1. Introduction
Shear Wave Elastography (SWE) is a potential diagnostic imaging modality for determining the stiffness of muscles after a stroke. Accurate and early musculoskeletal rehabilitation has a greater chance of reducing post-stroke muscle complications; however, identifying those patients most at need of intervention can be challenging. Current clinical assessments for post-stroke spasticity, such as the Modified Ashworth Scale and Tardieu Scale, are subjective and ordinal scales [
1] that are unable to differentiate between the neural and non-neural components [
2] of altered muscle stiffness. Quantitative, reliable measurements of the muscle stiffness can be achieved by utilising an advanced ultrasound technology: Shear Wave Elastography (SWE). SWE is able to evaluate the passive muscle stiffness and detect changes that occur over time with good correlation to clinical assessments [
3,
4]; however, more investigations are required before SWE can be integrated into the healthcare system. With SWE as a reliable diagnostic tool, stroke survivors may receive earlier interventions or treatments more specific to their individual pathologies, resulting in improved limb function and better stroke recovery.
Prior to applying the technology to stroke survivors, the stiffness of healthy muscles measured by SWE must be investigated in a range of settings and conditions. There are no current protocols for the application of SWE into the musculoskeletal system, in part due to the methodological inconsistencies in current research including participant positions [
5]; however, trends are emerging such as the effect of joint angles. Muscles in a passive state will increase in stiffness when held in their lengthened position (by joint extension or flexion depending on the muscle biomechanics), as well as when actively stretched and actively contracted. This has been demonstrated by an increased Shear Wave Velocity (SWV) [
6], shear modulus [
7,
8,
9,
10], or Young’s modulus [
9] in recent studies. People who have experienced a stroke may not be able to maintain a fully extended elbow joint, thus understanding muscle stiffness measurements at multiple joint angles will allow stroke survivors to receive a diagnostic investigation regardless of their limited arm positions.
Despite the constructive progress of research in musculoskeletal elastography, there has been limited investigations that take into account muscle morphology. The biceps brachii consists of two proximal origins, the short and the long head, and a distal insertion onto the radial tuberosity with an aponeurosis known as Lacertus fibrosis, which inserts on the superficial aponeurosis of the flexor muscles [
11,
12]. The long head of biceps originates on the supraglenoid tubercle in the glenohumeral joint, extends horizontally into the rotator cuff interval, enters the bicipital groove, and sits underneath the transverse humeral ligament; the short head of the biceps’ origin is on the coracoid process of the scapula [
11]. While both the muscle bellies flex the elbow and supinate the forearm, the muscle of the long head of the biceps brachii (LHB) assists slight shoulder abduction. The muscle of the short head of the bicep brachii (SHB) instead assists in shoulder internal rotation, weak flexion, and horizontal adduction, and resists dislocation of the shoulder [
12]. A recent paper by Iwane et al. [
13] showed that the SHB and LHB respond differently to shoulder movements; however, no comparison of the SHB to LHB was commented on. The difference in origin and biomechanics of each bicep brachii muscle belly may create different levels of stiffness between the two.
Previous unpublished research by the authors showed a difference in the SWV between the SHB and LHB at full extension and 30° flexion. This difference in muscle stiffness measured between the two bellies requires further investigation to confirm that muscle stiffness assessments should include consideration of muscle morphology. Therefore, this paper extends on from prior investigations to include the 60° angle and on a larger number of participants. A secondary novel aspect is the use of a different ultrasound machine to confirm the difference between the muscle bellies regardless of vendor.
The research in this paper was undertaken to deepen our understanding of muscle stiffness and the biomechanics of the bicep muscle. Specifically, this paper aims to determine the difference in passive stiffness between the short and long heads of the biceps brachii muscle bellies and how these measurements change with elbow flexion. It is hypothesised that the SHB will have a lower SWV than the LHB and that elbow flexion will decrease the SWV. This paper also aims to determine the reliability of the SWV with each combination of the muscle belly and elbow angle.
Given the limitations of the current clinical assessments, combined with the benefits SWE will provide by detecting changes in stiffness, there is immense potential for the development of a new diagnostic tool for muscle stiffness in the post-stroke population. The information gained from this research will be used to develop a robust SWE research protocol that can be applied to stroke survivors with upper limb impairment. Using SWE to reliably detect quantitative changes instead of the current subjective clinical assessments will lead to potentially earlier diagnosis, increased rehabilitation opportunities, and reduced development of chronic muscle pathologies.
