

Effectiveness of Virtual Reality Goggles as Distraction for Children in Dental Care—A Narrative Review


 ,
,
Abstract
:1. Introduction
- Facial Image Scale: Images of seven faces that represent children’s sense of responsiveness. It is used to measure dental anxiety in young children, who normally have a medium-low reading ability [11].
- Venham Picture Test: Eight cards with two figures each that are recorded as one point or zero points, with the range being between a minimum of zero and a maximum of eight. This test is acceptable for children between 6 and 15 years old [12].
- Likert-type scale: A technique that calculates favorable and unfavorable responses to a stimulus or information previously given. It is applied through some kind of questionnaire, which is created based on five sections, and the results are separated into three categories: the first and the last will indicate extreme affirmative and negative responses, and the average will express that the subject does not know what to think or is indecisive [22].
- Frankl’s Behavioral Scale: This technique has been used in a wide variety of behavioral studies because it is an easy, practical and inexpensive technique for rating patients’ behavior in four categories: type 1: definitely negative; type 2: negative; type 3: positive; type 4: definitely positive [23,24,25,26].
- Basic behavior management methods: Tell-show-do, voice control, nonverbal communication, positive reinforcement, distraction, parental presence or absence, and the use of nitrous oxide.
- Advanced Behavioral Management Approach: Protective Stabilization, Sedation, and General Anesthesia.
- Active interaction encourages the child patient to participate in some activities during treatment, such as interactive games, singing, squeezing objects, breath control or guided imagery, but has a high risk of increasing the patient’s physical activity, which could complicate the dentist’s work.
- Passive distraction requires only visual or auditory ability, such as:
- –
- Audiovisual media: Several studies have been published in recent decades. Prabhakar compared two different distraction techniques in his study: auditory and audiovisual techniques using a television. The authors concluded that the audiovisual technique outperformed the auditory one [9].
- –
- Auditory distraction: The concept was first used in 1959 by Gardner and Licklander. They showed that the use of music during a stressful process results in a feeling of relaxation and pain relief. Experts such as Bonny, Gfeller and Guzzetta suggest that music has a great distracting power in promoting the patient’s positive feelings of physical and mental relaxation by redirecting their attention to more pleasant emotional states and blocking unpleasant environmental sounds, such as in [2].
