1. Introduction
Older people normally manage their daily activities in residential aged care through family members, professional caregivers, or by themselves. However, most care agencies focused on the cost of employees and always have a lack of staff, leading to limitations on the healthcare systems [
1,
2]. In addition, differences in backgrounds between the generations can cause generation gap issues such as different ideas, education, and even political leanings [
3,
4]. The current method of human resources distribution, as assigned by care agencies, is insufficient because older people are participants in different social networks. In particular, the COVID-19 pandemic has made these long-term care facilities with staff much riskier than dynamic mutual ways to keep sufficient caretakers [
5,
6]. Older people interact with others on managing spiritual loneliness and watching out for accidents. Older people are often highly active, unlike those in nursing care with chronic diseases, so it is necessary to consider their willingness to collaborate. In the past, long-term care homes with social connections keep stable caretakers and well relationships among long-term care residents. However, from this traditional center architecture aspect to protect people living in long-term care from COVID-19 infection, some staff must restrict activities and interactions with old people, which could lead to a devastating impact on residents’ social connections [
5,
7]. Older people have different or interests or political thinking, so it is a challenge to match their needs through one particular method. The first research question (RQ1) is that what features could be suitable for a mapping procedure on a mutual algorithm to solve the manpower issues and alone living?
An effective method should be able to be customized with novel technologies to satisfy personal needs and preferences. Older people may have dynamic preferences even under the same features conditions, which may influence the chance of success when building a mutual algorithm. Therefore, the second research question is described as follows. RQ2: What kinds of mapping architectures and technologies can help us to build an effective mapping procedure based on the proposed mutual algorithm to coordinate human variability and privacy protection?
The motivation of the article is to clearly identify and solve the existing issues in long-term care to keep older people living safe and happy, and offer related organizations a solution to the shortage of manpower. The expected contributions include (1) solving existing issues on shortage of manpower on taking care of older people; (2) considering the fitness of the corporation for both sides for long-term care; (3) adjusting dynamically based on the human variety of characters; (4) recording the process and outcome of taking care of older people to be credited for the next arrangement; and (5) helping to measure the degree of the physical situation based on the records. An effective mutual algorithm should not only consider features related to personal characteristics and human variability, but also be able to record and improve collaboration or transaction processes through a highly trusted and rigid platform. The primary target of this study is to identify more accurate personal characteristics that can fit the mapping procedure. In addition, it aims to implement Artificial Intelligence (AI) based on a suitable mapping architecture to make the empirical process of the system both appropriate and reliable.
2. Architecture Theories
An ideal architecture of long-term care should consider whether or not it can bring older people a good service quality. Service quality of long-term care has been put in evaluating the long-term service from their perceptions [
8]. Older people are interested in quality of the long-term care system including health care provided. Most of the studies showed that long-term care providers do not always pay attention on the quality of services provided. Service quality can be used as a strategic tool for building distinctive features. Literature shows that service quality can be divided into dimensions such as technical and process functional dimension [
9]. Technical dimension on long-term care is defined as primarily on the basis of architecture design for maintaining good quality on the medical diagnoses and procedures services, as well as conformance to professional specification and standards such as centralized and the decentralized architecture of long-term cares [
10]. Functional dimension can be defined to refer to the manner of long-term care service is delivered to quality of older people relationship with the caregivers.
2.1. The Centralized Architecture of Long-Term Care
The centralized architecture of long-term care is the process by which the activities of long-term care agents who can offer caregivers. The caregivers are like insurance agents who would be trained, have care permits, and would be assigned to a set of older people. However, this is not simply a problem of financial centralization or decentralization. The agent caregivers may seek to take care of nice people and avoid some older people who are at the high-risk levels of uncomfortable people. Centralization of access to the agents of long-term care through specialized data services could have security or privacy issues to lead to the protection failure of the personal data of older people [
9,
10].
Traditionally, the centralized architecture of long-term care could have the decision-making power to be managed directly with the agents of long-term care. Due to saving cost, centralization of long-term care aims at ensuring effective enforcement of controlling activities of caregiver’s consistency in operation [
9,
10]. Therefore, the centralized architecture of long-term care, unlike many security agencies or entities in the human world, could have mutual problems because of unsuitable personality to let older people feel uncomfortable or lonely soul. In addition, privacy issues on personal data protection and insufficient manpower offered by agents of long-term care could be also serious problems through this the centralized architecture of long-term care.
2.2. The Decentralized Architecture of Long-Term Care
It is very important to consider service quality of caregivers based on the centralized architecture of long-term care. However, measuring service quality in long-term care is very difficult to evaluate. This is due to the fact that evaluation of understanding of real perceptions of older people and their satisfaction is quite complex [
8]. Different agents may provide the same types of services but different quality of services. Decentralization of long-term care is the process of shifting decision making a way from centralized control and closer to older people themselves of the services. In many countries the government has opted to decentralize health system as means of improving responsiveness and performance of delivering of long-term care [
10]. The decentralized architecture of long-term care has impacts on the performance of the systems based on some studies found [
11,
12]. In the decentralized architecture of long-term care, it still needs a way or create a model to handle the healthcare services because three main issues, including mental problems from unsuitable matches, privacy data of older people, and insufficient manpower, can be very important to contain the good service quality of caregivers.
