
Effectiveness of Augmented Reality in Stroke Rehabilitation: A Meta-Analysis



Abstract
:1. Introduction
2. Methods
2.1. Objective
2.2. Search Strategy
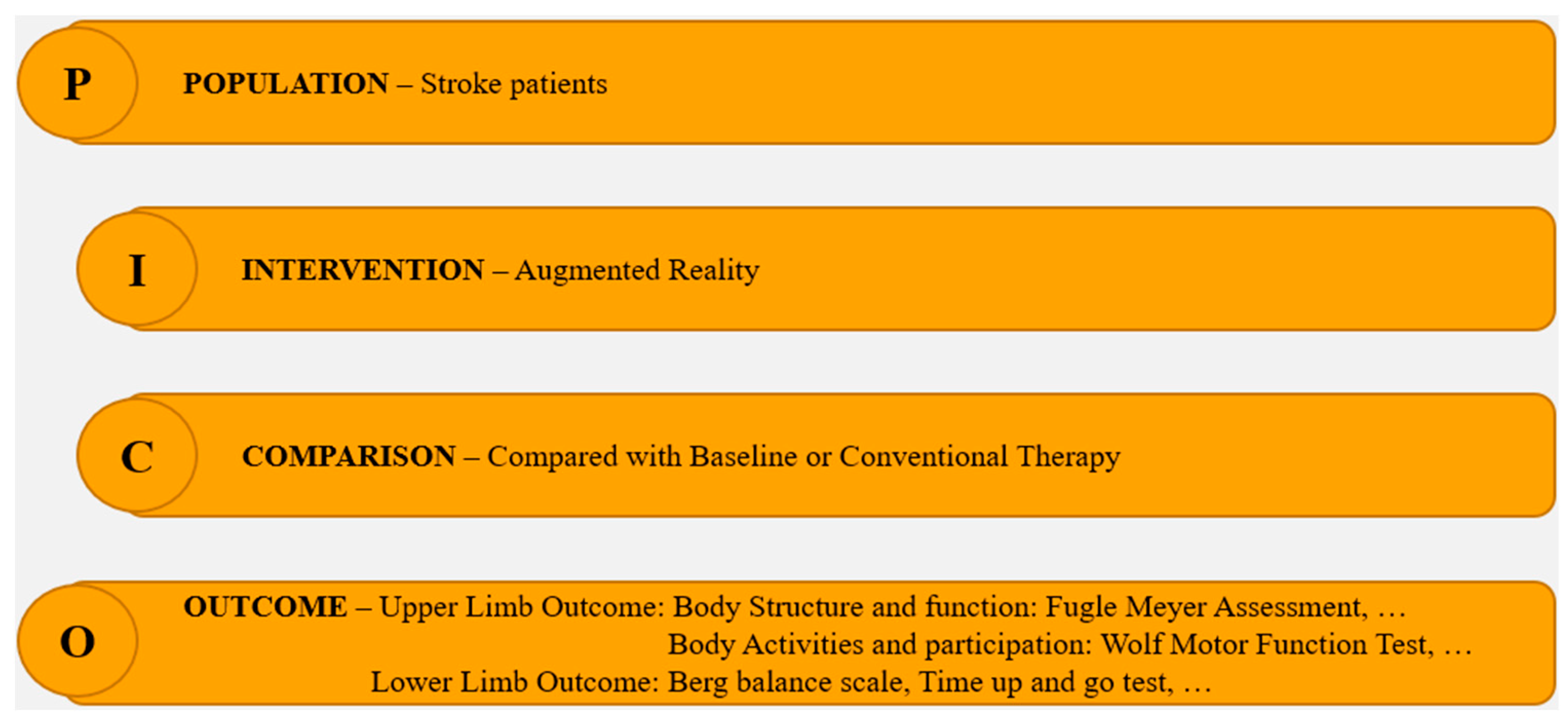
2.3. Inclusion Criteria
2.4. Exclusion Criteria
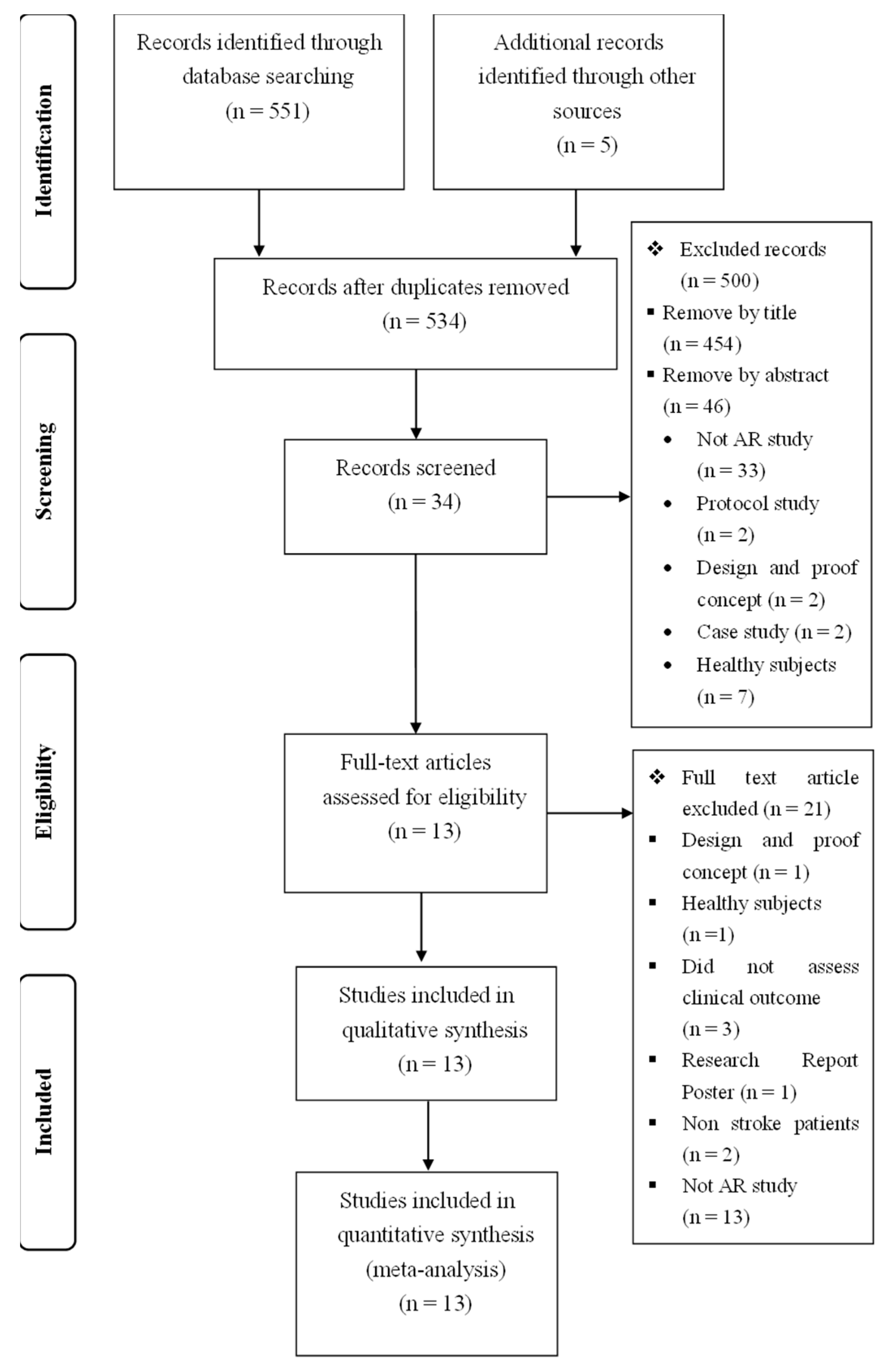
2.5. Study Selection
2.6. Data Extraction
2.7. Type of Outcome Measures
2.8. Studies Quality Assessment
2.9. Quantitative Analysis
3. Results and Discussion
3.1. AR Technique Overview
3.1.1. AR Technique for Upper Limb Rehabilitation
3.1.2. AR Technique for Lower Limb Function
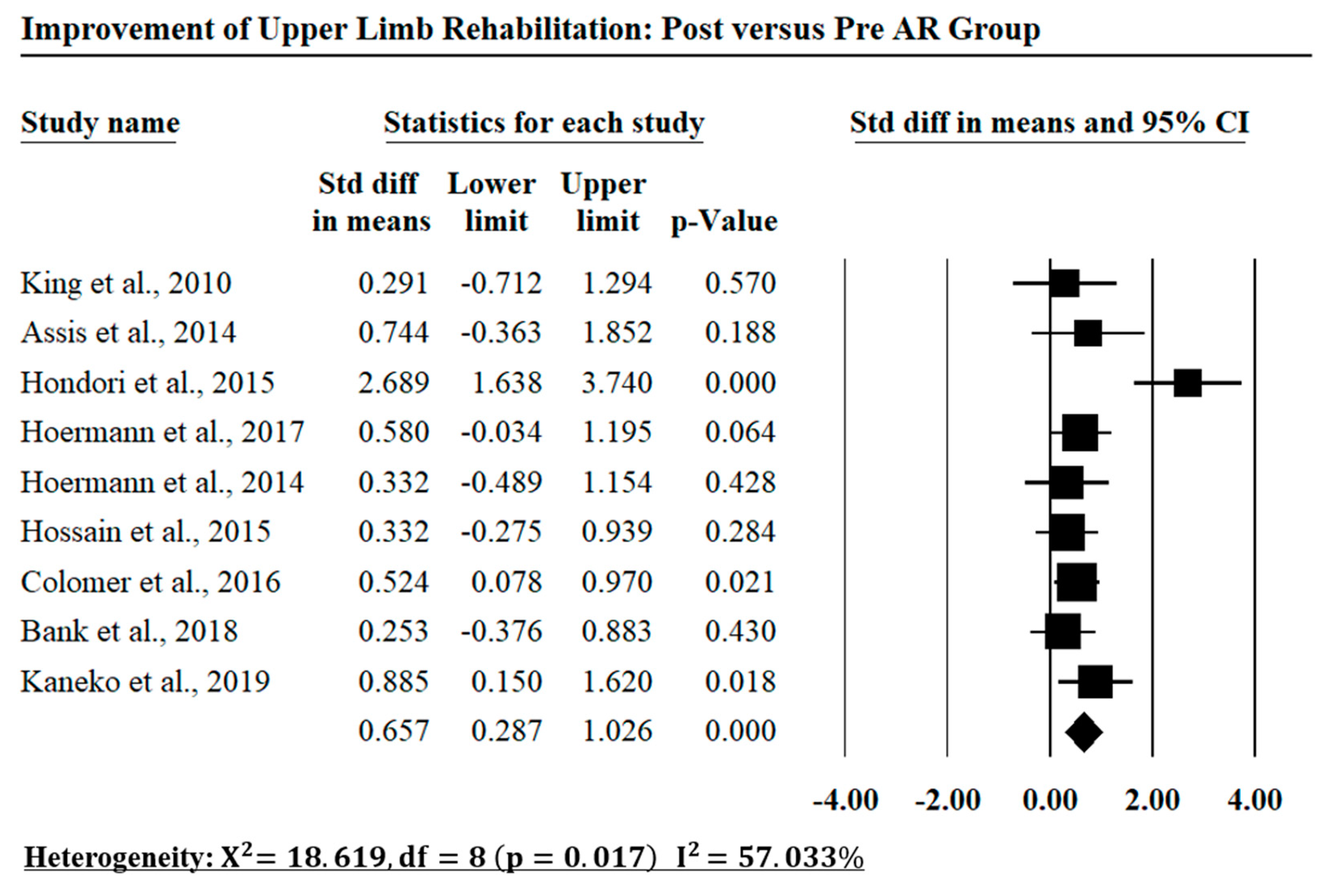
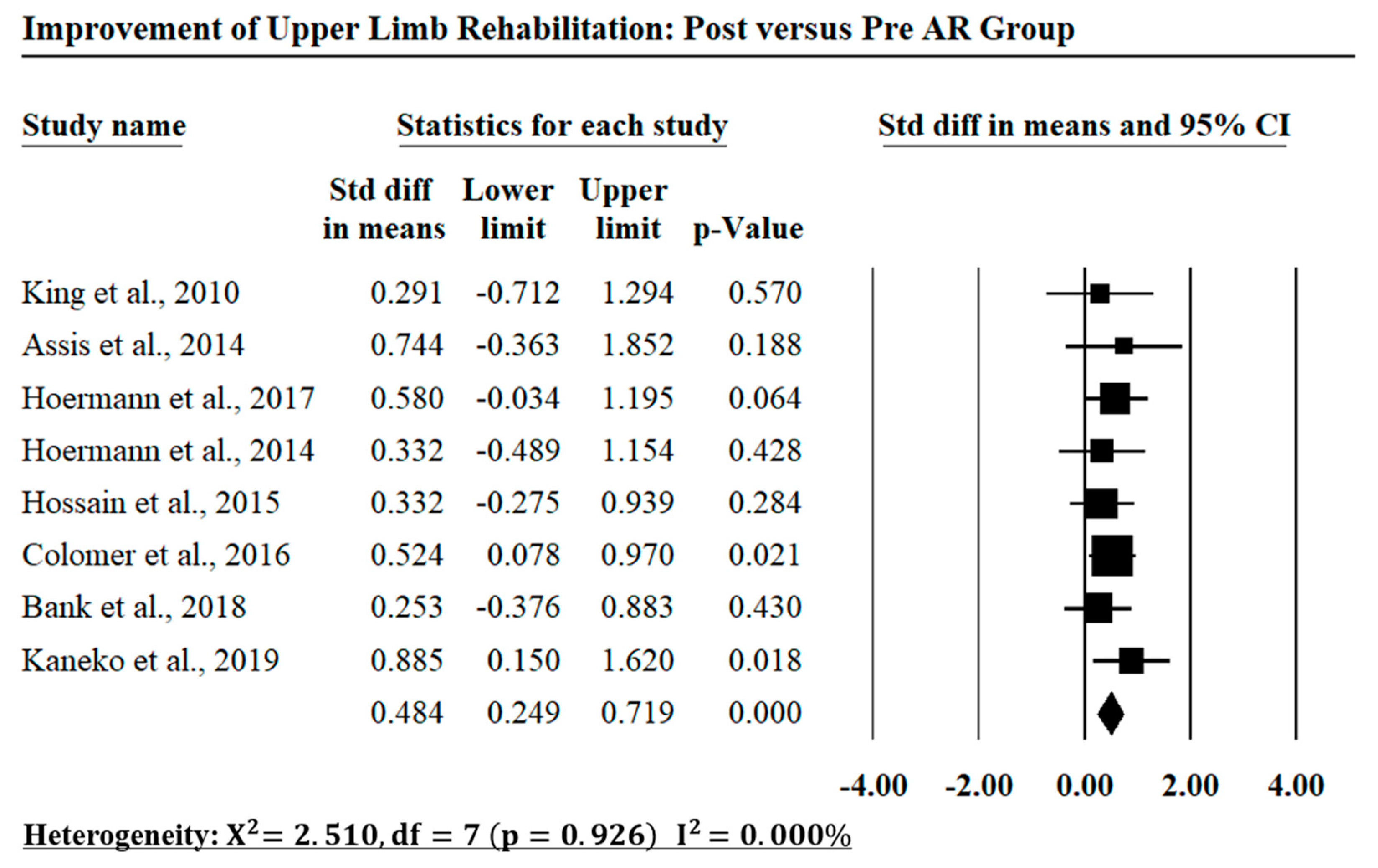
3.2. Evaluation
3.3. Comparison with the Literature
3.4. Potential Implications for Clinicians
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Association, A.H. Heart Disease and Stroke Statistics—2006 Update. Circulation 2006, 113, e85–e151. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. World Report on Disability; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Lunde, L.-K.; Koch, M.; Knardahl, S.; Wærsted, M.; Mathiassen, S.E.; Forsman, M.; Holtermann, A.; Veiersted, K.B. Musculoskeletal health and work ability in physically demanding occupations study protocol for a prospective field study on construction and health care workers. BMC Public Health 2014, 14, 1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatterji, S.; Byles, J.; Cutler, D.; Seeman, T.; Verdes, E. Health, functioning, and disability in older adults—present status and future implications. Lancet 2015, 385, 563–575. [Google Scholar] [CrossRef] [Green Version]
- Hanssen, J.-I.; Lindqvist, R. Rehabilitation; Concepts, Practices and Research. Scand. J. Disabil. Res. 2003, 5, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Borich, M.R.; Wolf, S.L.; Tan, A.Q.; Palmer, J.A. Targeted Neuromodulation of Abnormal Interhemispheric Connectivity to Promote Neural Plasticity and Recovery of Arm Function after Stroke: A Randomized Crossover Clinical Trial Study Protocol. Neural Plast. 2018, 2018, 9875326. [Google Scholar] [CrossRef] [Green Version]
- Alia, C.; Spalletti, C.; Lai, S.; Panarese, A.; Lamola, G.; Bertolucci, F.; Vallone, F.; Di Garbo, A.; Chisari, C.; Micera, S.; et al. Neuroplastic Changes Following Brain Ischemia and their Contribution to Stroke Recovery: Novel Approaches in Neurorehabilitation. Front. Cell. Neurosci. 2017, 11, 1–22. [Google Scholar] [CrossRef]