2. Materials and Methods
A total of 38 healthy participants (19 males, 19 females) with a mean (±SD) age of 36.3 (10.5), height of 173.9 cm (8.2), and body mass of 79.4 kg (17.1) were recruited via email advertising through university services. The inclusion criteria were set for participants between 18 and 65 years; the exclusion criteria were set as a history of stroke or a history of injury or surgery to the arm. Ethical approval was sought from the Queensland University of Technology Human Research Ethics Committee (approval number 2000001094), and all participants provided written informed consent.
Participants were positioned supine with their upper arm and wrist resting on the bed comfortably next to their body. The participants were asked to hold a gel bottle so that the hand was in supination and their arm would not inadvertently internally rotate. The distance between the participants’ acromioclavicular joint and the cubital fossa was measured, and the 75% distance was marked on their arms with a skin-safe marker to indicate the site of measurement with the least variability [
14]. The right arm was assessed first with the elbow in full extension at 0° flexion, then with the forearm resting on a 30° wedge, and then on a 60° wedge, as is shown in
Figure 1. The left arm was then assessed in the same pattern.
2.1. Shear Wave Elastography
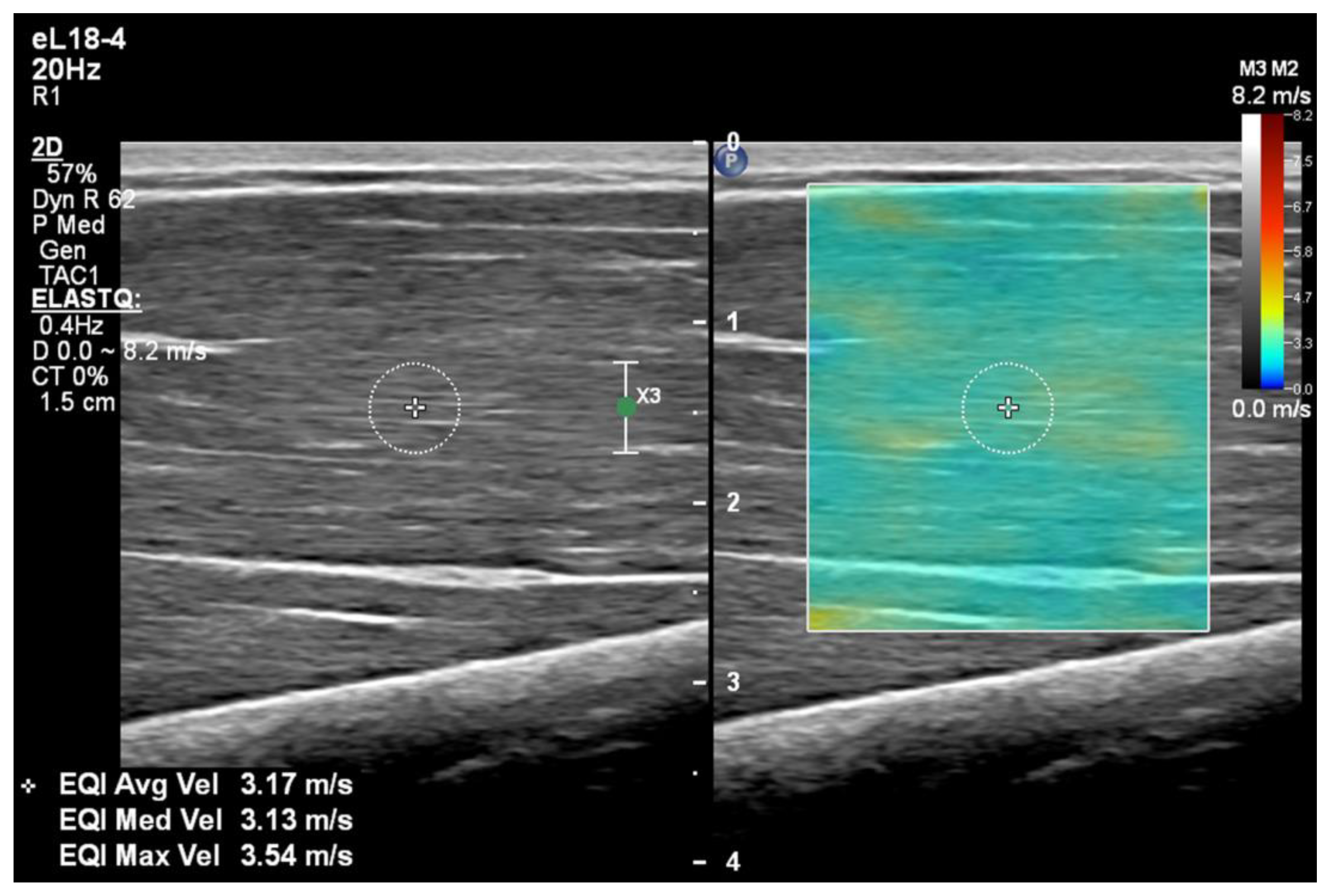
SWE was used to assess the stiffness of the two biceps brachii muscle bellies using a Philips EPIQ Elite (Amsterdam, The Netherlands) with a linear eL18-4 MHz transducer. The SWE and ultrasound assessments were performed by an experienced sonographer. The transducer was placed longitudinally on the arm at the level of the skin mark and adjusted in B-mode to view the fascicles of the muscle in the longest length, with the depth adjusted as required. Using the ElastQ SWE setting on the ultrasound machine, the elastogram box was placed in the mid-depth of the muscle belly.
The participants were asked to relax and not move or contract their muscles during the scan. If the muscle was activated in this way, the SWE would display higher colour maps almost instantly. The participant would then be reminded to relax, and the measurement would be re-taken a few seconds later. Once the elastogram was stable, the image was frozen and a 5 mm calliper was placed in the middle of the elastogram, avoiding any fascia, nerves, or vessels (
