
Adjuvant Effects of Lavandula angustifolia Oil in Experimental Carrageenan-Induced Thrombosis

 ,
,  , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
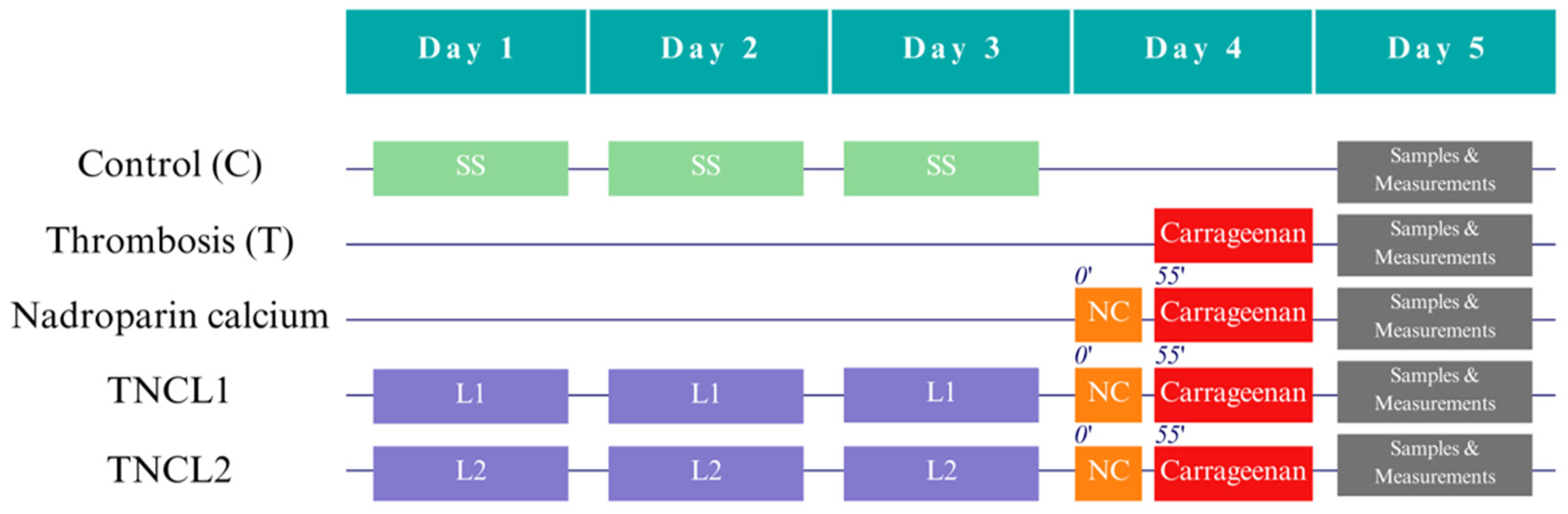
2.1. Study Design
2.2. Measurements
2.3. Statistical Methods
3. Results
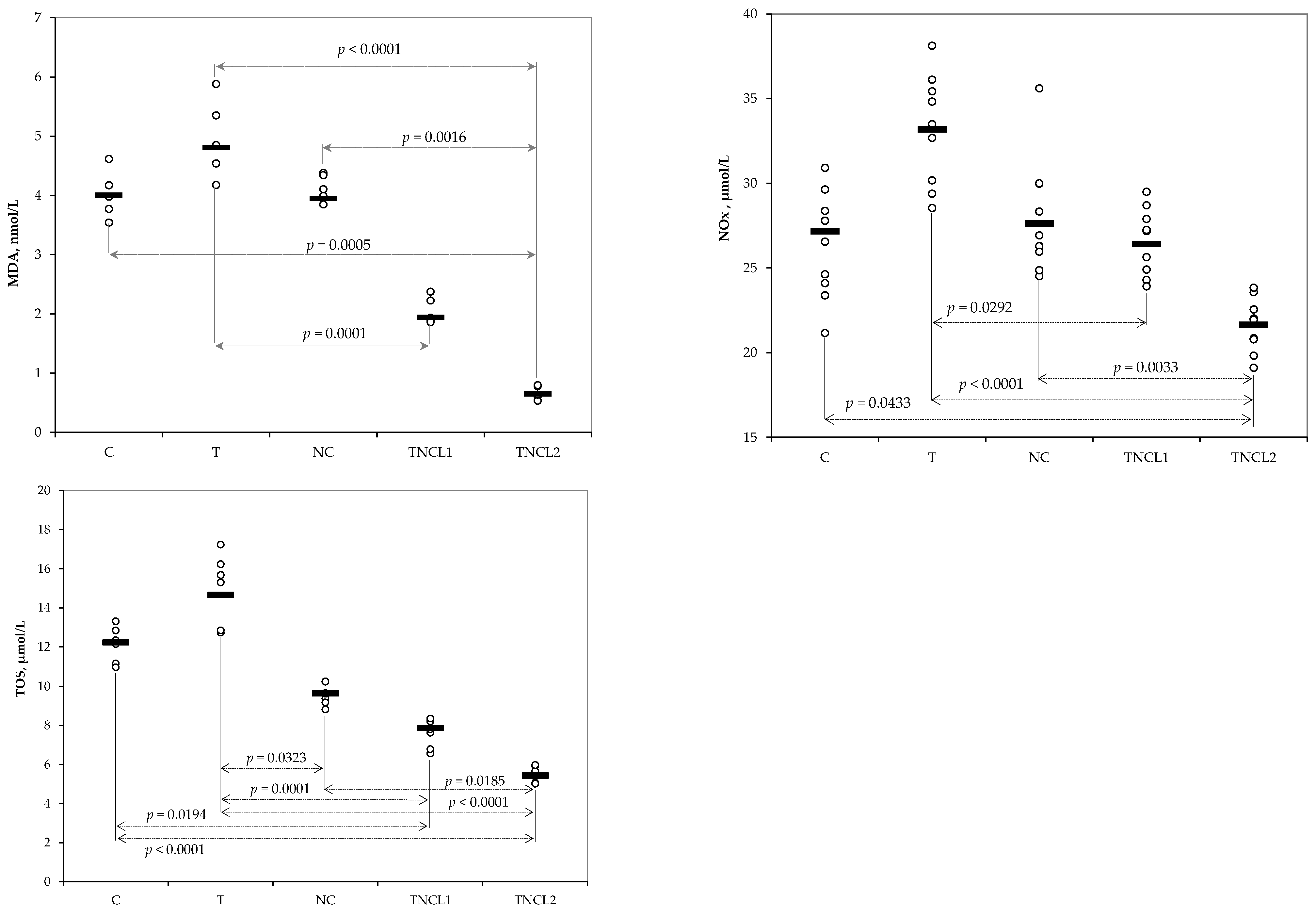
3.1. Levels of Oxidative Stress Parameters
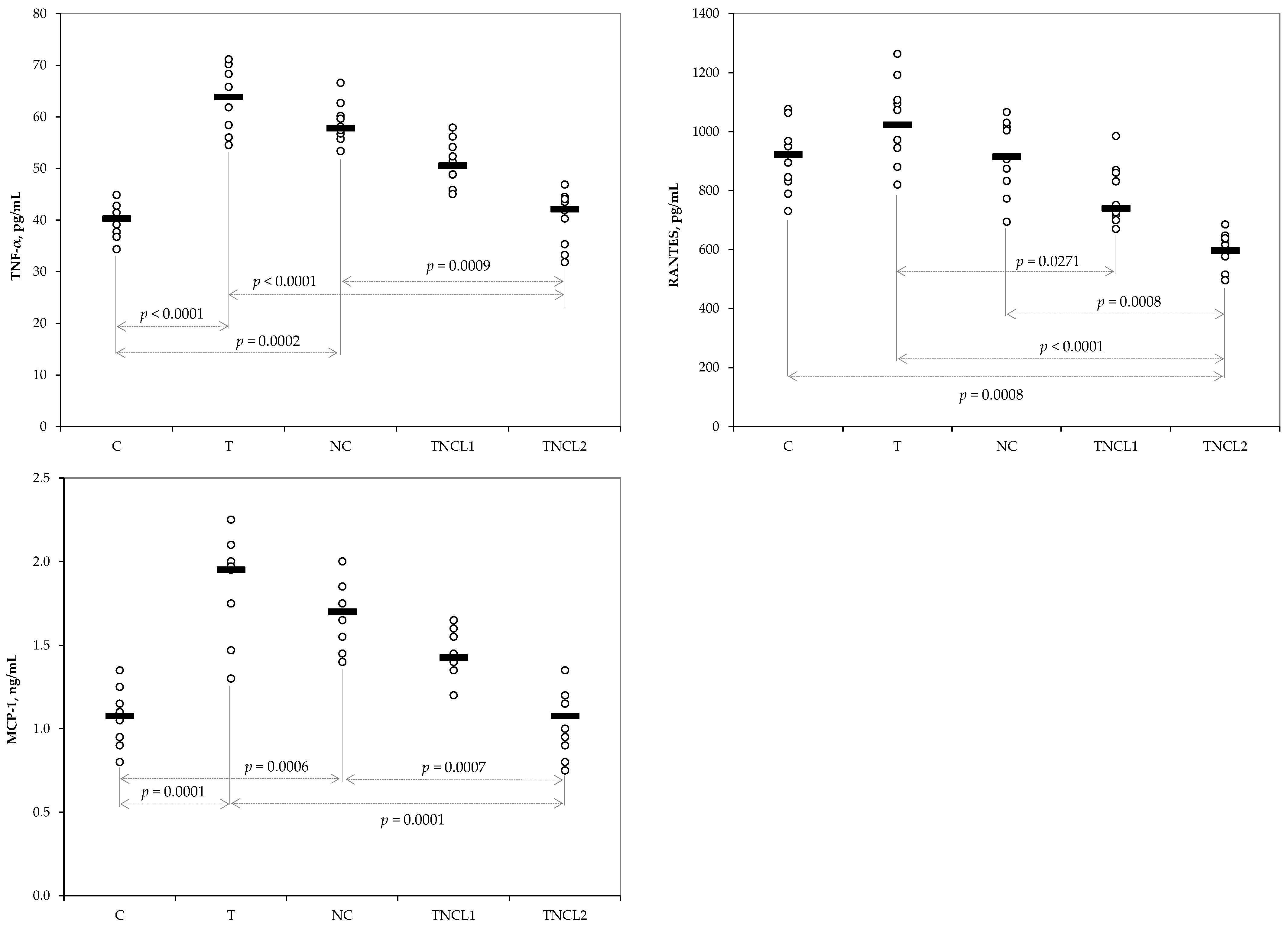
3.2. Plasma Levels of Inflammatory Cytokines
3.3. Variation of Bleeding and Clotting Time and Thrombus Length
3.4. Renal and Liver Functions
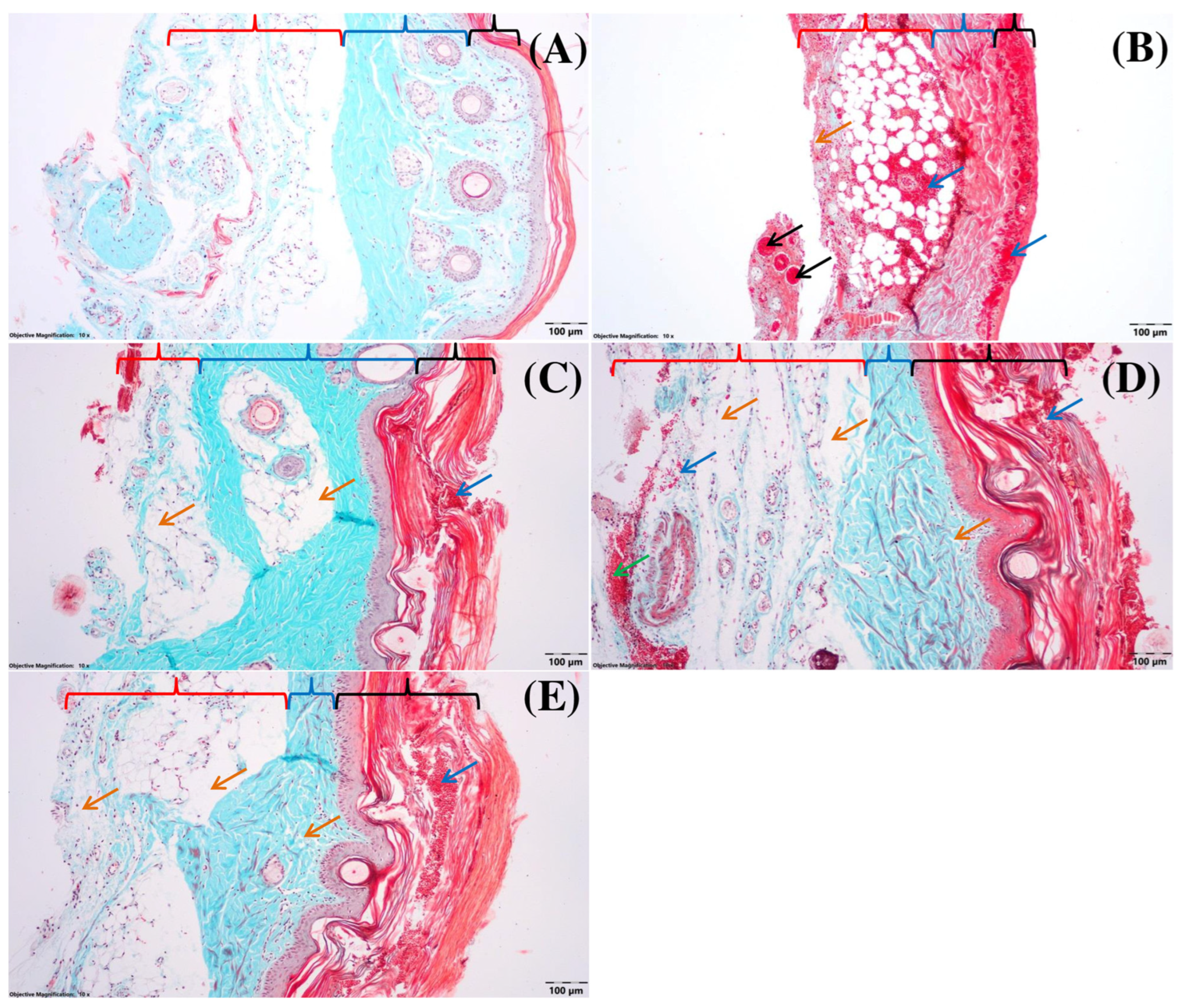
3.5. Histological Assay
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wendelboe, A.M.; Raskob, G.E. Global Burden of Thrombosis: Epidemiologic Aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef]
- ISTH Steering Committee for World Thrombosis Day. Thrombosis: A major contributor to the global disease burden. J. Thromb. Haemost. 2014, 12, 1580–1590. [Google Scholar] [CrossRef]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.J.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Martin, K.A.; Molsberry, R.; Cuttica, M.J.; Desai, K.R.; Schimmel, D.R.; Khan, S.S. Time Trends in Pulmonary Embolism Mortality Rates in the United States, 1999 to 2018. J. Am. Heart Assoc. 2020, 9, e016784. [Google Scholar] [CrossRef] [PubMed]
- Lutsey, P.L.; Zakai, N.A. Epidemiology and prevention of venous thromboembolism. Nat. Rev. Cardiol. 2023, 20, 248–262. [Google Scholar] [CrossRef] [PubMed]
- Brækkan, S.K.; Hansen, J.B. VTE epidemiology and challenges for VTE prevention at the population level. Thromb. Update 2023, 10, 100132. [Google Scholar] [CrossRef]
- Siegal, D.M.; Eikelboom, J.W.; Lee, S.F.; Rangarajan, S.; Bosch, J.; Zhu, J.; Yusuf, S. Venous Thromboembolism Collaboration. Variations in incidence of venous thromboembolism in low-, middle-, and high-income countries. Cardiovasc. Res. 2021, 117, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P.; Noventa, F.; Ghirarduzzi, A.; Pengo, V.; Bernardi, E.; Pesavento, R.; Iotti, M.; Tormene, D.; Simioni, P.; Pagnan, A. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1626 patients. Haematologica 2007, 92, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Naess, I.A.; Christiansen, S.C.; Romundstad, P.; Cannegieter, S.C.; Rosendaal, F.R.; Hammerstrøm, J. Incidence and mortality of venous thrombosis: A population-based study. J. Thromb. Haemost. 2007, 5, 692–699. [Google Scholar] [CrossRef] [PubMed]