- Mehta, U.M.; Keshavan, M.S. Cognitive Rehabilitation and Modulating Neuroplasticity with Brain Stimulation: Promises and Challenges. J. Psychosoc. Rehabil. Ment. Health 2015, 2, 5–7. [Google Scholar] [CrossRef]
- Huang, L.L.; Lee, C.F.; Hsieh, C.L.; Chen, M.H. Upper extremity rehabilitation equipment for stroke patients in Taiwan: Usage problems and improvement needs. Occup. Ther. Int. 2013, 20, 205–214. [Google Scholar] [CrossRef]
- Druzbicki, M.; Przysada, G.; Guzik, A.; Brzozowska-Magon, A.; Kolodziej, K.; Wolan-Nieroda, A.; Majewska, J.; Kwolek, A. The Efficacy of Gait Training Using a Body Weight Support Treadmill and Visual Biofeedback in Patients with Subacute Stroke: A Randomized Controlled Trial. BioMed Res. Int. 2018, 2018, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Bickerton, W.L.; Humphreys, G.W.; Riddoch, J.M. The use of memorised verbal scripts in the rehabilitation of action disorganisation syndrome. Neuropsychol. Rehabil. 2006, 16, 155–177. [Google Scholar] [CrossRef]
- Forde, E.M.E.; Humphreys, G.W. Dissociations in Routine Behaviour across Patients and Everyday Tasks. Neurocase 2002, 8, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Burdea, G. Virtual Rehabilitation-Benefits and Challenges. Methods Inf. Med. 2003, 42, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Azuma, R.; Baillot, Y.; Behringer, R.; Feiner, S.; Julier, S.; MacIntyre, B. Recent Advances in Augmented Reality. IEEE Comput. Graph. Appl. 2001, 21, 34–47. [Google Scholar] [CrossRef] [Green Version]
- Sigrist, R.; Rauter, G.; Riener, R.; Wolf, P. Augmented visual, auditory, haptic, and multimodal feedback in motor learning: A review. Psychon. Bull. Rev. 2013, 20, 21–53. [Google Scholar] [CrossRef] [Green Version]
- Da Gama, A.E.; Chaves, T.M.; Figueiredo, L.S.; Baltar, A.; Meng, M.; Navab, N.; Teichrieb, V.; Fallavollita, P. MirrARbilitation: A clinically-related gesture recognition interactive tool for an AR rehabilitation system. Comput. Methods Programs Biomed. 2016, 135, 105–114. [Google Scholar] [CrossRef]
- Tang, A.; Biocca, F. Comparing Differences in Presence during Social Interaction in Augmented Reality versus Virtual Reality Environments An Exploratory Study. In Proceedings of the PRESENCE 2004, Seventh Annual International Workshop on Presence, Valencia, Spain, 13–15 October 2004; pp. 204–207. [Google Scholar]
- Ong, S.K.; Shen, Y.; Zhang, J.; Nee, A.Y.C. Augmented Reality in Assistive Technology and Rehabilitation Engineering; Springer: New York, NY, USA, 2011; pp. 603–630. [Google Scholar] [CrossRef]