Existing studies present a personal information management, which can offer specific features such as interests or contact lists related to the characteristics of older people, to manage communication through a centralized cloud system [
13,
14,
15,
16]. The basic idea behind the decentralized architecture of long-term care to replace or support human resource agencies or other specific local platforms as controlled centers is that good services can consider all human resources to adjust to or coordinate their needs [
17]. Existing studies still try to offer cloud services to achieve sharing medical data with entities with minimal data privacy [
18]. Although existing studies suggest using smart contracts to track the behavior of violations of data permissions, the current studies have some serious problems since it does not consider other impacts for older people such as risk levels. In addition, one of the common limitations of those approaches is that many older people long for a social network in order to have regular interaction with one another to manage spiritual loneliness, and they lack a platform for mutual algorithm and adjusted abilities based on a mapping process suitable for older people [
19]. To the second research question, one of the major challenges is to face in this field is to explore a process innovation [
20] in search of this answer. In order to solve the second research question and the problems mentioned above, this study proposes the use of the decentralized architecture of long-term care to store a mapping or transaction procedure based on AI methods, and the information would be secured and shared across all network candidates.
3. The Mutual Algorithm
When older people are engaging in their daily activities, they may defer or give up their current activities to take part in a mutual algorithm effort. Accordingly, a good mutual algorithm should consider if older people prefer to continue working on their main tasks and be given the opportunity to defer a mutual algorithm until they have completed their current activities. This also implies that a good mutual algorithm can allow older people to flow in and out freely, helping them to realize any rationalization and optimization from their participation in the structure. Older people are often highly active, unlike those in nursing care with chronic diseases, so it is necessary to consider their willingness to collaborate.
Clustering is one of the unsupervised learning methods in the field of machine learning, and it includes various algorithms that may differ significantly in the cluster analysis and efficiently identify factors across similar features [
21,
22]. This study uses the mapping mutual clustering (i.e., MMC) algorithm referred by the clustering method in the long-term care field. Based on the mutual features mapping mutual algorithm selection, this study assumes that each mapping round is repeated and there is an outcome (i.e., optimization) for each round. Therefore, the feedback of each collaboration should consider both the feedback and the probability of using the proposed mutual algorithm.