- De Azeredo, E.L.; Monteiro, R.Q.; de-Oliveira Pinto, L.M. Thrombocytopenia in Dengue: Interrelationship between Virus and the Imbalance between Coagulation and Fibrinolysis and Inflammatory Mediators. Mediat. Inflamm. 2015, 2015, 313842. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, B.; Wu, J.; Yu, H.; Huang, H.; Chen, X.; Chen, B.; Wu, S.; Ma, J.; Liu, W.; et al. The inhibitory effect of tachyplesin I on thrombosis and its mechanisms. Chem. Biol. Drug Des. 2019, 94, 1672–1679. [Google Scholar] [CrossRef] [PubMed]
- Barradell, L.B.; Buckley, M.M. Nadroparin Calcium1: A Review of its Pharmacology and Clinical Applications in the Prevention and Treatment of Thromboembolic Disorders. Drugs 1992, 44, 858–888. [Google Scholar] [CrossRef] [PubMed]
- Casu, B.; Oreste, P.; Torri, G.; Zoppetti, G.; Choay, J.; Lormeau, J.C.; Petitou, M.; Sinac, P. The structure of heparin oligosaccharide fragments with high anti-(factor Xa) activity containing the minimal antithrombin III-binding sequence. Chemical and 13C nuclear-magnetic-resonance studies. Biochem. J. 1981, 197, 599–609. [Google Scholar] [CrossRef]
- Zhong, G.L.; Gong, Y.; Yu, C.; Wu, S.; Ma, Q.; Wang, Y.; Ren, J.; Zhang, X.-C.; Yang, W.-H.; Zhu, W. Significantly inhibitory effects of low molecular weight heparin (Fraxiparine) on the motility of lung cancer cells and its related mechanism. Tumor Biol. 2015, 36, 4689–4697. [Google Scholar] [CrossRef]
- Souri, F.; Rakhshan, K.; Erfani, S.; Azizi, Y.; Nasseri Maleki, S.; Aboutaleb, N. Natural lavender oil (Lavandula angustifolia) exerts cardioprotective effects against myocardial infarction by targeting inflammation and oxidative stress. Inflammopharmacology 2019, 27, 799–807. [Google Scholar] [CrossRef]
- Białoń, M.; Krzyśko-Łupicka, T.; Nowakowska-Bogdan, E.; Wieczorek, P.P. Chemical Composition of Two Different Lavender Essential Oils and Their Effect on Facial Skin Microbiota. Molecules 2019, 24, 3270. [Google Scholar] [CrossRef]