- Al-Issa, H.; Regenbrecht, H.; Hale, L. Augmented reality applications in rehabilitation to improve physical outcomes. Phys. Ther. Rev. 2012, 17, 16–28. [Google Scholar] [CrossRef]
- Rosanna Maria Viglialoro, S.C.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Review of the Augmented Reality Systems for Shoulder Rehabilitation. Information 2019, 10, 154. [Google Scholar] [CrossRef] [Green Version]
- Gorman, C.; Gustafsson, L.A.-O. The use of augmented reality for rehabilitation after stroke: A narrative review. Disabil. Rehabil. Assist. Technol. 2020, 1–9. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- WHO. The International Classification of Functioning, Disability and Health; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Aminov, A.A.-O.; Rogers, J.M.; Middleton, S.; Caeyenberghs, K.; Wilson, P.H. What do randomized controlled trials say about virtual rehabilitation in stroke? A systematic literature review and meta-analysis of upper-limb and cognitive outcomes. J. Neuroeng. Rehabil. 2018, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessmemt Criteria for Evaluating Primary Research Papers from a Variety of Fields; Institute of Health Economics: Dhaka, AB, Canada, 2004. [Google Scholar]
- King, M.; Hale, L.; Pekkari, A.; Persson, M.; Gregorsson, M.; Nilsson, M. An affordable, computerised, table-based exercise system for stroke survivors. Disabil. Rehabil. Assist. Technol. 2010, 5, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.S.; Hardy, S.; Alamri, A.; Alelaiwi, A.; Hardy, V.; Wilhelm, C. AR-based serious game framework for post-stroke rehabilitation. Multimed. Syst. 2015, 22, 659–674. [Google Scholar] [CrossRef]
- Mousavi Hondori, H.; Khademi, M.; Dodakian, L.; McKenzie, A.; Lopes, C.V.; Cramer, S.C. Choice of Human-Computer Interaction Mode in Stroke Rehabilitation. Neurorehabilit. Neural Repair 2015, 30, 258–265. [Google Scholar] [CrossRef] [Green Version]
- Bank, P.J.M.; Cidota, M.A.; Ouwehand, P.E.W.; Lukosch, S.G. Patient-Tailored Augmented Reality Games for Assessing Upper Extremity Motor Impairments in Parkinson's Disease and Stroke. J. Med. Syst. 2018, 42, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoermann, S.; Ferreira Dos Santos, L.; Morkisch, N.; Jettkowski, K.; Sillis, M.; Devan, H.; Kanagasabai, P.S.; Schmidt, H.; Kruger, J.; Dohle, C.; et al. Computerised mirror therapy with Augmented Reflection Technology for early stroke rehabilitation: Clinical feasibility and integration as an adjunct therapy. Disabil. Rehabil. 2017, 39, 1503–1514. [Google Scholar] [CrossRef]