Figure 2). The ultrasound machine calculates the velocity of the Shear Wave within the calliper and returns a measurement in m/s. Five measurements were taken in each muscle belly, at each elbow position, in each arm.
2.2. Cross-Sectional Area
The cross-sectional area of the entire biceps muscle was measured at the marked location to determine if the size influenced the SWV. To acquire the cross-sectional area measurement, B-mode was selected, and the transducer was placed in a transverse plane and optimised to improve the resolution of the epimysium. The cross-sectional area was measured by a freehand continuous trace performed by the sonographer on the frozen image and recorded in cm2.
2.3. Statistics
We conducted a regression analysis to predict the SWV based on potential covariates: SWV measurement, side (left, right), elbow angle (full extension, 30° flexed, 60° flexed), muscle belly (SHB, LHB), age, sex, height, and body mass. A Bayesian framework was utilised for this regression analysis, where a log transform was applied to the SWV to improve the normality assumptions. Initially, we considered the relationship between the covariates and our response—a log transform of the SWV—revealing a random slope effect for the elbow angle based on identification (ID) was needed. To determine appropriate covariates, we used a stepwise regression based on Bayesian information criterion (BIC). Our final model includes both the elbow angle, muscle belly, an interaction between them and a random slope effect for the elbow angle based on ID. All statistics were performed using the statistical software R v.4.1 [
15], with the regression models fitted using the BRMS package version 2.17.0 [
16].
Test–retest reliability was calculated to determine the variation in measurements taken on the same subject under the same conditions with the same rater/sonographer. The intraclass correlation coefficient (ICC) with a 95% confidence interval was based on a two-way mixed effects model with absolute agreement, with single measures (3.1) using the irr package version 0.84.1 [
17]. Calculated ICC values <0.5 indicate poor reliability, 0.5–0.75 indicate good reliability, and values >0.9 indicate excellent reliability, as per Koo and Li [
18].
4. Discussion
The SWV of the short and long heads of the biceps brachii muscle was measured in both arms with the elbow at full extension and flexed at 30° and 60°, with the aim of determining the difference in stiffness between the muscles and the effect of elbow angles.
