
Accuracy of Assessing Weight Status in Adults by Structured Observation

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Selection and Recruitment
2.2. Recruitment and Training of the Observers
2.3. Procedures for Data Collection
2.3.1. Measures Estimated by Observation
- -
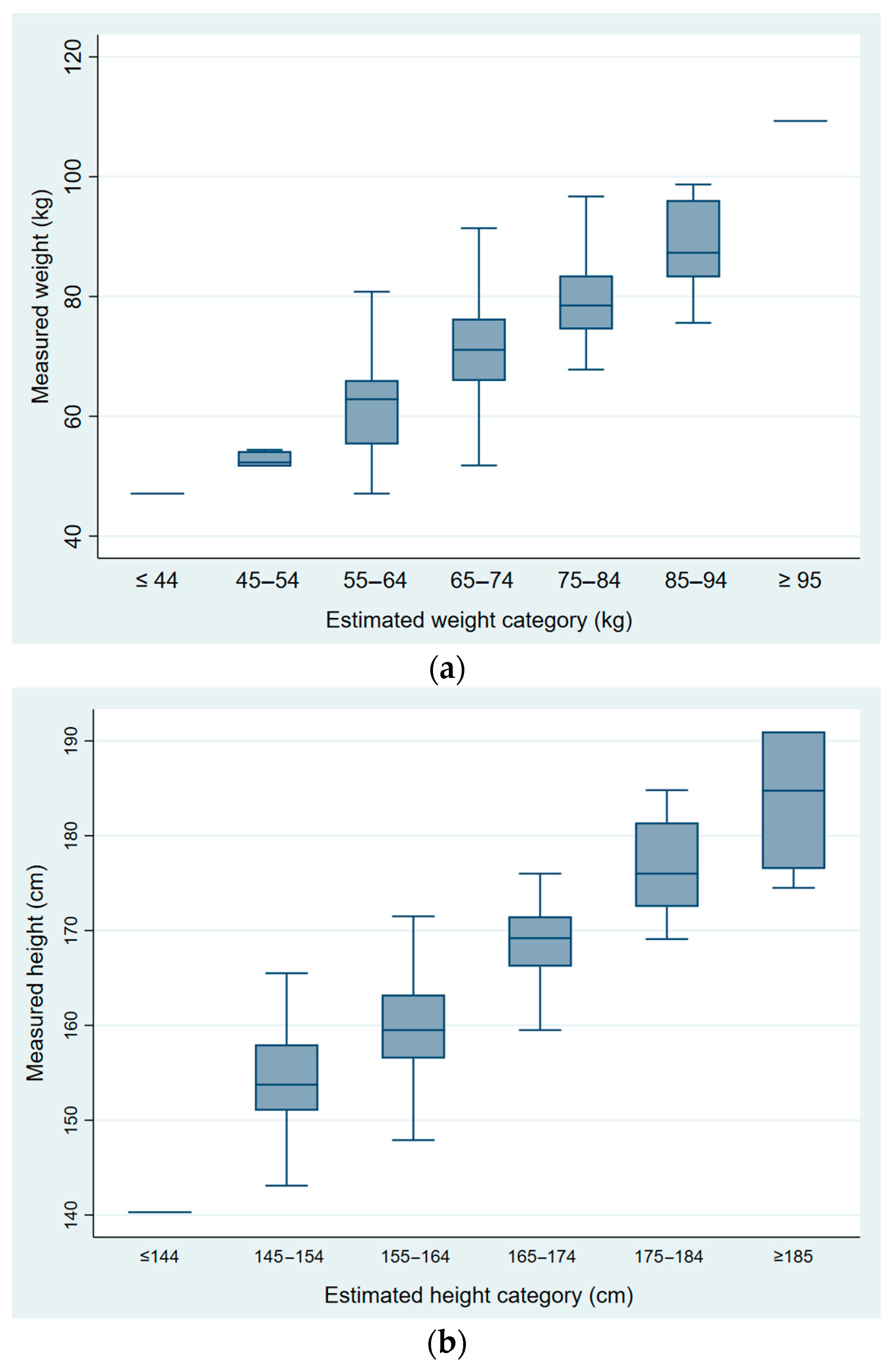
- Height: (1) ≤144 cm, (2) 145–154 cm, (3) 155–164 cm, (4) 165–174 cm, (5) 175–184 cm, (6) ≥185 cm;
- -
- Weight: (1) ≤44 kg, (2) 45–54 kg, (3) 55–64 kg, (4) 65–74 kg, (5) 75–84 kg, (6) 85–94 kg, (7) ≥95 kg.