- Pandur, E.; Balatinácz, A.; Micalizzi, G.; Mondello, L.; Horváth, A.; Sipos, K.; Horváth, G. Anti-inflammatory effect of lavender (Lavandula angustifolia Mill.) essential oil prepared during different plant phenophases on THP-1 macrophages. BMC Complement Med. Ther. 2021, 21, 287. [Google Scholar] [CrossRef]
- Giovannini, D.; Gismondi, A.; Basso, A.; Canuti, L.; Braglia, R.; Canini, A.; Mariani, F.; Cappeli, G. Lavandula angustifolia Mill. Essential Oil Exerts Antibacterial and Anti-Inflammatory Effect in Macrophage Mediated Immune Response to Staphylococcus aureus. Immunol. Investig. 2016, 45, 11–28. [Google Scholar] [CrossRef]
- Cardia, G.F.E.; Silva-Filho, S.E.; Silva, E.L.; Uchida, N.S.; Cavalcante, H.A.O.; Cassarotti, L.L.; Salvadego, V.E.C.; Spironello, R.A.; Bersani-Amado, C.A.; Cuman, R.K.N. Effect of Lavender (Lavandula angustifolia) Essential Oil on Acute Inflammatory Response. Evid. Based Complement. Altern. Med. 2018, 2018, 1413940. [Google Scholar] [CrossRef]
- Silva, G.L.; Luft, C.; Lunardelli, A.; Amaral, R.H.; Melo, D.A.; Donadio, M.V.; Nunes, F.B.; Azambuja, M.S.D.; Santana, J.C.; Moraes, C.M.B. Antioxidant, analgesic and anti-inflammatory effects of lavender essential oil. An. Acad. Bras. Cienc. 2015, 87, 1397–1408. [Google Scholar] [CrossRef]
- Hawrył, A.; Hawrył, M.; Waksmundzka-Hajnos, M. Liquid chromatography fingerprint analysis and antioxidant activity of selected lavender species with chemometric calculations. PLoS ONE 2019, 14, e0218974. [Google Scholar] [CrossRef] [PubMed]
- Ben Salah, M.; Abderraba, M.; Tarhouni, M.R.; Abdelmelek, H. Effects of ultraviolet radiation on the kinetics of in vitro percutaneous absorption of lavender oil. Int. J. Pharm. 2009, 382, 33–38. [Google Scholar] [CrossRef] [PubMed]
- But, V.M.; Bulboacă, A.E.; Rus, V.; Ilyés, T.; Gherman, M.L.; Bolboacă, S.D. Anti-inflammatory and antioxidant efficacy of lavender oil in experimentally induced thrombosis. Thromb. J. 2023, 21, 85. [Google Scholar] [CrossRef] [PubMed]
- Boarescu, I.; Pop, R.M.; Boarescu, P.-M.; Bocsan, I.C.; Gheban, D.; Bulboaca, A.E.; Buzoianu, A.D.; Bolboaca, S.D. Ginger (Zingiber officinale) Root Capsules Enhance Analgesic and Antioxidant Efficacy of Diclofenac Sodium in Experimental Acute Inflammation. Antioxidants 2023, 12, 745. [Google Scholar] [CrossRef] [PubMed]
