ROM Covered (Degrees) | Difficulty |
|---|---|---|---|---|
| Destroy all the spheres | Shoulder | Flexion/extension and abduction/adduction | 0–100 | Medium |
| Knock down the structures | Shoulder and Elbow | Elbow flexion/extension, shoulder flexion/extension, and shoulder abduction/adduction | 0–150 (Elbow), 0–120 (Shoulder) | Hard |
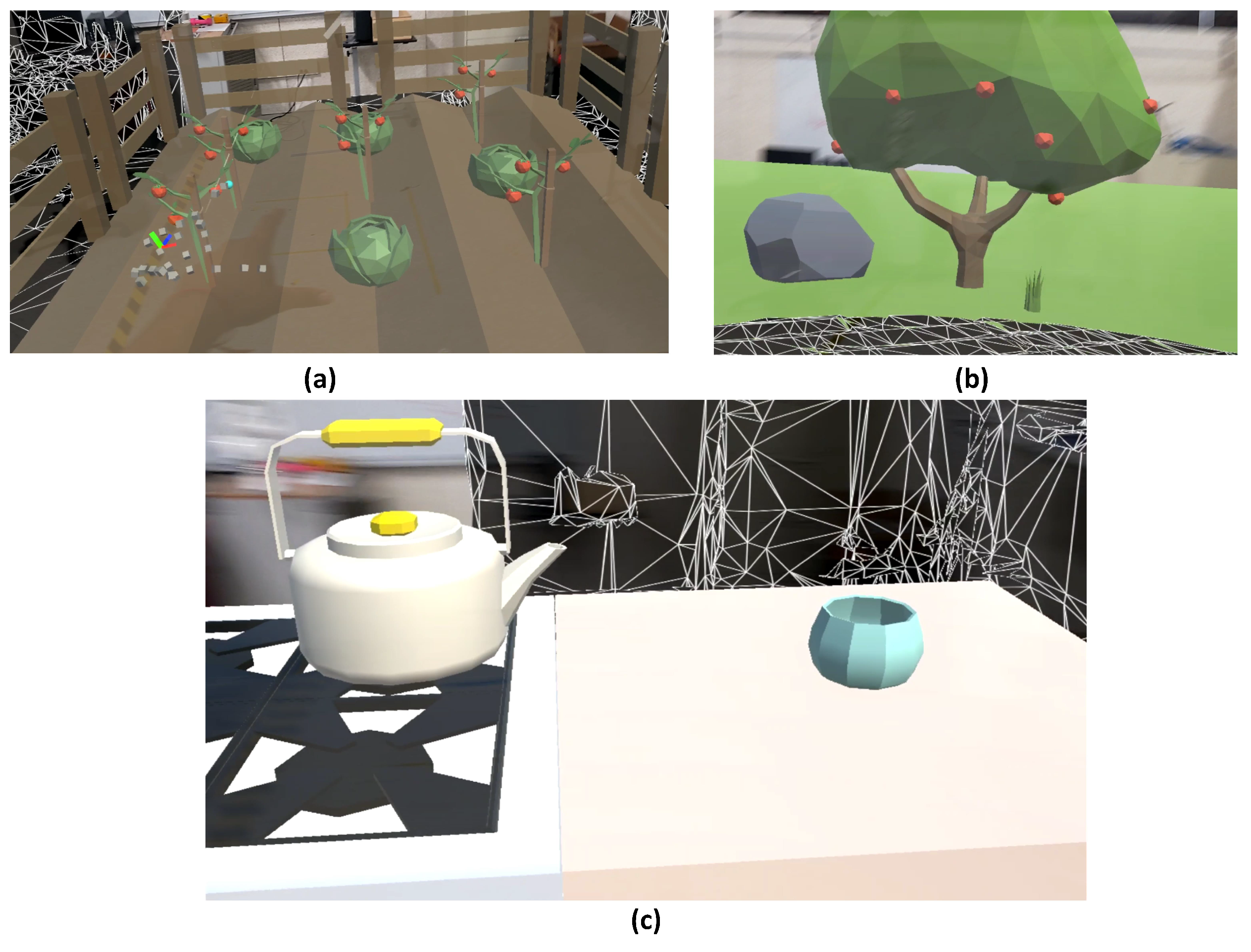
| Picking apples from a tree | Shoulder | Flexion/extension and abduction/adduction | 0–150 | Hard |
| Picking cabbages in the garden | Shoulder | Flexion/extension and abduction/adduction | 0–60 | Easy |
| Select the spheres in the order of the rainbow | Shoulder | Flexion/extension and abduction/adduction | 0–100 | Medium |
| Pour a cup of tea | Shoulder and Elbow | Elbow flexion/extension, and shoulder rotation | 0–50 (Elbow), 0–30 (Shoulder) | Easy |
| Put the ball in the box | Wrist and finger | Wrist flexion/extension, wrist abduction/adduction, and finger flexion/extension | −50–50 (Wrist flexion/extension), −30–30 (Wrist abduction/adduction), 0–60 (Finger flexion/extension) | Hard |
| Range of Motion | Shoulder Abduction/Adduction | Shoulder Flexion/Extension | Shoulder Internal/External Rotation | Elbow Flexion/Extension |
|---|---|---|---|---|
| p-Value | 0.82 | 0.25 | 0.19 | 0.14 |
| Item | Criteria | Questions | Avg. Score |
|---|---|---|---|
| (n = 12) | |||
| 1 | Usability | I think the MR Game is easy to use. | 4.64 |
| 2 | Functionality | I think the functionalities of the MR Game are well integrated | 4.57 |
| 3 | Learnability | I think the most users can quickly learn to use the MR Game | 4.68 |
| 4 | Motivation | I am confident when using the MR Game | 4.8 |
| 5 | Comfortability | I would like to use the MR Game on a daily basis | 4.78 |
| 6 | Overall Satisfaction | How do you rate the MR game? | 4.72 |
| 7 | OT Assessment | (i) How do you rate the comfort of using the MR Game? | 4.88 |
| (ii) How do you rate the accuracy of the MR Game’s capabilities for measuring the shoulder’s flexion/extension ROM? | 4.83 | ||
| (iii) How do you rate the accuracy of the MR Game’s capabilities for measuring the shoulder’s abduction/adduction ROM? | 4.89 | ||
| (iv) How do you rate the accuracy of the MR Game’s capabilities for measuring the shoulder’s internal/external rotation ROM? | 4.60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pillai, A.; Sunny, M.S.H.; Shahria, M.T.; Banik, N.; Rahman, M.H. Gamification of Upper Limb Rehabilitation in Mixed-Reality Environment. Appl. Sci. 2022, 12, 12260. https://doi.org/10.3390/app122312260
Pillai A, Sunny MSH, Shahria MT, Banik N, Rahman MH. Gamification of Upper Limb Rehabilitation in Mixed-Reality Environment. Applied Sciences. 2022; 12(23):12260. https://doi.org/10.3390/app122312260
Chicago/Turabian StylePillai, Aditya, Md Samiul Haque Sunny, Md Tanzil Shahria, Nayan Banik, and Mohammad Habibur Rahman. 2022. "Gamification of Upper Limb Rehabilitation in Mixed-Reality Environment" Applied Sciences 12, no. 23: 12260. https://doi.org/10.3390/app122312260
APA StylePillai, A., Sunny, M. S. H., Shahria, M. T., Banik, N., & Rahman, M. H. (2022). Gamification of Upper Limb Rehabilitation in Mixed-Reality Environment. Applied Sciences, 12(23), 12260. https://doi.org/10.3390/app122312260