- -
- Height: (1) ≤154 cm, (2) 155–164, (3) ≥165 cm;
- -
- Weight: (1) ≤54 kg, (2) 55–74 kg, (3) ≥75 kg.
2.3.2. Anthropometric Measures
2.4. Statistical Analyses
3. Results
3.1. Demographic and Anthropometric Measurements of Observers and Participants
3.2. Associations between Measured and Estimated Weight and Height
3.3. Validity of Estimating BMI by Trained Observers
3.4. Inter-Observer Reliability Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gorber, S.C.; Tremblay, M.; Moher, D.; Gorber, B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: A systematic review. Obes. Rev. 2007, 8, 307–326. [Google Scholar] [CrossRef]
- Skopec, L.; Musco, T.; Sommers, B.D. A Potential New Data Source for Assessing the Impacts of Health Reform: Evaluating the Gallup-Healthways Well-Being Index. Healthcare 2014, 2, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Keith, S.W.; Fontaine, K.R.; Pajewski, N.M.; Mehta, T.; Allison, D.B. Use of self-reported height and weight biases the body mass index-mortality association. Int. J. Obes. 2011, 35, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Wetmore, C.M.; Mokdad, A.H. In denial: Misperceptions of weight change among adults in the United States. Prev. Med. 2012, 55, 93–100. [Google Scholar] [CrossRef]
- Gorber, S.C.; Tremblay, M.S. The Bias in Self-reported Obesity From 1976 to 2005: A Canada–US Comparison. Obesity 2010, 18, 354–361. [Google Scholar] [CrossRef]
- Wright, F.L.; Green, J.; Reeves, G.; Beral, V.; Cairns, B.J.; On behalf of the Million Women Study. Validity over time of self-reported anthropometric variables during follow-up of a large cohort of UK women. BMC Med. Res. Methodol. 2015, 15, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gildner, T.E.; Barret, T.M.; Liebert, M.A.; Kowal, P.; Snodgrass, J.J. Does BMI generated by self-reported height and weight measure up in older adults from middle-income countries? Results from the study on global AGEing and adult health (SAGE). BMC Obes. 2015, 2, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, E. Overweight but unseen: A review of the underestimation of weight status and a visual normalization theory. Obes. Rev. 2017, 18, 1200–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, E.A.; Appleby, P.N.; Davey, G.K.; Key, T.J. Validity of self-reported height and weight in 4808 EPIC-Oxford participants. Public Health Nutr. 2001, 5, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Madrigal, H.; Martínez-González, M.A.; Kearney, J.; Gibney, M.J.; De Irala, J.; Martinez, J.A. Perception of body image as indicator of weight status in the European Union. J. Hum. Nutr. Diet. 2001, 14, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Flegal, K.M.; Ogden, C.L.; Fryar, C.; Afful, J.; Klein, R.; Huang, D.T. Comparisons of Self-Reported and Measured Height and Weight, BMI, and Obesity Prevalence from National Surveys: 1999–2016. Obesity 2019, 27, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.; Choi, S.; Won, J.; Lee, Y.-K.; Kim, D.-H.; Lee, S.K. Differences in accuracy of height, weight, and body mass index between self-reported and measured using the 2018 Korea Community Health Survey data. Epidemiol. Health 2022, 44, e2022024. [Google Scholar] [CrossRef] [PubMed]
- Roystonn, K.; Abdin, E.; Sambasivam, R.; Zhang, Y.; Chang, S.; Shafie, S.; Chua, B.Y.; Vaingankar, J.A.; Chong, S.A.; Subramaniam, M. Accuracy of self-reported height, weight and BMI in a multiethnic Asian population. Ann. Acad. Med. Singap. 2021, 50, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Thomson, C.A.; Hendryx, M.; Tinker, L.F.; Manson, J.E.; Li, Y.; Nelson, D.A.; Vitolins, M.Z.; Seguin, R.A.; Eaton, C.B.; et al. Accuracy of self-reported weight in the Women’s Health Initiative. Public Health Nutr. 2019, 22, 1019–1028. [Google Scholar] [CrossRef] [Green Version]
- Peterson, M.; Orsega-Smith, E.; Tholstrup, L. Validity of the body mass index silhouette matching test. Am. J. Health Behav. 2004, 28, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Harris, C.V.; Bradlyn, A.S.; Coffman, J.; Gunel, E.; Cottrell, L. BMI-based body size guides for women and men: Development and validation of a novel pictorial method to assess weight- related concepts. Int. J. Obes. 2007, 32, 336–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stunkard, A.; Sorensen, T.; Schlusinger, F. Use of Danish adoption register for the study of obesity and thinness. In The Genetics of Neurological and Psychiatric Disorders; Kety, S., Roland, L., Sidman, R., Matthysse, S., Eds.; Raven Press: New York, NY, USA, 1983; pp. 115–120. [Google Scholar]
- Bulik, C.M.; Wade, T.D.; Heath, A.C.; Martin, N.G.; Stunkard, A.J.; Eaves, L.J. Relating body mass index to figural stimuli: Population-based normative data for Caucasians. Int. J. Obes. 2001, 25, 1517–1524. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, T.; Stunkard, A.J. Does obesity run in families because of genes? An adoption study using silhouettes as a measure of obesity. Acta Psychiatr. Scand. 1993, 370, 67–72. [Google Scholar] [CrossRef]
- Direcção-Geral da Saúde. Orientação no 017/2013 de 05/12/2013—Avaliação Antropométrica no Adulto. Direcção-Geral da Saúde. 2013. Available online: https://www.dgs.pt/directrizes-da-dgs/orientacoes-e-circulares-informativas/orientacao-n-0172013-de-05122013-pdf.aspx (accessed on 12 January 2018).