- Hagimori, M.; Kamiya, S.; Yamaguchi, Y.; Arakawa, M. Improving frequency of thrombosis by altering blood flow in the carrageenan-induced rat tail thrombosis model. Pharmacol. Res. 2009, 60, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Kod’ousek, R.; Jezdínský, J.; Krajcí, D. Histological and ultrastructural changes of cardiomyocytes in experimental rats with tail thrombosis following subplantar application of carrageenin. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2007, 16, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Weissgerber, T.L.; Milic, N.M.; Winham, S.J.; Garovic, V.D. Beyond bar and line graphs: Time for a new data presentation paradigm. PLoS Biol. 2015, 13, e1002128. [Google Scholar] [CrossRef] [PubMed]
- Lei, Y.; Wang, K.; Deng, L.; Chen, Y.; Nice, E.C.; Huang, C. Redox Regulation of Inflammation: Old Elements, a New Story: Redox Modifications in Inflammation. Med. Res. Rev. 2015, 35, 306–340. [Google Scholar] [CrossRef]
- Medcalf, R.L. Fibrinolysis, inflammation, and regulation of the plasminogen activating system. J. Thromb. Haemost. 2007, 5, 132–142. [Google Scholar] [CrossRef]
- Stark, K.; Massberg, S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat. Rev. Cardiol. 2021, 18, 666–682. [Google Scholar] [CrossRef]
- Kuijpers, M.J.E.; Heemskerk, J.W.M.; Jurk, K. Molecular Mechanisms of Hemostasis, Thrombosis and Thrombo-Inflammation. Int. J. Mol. Sci. 2022, 23, 5825. [Google Scholar] [CrossRef]
- Sriram, K.; Insel, P.A. Inflammation and thrombosis in COVID-19 pathophysiology: Proteinase-activated and purinergic receptors as drivers and candidate therapeutic targets. Physiol. Rev. 2021, 101, 545–567. [Google Scholar] [CrossRef]
- Rai, V.K.; Sinha, P.; Yadav, K.S.; Shukla, A.; Saxena, A.; Bawankule, D.U.; Tandon, S.; Khan, F.; Chanotiya, C.S.; Yadav, N.P. Anti-psoriatic effect of Lavandula angustifolia essential oil and its major components linalool and linalyl acetate. J. Ethnopharmacol. 2020, 261, 113127. [Google Scholar] [CrossRef]
- Aykal, G.; Güven, R.; Yeğin, A.; Ellidağ, H.Y.; Bayindir, A.; Yilmaz, N. The Diagnostic Value of Oxidative/Antioxidative Balance Parameters in Venous Thromboembolism. Clin. Lab. 2015, 61, 769–775. [Google Scholar] [CrossRef]
