Investigation of Effective Modification Treatments for Titanium Membranes

Abstract
:1. Introduction
2. Methods
2.1. Sample Preparation
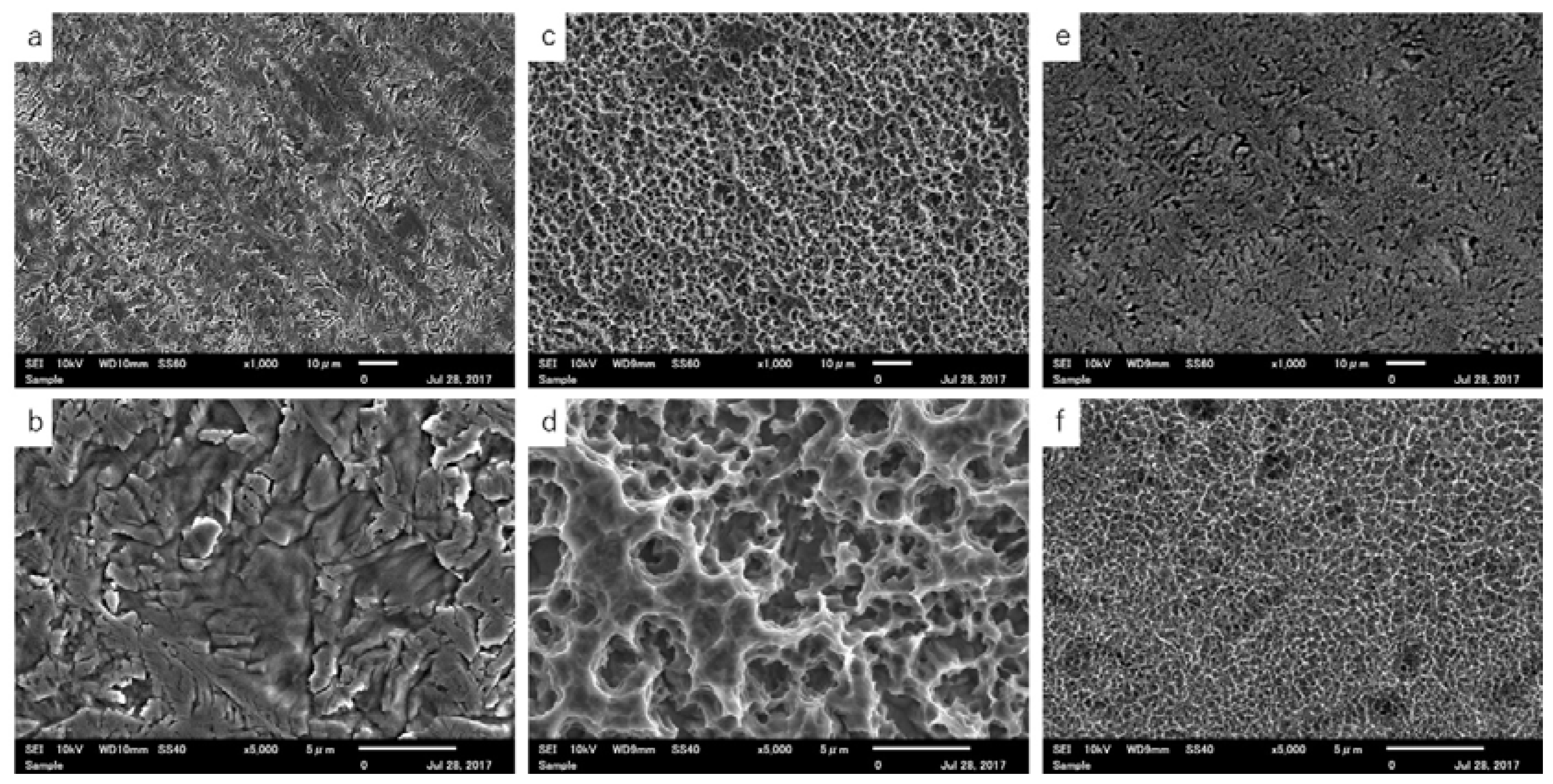
2.2. Scanning Electron Microscopy (SEM)
2.3. Thickness
2.4. Tensile Strength
2.5. Evaluation of Wettability
2.6. Statistical Analyses
3. Results
3.1. SEM Observations
3.2. Thickness
3.3. Tensile Strength
3.4. Evaluation of Wettability
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Johansson, B.; Bäck, T.; Hirsch, J.M. Cutting torque measurements in conjunction with implant placement in grafted and nongrafted maxillas as an objective evaluation of bone density: A possible method for identifying early implant failures? Clin. Implant Dent. Relat. Res. 2004, 6, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, C.H.F.; Karring, T. Guided bone regeneration at oral implant sites. Periodontology 1998, 17, 151–175. [Google Scholar] [CrossRef]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implants 2009, 24, 237–259. [Google Scholar] [PubMed]
- Becker, W.; Becker, B.; Mellonig, J. A prospective multicenter study evaluating periodontal regeneration for class II furcation invasions and infrabony defects after treatment with a bioabsorbable barrier membrane: 1-Year results. J. Periodontol. 1996, 67, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Naef, R.; Scharer, P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration. Int. J. Oral Maxillofac. Implants 1997, 12, 844–852. [Google Scholar] [PubMed]
- Zablotsky, M.; Meffert, R.; Caudill, R. Histological and clinical compar-isons of guided tissue regeneration on dehisced hydroxylapatite-coated and titanium endosseous implant surfaces. A pilot study. Int. J. Oral Maxillofac. Implants 1991, 6, 294. [Google Scholar] [PubMed]
- Wang, R.R.; Fenton, A. Titanium for prosthodontic applications: A review of the literature. Quintessence Int. 1996, 27, 401–408. [Google Scholar] [PubMed]
- Degidi, M.; Scarano, A.; Piattelli, A. Regeneration of the alveolar crest using titanium micromesh with autologous bone and a resorbable membrane. J. Oral Implantol. 2003, 29, 86. [Google Scholar] [CrossRef]
- Cole, B.J.; Bostrom, M.P.; Pritchard, T.L.; Sumner, D.R.; Tomin, E.; Lane, J.M.; Weiland, A.J. Use of bone morphogenetic protein 2 on ectopic porous coated implants in the rat. Clin. Orthop. Relat. Res. 1997, 345, 219–228. [Google Scholar] [CrossRef]