- Stewart, A.; Marfell-Jones, M. International Standards for Anthropometric Assessment, 3rd ed.; International Society for the Advancement of Kinanthropometry: Lower Hutt, New Zealand, 2011. [Google Scholar]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry: Report of a World Health Organization Expert Committee; World Health Organization: Geneva, Switzerland, 1995; Available online: http://www.who.int/iris/handle/10665/37003 (accessed on 12 January 2018).
- Hall, W.L.; Larkin, G.L.; Trujillo, M.J.; Hinds, J.L.; Delaney, K.A. Errors in weight estimation in the emergency department: Comparing performance by providers and patients. J. Emerg. Med. 2004, 37, 219–224. [Google Scholar] [CrossRef]
- Breuer, L.; Nowe, T.; Huttner, H.B.; Blinzler, C.; Kollmar, R.; Schellinger, P.D.; Schwab, S.; Köhrmann, M. Weight approximation in stroke before thrombolysis—The WAIST-Study. Stroke. 2010, 41, 2867–2871. [Google Scholar] [CrossRef] [Green Version]
- Corbo, J.; Canter, M.; Grinberg, D.; Bijur, P. Who should be estimating a patient’s weight in the emergency department? Acad. Emerg. Med. 2005, 12, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Menon, S.; Kelly, A.M. How accurate is weight estimation in the emergency department? Emerg. Med. Australas. 2005, 17, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Khan, C.A.; Oman, J.A.; Rudkin, S.E.; Anderson, C.L.; Sultani, D. Can ED staff accurately estimate the weight of adult patients? Am. J. Emerg. Med. 2007, 25, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.W.; Yoshida, D.; Quinn, J.; Strehlow, M. A better way to estimate adult patients’ weights. Am. J. Emerg. Med. 2009, 27, 1060–1064. [Google Scholar] [CrossRef] [PubMed]
- Lessing, J.K.; Ford, W.J.H.; Steel, P.A.; Clark, S.; Sharma, R.; Arbo, J.E. Use of Physician-Estimated and Patient Self-Reported Weights to Guide Initial Fluid Resuscitation in Emergency Department Patients With Suspected Sepsis. J. Intensive Care Med. 2021, 36, 793–797. [Google Scholar] [CrossRef]
- Thomas, R.A.; Empey, J.A.; Seth, S.; Crozier, J. Guess the weight: The accuracy of estimated weight for surgical admissions—A comparison study. Scott. Med. J. 2019, 64, 56–61. [Google Scholar] [CrossRef]
- Ikeda, N. Validity of self-reports of height and weight among the general adult population in Japan: Findings from National Household Surveys, 1986. PLoS ONE. 2016, 11, e0148297. [Google Scholar] [CrossRef]
- Johnson-Taylor, W.L.; Fisher, R.A.; Hubbard, V.S.; Starke-Reed, P.; Eggers, P.S. The change in weight perception of weight status among the overweight: Comparison of NHANES III (1988–1994) and 1999-2004 NHANES. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 9. [Google Scholar] [CrossRef] [Green Version]
- Aylward, L.L.; Schneider, K.L.; Sanchez-Johnsen, L. Misreporting Weight and Height Among Mexican and Puerto Rican Men. Am. J. Mens. Health 2021, 15, 15579883211001198. [Google Scholar] [CrossRef]
- Haakstad, L.A.H.; Stensrud, T.; Gjestvang, C. Does Self-Perception Equal the Truth When Judging Own Body Weight and Height? Int. J. Environ. Res. Public Health 2021, 18, 8502. [Google Scholar] [CrossRef]