- Türker, F.S.; Malbora, A.; Erisir, M. Oxidative status and antioxidant enzyme levels in deep venous thrombosis patients. Am. J. Cardiovasc. Dis. 2021, 11, 176–183. [Google Scholar]
- Aboutaleb, N.; Jamali, H.; Abolhasani, M.; Pazoki Toroudi, H. Lavender oil (Lavandula angustifolia) attenuates renal ischemia/reperfusion injury in rats through suppression of inflammation, oxidative stress and apoptosis. Biomed. Pharmacother. 2019, 110, 9–19. [Google Scholar] [CrossRef]
- Amer, S.A.; Abdel-Wareth, A.A.A.; Gouda, A.; Saleh, G.K.; Nassar, A.H.; Sherief, W.R.I.A.; Albogami, S.; Shalaby, S.I.; Abdelazim, A.M.; Abomughaid, M.M.I. Impact of Dietary Lavender Essential Oil on the Growth and Fatty Acid Profile of Breast Muscles, Antioxidant Activity, and Inflammatory Responses in Broiler Chickens. Antioxidants 2022, 11, 1798. [Google Scholar] [CrossRef]
- Plastina, P.; Apriantini, A.; Meijerink, J.; Witkamp, R.; Gabriele, B.; Fazio, A. In Vitro Anti-Inflammatory and Radical Scavenging Properties of Chinotto (Citrus myrtifolia Raf.) Essential Oils. Nutrients 2018, 10, 783. [Google Scholar] [CrossRef] [PubMed]
- Sadeghzadeh, J.; Vakili, A.; Bandegi, A.R.; Sameni, H.R.; Zahedi Khorasani, M.; Darabian, M. Lavandula Reduces Heart Injury via Attenuating Tumor Necrosis Factor-Alpha and Oxidative Stress in A Rat Model of Infarct-Like Myocardial Injury. Cell J. 2017, 19, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Xu, H.; Wu, J.; Qu, C.; Sun, F.; Xu, S. Linalool inhibits cigarette smoke-induced lung inflammation by inhibiting NF-κB activation. Int. Immunopharmacol. 2015, 29, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Kursat Poyrazoglu, O.; Dogukan, A.; Yalnız, M.; Seckin, D.; lhsan Gunal, A. Acute Effect of Standard Heparin Versus Low Molecular Weight Heparin on Oxidative Stress and Inflammation in Hemodialysis Patients. Ren. Fail. 2006, 28, 723–727. [Google Scholar] [CrossRef]
- Romano, L.G.R.; Hunfeld, N.G.M.; Kruip, M.J.H.A.; Endeman, H.; Preijers, T. Population pharmacokinetics of nadroparin for thromboprophylaxis in COVID-19 intensive care unit patients. Br. J. Clin. Pharmacol. 2023, 89, 1617–1628. [Google Scholar] [CrossRef]
