Devices and Protocols for Upper Limb Robot-Assisted Rehabilitation of Children with Neuromotor Disorders


Abstract
:1. Introduction
2. Materials and Methods
3. Results
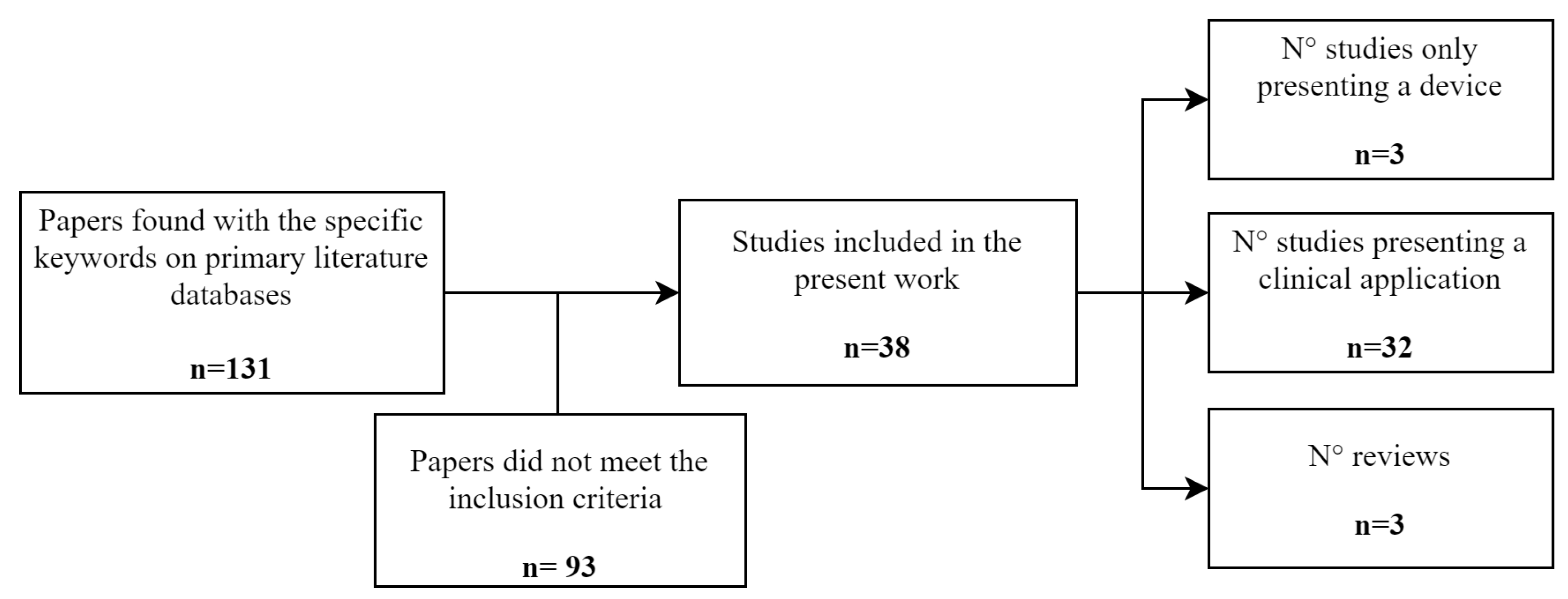
3.1. Literature Search
- Fasoli et al. [41] based their work on a detailed review of the application of one specific robot (InMotion2, later explained) for children with hemiplegia due to CP;
- Chen et al. [42] examined the effectiveness of several upper limb robots applied only to children with CP;
- the third review [43] is focused on clinical protocols performed on children with different neurological diseases but with the use of two specific robots (InMotion2 and NJIT-RAVR).