- Hoermann, S.; Hale, L.; Winser, S.J.; Regenbrecht, H. Patient engagement and clinical feasibility of Augmented Reflection Technology for stroke rehabilitation. Int. J. Disabil. Hum. Dev. 2014, 13, 355–360. [Google Scholar] [CrossRef]
- Assis, G.A.; Correa, A.G.; Martins, M.B.; Pedrozo, W.G.; Lopes Rde, D. An augmented reality system for upper-limb post-stroke motor rehabilitation: A feasibility study. Disabil. Rehabil. Assist. Technol. 2014, 11, 521–528. [Google Scholar] [CrossRef]
- Colomer, C.; Llorens, R.; Noe, E.; Alcaniz, M. Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke. J. NeuroEng. Rehabil. 2016, 13, 521–528. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.H.; Lee, C.H.; Kim, H.J. A pilot study of augmented reality-based postural control training in stroke rehabilitation. Phys. Ther. Rehabil. Sci. 2014, 3, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-H.; Kim, Y.; Lee, B.-H. Augmented reality-based postural control training improves gait function in patients with stroke: Randomized controlled trial. Hong Kong Physiother. J. 2014, 32, 51–57. [Google Scholar] [CrossRef]
- Kim, I.C.; Lee, B.H. Effects of Augmented Reality with functional electric Stimulation on Muscle Strength, Balance and Gait of Stroke patients. J. Phys. Ther. Sci. 2012, 24, 755–762. [Google Scholar] [CrossRef] [Green Version]
- Jung, G.U.; Moon, T.H.; Park, G.W.; Lee, J.Y.; Lee, B.H. Use of Augmented Reality-Based Training with EMG-Triggered Functional Electric Stimulation in Stroke Rehabilitation. J. Phys. Ther. Sci. 2013, 25, 147–151. [Google Scholar] [CrossRef] [Green Version]
- Kaneko, F.; Shindo, K.; Yoneta, M.; Okawada, M.; Akaboshi, K.; Liu, M. A Case Series Clinical Trial of a Novel Approach Using Augmented Reality That Inspires Self-body Cognition in Patients With Stroke: Effects on Motor Function and Resting-State Brain Functional Connectivity. Front. Syst. Neurosci. 2019, 13, 76. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Propst, M.; Nelson, S.G. Reliability of the Fugl-Meyer Assessment of Sensorimotor Recovery Following Cerebrovascular Accident. Phys. Ther. 1982, 63, 1606–1610. [Google Scholar] [CrossRef]