- Ballabeni, V.; Tognolini, M.; Chiavarini, M.; Impicciatore, M.; Bruni, R.; Bianchi, A.; Barocelli, E. Novel antiplatelet and antithrombotic activities of essential oil from Lavandula hybrida Reverchon “grosso”. Phytomedicine 2004, 11, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Venmathi Maran, B.A.; Iqbal, M.; Gangadaran, P.; Ahn, B.C.; Rao, P.V.; Shah, M.D. Hepatoprotective Potential of Malaysian Medicinal Plants: A Review on Phytochemicals, Oxidative Stress, and Antioxidant Mechanisms. Molecules 2022, 27, 1533. [Google Scholar] [CrossRef] [PubMed]
- Dogaru, G.; Bulboaca, A.E.; Gheban, D.; Boarescu, P.M.; Rus, V.; Festila, D.; Sitar-Taut, A.-V.; Stanescu, I. Effect of Liposomal Curcumin on Acetaminophen Hepatotoxicity by Down-regulation of Oxidative Stress and Matrix Metalloproteinases. In Vivo 2020, 34, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Bulboaca, A.E.; Porfire, A.; Bolboaca, S.D.; Nicula, C.A.; Festila, D.G.; Roman, A.; Râjnoveanu, R.M.; Râjnoveanu, A.; Dogaru, G.; Boarescu, P.-M.; et al. Protective Effects of Liposomal Curcumin on Oxidative Stress/Antioxidant Imbalance, Metalloproteinases 2 and -9, Histological Changes and Renal Function in Experimental Nephrotoxicity Induced by Gentamicin. Antioxidants 2021, 10, 325. [Google Scholar] [CrossRef] [PubMed]
- Boarescu, I.; Pop, R.M.; Boarescu, P.-M.; Bocșan, I.C.; Gheban, D.; Râjnoveanu, R.-M.; Râjnoveanu, A.; Bulboacă, A.E.; Buzoianu, A.D.; Bolboacă, S.D. Anti-Inflammatory and Analgesic Effects of Curcumin Nanoparticles Associated with Diclofenac Sodium in Experimental Acute Inflammation. Int. J. Mol. Sci. 2022, 23, 11737. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | MDA, nmol/L | NOx, μmol/L | TOS, μmol H2O2 equiv./L |
|---|---|---|---|
| C | 4 [3.77 to 4.34] | 27.18 [24.23 to 29.32] | 12.23 [11.13 to 12.72] |
| {3.42 to 4.73} | {21.17 to 30.91} | {10.39 to 13.68} | |
| T | 4.81 [4.56 to 5.3] | 33.18 [30.8 to 35.28] | 14.66 [13.88 to 16.09] |
| {4.18 to 5.88} | {28.54 to 38.12} | {12.73 to 17.23} | |
| NC | 3.95 [3.80 to 4.08] | 27.63 [26.05 to 30.00] | 9.64 [9.23 to 10.23] |
| {3.44 to 4.38} | {24.52 to 35.61} | {8.5 to 10.98} | |
| TNCL1 | 1.94 [1.91 to 2.18] | 26.41 [24.67 to 27.73] | 7.87 [7.51 to 8.18] |
| {1.86 to 2.38} | {23.91 to 29.50} | {6.56 to 8.35} | |
| TNCL2 | 0.64 [0.61 to 0.76] | 21.64 [20.80 to 22.42] | 5.43 [5.03 to 5.64] |