To formalize the mutual algorithm, this study formulates older people as a four-element vector,
(
,
,
,
), where
n is the total older number of people in the mutual algorithm;
; and terms
O,
R,
P,
M,
D represent older people, risk level, physiology, medical record, and demography, respectively. Distances are normally used to measure the similarity or dissimilarity between two older people, so
S ,
refers to the similarity between two older people,
s = (
s1,
s2, …,
si), and
t = (
t1,
t2, …,
ti). The similarity function of mapping process for each person is defined in Equation (1):
According to Equation (1), this study continues to compute the minimum similarity distance of older people in the same group into
K nonempty subsets in Equation (2):
According to Equation (2), the mutual algorithm continues to compute seed older people as the centroids of the current clusters:
,
, …,
, and then the mutual algorithm uses
S (
,
) to subtract
to obtain a new
S ,
for Equation (3) and new
K groups in Equation (4):
To test MMC, the process of implementation is used to identify initialization of parameters, setting groups, computing similarity, and building final mutual algorithm. The basic idea of the mutual algorithm is that the mapping mutual clustering (MMC) is implemented as an algorithm called the mutual algorithm (Algorithm 1), which can identify some features of older people such as risk level, and group them based on these features. The mutual algorithm is a finite sequence of well-defined, computer-implementable instructions for the mutual algorithm in order to perform a computation upon evaluation. The detailed description of the mutual algorithm is clear as follows, and it is possible to evaluate and verify its feasibility and correctness by building the measurable architecture described in the next subsection to be implemented through the evaluation plan. In the mutual algorithm, there are several steps that need to be implemented, (1) setting initialization of parameters such as risk level, medical record, etc. of older people; (2) giving an original group based on the first glance; (3) resetting their groups based the later features by using clustering to dynamically adjust for human variety characters; (4) building new corporation relationships and making arrangements based on the novel matching way on step three.
| Algorithm 1. Implementation of the Mapping Mutual Clustering (MMC) Algorithm |
| 1. Require: Initialization of parameters: | | | | | |
| getRiskLevel, getPhysiology, getMedicalRecord, getDemography, getOlderPeopleID |
| 2. Set up groups: | | | | | | | | |
| groupA (getOlderPeopleID) ← groupA (getRiskLevel, getPhysiology, getMedicalRecord, getDemography) |