The difference in stiffness between the short and long head of the biceps brachii is due to their different attachment sites and functions. The SHB consistently displayed velocities lower than the LHB at all three elbow angles. Anatomically, the arm positioned directly by the participants side resulted in the stiffness of the LHB to be greater than the SHB. This is an important distinction to make as previous research has not reached a consensus on the stiffness of the bicep muscles of stroke survivors [
3]. Such previous research approaches, however, have not addressed the separate muscle bellies nor assessed the biceps without distinction, and it can be theorised that this is a leading reason for the discrepancies. Future comparisons of clinical assessments, such as the Modified Ashworth or Tardieu Scale, to the SWV measurements should distinguish which muscle belly has been selected for measurement by elastography.
In considering biomechanics, extending the elbow increases the length of the biceps brachii; however, one or both proximal origins might require shoulder extension in combination with elbow extension to reach maximum length. A recent paper by Chodock et al. [
19] found that the stiffness of the biceps increases with humeral abduction. There is potential that altering the shoulder position may lead to less of a difference in stiffness between the two muscle bellies, though this requires specific investigation. The selected supine position with arms adjacent to the body is comfortable, relatively reproducible, and has good clinical feasibility. In particular, this position can be easily created in a hospital setting, where participants may be restricted to a bed, especially in the initial time period after a stroke.
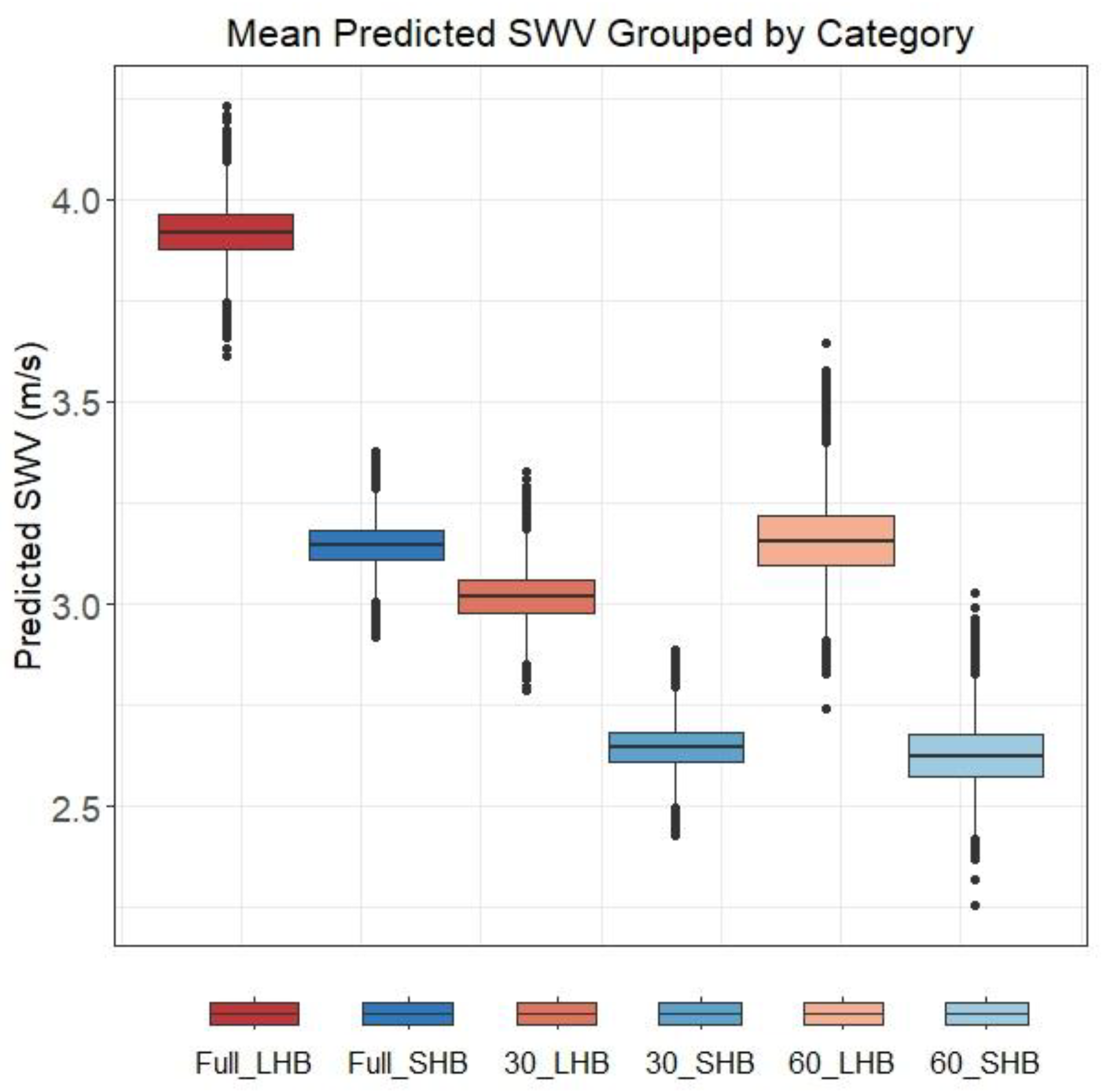
Consistent with previous research, the stiffness of the biceps muscle, both short and long heads, was greatest at full extension of the elbow joint. The estimated mean SWV decreased with flexion to 30°; however, this trend was not consistently seen at the 60° elbow angle. The SWV of both the SHB and LHB at 60° elbow flexion demonstrated the largest standard deviations despite being lower in velocity. Concerning the analysis, the stiffness continued to decrease with increasing elbow flexion in 18 (47%) participants, as was hypothesized; however, in the remaining participants, the stiffness of the bicep muscle at 60° flexion was higher than the 30° SWV measurement. On further analysis, this finding was not specific to either gender, as seen in
Figure 4.
We theorise that the muscle of the arm could have been activated inadvertently, increasing the stiffness. When the participant is in a supine position and the elbow is flexed to 60°, the forearm and wrist could have felt less stable, requiring minor activation of the biceps brachii during the evaluation with the SWE. Future investigations should assess the bicep muscle with the elbow at 60° flexion while seated or in a reclined position or using electromyography to confirm the passive state of the muscle. Alternatively, a more stable position might be achieved by utilising a brace for the distal arm and hand.