- Woodbury, M.; Velozo, C.A.; Thompson, P.A.; Light, K.; Uswatte, G.; Taub, E.; Winstein, C.J.; Morris, D.; Blanton, S.; Nichols-Larsen, D.S.; et al. Measurement structure of the Wolf Motor Function Test: Implications for motor control theory. Neurorehabilit. Neural Repair 2010, 24, 791–801. [Google Scholar] [CrossRef] [Green Version]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of Manual Dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Koo, K.I.; Park, D.K.; Youm, Y.S.; Cho, S.D.; Hwang, C.A.-O. Enhanced Reality Showing Long-Lasting Analgesia after Total Knee Arthroplasty: Prospective, Randomized Clinical Trial. Sci. Rep. 2018, 8, 2343. [Google Scholar] [CrossRef] [Green Version]
- Phan, H.L.; Kim, J.P.; Kim, K.; Hwang, C.H.; Koo, K.-i. Wrist Rehabilitation System Using Augmented Reality for Hemiplegic Stroke Patient Rehabilitation: A Feasibility Study. Appl. Sci. 2019, 9, 2892. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | Search Syntax | No. of Articles |
|---|---|---|
| Web of Science | (Augmented Reality OR AR) AND (stroke OR Hemiplegia) AND (rehabilitation) AND (Upper Limb OR Upper Extremity OR Lower Limb OR Lower Extremity OR Gait and Balance) | 41 |
| Science Direct | (Augmented Reality OR AR) AND (stroke OR Hemiplegia) AND (rehabilitation) AND (Upper Limb OR Upper Extremity OR Lower Limb OR Lower Extremity OR Gait and Balance) | 339 |
| PubMed | (Augmented Reality OR AR) AND (stroke OR Hemiplegia) AND (rehabilitation) AND (Upper Limb OR Upper Extremity OR Lower Limb OR Lower Extremity OR Gait and Balance) | 53 |
| Embase | (Augmented Reality OR AR) AND (stroke OR Hemiplegia) AND (rehabilitation) AND (Upper Limb OR Upper Extremity OR Lower Limb OR Lower Extremity OR Gait and Balance) | 20 |
| SAGE Publication | (Augmented Reality OR AR) AND (stroke OR Hemiplegia) AND (rehabilitation) AND (Upper Limb OR Upper Extremity OR Lower Limb OR Lower Extremity OR Gait and Balance) | 98 |
| Author | AR Rehab System | Physiotherapy Application | Tracking Method | AR Interface |
|---|---|---|---|---|
| Marcus King et al. (2010) [26] | ARS | Shoulder elbow movements | Wearable marker-based AR/Fiducial markers (B/W pattern), IR Fiducial markers | Screen |
| Assis et al. (2014) [32] | NeuroR | Shoulder abduction–flexion, Shoulder horizontal flexion, Finger extension, Hand grasping | Wearable’s marker-based AR/Markerless AR/Fiducial markers (B/W pattern) | Projector/PC audio speakers |
| Hondori et al. (2015) [28] | A-based Fruit Ninja game | Hand movement/Shoulder movements | Non-wearable marker-based AR/Colored Fiducial markers | Projector/PC audio speakers |
| Hossain et al. (2015) [27] | AR-REHAB | Hand movement/Wrist movement | Fiducial markers | Screen |