| groupB (getOlderPeopleID) ← groupB (getRiskLevel, getPhysiology, getMedicalRecord, getDemography) |
| groupC (getOlderPeopleID) ← groupC (getRiskLevel, getPhysiology, getMedicalRecord, getDemography) |
| 3. Compute similarity: | | | | | | | |
| for groupA () | | | | | | | | |
| groupA (getOlderPeopleID) ← retrieve (minimum distance) | | | | |
| end for groupA () | | | | | | | | |
| for groupB () | | | | | | | | |
| groupB (getOlderPeopleID) ← retrieve (minimum distance) | | | | |
| end for groupB () | | | | | | | | |
| for groupC () | | | | | | | | |
| groupC (getOlderPeopleID) ← retrieve (minimum distance) | | | | |
| end for groupC () | | | | | | | | |
| 4. Build collaboration: | | | | | | | |
| if groupA (getOlderPeopleID) > groupB (getOlderPeopleID) > groupC (getOlderPeopleID) then | |
| groupA (getOlderPeopleID) ← assign (groupC (getOlderPeopleID)) | | | |
| else if groupA (getOlderPeopleID) > groupC (getOlderPeopleID) > groupB (getOlderPeopleID) then |
| groupA (getOlderPeopleID) ← assign (groupB (getOlderPeopleID)) | | | |
| else if groupB (getOlderPeopleID) > groupA (getOlderPeopleID) > groupC (getOlderPeopleID) then |
| groupB (getOlderPeopleID) ← assign (groupC (getOlderPeopleID)) | | | |
| else if groupB (getOlderPeopleID) > groupC (getOlderPeopleID) > groupA (getOlderPeopleID) then |
| groupB (getOlderPeopleID) ← assign (groupA (getOlderPeopleID)) | | | |
| else if groupC (getOlderPeopleID) > groupA (getOlderPeopleID) > groupB (getOlderPeopleID) then |
| groupC (getOlderPeopleID) ← assign (groupB (getOlderPeopleID)) | | | |
| else | | | | | | | | | |
| groupC (getOlderPeopleID) ← assign (groupA (getOlderPeopleID)) | | | |
| end if | | | | | | | | | |
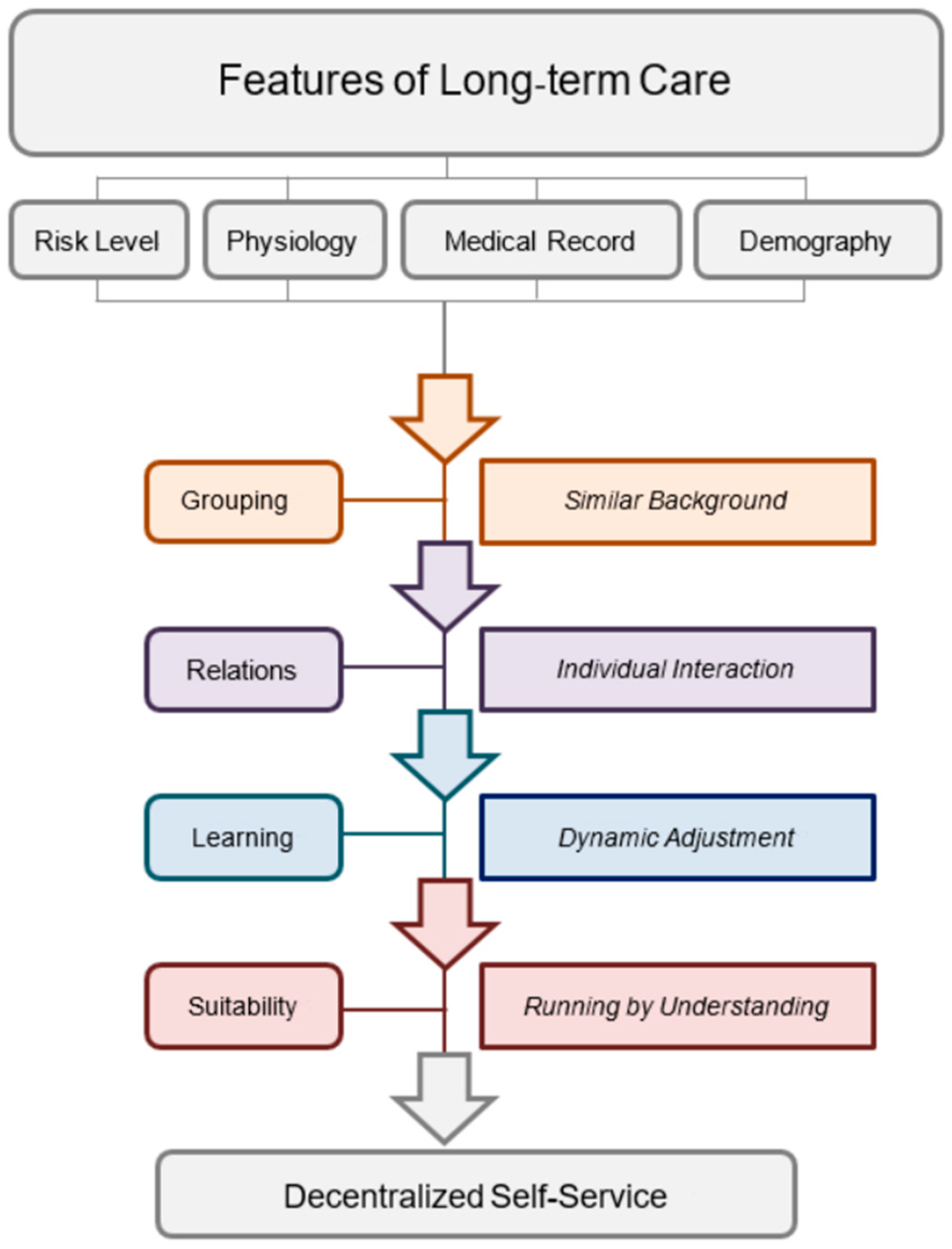
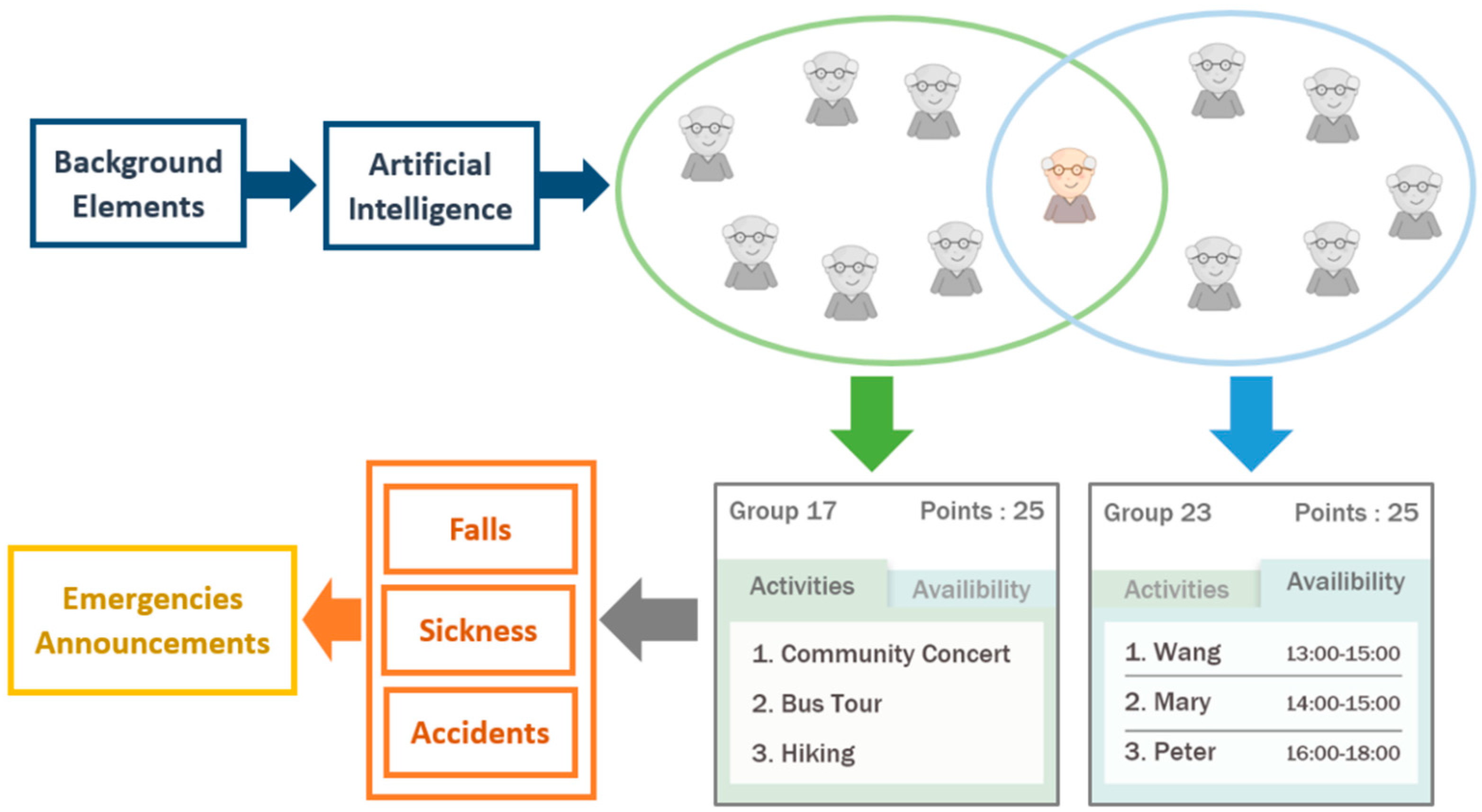
According to the proposed mapping mutual clustering method and its implementation with the mutual algorithm as a description of the implementation of the mapping mutual clustering algorithm above, in order to build a long-term and comprehensive guideline for further system applications, it is necessary to build a framework called the decentralized self-service framework as
Figure 1 depicted. The basic idea of the decentralized self-service framework is that the features are identified clearly with four factors including rick level, physiology, medical records, and demography, the steps are illustrated obviously from grouping to suitability, and the service is grouped into a kind of self-service, which can open to social networks. Based on extant approaches and their limitations, the proposed mutual algorithm not only integrates different data from diverse features but also considers utilizing a classification algorithm in Artificial Intelligence to dynamically increase accuracy. Therefore, adding a self-service mechanism is an important step before building the proposed the decentralized architecture of long-term care. The self-service framework is a grouping based on their similar backgrounds, finding relations of individual interaction; and learning by dynamic adjustment, and running suitably and successfully through mutual understanding.