Despite the unexpected trend for the 60° flexion and increased variability, the difference in the ICCs appears to be more dependent on the muscle belly. The ICC values for the SHB at all three elbow angles were between 0.64 and 0.67, which Koo and Li [
18] categorise as good, while the LHB muscle/elbow angle combinations all returned excellent reliability (0.9–0.92). This indicates that while the returned velocity may have continued to decrease or increase with increasing elbow flexion, the measurement reliability in the LHB was consistently better than the SHB. These findings suggest that investigations aiming to determine changes in muscle stiffness are likely to detect the change earlier in the LHB compared to the SHB, assuming that the two muscle bellies are equally affected by the change in stiffness.
The other variables returned no significant effect on the SWV in this study; however, some authors have argued that these may need to be taken into consideration. The gender of the participant had no effect on muscle stiffness in this study, which appears to be a prevalent finding in other studies surrounding the SWE of healthy muscles [
5,
19,
20,
21] and stroke survivors [
22]. In contrast, Eby et al. [
23] noted the SWV in the biceps brachii of females to be higher. There was no effect of right verses left, nor weight, which is consistent with the investigations by Phan et al. [
21] and Alfuraih et al. [
20], though it was noted that a decreased BMI correlated with an increased SWV in the biceps brachii in the study by Chodock et al. [
19].
The participant position within this project was selected based on comfort and reproducibility within a clinical setting. The research design required the participants to be supine and positioned at three elbow angles; however, there are potential future research directions that involve varying this position. Initial investigations could include increasing the elbow angle, adjusting the abduction of the humerus, altering the pronation and supination of the hand, and changing the incline from supine to erect. Investigations into the differences in muscle stiffness with these variations would provide further information about the biomechanics of the muscles as well as determining the most reliable measurement positions.
Combining the findings from the research presented here on healthy participants and knowledge from previous research using SWE to assess the muscles of stroke survivors, we recommended that the morphology of the muscle be taken into consideration. While previous research has shown correlations between the SWV and the clinical assessments for post-stroke muscle stiffness, none have considered the two origins of the biceps and the effect this might have on the corresponding muscle belly stiffness. Therefore, there would be a definite need to measure both muscle bellies to specifically determine the difference and whether one muscle belly is affected more predominantly or earlier than the other. Protocols for future scans of stroke survivors will be based off the findings from this work and build on to create a new diagnostic tool for quantifying post-stroke muscle stiffness.










{kind=link}
{kind=link}
{kind=link}
{kind=link}