- Drieskens, S.; Demarest, S.; Bel, S.; Ridder, K.D.; Tafforeau, J. Correction of self-reported BMI based on objective measurements: A Belgian experience. Arch. Public Health 2018, 76, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelissen, K.; Gledhill, L.J.; Cornelissen, P.L.; Tovée, M.J. Visual biases in judging body weight. Br. J. Health Psychol. 2016, 21, 555–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldham, M.; Robinson, E. Visual body size norms and the under-detection of overweight and obesity. Obes. Sci. Pract. 2017, 4, 29–40. [Google Scholar] [CrossRef] [Green Version]
- Robinson, E.; Kersbergen, I. Overweight or about right? A norm comparison explanation of perceived weight status. Obes. Sci. Pract. 2017, 3, 36–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldham, M.; Robinson, E. Visual weight status misperceptions of men: Why overweight can look like a healthy weight. J. Health Psychol. 2016, 21, 1768–1777. [Google Scholar] [CrossRef] [Green Version]
- Muttarak, R. Normal¬ization of Plus Size and the Danger of Unseen Overweight and Obesity in England. Obesity 2018, 26, 1125–1129. [Google Scholar] [CrossRef] [Green Version]
- Lancki, N.; Siddique, J.; Schneider, J.A.; Kanaya, A.M.; Fujimoto, K.; Dave, S.S.; Puri-Taneja, A.; Kandula, N.R. Social network body size is associated with body size norms of South Asian adults. Obes. Med. 2018, 11, 25–30. [Google Scholar] [CrossRef]
- Opie, C.A.; Glenister, K.; Wright, J. Is social exposure to obesity associated with weight status misperception? Assessing Australians ability to identify overweight and obesity. BMC Public Health 2019, 19, 1222. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.W.Y.; Noles, D.L.; Utkov, N.; Akbilgic, O.; Smith, W. Misalignment between perceptual boundaries and weight categories reflects a new normal for body size perception. Sci. Rep. 2021, 11, 10442. [Google Scholar] [CrossRef]
- Ata, R.N.; Thompson, J.K. Weight bias in the media: A review of recent research. Obes. Facts. 2010, 3, 41–46. [Google Scholar] [CrossRef]
- Schwartz, M.B.; Chambliss, H.O.; Brownell, K.D.; Blair, S.N.; Billington, C. Weight bias among health professionals specializing in obesity. Obes. Res. 2003, 11, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Caccamese, S.M.; Kolodner, K.; Wright, S.M. Comparing patient and physician perception of weight status with body mass index. Am. J. Med. 2002, 112, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Goutelle, S.; Bourguignon, L.; Bertrand-Passeron, N.; Jelliffe, R.W.; Maire, P. Visual estimation of patients’ body weight in hospital: The more observers, the better? Pharm. World Sci. 2009, 31, 422–425. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 127) | Women (n = 70) | Men (n = 57) | p-Value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 50.3 ± 16.3 | 47.9 ± 1.7 | 53.4 ± 2.5 | 0.058 |
| Age categories, n (%) | ||||
| 18–34 | 24 (18.9) | 15 (21.4) | 9 (15.8) | 0.127 |
| 35–54 | 53 (41.7) | 33 (47.1) | 20 (35.1) | |
| ≥55 | 50 (39.4) | 22 (31.4) | 28 (49.1) | |
| Height (cm), mean ± SD | 164.9 ± 9.6 | 159.7 ± 0.8 | 171.5 ± 1.1 | <0.001 a |
| Height categories, n (%) | ||||
| ≤154 | 14 (11.0) | 13 (18.6) | 1 (1.8) | <0.001 b |
| 155–164 | 52 (40.9) | 42 (60.0) | 10 (17.5) | |
| ≥165 | 61 (48.0) | 15 (21.4) | 46 (80.7) | |
| Weight (kg), mean ± SD | 73.1 ± 12.9 | 68.3 ± 1.4 | 79.1 ± 1.6 | <0.001 a |