- Ferretti, C.; Ripamonti, U. Human segmental mandibular defects treated with naturally derived bone morphogenetic proteins. J. Craniofac. Surg. 2002, 13, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Le Guéhennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Jemat, A.; Ghazali, M.J.; Razali, M.; Otsuka, Y. Surface Modifications and Their Effects on Titanium Dental Implants. BioMed Res. Int. 2015, 2015, 791725. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.M.; Miyaji, F.; Kokubo, T.; Nakamura, T. Preparation of bioactive Ti and its alloys via simple chemical surface treatment. J. Biomed. Mater. Res. 1996, 32, 409–417. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Kato, H.; Fujita, H.; Kim, H.M.; Miyaji, F.; Kokubo, T.; Nakamura, T. Enhancement of bone-bonding strengths of titanium alloy implants by alkali and heat treatments. J. Biomed. Mater. Res. 1999, 48, 689–696. [Google Scholar] [CrossRef]
- Fujibayashi, S.; Nakamura, T.; Nishiguchi, S.; Tamura, J.; Uchida, M.; Kim, H.M.; Kokubo, T. Bioactive titanium: Effect of sodium removal on the bone-bonding ability of bioactive titanium prepared by alkali and heat treatment. J. Biomed. Mater. Res. 2001, 56, 562–570. [Google Scholar] [CrossRef]
- Takemoto, M.; Fujibayashi, S.; Neo, M.; Suzuki, J.; Matsushita, T.; Kokubo, T.; Nakamura, T. Osteoinductive porous titanium implants: Effect of sodium removal by dilute HCl treatment. Biomaterials 2006, 27, 2682–2691. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, T.; Miyaji, F.; Kim, H.M. Spontaneous formation of bone like apatite layer on chemically treated titanium metals. J. Am. Ceram. Soc. 1996, 79, 1127–1129. [Google Scholar] [CrossRef]
- Kim, H.M.; Miyaji, F.; Kokubo, T.; Nakamura, T. Effect of heat treatment on apatite-forming ability of Ti metal induced by alkali treatment. J. Mater. Sci. Mater. Med. 1997, 8, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Ban, S.; Iwaya, Y.; Kono, H.; Sato, H. Surface modification of titanium by etching in concentrated sulfuric acid. Dent. Mater. 2006, 22, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Kono, H.; Miyamoto, M.; Ban, S. Bioactive Apatite coating on titanium using an alternate soaking process. Dent. Mater. J. 2007, 26, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Takemoto, M.; Fujibayashi, S.; Akiyama, H.; Tanaka, M.; Yamaguchi, S.; Pattanayak, D.K.; Doi, K.; Matsushita, T.; Nakamura, T.; et al. Osteoinduction on acid and heat treated porous Ti metal samples in canine muscle. PLoS ONE 2014, 9, e88366. [Google Scholar] [CrossRef] [PubMed]
- Iwaya, Y.; Machigashira, M.; Kanbara, K.; Miyamoto, M.; Noguchi, K.; Izumi, Y.; Ban, S. Surface properties and biocompatibility of acid-etched titanium. Dent. Mater. J. 2008, 27, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Rakhmatia, Y.D.; Ayukawa, Y.; Jinno, Y.; Furuhashi, A.; Koyano, K. Micro-computed tomography analysis of early stage bone healing using micro-porous titanium mesh for guided bone regeneration: Preliminary experiment in a canine model. Odontology 2017. [Google Scholar] [CrossRef] [PubMed]