- –
- Virtual reality (VR) through the use of glasses or goggles: VR is a human–computer interface that creates a realistic 3D environment that provides different sensory stimuli (visual and auditory) through the use of glasses, thus blocking the outside and promoting patient distraction. Some studies have found that the use of VR is effective in reducing anxiety and pain perception by reducing negative emotions and increasing positive ones, but this technology, like any other, has its limitations in behavioral management, since it can only be used in single dental procedures, and it is necessary for the dentist to have adequate time control.
- –
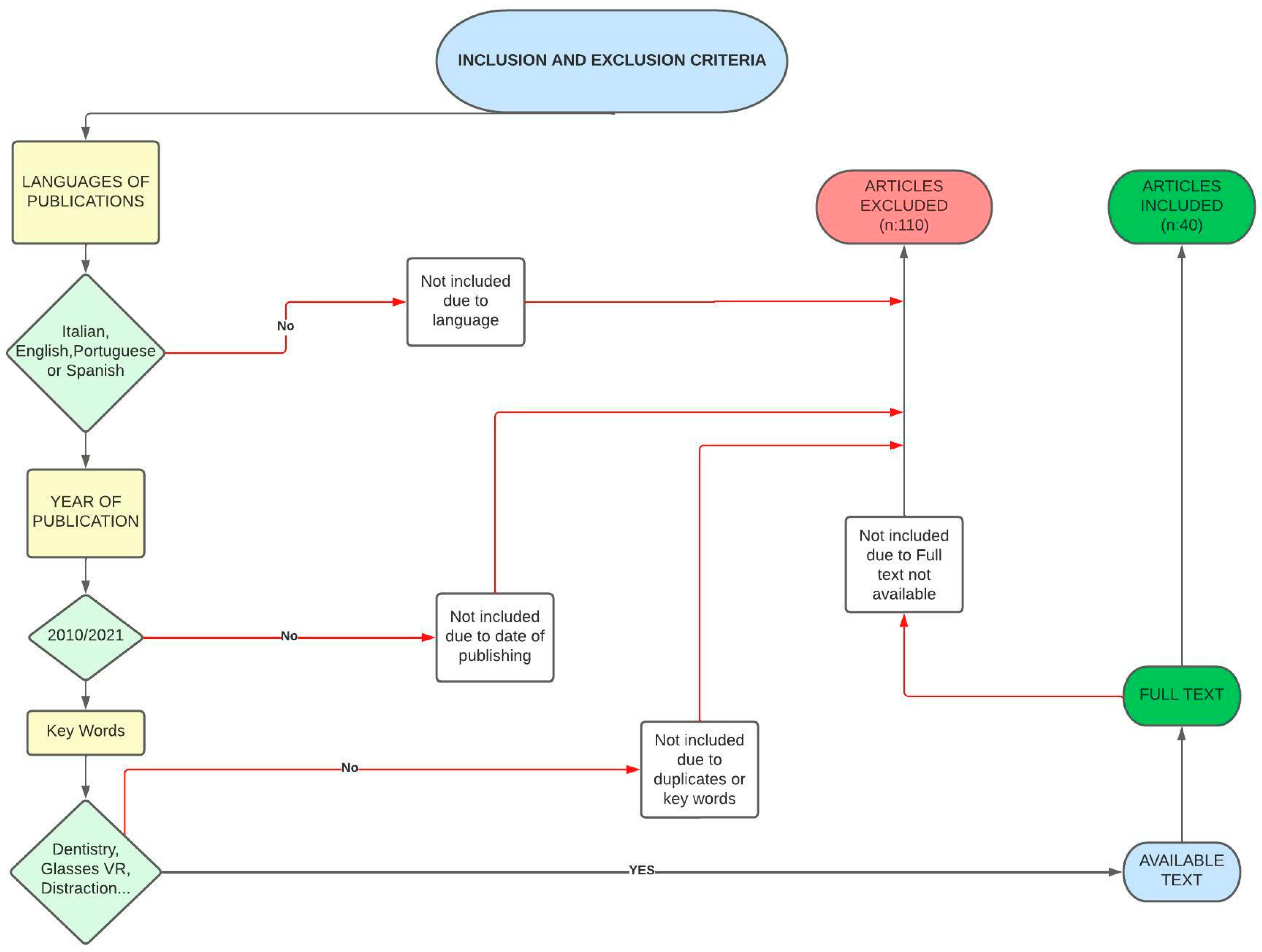
2. Materials and Methods
- Main objective:
- –
- To know the effectiveness of the use of virtual reality glasses as a distraction in a pediatric dentistry consultation.
- Secondary objective:
- –
- To analyze whether the use of virtual reality reduces anxiety during a pediatric dentistry consultation.
3. Results and Discussion
- Whether the patient wears glasses and whether VR glasses can be worn over the patient’s glasses without discomfort;
- The size of the glasses and the child, as they may be too large for very small patients.
- Oral prophylaxis: the study group obtained a mean pain score of 0.35, significantly lower than that of the control group, which was 1.10, and the pulse rate results were not statistically significant between the two groups.
- Dental restoration: the mean pain score was 1.25 for the study group and 2.05 for the control group, which makes it statistically significant; the pulse rate was lower for the study group with a total of 113.35, whereas it was 117.7 for the control group, a statistically significant difference.
- Pulpectomy: the study group had a lower score of 2.20, while the control group had a score of 3.55, which is statistically significant; the score obtained for the pulse frequency for this type of treatment was not statistically significant.
- Children with high levels of anxiety did not respond well to these methods, as they do not eliminate full visual access, and not all children knew how to use the video game technique, so it was necessary to explain its use to them beforehand.
- The subjective assessment of pain using the Wong–Baker Face scale was used, and significant differences were observed.
- The objective assessment of pain during treatment showed a score of 6.77 at the beginning of treatment, a decrease to 2.57 during treatment and 0.24 at the end of treatment, which were significant results.
- The assessment of anxiety was studied by means of two factors:
- –
- The pulse rate was 93.53 at the beginning of treatment and 95.97 at the end of treatment.