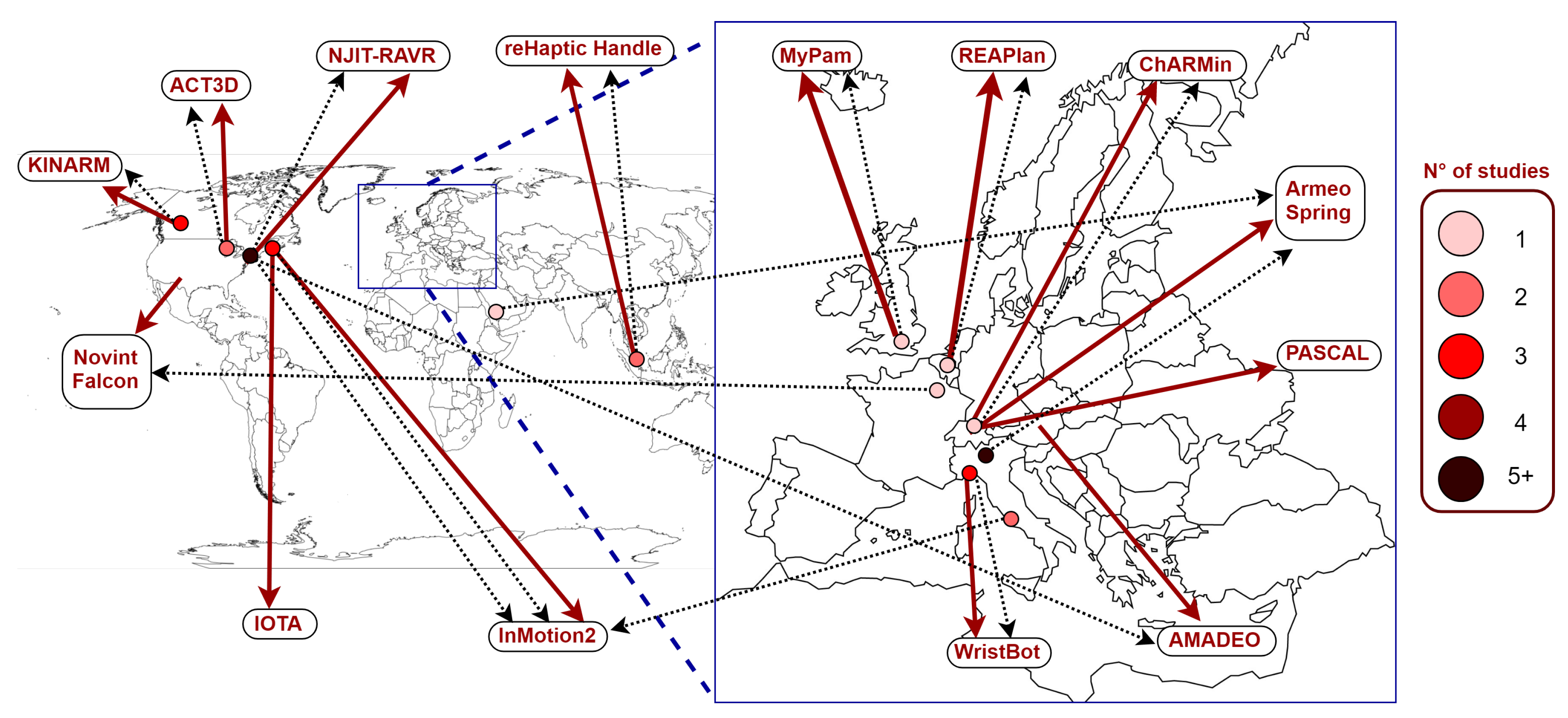
3.2. Robotic Devices
- KINARM [46] is a bimanual robot, which allows movements in the horizontal plane (2 D) targeting the human shoulder and/or elbow joints; it can be used in an exoskeleton or end-effector configuration;
- Armeo Spring [44] is an exoskeleton with 5 DoFs with a rehabilitation target of the entire human arm; it is actuated by passive springs with the role of supporting the weight of the arm, allowing natural movements in the 3D space with a wide range of motion;
- ACT3D [47] is an end-effector robot that allows movements in 3D space properly designed to treat shoulder and elbow; it consists of a modified 3D HapticMaster (admittance controlled robot for shoulder and elbow) [58] with an instrumented end-effector and the patient’s arm is connected to the robot through a lightweight forearm-hand orthosis;
- WristBot [54] is a 3 DoFs end-effector robot specifically designed to treat wrist and forearm; it provides haptic feedback and compensates for its weight and inertia;
- Novint Falcon [56] is a 3 DoFs end-effector robot for shoulder and elbow; it was initially created as a computer input device, but later used also in the rehabilitation field;
- AMADEO [53] is an end-effector robot conceived for the rehabilitation of the hand with 1 DoF for each finger;
- IOTA [55] is a 2 DoFs exoskeleton that rehabilitates the carpometacarpal (CMC) and metacarpophalangeal (MCP) joints (thumb) needed to perform some of the activities of daily living such as opposition grasp;
- PASCAL [52] is an end-effector robot for shoulder and elbow treatment with 5 DoFs: 3 DoFs to allow movements in the 3D space (shoulder, elbow) and 2 DoFs to ensure only exchange of interaction forces; in some applications there is the possibility to combine this robot with the Lokomat [59] to allow simultaneous rehabilitation of both upper and lower limbs [60];
- reHaptic Handle [49] is an end-effector robot with 2 DoFs to train pinching, forearm pronation/supination and wrist flexion/extension movements;
- REAPlan [15] is a planar end-effector device with 2 DoFs and intended for the rehabilitation of shoulder and elbow;
- MyPam [50] is a bimanual end-effector robot for shoulder and elbow allowing movements in the horizontal plane; it has been designed to perform rehabilitation in a school environment and it can be used also in unimanual mode.