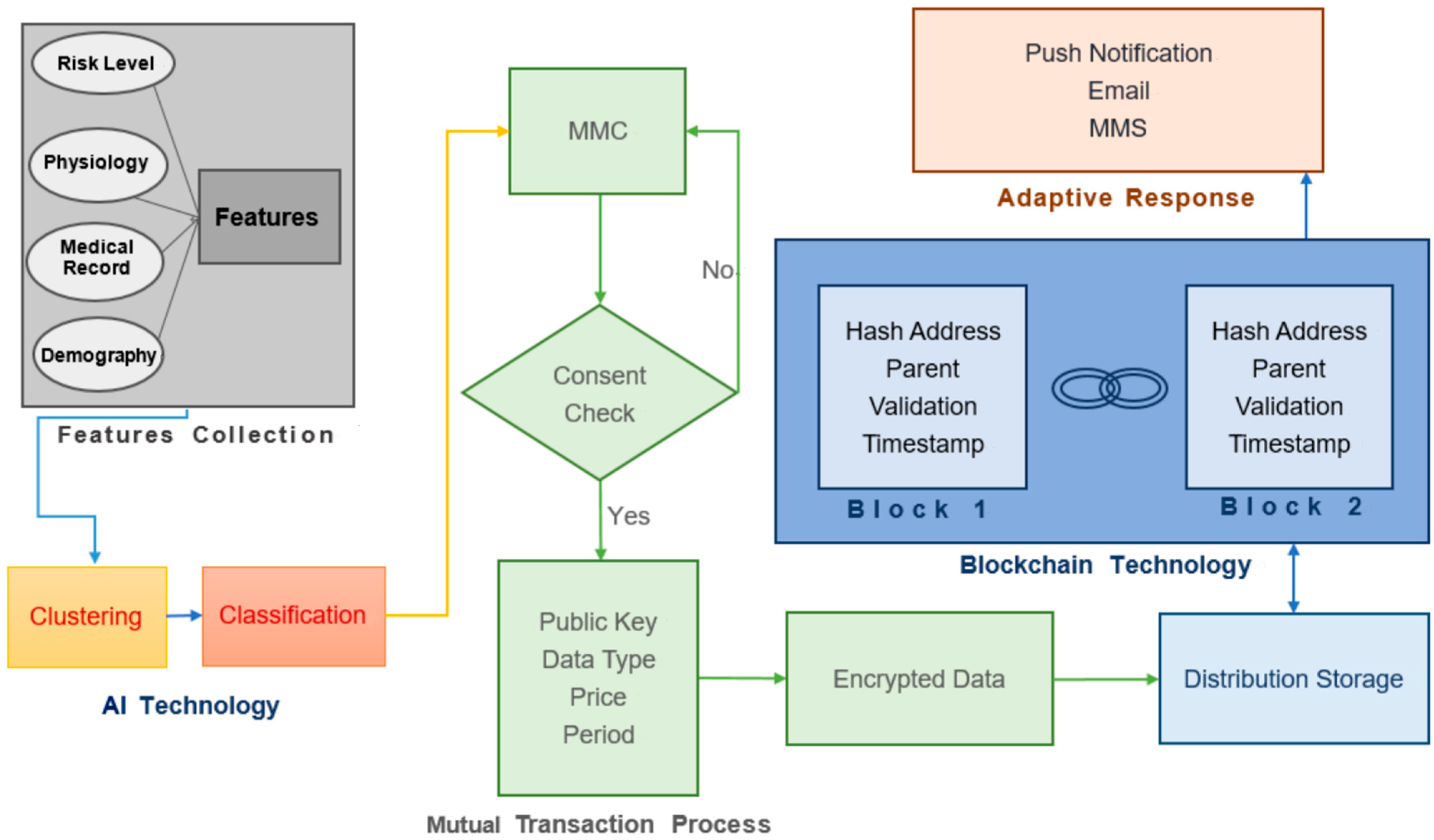
The proposed architecture (LCDA) applies Blockchain technology to demonstrate trusted and auditable computing and the decentralized networks of all older people accompanied by a public collaborative ledger (
Figure 2). LCDA can solve the issues of cost and time consumption related to data acquisition and inappropriate distribution relations between older people. In addition, this architecture can solve the existing issues of care agencies, which now are under third-party authorization. The proposed architecture also can save the costs of transmission and integration through quick and direct data exchanges between older people. Through this LCDA, the proposed mutual algorithm could ensure the non-destructibility of data, which can make the MMC be recorded of older people in a more secure way. The LCDA algorithm (Algorithm 2) demonstrates initialization of parameters from older people; setting up functions such as hash, encryption, and signature to ensure data of older people more secure; computing proof-of-work to let the system operate effectively; and adding blocks to ledgers to let the systems adjust dynamically.
| Algorithm 2. Implementation of the Long-term Care Decentralized Architecture (LCDA) Algorithm |
| 1. Require: Initialization of parameters: | |
| getOlderPeopleID, getOlderPeopleRecords | |
| 2. Set up functions: | | | |
| hash (getOlderPeopleID, getOlderPeopleRecords) | |
| encryption (getOlderPeopleID, getOlderPeopleRecords) |
| signature (getOlderPeopleID, getOlderPeopleRecords) |
| 3. Compute proof-of-work: | | | |
| for pow (time) | | | | |
| constructing blocks ← hashcash (getOlderPeopleID) == true |
| end for | | | | | |
| 4. Add blocks to ledgers: | | | |
| if constructing blocks == true then | | |
| confidential transactions ← hash () + encryption () + signature () |
| upchain to the decentralized platform | | |
| end if | | | | | |
| decryption (getOlderPeopleID, getOlderPeopleRecords) |
The mapping or transaction procedure is a type of distributed ledger, which can view transactions anytime to make LCDA immutable and irreversible.
4. Research Model
This study proposes methods including the mapping mutual clustering (MMC) algorithm and the long-term care decentralized architecture (LCDA) algorithm for creating an innovative manner to solve problems as research questions described. The user perceptions can include user satisfaction, ease of use, usefulness, and user intention, which are all popular for evaluating systems [
26,
27]. To evaluate the system proposed as RQ1 mentioned, this first hypothesis considers medical records, risk level, physiology, and demography to improve the users’ perceived usefulness, ease of use, satisfaction, and intention to use the long-term care system.