- –
- The evaluation of oxygen saturation showed a nonsignificant increase compared to the beginning of the treatment.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guinot, F.; Mayné, R.; Barbero, V.; Sáez, S.; Martínez, P.; Bellet, I.J. Behavioral management through audiovisual media. Odontol. Pediátr. 2004, 12, 88–92. [Google Scholar]
- Guinot, F.; Mercadé, M.; Oprysnyk, L.; Veloso, A.; Boj, J.R. Comparison of active versus passive audiovisual distraction tools on children’s behaviour, anxiety and pain in paediatric dentistry: A randomised crossover clinical trial. EJPD 2021, 22, 230–236. [Google Scholar]
- Fonseca, L.; Sanchis, C. Comparative analysis between different scales for assessing dental behavior, anxiety and fear in pediatric dentistry. Therapeía 2013, 81–95. [Google Scholar]
- Marcano, A.; Figueredi, A.; Orozco, G. Evaluation of anxiety and fear in school children in pediatric dentistry. Rev. Odontopediatr. Latinoam. 2021, 2, 65–71. [Google Scholar]
- Alfaro, L.; Ramos, K.; Redondo, A.; Rangel, T.; González, F. Intervention to Reduce Dental Fear and Anxiety in Children Aged 5 to 9 Years. Ph.D. Thesis, University of Cartagena, Bolivar, Venezuela, 2014. [Google Scholar]
- Krishnappa, S.; Srinath, S.; Vishwanath, S.K.; Bhardwaj, P.; Singh, R. Evaluation of Facial Image Scale and Venham Picture Test Used to Assess Dental Anxiety in Children. JIAPHD 2013, 11, 31–35. [Google Scholar]
- Ramirez, A.; Haro, M.; Hernandez, C.; Gastelum, G. Anxiety level in patients prior to their dental care at the first level of care. Rev. Tamé 2019, 8, 860–862. [Google Scholar]
- Gutierrez, A.; Mirella, A.; Díaz, W.; Xiomi, F. Evaluation of Dental Anxiety Applying 3 Scales in Children Attending a University Health Center for the First Time. Ph.D. Thesis, Universidad Peruana de Ciencias Aplicadas, Lima, Peru, 2017. [Google Scholar]
- Nunna, M.; Dasaraju, R.; Kamatham, R.; Mallineni, S.; Nuvvula, S. Comparative evaluation of virtual reality distraction and counter—Stimulation on dental anxiety and pain perception in childer. J. Dent. Anesth. Pain Med. 2019, 19, 277–288. [Google Scholar] [CrossRef]
- Cusme, E. Research Topic: Effectiveness of Nitrous Oxide in Pediatric Dentistry. Ph.D. Thesis, University of Guayaquil, Av. Delta, Guayaquil, 2020. [Google Scholar]
- Yahaya, W.; Salam, S. Smiley Faces: Scales Measurement for Children Assessment. In Proceedings of the 2nd International Malaysian, Kuantan, Malaysia, 4–7 November 2008. [Google Scholar]
- Guinot, F. Effect of the Use and Different Audiovisual Devices during Dental Treatment in Child Patients. Ph.D. Thesis, International University of Catalonia, Barcelona, Spain, 2014. [Google Scholar]
- Orellana, J.; Morales, V.; González, M. Wong-Baker FACES® Visual Analog Scale and its Utility in Pediatric Dentistry. Health Manag. 2018, 5, 51–57. [Google Scholar]
- Rodriguez, C.; Escobar, F.; Soto, L. Temporomandibular disorders in children and adolescents. Rev. Gastrohnup. 2015, 17, 10–17. [Google Scholar]
- Soria, J. Dental Anxiety in Children Subjected to Conscious Sedation at the San Antonio Dental Clinic in the City of Huancayo. Ph.D. Thesis, Escuela Académica Profesional de Odontología de Huancayo, Huancayo, Peru, 2017. [Google Scholar]
- Koticha, P.; Katge, F.; Shetty, S.; Patil, D. Effectiveness of virtual reality eyeglasses as a distraction Aid to reduce anxiety among 6-10-year-old children undergoing dental extraction procedure. IJPD 2019, 12, 297–302. [Google Scholar]
- Gomez, R.; Durán, L.; Cabra, L.; Pinzón, C.; Rodríguez, N. Music therapy for the control of dental anxiety in children with Down syndrome. Hacia Promoc. Salud 2012, 17, 13–24. [Google Scholar]
- Zafra, M.; Medino, J.; Navas, L.; Hernando, P. Finger pulse oximeter: A new tool for self-monitoring in arma? Rev. Pediatr. Aten. Primaria 2014, 16, 317–320. [Google Scholar]