| Hoermann et al. (2017) [30] | ART | Fingers extension/Wrist flexion/extension | Markerless AR | Screen/ |
| Colomer et al. (2016) [33] | AR System | Wrist flexion–extension/Elbow flexion–extension/Finger flexion–extension/Grasping objects/Shoulder rotation | Markerless AR (Microsoft, Kinect) | Projector/PC audio speakers |
| Hoermann et al. (2014) [31] | ART | Hand movement | Markerless AR/finger-tracking extension | Screen |
| Bank et al. (2018) [29] | AR games | Wrist movement/Elbow movement/Shoulder movement | Leap motion/Microsoft Kinect | Head-mounted display |
| Kaneko et al. (2019) [38] | KINVIS | Shoulder/elbow/forearm/wrist/hand movement | Markerless AR | Screen |
| Park et al. (2014) [34] | ARPC system | Balance and gait function | Markerless AR | Head-mounted display/PC audio speakers |
| Lee et al. (2014) [35] | AR-based postural control training | Balance and gait function | Markerless AR | Head-mounted display |
| Kim et al. (2012) [36] | AR-FES | Muscle strength/balance and gait function | Markerless AR | Head-mounted display |
| Jung et al. (2013) [37] | ARR-EMG | Ankle dorsiflexion | Markerless AR | Head-mounted display |
| Author | Design | Number of Patients | Mean Age (Year) | Time since Stroke Onset | Rehabilitation Settings | Intervention |
|---|---|---|---|---|---|---|
| Marcus King et al. (2010) [26] | Pre/post | 4 | Over 18 | Chronic | Home setting Clinical setting | 30 min/day, 3 days/week, 4 weeks |
| Assis et al. (2014) [32] | Pre/post | EG = 4 CG = 4 | 50.5 59.5 | >5 years >4 years | Home setting Clinical setting | 1 h/week, 4 weeks |
| Hondori et al. (2015) [28] | Pre/post | 18 | 57 | >5 years | Clinical setting | 90 s/round, 3 rounds/day |
| Hossain et al. (2015) [27] | Pre/post | 11 | 63.72 | 2 months | Clinical setting | 1 week/1 month |
| Hoermann et al. (2017) [30] | Pre/post | 12 | 61 | 2 months | Clinical setting | 30 min/session, 2 weeks |
| Colomer et al. (2016) [33] | Pre/post | 30 | 58.3 | >1 year | Clinical setting | 45 min/day, 5 days/week |
| Hoermann et al. (2014) [31] | Pre/post | 6 | 53.3 | >5 years | Clinical setting | 60 min/session |
| Bank et al. (2018) [29] | Pre/post | CG: 10 EG: 10 | 61.6 60.5 | >3 months | Clinical setting | 35–105 min/session |
| Kaneko et al. (2019) [38] | Pre/post | 11 | 54.7 | >3 months | Clinical setting | 80 min/day in 10 days |
| Park et al. (2014) [34] | RCT | CG: 10 EG: 10 | 47.38 | >6 months | Clinical setting | 60 min/day, 5 days/week, 4 weeks |