| {0.52 to 0.82} | {19.11 to 23.84} | {4.80 to 5.97} | |
| * stat. (p-value) | 43.4 (<0.0001) | 32.8 (<0.0001) | 46.3 (<0.0001) |
| Group | TAC, mmol Trolox/L | THIOL, μmol/L |
|---|---|---|
| C | 1.093 [1.091 to 1.098] | 297.5 [289.25 to 304.25] |
| {1.08 to 1.11} | {269 to 334} | |
| T | 0.98 [0.9 to 0.99] | 243 [214 to 254.5] |
| {0.82 to 1.06} | {204 to 261} | |
| NC | 1.07 [1.06 to 1.07] | 249 [236 to 276.5] |
| {1.05 to 1.08} | {215 to 309} | |
| TNCL1 | 1.086 [1.086 to 1.088] | 271 [254.5 to 282.5] |
| {1.085 to 1.088} | {221 to 305} | |
| TNCL2 | 1.089 [1.086 to 1.094] | 318 [291.3 to 342.8] |
| {1.09 to 1.10} | {282 to 367} | |
| * stat. (p-value) | 40.4 (<0.0001) | 29.9 (<0.0001) |
| Group | TNF-α, pg/mL | RANTES, pg/mL | MCP-1, ng/mL |
|---|---|---|---|
| C | 40.28 [38.08 to 41.21] | 922.68 [835.29 to 985.39] | 1.08 [0.91 to 1.23] |
| {34.38 to 44.92} | {730.45 to 1077.15} | {0.8 to 1.35} | |
| T | 63.85 [58.42 to 69.75] | 1022.75 [949.84 to 1104.55] | 1.95 [1.54 to 1.99] |
| {54.56 to 77.05} | {820.15 to 1263.8} | {1.3 to 2.25} | |
| NC | 57.82 [55.06 to 60.06] | 914.5 [843.34 to 1012.98] | 1.7 [1.58 to 1.85] |
| {52.81 to 66.63} | {694.9 to 1066.55} | {1.4 to 2} | |
| TNCL1 | 50.52 [48.85 to 53.72] | 739.2 [703.98 to 853.64] | 1.43 [1.31 to 1.55] |
| {45.06 to 57.93} | {670.5 to 985.4} | {1.2 to 1.65} | |
| TNCL2 | 42.13 [36.57 to 43.96] | 596.85 [518.06 to 637.93] | 1.08 [0.91 to 1.20] |
| {31.86 to 46.92} | {496.45 to 685.5} | {0.75 to 1.35} | |
| * stat. (p-value) | 41.0 (<0.0001) | 32.4 (<0.0001) | 35.6 (<0.0001) |
| Group | Length, cm | Bleeding Time, s | Clotting Time, s |
|---|---|---|---|
| C | 0 | 168.5 [165.5 to 175.75] | 137 [133 to 140.5] |
| {160 to 178} | {130 to 142} | ||
| T | 9.25 [8.95 to 9.58] | 74.5 [71.5 to 76.75] | 50.5 [47.25 to 52.75] |
| {8.3 to 9.9} | {69 to 81} | {45 to 58} | |
| NC | 0 | 229.5 [228.25 to 231.75] | 178.5 [173 to 181.75] |
| {222 to 241} | {168 to 185} | ||
| TNCL1 | 0 | 276.5 [274 to 281.25] | 224.5 [221.25 to 229.75] |
| {270 to 288} | {217 to 233} | ||
| TNCL2 | 0 | 281 [276.25 to 285.25] | 229 [226.25 to 233.75] |
| {274 to 288} | {221 to 241} | ||
| * stat. (p-value) | n.a. | 45.0 (<0.0001) | 45.2 (<0.0001) |