- Niederbacher, J.; García, M.; Gómez, G. Reference values of arterial oxygen saturation by pulse oximetry in healthy children in Bucaramanga. MedUNAB 2003, 6, 63–69. [Google Scholar]
- Mafla, A.; Villalobos, F.; Pinchao, W.; Lucero, D. Psychometric properties of the Spanish Version of the Abeer Children Dental Anxiety Scale (ACDAS) for the Measurement of Dental Anxiety in Children. Int. J. Odontostomat. 2017, 11, 182–191. [Google Scholar] [CrossRef] [Green Version]
- Flores, G.; Crespo, M. Anxiety Knowledge and Behavior Prior to Pediatric Dentistry Care in Stomatology Students of the University of Huancayo Franklin Roosevelt. Ph.D. Thesis, University of Huancayo Franklin Roosevelt, Huancayo, Peru, 2021. [Google Scholar]
- Mazurek, J.; Pérez, C.; Fernández, C.; Magnot, J.; Magnot, T. The 5 item likert scale and Percentage Scale Correspondence with Implications for the Use of Models with (fuzzy) Linguistic Variables. Rev. Met. Quant. 2021, 31, 3–16. [Google Scholar] [CrossRef]
- Rivera, A.; González, M.; Rangel, C.; Trique, C.; Bustos, A.; Palmet, S.; Lence, E.; Mora, I.; Bautista, G. Behavior and perception of pain in Colombian children undergoing surface electromyography. Vital Dent. 2017, 26, 21–28. [Google Scholar]
- Loayza, S.; Azanza, S. Effectiveness of two conditioning techniques for the care of children 6 to 10 years of age from a public scale in Quito-Ecuador. ALOP 2017, 7, 106–115. [Google Scholar]
- Munayco, E.; Mattos, M.; Torres, G.; Blanco, D. Relationship between anxiety, parental dental fear and children’s collaboration to dental treatment. Odovtos Int. J. Dent. Sci. 2018, 20, 81–91. [Google Scholar]
- Cabeza, C.; Ortiz, G.; Mancilla, H.; Mondragón, T.; Avecilla, P. Evolution of Behavior According to Frankl’s Scale in Children Aged 4 to 8 Years Who Attend the Pediatric Dentistry Postgraduate Course at the FMUAQ. Ph.D. Thesis, University of Querétaro, Cerro de las Campanas, Mexico, 2012. [Google Scholar]
- Charvin, P. A Influência da Música em Odontopediatria: Uma Revisão Sistemática Integrativa. Ph.D. Thesis, CESPU, Gandra, Portugal, 2021. [Google Scholar]
- Prabhakar, A.; Marwah, N.; Raju, O. A comparison between audio and audiovisual distraction techniques in managing anxious pediatric dental patients. J. Indian Soc. Pedod. Prev. Dent. 2007, 25, 177–182. [Google Scholar]
- Cunningham, A.; McPolin, O.; Fallis, R.; Coyle, C.; Best, P.; McKennan, G. A Systematic review of the use of virtual reality or dental smathphone applications as interventions for management of pediatric dental anxiety. BMC Oral. Health 2021, 21, 2–11. [Google Scholar] [CrossRef]
- García, M.; Paulo, J.; Martínez, M.; Teller, C.; Guitiérrez, A.; Gutiérrez, M.; Cárdenas, J.; Cadavid, P.; Jaramillo, A. Development of virtual environments for the distraction of children between 4 and 6 years of age. CES Odont. Rev. 2003, 16, 35–41. [Google Scholar]
- Roa, D.; Havale, R.; Nagaraj, N.; Karobari, N.; Latha, A.; Tharay, N.; Shrutha, S. Assessment of efficacy of virtual reality distraction in reducing pain perception and anxiety in children aged 6–10 years: A behavioral interventional study. IJCPD 2019, 12, 510–513. [Google Scholar]
- Ran, L.; Zhao, N.; Fan, L.; Zhou, P.; Zhang, C.; Yu, C. Application of virtual reality on non-drug behavioral management of short-term dental procedure in children. Trials 2021, 22, 2–9. [Google Scholar] [CrossRef]
- Venham, L.; Goldstein, M.; Goulin, E.; Peteros, K.; Cohan, J.; Faiybanks, J. Effectiveness of a distraction technique in managing young dental patients. Pediatr. Dent. 1981, 3, 7–11. [Google Scholar]
- Rodriguez, N.; Olmo, R.; Mourelle, R.; Gallardo, N. Study of childhood anxiety before dental treatment. Dent. Gaz. 2008, 195, 150–163. [Google Scholar]