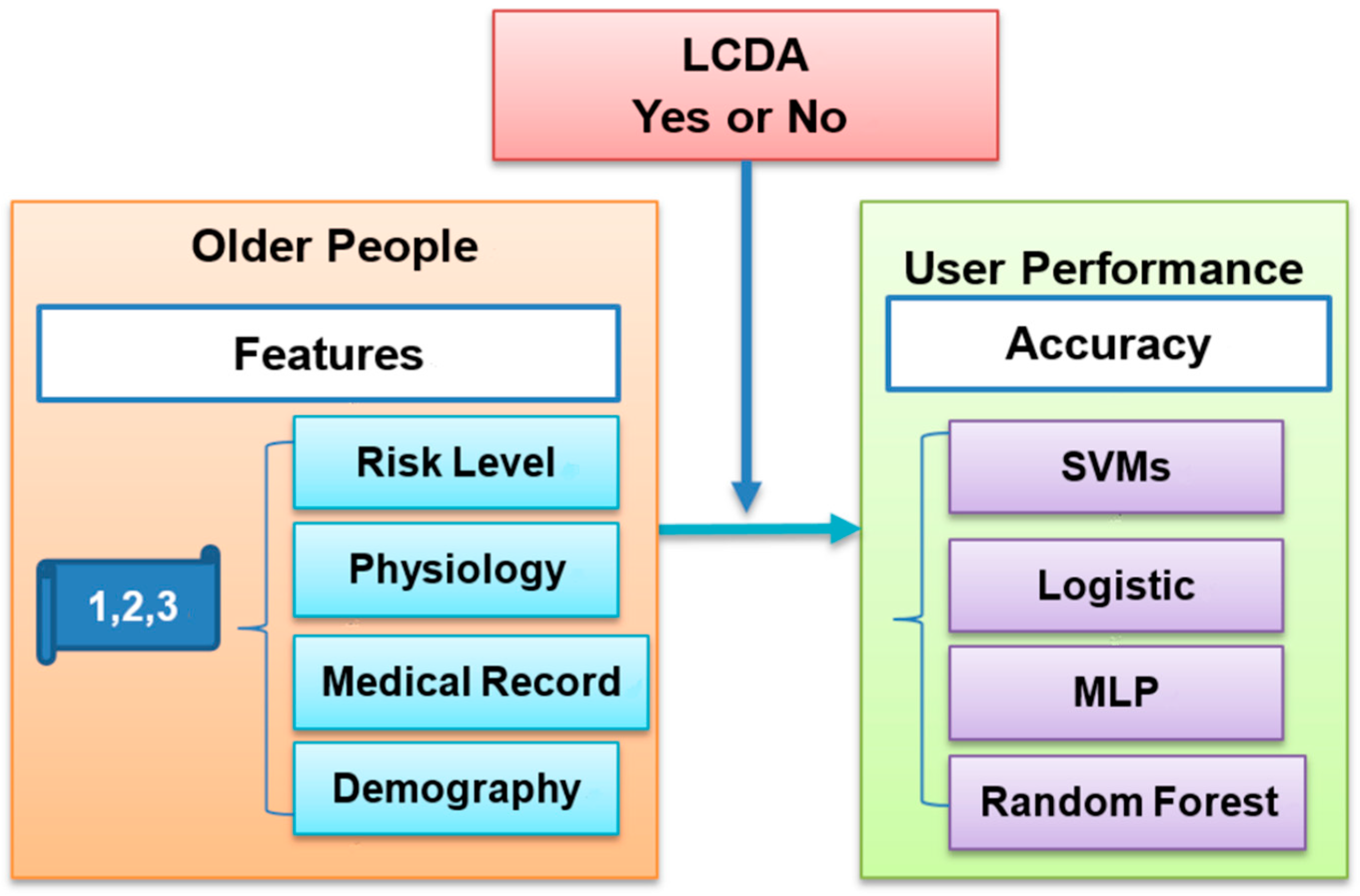
The research model (
Figure 3) mainly focuses on the support vector machines (SVMs), which is widely-used algorithm [
28] for risk minimization [
29,
30]. Other algorithms such as the random forest is suitable for classification trees to put the input vector down each tree in the forest [
30].
This research also uses LCDA to solve the issues of human variability. According to the second research question (RQ2), the second hypothesis examines whether or not the accuracy of the LCDA is higher than the mutual algorithm without the proposed method. The detailed description of the MMC and LCDA algorithm is very clear in the previous two sections, and it is possible to evaluate and verify its feasibility and correctness by building the measurable research model and implementing it through the evaluation plan.
5. Experiment Design
Twelve participants were randomly recruited from various locations (e.g., nursing home, hospital, park) to fill out a questionnaire in order to collect features data (
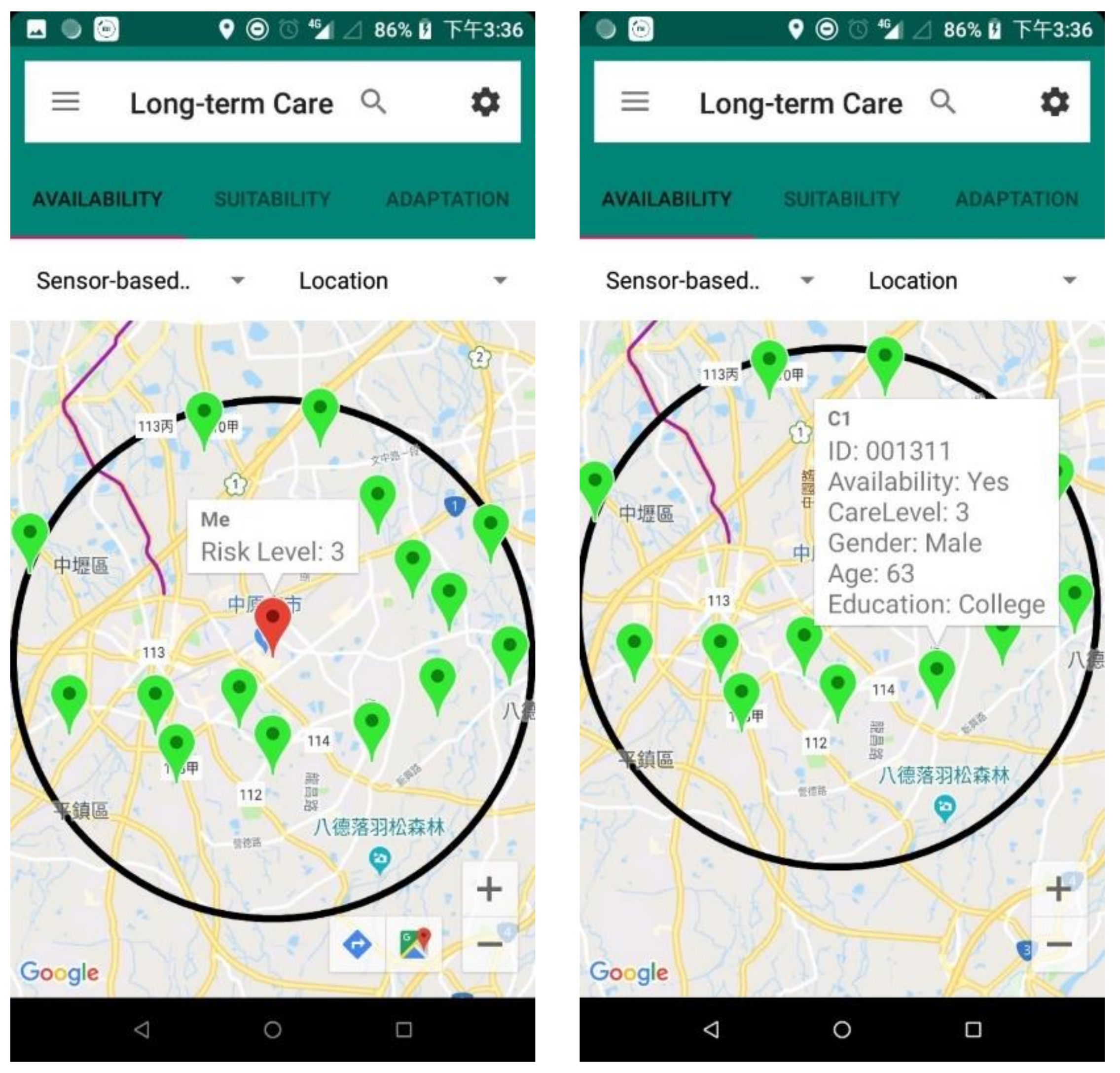
https://drive.google.com/file/d/1rvx-T9krnsZ-ErRgl-wESieP2qFnBfos/view?usp=sharing, accessed on 1 January 2022) of LCDA. To help participants understand LCDA, the prototype system (
Figure 4) has been developed with mobile application software to assist them in completing the questionnaire successfully.
The system architecture (
Figure 5) uses Android Studio software for designing Java programming and mobile application services (APPs).
Participants were over 65 years old. All participants were informed that any potentially identifying information learned and collected from this study would remain confidential and disclosed only upon receipt of permission from the participant. There are three levels for each factor. For the risk level factor, if older people consider that they do not require assistance from