| Lee et al. (2014) [35] | RCT | CG: 11 EG: 10 | 47.9–54 | 11.7 months | Clinical setting | 30 min/day, 5 days/week, 4 weeks |
| Kim et al. (2012) [36] | Pre/post | 28 | 49.35 | >9 months | Clinical setting | 20 min/day, 3 times/week, 8 weeks. |
| Jung et al. (2013) [37] | Pre/post | CG: 5 EG: 5 | 58.4 57.8 | 7.6 months 7 months | Clinical setting | 20 min/day, 5 times/week, 4 weeks |
| Author | Time since Stroke Onset | Total No. of Session | Measurement | Findings |
|---|---|---|---|---|
| Marcus King et al. (2010) [26] | Chronic | 9 sessions | FM; WMFT; DASH | Post-training improvement in FM 11.8%, respectively, time improvement in WMFT 9.58%, improvement in DASH 19.1% |
| Assis et al. (2014) [32] | Chronic | 8 sessions | FM, ROM | Case study 1: Improvement in FM UEMSS in both groups (17–62% in AR Group, 4–14% in Control Group) Case study 2: Significant gain in ROM in all participants (varying from 46.7% to 73.9% in AR Group, varying 61.3% to 90% in Control Group) |
| Hondori et al. (2015) [28] | Chronic | - | FM, BBT | Significant improvement in FM hand/wrist FM proximal subscore, BBT score in AR Game |
| Hossain et al. (2015) [27] | Chronic | - | TCT | Improvement in TCT 16.74% |
| Hoermann et al. (2017) [30] | 2 months | 14 sessions | FMUL, SULCS | Improvement in FMUL 35.8% and in SULCS 28.8% |
| Colomer et al. (2016) [33] | Chronic | 30 sessions | WMFT, BBT, NHPT, FM | Improvement in FM 1.79% (AR) vs. 1.39% (control) Improvement in WMFT 7.8% (AR) vs. 2.9% (control) (p < 0.01) Improvement in BBT 11.2% (AR) vs. 2.0% (control) (p < 0.01) Improvement in NHPT 15.7% (AR) vs. 3.14% (control) (p < 0.01) |
| Hoermann et al. (2014) [31] | Chronic | 24 sessions | FM | Improvements in FM 43.75% |
| Bank et al. (2018) [29] | >3 months | - | Movement speed | Improvement in movement speed 15.5% |
| Kaneko et al. (2019) [38] | >3 months | - | FM, MAS, MAL, ARAT, BBT | Significant improvement in the FM 8.61% (p = 0.003), the MAS (p = 0.001 with wrist flexor muscles, p = 0.008 with 2nd to 5th finger flexor muscles), the MAL (p = 0.007), the total ARAT score (p = 0.018). Improvement in BBT score 54% (p = 0.066) |
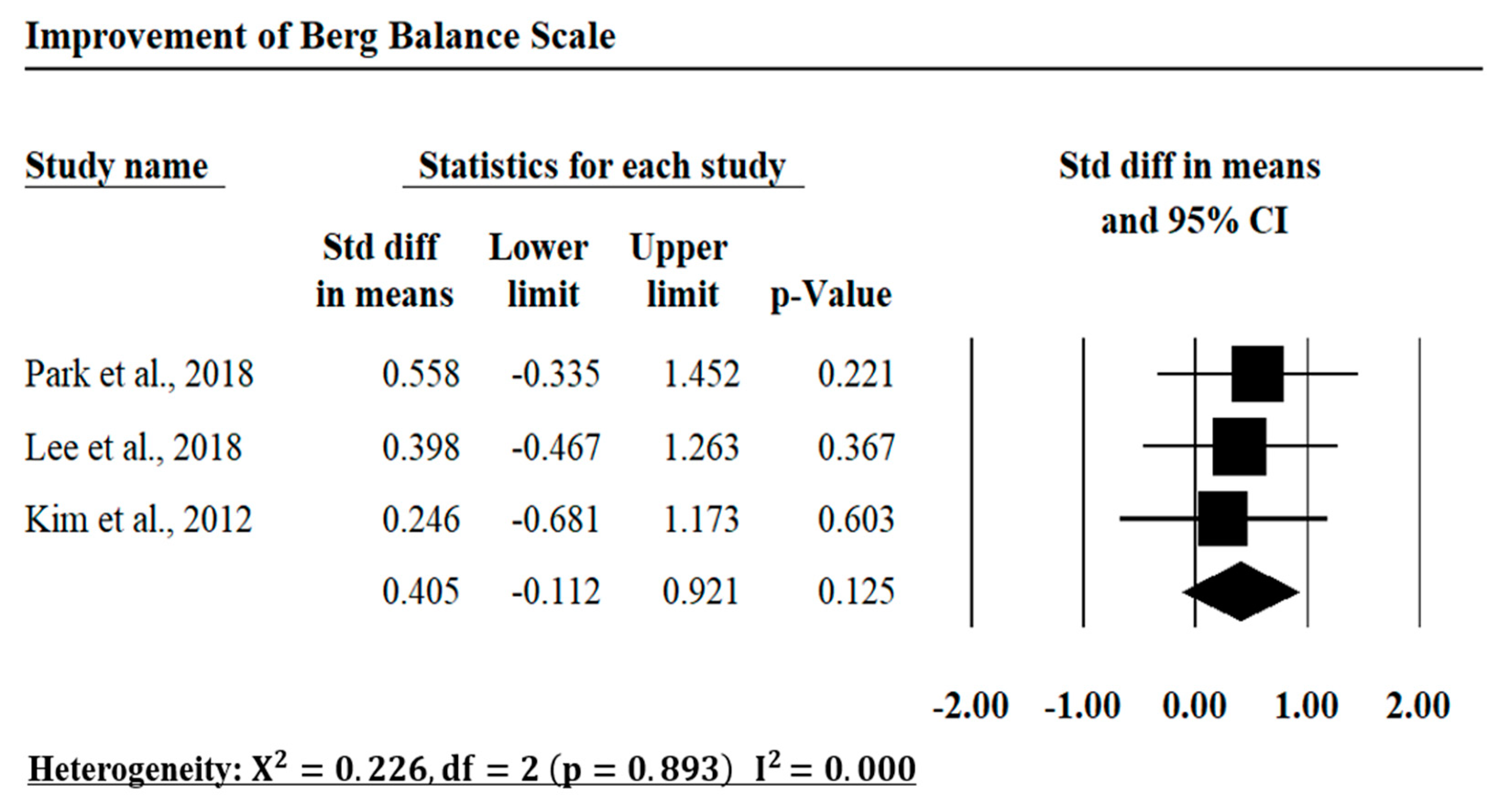
| Park et al. (2014) [34] | Chronic | 20 sessions | BBS, 10 MWT | Significant improvement in the BBS 11.46% (AR) vs. 4.35% (control) (p < 0.05) Significant improvement in the 10 MWT 39.49% (AR) vs. 14.1% (control) (p < 0.05) |
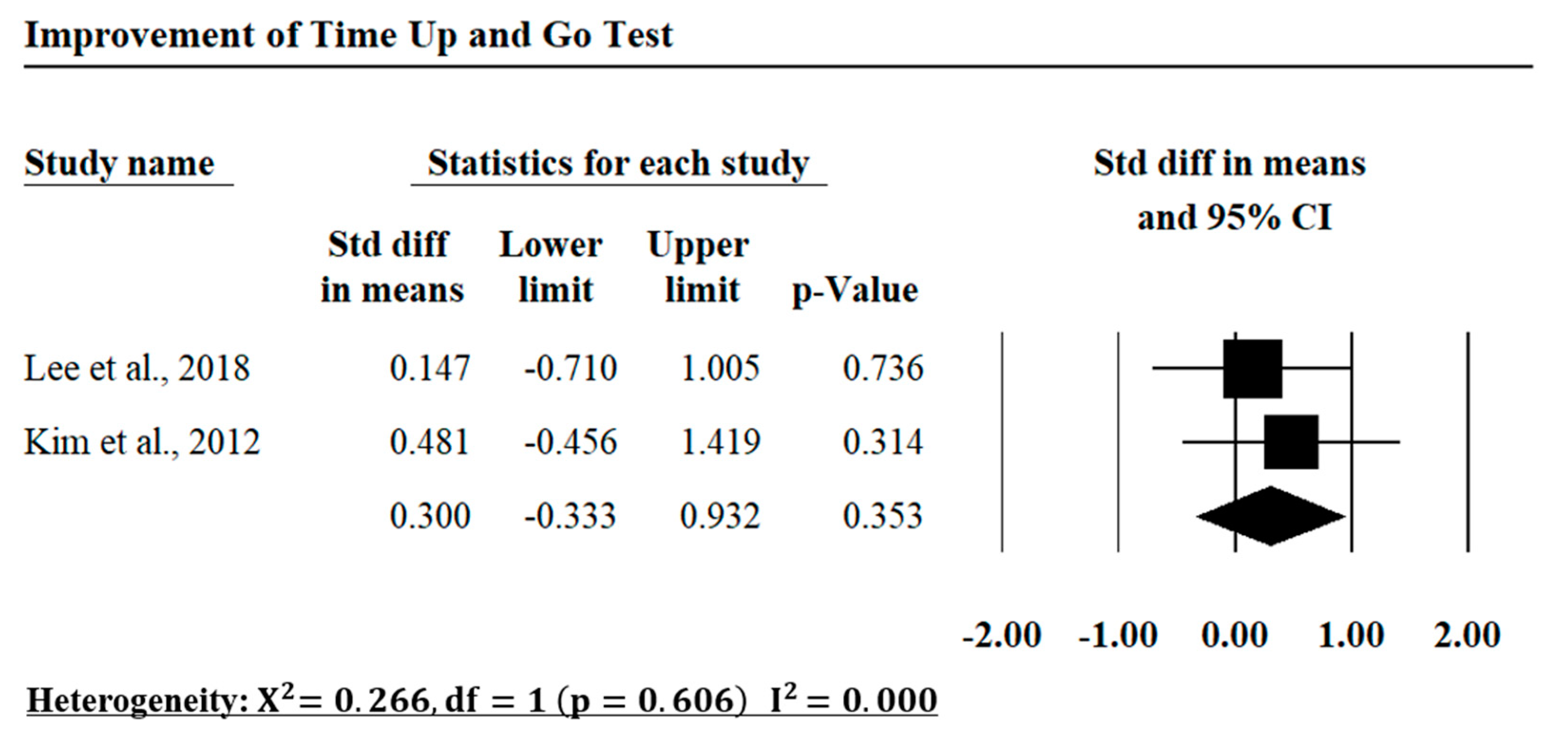