- Vovk, V.; Vovk, Y. Results of the guided bone regeneration in patients with jaw defects and atrophies by means of Mondeal® occlusive titanium membranes. J. Oral Maxillofac. Surg. 2005, 34, 74. [Google Scholar] [CrossRef]
- Juodzbalys, G.; Sapragoniene, M.; Wennerberg, A. New acid etched titanium dental implant surface. Stomatologija 2003, 5, 101–105. [Google Scholar]
- Van Gestel, T.; Vandecasteele, C.; Buekenhoudt, A.; Dotremont, C.; Luyten, J.; Van der Bruggen, B.; Maes, G. Corrosion properties of alumina and titania NF membranes. J. Membr. Sci. 2003, 214, 21–29. [Google Scholar] [CrossRef]
- Camargo, W.A.; Takemoto, S.; Hoekstra, J.W.; Leeuwenburgh, S.C.G.; Jansen, J.A.; van den Beucken, J.J.J.P.; Alghamdi, H.S. Effect of surface alkali-based treatment of titanium implants on ability to promote in vitro mineralization and in vivo bone formation. Acta Biomater. 2017, 57, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Dalby, M.J.; McCloy, D.; Robertson, M.; Wilkinson, C.D.; Oreffo, R.O. Osteoprogenitor response to defined topographies with nanoscale depths. Biomaterials 2006, 27, 1306–1315. [Google Scholar] [CrossRef] [PubMed]
- Tugulu, S.; Löwe, K.; Scharnweber, D.; Schlottig, F. Preparation of superhydrophilic microrough titanium implant surfaces by alkali treatment. J. Mater. Sci. Mater. Med. 2010, 21, 2751–2763. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surface Treatment | Thickness (μm) (SD) |
|---|---|
| control (non-treated) | 20.0 ± 0.75 |
| acid | 15.1 ± 0.64 * |
| alkali | 19.7 ± 0.46 |
| Surface Treatment | Maximum Tensile Strength (N) (SD) |
|---|---|
| control (non-treated) | 309.5 ± 29.3 |
| acid | 158.4 ± 20.2 * |
| alkali | 295.0 ± 48.3 |
| Surface Treatment | Contact Angle (°) (SD) |
|---|---|
| control (non-treated) | 71.1 ± 1.63 * |
| acid | 103.1 ± 3.81 |
| alkali | not determined |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobatake, R.; Doi, K.; Oki, Y.; Umehara, H.; Kawano, H.; Kubo, T.; Tsuga, K. Investigation of Effective Modification Treatments for Titanium Membranes. Appl. Sci. 2017, 7, 1022. https://doi.org/10.3390/app7101022
Kobatake R, Doi K, Oki Y, Umehara H, Kawano H, Kubo T, Tsuga K. Investigation of Effective Modification Treatments for Titanium Membranes. Applied Sciences. 2017; 7(10):1022. https://doi.org/10.3390/app7101022
Chicago/Turabian StyleKobatake, Reiko, Kazuya Doi, Yoshifumi Oki, Hanako Umehara, Hiromichi Kawano, Takayasu Kubo, and Kazuhiro Tsuga. 2017. "Investigation of Effective Modification Treatments for Titanium Membranes" Applied Sciences 7, no. 10: 1022. https://doi.org/10.3390/app7101022
APA StyleKobatake, R., Doi, K., Oki, Y., Umehara, H., Kawano, H., Kubo, T., & Tsuga, K. (2017). Investigation of Effective Modification Treatments for Titanium Membranes. Applied Sciences, 7(10), 1022. https://doi.org/10.3390/app7101022