others most of the time, this is Level 1. If they estimate a nearly fifty-fifty chance that they need care from others, it is Level 2. The remaining risk level is Level 3. Older people can refer to their own Barthel index, as assessed by the government, to complete this part. Other features such as physiology, medical record, and demography are also classified according to three levels as shown in
Table 1. The survey questionnaire about whether or not the proposed system can improve users’ (a) perceived usefulness, (b) ease of use, (c) satisfaction, and (d) intention to use for long-term care. A five-point Likert scale [
31] was used with 1 indicating “strongly disagree,”, 3 indicating “neutral,” and 5 indicating “strongly agree”.
6. Results
For the first hypothesis, Cronbach’s alpha for user perception was 0.88, which revealed the consistency is reliable. A one-sample
t-test is used for evaluating whether or not the average of user perception is equal to 3 (neutral) based on the middle point of Likert scale [
32]. The perceived usefulness mean difference is 1.33 (
p < 0.01), perceived ease of use is 1.29 (
p < 0.01), user satisfaction is 0.96 (
p < 0.01), and user intention mean difference is 1.17 (
p < 0.01) are all significant. Therefore, the first hypothesis is supported. The data of all participants were collected from the questionnaire based on the proposed features shown in
Table 2.
According to the MMC steps (1–3), including initial partition for older people, choosing seeds as temporary center members, and assigning older people to new groups based on the similarity computations, the dataset is represented in
Table 3,
Table 4 and
Table 5, respectively.
According to the center means of temporary groups, this study continues to compute the minimum similarity distance of older people for the temporary and final groups as shown in
Table 6 and
Table 7, respectively.