| Group | Creatinine, mg/dL | Urea, mg/dL | ALT, UI | AST, UI |
|---|---|---|---|---|
| C | 0.86 [0.79 to 0.92] | 49.15 [46.42 to 50.99] | 45.47 [42.61 to 48.24] | 41.93 [38.19 to 43.79] |
| {0.73 to 1.01} | {43.05 to 54.35} | {37.88 to 49.99} | {31.75 to 47.24} | |
| T | 0.98 [0.96 to 1.01] a1 | 54.39 [50.37 to 57.1] | 58.02 [54.69 to 61.45] | 50.64 [45.7 to 53.53] |
| {0.9 to 1.22} | {46.31 to 61.03} | {53.01 to 67.52} | {43.48 to 56.88} | |
| NC | 0.90 [0.88 to 0.96] | 46.63 [45.67 to 49.69] | 42.7 [39.68 to 45.45] | 44.96 [42.85 to 49.95] |
| {0.75 to 0.98} | {44.38 to 52.1} | {38.21 to 52.52} | {39.93 to 52.11} | |
| TNCL1 | 0.90 [0.82 to 0.92] | 45.99 [45.19 to 46.79] b1 | 35.84 [32.95 to 38.97] c1 | 35.95 [33.4 to 38.51] d1,d2 |
| {0.79 to 0.99} | {42.45 to 48.24} | {29.48 to 42.7} | {31.38 to 40.92} | |
| TNCL2 | 0.79 [0.76 to 0.85] a2 | 40.85 [38.06 to 41.93] b2,b3,b4 | 31.03 [29.7 to 33.72] c2,c3,c4 | 29.02 [26.08 to 30.4] d3,d4,d5 |
| {0.71 to 0.87} | {35.03 to 44.38} | {26.43 to 35.95} | {24.4 to 32.4} | |
| * stat. (p-value) | 22.1 (0.0001) | 32.7 (<0.0001) | 40.5 (<0.0001) | 39.5 (<0.0001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
But, V.M.; Rus, V.; Ilyés, T.; Gherman, M.L.; Stănescu, I.C.; Bolboacă, S.D.; Bulboacă, A.E. Adjuvant Effects of Lavandula angustifolia Oil in Experimental Carrageenan-Induced Thrombosis. Appl. Sci. 2024, 14, 1852. https://doi.org/10.3390/app14051852
But VM, Rus V, Ilyés T, Gherman ML, Stănescu IC, Bolboacă SD, Bulboacă AE. Adjuvant Effects of Lavandula angustifolia Oil in Experimental Carrageenan-Induced Thrombosis. Applied Sciences. 2024; 14(5):1852. https://doi.org/10.3390/app14051852
Chicago/Turabian StyleBut, Valeriu Mihai, Vasile Rus, Tamás Ilyés, Mădălina Luciana Gherman, Ioana Cristina Stănescu, Sorana D. Bolboacă, and Adriana Elena Bulboacă. 2024. "Adjuvant Effects of Lavandula angustifolia Oil in Experimental Carrageenan-Induced Thrombosis" Applied Sciences 14, no. 5: 1852. https://doi.org/10.3390/app14051852
APA StyleBut, V. M., Rus, V., Ilyés, T., Gherman, M. L., Stănescu, I. C., Bolboacă, S. D., & Bulboacă, A. E. (2024). Adjuvant Effects of Lavandula angustifolia Oil in Experimental Carrageenan-Induced Thrombosis. Applied Sciences, 14(5), 1852. https://doi.org/10.3390/app14051852