| Weight categories, n (%) | ||||
| ≤ 54 | 11 (8.7) | 10 (14.3) | 1 (1.8) | <0.001 b |
| 55–74 | 63 (49.6) | 41 (58.6) | 22 (38.6) | |
| ≥75 | 53 (41.7) | 19 (27.1) | 34 (59.6) | |
| BMI (kg/m2), mean ± SD | 26.9 ± 4.1 | 26.8 ± 0.5 | 26.9 ± 0.5 | 0.900 |
| BMI categories, n (%) | ||||
| <18.5 | 5 (3.9) | 4 (5.7) | 1 (1.8) | 0.006 b |
| 18.5–24.9 | 32 (25.2) | 21 (30.0) | 11 (19.3) | |
| 25.0–29.9 | 61 (48.0) | 24 (34.3) | 37 (64.9) | |
| ≥30 | 29 (22.8) | 21 (30.0) | 8 (14.0) |
| Participants’ Characteristics | Sensitivity | Specificity | Likelihood Ratio | |
|---|---|---|---|---|
| Positive (LR+) | Negative (LR−) | |||
| Weight status | ||||
| Obesity | 41.4% | 96.4% | 11.5 | 0.61 |
| Overweight/obesity | 72.8% | 78.4% | 3.4 | 0.35 |
| Obesity | Overweight/Obesity | |||||||
|---|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Likelihood Ratio | Sensitivity | Specificity | Likelihood Ratio | |||
| Positive (LR+) | Negative (LR−) | Positive (LR+) | Negative (LR−) | |||||
| Gender of Observer | ||||||||
| Female | 56.8% | 95.0% | 11.4 | 0.45 | 76.6% | 76.6% | 3.3 | 0.31 |
| Male | 14.3% | 98.7% | 11.0 | 0.87 | 66.7% | 81.5% | 3.6 | 0.41 |
| p = 0.002 | p = 0.184 | p = 0.146 | p = 0.623 | |||||
| Gender of Participant | ||||||||
| Female | 50.0% | 92.9% | 7.0 | 0.54 | 65.6% | 100% | - | 0.34 |
| Male | 38.1% | 100% | - | 0.62 | 80.0% | 68.0% | 2.5 | 0.29 |
| p = 0.411 | p = 0.014 | p = 0.029 | p = 0.002 | |||||
| Age of Participant (years) | ||||||||
| 18–34 | 20.0% | 100% | - | 0.80 | 79.2% | 91.7% | 9.5 | 0.23 |
| 35–54 | 37.5% | 97.6% | 15.6 | 0.64 | 66.2% | 78.1% | 3.0 | 0.43 |
| ≥55 | 54.2% | 93.4% | 8.2 | 0.49 | 76.8% | 61.1% | 2.0 | 0.38 |
| p = 0.161 | p = 0.206 | p = 0.249 | p = 0.059 | |||||
| <50 or ≥50 years | ||||||||
| <50 | 33.3% | 100% | - | 0.67 | 69.2% | 85.4% | 4.7 | 0.36 |
| ≥50 | 50.0% | 93.0% | 7.1 | 0.54 | 75.5% | 65.4% | 2.2 | 0.37 |
| p = 0.198 | p = 0.014 | p = 0.350 | p = 0.046 | |||||
| Kappa | 95%CI | |
|---|---|---|
| Height (cm) | ||
| ≤154 | 0.63 | 0.49–0.76 |
| 155–164 | ||
| ≥165 | ||
| Weight (kg) | ||
| ≤54 | 0.46 | 0.31–0.62 |
| 55–74 | ||
| ≥75 | ||
| BMI (kg/m2) | ||
| <18.5 | 0.52 | 0.39–0.64 |
| 18.5–24.9 | ||
| 25.0–29.9 | ||
| ≥30 | ||
| <25 | 0.67 | 0.50–0.83 |
| ≥25 | ||
| Stunkard Body Figures (1 to 9) | 0.30 | 0.22–0.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jorge, T.; Sousa, S.; do Carmo, I.; Lunet, N.; Padrão, P. Accuracy of Assessing Weight Status in Adults by Structured Observation. Appl. Sci. 2023, 13, 8185. https://doi.org/10.3390/app13148185
Jorge T, Sousa S, do Carmo I, Lunet N, Padrão P. Accuracy of Assessing Weight Status in Adults by Structured Observation. Applied Sciences. 2023; 13(14):8185. https://doi.org/10.3390/app13148185
Chicago/Turabian StyleJorge, Tânia, Sofia Sousa, Isabel do Carmo, Nuno Lunet, and Patrícia Padrão. 2023. "Accuracy of Assessing Weight Status in Adults by Structured Observation" Applied Sciences 13, no. 14: 8185. https://doi.org/10.3390/app13148185
APA StyleJorge, T., Sousa, S., do Carmo, I., Lunet, N., & Padrão, P. (2023). Accuracy of Assessing Weight Status in Adults by Structured Observation. Applied Sciences, 13(14), 8185. https://doi.org/10.3390/app13148185