The dataset of features of older people includes RL1, Phy1, MR1, Dem1, RL2, Phy2, MR2, and Dem2 to represent the risk level, physiology, medical record, and demography, respectively (
Table 8). The LCDA dataset shows a total of 66 observations calculated in Equation (5):
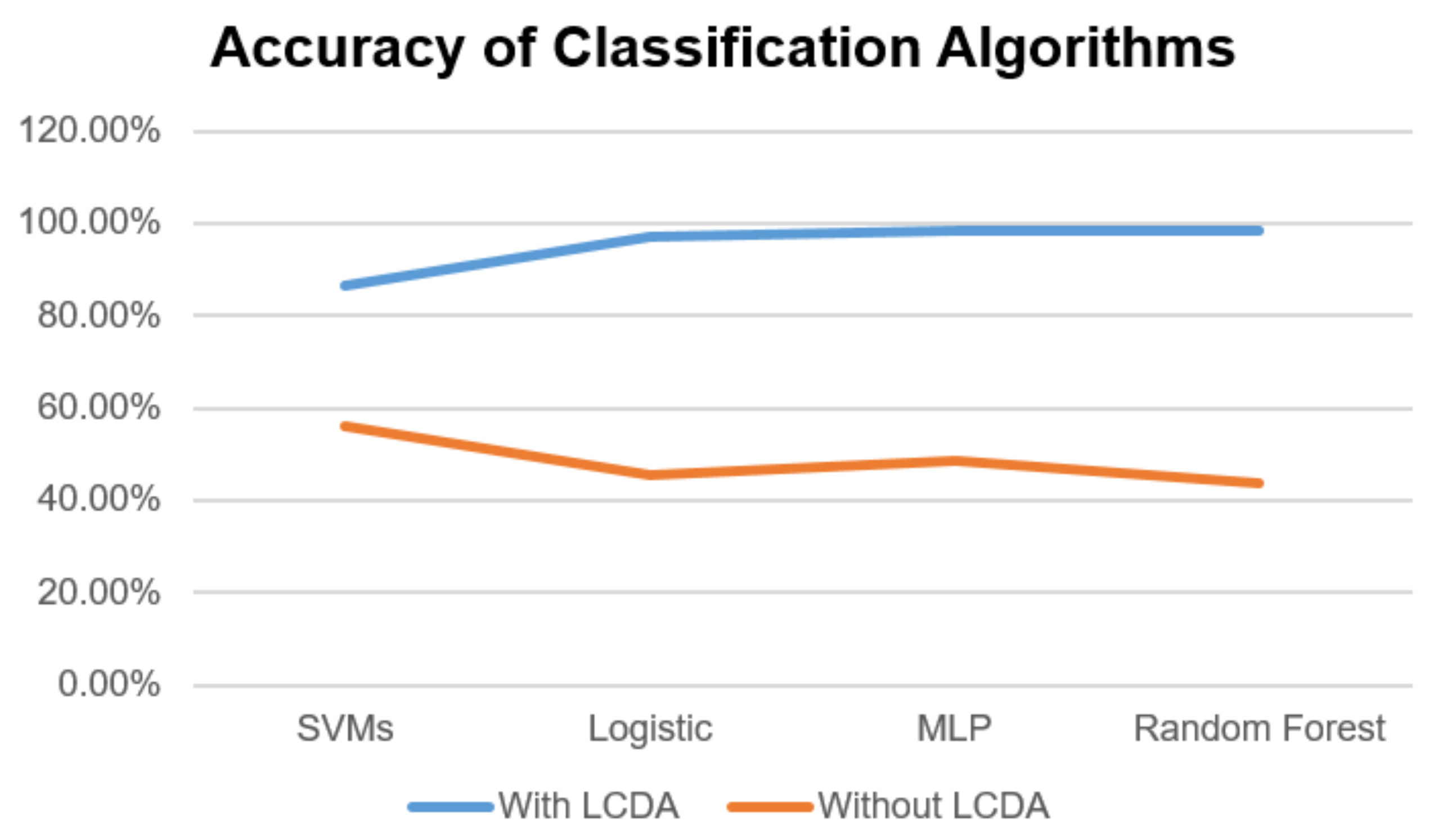
The accuracies are 86.36%, 96.97%, 98.48%, and 98.48% using SVMs, logistic, and MLP, random forest, respectively. The MLP and random forests achieve the highest level of accuracy (
Figure 6).
The collaboration is built randomly 66 times, and the highest accuracy is 56.06% from SVMs. The mean difference is −30.3 (p < 0.01), which is significant. Therefore, the second hypothesis is also supported.
7. Discussion
Based on the literature review, currently, the design of long-term care intends to use centralized architecture, which means agencies assign caretakers to older people based on their manpower policies without taking the appropriate characteristics of older people into consideration. The study proposed methods including MMC and LCDA to overcome some important issues based on the existing architecture that could lead to shortages of manpower and inappropriate cooperation between caretakers and older people. After being systematically evaluated in the experiment, the hypotheses are all supported, those issues can be confirmed to be solved by using the proposed mapping mutual clustering method and long-term care decentralized architecture. Older people sense the suitable caretakers around them, cognitively group caretakers by some characteristics generated from MMC, form long-term corporation relationships with LCDA, and generate records in order to adjust groups dynamically.
With the proposed methods, older people can involve and generate a corporate process when realistic circumstances are acted out in the long-term care systems in order to better understand the outcome of caretakers no matter they are coming from. Because individual caretakers may behave differently attitudes or performance even under the same situation, attempting to define the qualified ability of caretakers and associated system reactions in a static way that is desired by all older people is impossible and can result in risks and difficulty for caretakers. Therefore, a long-term care system should provide a dynamic interaction for all participants so that they can map mutual rules at any time. The decentralized architecture emphasizes the importance of understanding older people in their mapping mutual process and involves characteristics such as risk level while going out for a walk in a dangerous environment.
8. Conclusions
The study makes many significant contributions to proposing novel methods. First, existing mutual algorithms for long-term care mainly focus on benefits with centralized care agencies to match healthcare workers and older people. However, the benefits of care agencies and cannot solve the issue of manpower. To address the first research question, this study proposes a novel method, called the mapping mutual clustering algorithm, considering all possible features across all older people. Second, the proposed long-term care decentralized architecture algorithm applies Artificial Intelligence and Blockchain to solve the issues of dynamically adjusting, coordinating human variability, and the privacy protection, which can address the second research question. Third, this study applies an empirical process to long-term care.
There are a few limitations and future works to this study. First, this study evaluated the proposed decentralized architecture of long-term care through a features-based questionnaire, which could not immediately reflect current long-term care operational mechanisms in reality. Therefore, it is better to perform an experiment with a larger sample based on the proposed methods in future studies. In the future, enlarging the dataset by building the decentralized system will overcome any limitation on the accuracy of the classification. Second, due to considering privacy issues, the relevant features categorized on the risk levels 1, 2, and 3 do not correspond to the Barthel index, as measured by official investigation reports. To guide practical insights to the long-term care system, the sub-item categories should be clearly identified to solve the issue of disclosing information.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}