| Lee et al. (2014) [35] | Chronic | 12 sessions | TUG, BBS, Gait velocity (cm/s) | Improvement in BBS 8.95% (AR) vs. 4.17% (control) Time improvement in TUG 18.95% (AR) vs. 8.97 % (control) Improvement in Gait velocity 37.38% (AR) vs. 8.47% (control) |
| Kim et al. (2012) [36] | Chronic | 24 sessions | BBS, TUG | Improvement in BBS 21.65% (AR) vs. 21.22% (control) Time improvement in TUG 22.43% (AR) vs. 13.27% (control) |
| Jung et al. (2013) [37] | Chronic | 12 sessions | Muscle strength | Improvement in Medical GCM dorsiflexion 56.48% (AR) vs. 3.81% (control) Improvement in Medical GCM plantarflexion 78.45% (AR) vs. 9.33% (control) Improvement in Lateral GCM plantarflexion 35.2% (AR) vs. 20.13% (control) Improvement in Lateral GCM dorsiflexion 31.08% (AR) vs. 62.46% (control) Improvement in ankle range of motion 17.77% (AR) vs. 12.17% (control) |
| Authors | Averaged Summary Score | Standard Deviation between Reviewers 1 and 2 |
|---|---|---|
| Marcus King et al. (2010) [26] | 68.8% | 0.088 |
| Assis et al. (2014) [32] | 59.9% | 0.023 |
| Hondori et al. (2015) [28] | 86% | 0.004 |
| Hossain et al. (2015) [27] | 83.2% | 0.035 |
| Hoermann et al. (2017) [30] | 66.1% | 0.009 |
| Colomer et al. (2016) [33] | 91% | 0.025 |
| Hoermann et al. (2014) [31] | 76.4% | 0.02 |
| Bank et al. (2018) [29] | 95.9% | 0.005 |
| Kaneko et al. (2019) [38] | 93.2% | 0.033 |
| Park et al. (2014) [34] | 94.7% | 0.025 |
| Lee et al. (2014) [35] | 94.4% | 0.029 |
| Kim et al. (2012) [36] | 86.6% | 0.028 |
| Jung et al. (2013) [37] | 56.7% | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phan, H.L.; Le, T.H.; Lim, J.M.; Hwang, C.H.; Koo, K.-i. Effectiveness of Augmented Reality in Stroke Rehabilitation: A Meta-Analysis. Appl. Sci. 2022, 12, 1848. https://doi.org/10.3390/app12041848
Phan HL, Le TH, Lim JM, Hwang CH, Koo K-i. Effectiveness of Augmented Reality in Stroke Rehabilitation: A Meta-Analysis. Applied Sciences. 2022; 12(4):1848. https://doi.org/10.3390/app12041848
Chicago/Turabian StylePhan, Huu Lam, Thi Huong Le, Jung Min Lim, Chang Ho Hwang, and Kyo-in Koo. 2022. "Effectiveness of Augmented Reality in Stroke Rehabilitation: A Meta-Analysis" Applied Sciences 12, no. 4: 1848. https://doi.org/10.3390/app12041848
APA StylePhan, H. L., Le, T. H., Lim, J. M., Hwang, C. H., & Koo, K. -i. (2022). Effectiveness of Augmented Reality in Stroke Rehabilitation: A Meta-Analysis. Applied Sciences, 12(4), 1848. https://doi.org/10.3390/app12041848