- Ram, D.; Shapira, J.; Holan, G.; Mahora, F.; Cohen, S.; Davidovich, E. Audiovisual video eyeglass distraction during dental treatment in children. Quintessence Int. 2010, 41, 673–679. [Google Scholar]
- Haytham, F.; Azza, A.; Mahmoud, A. Effectiveness of New Distraction Technique on Pain Associated with Injection of Local Anesthesia for Children. Ped. Dent. 2012, 34, 142–145. [Google Scholar]
- Chaturvedi, S.; Walimbe, H.; Karekar, P.; Nalawade, H.; Nankar, M.; Nene, K. Comparative evaluation of anxiety level during the conventional dental procedures with and without audiovisual distraction eyeglasses in pediatric dental patients. J. Int. Oral Health 2016, 8, 1016. [Google Scholar]
- Felemban, O.; Alshamarani, R.; Aljeddawi, D.; Bagher, S. Effect of virtual distraction on pain and anxiety during infiltration anesthesia in pediatric patients: A randomized clinical trial. BMC Oral. Health 2021, 21, 321. [Google Scholar] [CrossRef]
- Shetty, V.; Suresh, L.; Hegde, A. Effect of Virtual Reality Distraction on Pain and Anxiety during Dental Treatment in 5 to 8 Year Old Children. IJCPD 2019, 2, 97–101. [Google Scholar] [CrossRef]
- Kim, I.H.; Cho, H.; Song, J.S.; Park, W.; Shin, Y.; Lee, K.E. Assessment of Real-Time Active Noise Control Devices in Dental Treatment Conditions. Int. J. Environ. Res. Public Health 2022, 19, 9417. [Google Scholar] [CrossRef] [PubMed]
- Vitale, M.C.; Gallo, S.; Pascadopoli, M.; Alcozer, R.; Ciuffreda, C.; Scribante, A. Local anesthesia with SleeperOne S4 computerized device vs traditional syringe and perceived pain in pediatric patients: A randomized clinical trial. J. Clin. Pediatr. Dent. 2023, 47, 82–90. [Google Scholar] [PubMed]


{kind=link}
| Author (Year) | Virtual Reality Glasses | Audiovisual Goggles | Other Methods | Measurement of Anxiety Levels * | Efficacy of the Method ** |
|---|---|---|---|---|---|
| Venham et al. (1981) [33] | TV programs | NO | YES | ||
| Prabhakar et al. (2007) [28] | Audiovisual distraction | NO | YES | ||
| Ram et al. (2010) [35] | YES | NO | YES | ||
| Haytham et al. (2012) [36] | YES | DECREASED WITH DISTRACTION | YES | ||
| Chaturvedi et al. (2016) [37] | YES | DECREASED WITH DISTRACTION | YES | ||
| Shetty et al. (2019) [39] | YES | DECREASED WITH DISTRACTION | YES | ||
| Roa et al. (2019) [31] | YES | DECREASED WITH DISTRACTION | YES | ||
| Koticha et al. (2019) [16] | YES | NOT DECREASED WITH DISTRACTION | YES | ||
| Felemban et al. (2021) [38] | YES | DECREASED WITH DISTRACTION | YES | ||
| Ran et al. (2021) [32] | YES | DECREASED WITH DISTRACTION | YES | ||
| Guinot et al. (2021) [2] | YES | DECREASED WITH DISTRACTION | YES |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Constantini Leopardi, A.; Adanero Velasco, A.; Espí Mayor, M.; Miegimolle Herrero, M. Effectiveness of Virtual Reality Goggles as Distraction for Children in Dental Care—A Narrative Review. Appl. Sci. 2023, 13, 1307. https://doi.org/10.3390/app13031307
Constantini Leopardi A, Adanero Velasco A, Espí Mayor M, Miegimolle Herrero M. Effectiveness of Virtual Reality Goggles as Distraction for Children in Dental Care—A Narrative Review. Applied Sciences. 2023; 13(3):1307. https://doi.org/10.3390/app13031307
Chicago/Turabian StyleConstantini Leopardi, Alessandra, Alberto Adanero Velasco, Miguel Espí Mayor, and Monica Miegimolle Herrero. 2023. "Effectiveness of Virtual Reality Goggles as Distraction for Children in Dental Care—A Narrative Review" Applied Sciences 13, no. 3: 1307. https://doi.org/10.3390/app13031307
APA StyleConstantini Leopardi, A., Adanero Velasco, A., Espí Mayor, M., & Miegimolle Herrero, M. (2023). Effectiveness of Virtual Reality Goggles as Distraction for Children in Dental Care—A Narrative Review. Applied Sciences, 13(3), 1307. https://doi.org/10.3390/app13031307