3.3. Safety and Usability of Robotic Devices
3.4. Robotic Protocols for Upper Limb Assessment
3.5. Robotic Protocols for Upper Limb Rehabilitation
3.6. Motor Learning in Robot-Assisted Therapy
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Cook, A.; Encarnação, P.; Adams, K. Robots: Assistive technologies for play, learning and cognitive development. Technol. Disabil. 2010, 22, 127–145. [Google Scholar] [CrossRef]
- Odding, E.; Roebroeck, M.E.; Stam, H.J. The epidemiology of cerebral palsy: Incidence, impairments and risk factors. Disabil. Rehabil. 2006, 28, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Eunson, P. Aetiology and epidemiology of cerebral palsy. Paediatr. Child Health 2012, 22, 361–366. [Google Scholar] [CrossRef]
- Morris, C. Definition and classification of cerebral palsy: A historical perspective. Dev. Med. Child Neurol. 2007, 49, 3–7. [Google Scholar] [CrossRef]
- Raju, T.N.; Nelson, K.B.; Ferriero, D.; Lynch, J.K. Ischemic perinatal stroke: Summary of a workshop sponsored by the National Institute of Child Health and Human Development and the National Institute of Neurological Disorders and Stroke. Pediatrics 2007, 120, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Mallick, A.A.; O’Callaghan, F.J. The epidemiology of childhood stroke. Eur. J. Paediatr. Neurol. 2010, 14, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Eeg-Olofsson, O.; Ringheim, Y. Stroke in children. Clinical characteristics and prognosis. Acta Paediatr. 1983, 72, 391–395. [Google Scholar] [CrossRef]
- Morrissey, K.; Fairbrother, H. Severe Traumatic Brain Injury In Children: An Evidence-Based Review of Emergency Department Management. Pediatr. Emerg. Med. Pract. 2016, 13, 1–28. [Google Scholar] [PubMed]
- Thurman, D.J. The Epidemiology of Traumatic Brain Injury in Children and Youths: A Review of Research Since 1990. J. Child Neurol. 2016, 31, 20–27. [Google Scholar] [CrossRef]
- Jones, M.W.; Morgan, E.; Shelton, J.E.; Thorogood, C. Cerebral palsy: Introduction and diagnosis (part I). J. Pediatr. Health Care 2007, 21, 146–152. [Google Scholar] [CrossRef]
- Steenbergen, B.; Veringa, A.; de Haan, A.; Hulstijn, W. Manual dexterity and keyboard use in spastic hemiparesis: A comparison between the impaired hand and the ‘good’ hand on a number of performance measures. Clin. Rehabil. 1998, 12, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Heim, A.; van Hedel, H.J. Robot-assisted and computer-enhanced therapies for children with cerebral palsy: Current state and clinical implementation. In Seminars in Pediatric Neurology; Elsevier: Amsterdam, The Netherlands, 2013; Volume 20, pp. 139–145. [Google Scholar]
- Fasoli, S.E.; Fragala-Pinkham, M.; Hughes, R.; Hogan, N.; Krebs, H.I.; Stein, J. Upper limb robotic therapy for children with hemiplegia. Am. J. Phys. Med. Rehabil. 2008, 87, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Gilliaux, M.; Renders, A.; Dispa, D.; Holvoet, D.; Sapin, J.; Dehez, B.; Detrembleur, C.; Lejeune, T.M.; Stoquart, G. Upper limb robot-assisted therapy in cerebral palsy: A single-blind randomized controlled trial. Neurorehabilit. Neural Repair 2015, 29, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Rose, F.; Johnson, D.; Attree, E. Rehabilitation of the head-injured child: Basic research and new technology. Pediatr. Rehabil. 1997, 1, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Damiano, D.L. Activity, activity, activity: Rethinking our physical therapy approach to cerebral palsy. Phys. Ther. 2006, 86, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Emken, J.L.; Benitez, R.; Sideris, A.; Bobrow, J.E.; Reinkensmeyer, D.J. Motor adaptation as a greedy optimization of error and effort. J. Neurophysiol. 2007, 97, 3997–4006. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.S.; Veeravagu, A.; Grant, G. Neuroplasticity after traumatic brain injury. In Translational Research in Traumatic Brain Injury; Laskowitz, D., Grant, G., Eds.; CRC Press/Taylor and Francis Group: Boca Raton, FL, USA, 2016. [Google Scholar]
- Vahdat, S.; Darainy, M.; Thiel, A.; Ostry, D.J. A Single Session of Robot-Controlled Proprioceptive Training Modulates Functional Connectivity of Sensory Motor Networks and Improves Reaching Accuracy in Chronic Stroke. Neurorehabilit. Neural Repair 2019, 33, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Ladenheim, B.; Altenburger, P.; Cardinal, R.; Monterroso, L.; Dierks, T.; Mast, J.; Krebs, H.I. The effect of random or sequential presentation of targets during robot-assisted therapy on children. NeuroRehabilitation 2013, 33, 25–31. [Google Scholar]
- Reid, L.B.; Rose, S.E.; Boyd, R.N. Rehabilitation and neuroplasticity in children with unilateral cerebral palsy. Nat. Rev. Neurol. 2015, 11, 390. [Google Scholar] [CrossRef]
- Reid, L.B.; Pagnozzi, A.M.; Fiori, S.; Boyd, R.N.; Dowson, N.; Rose, S.E. Measuring neuroplasticity associated with cerebral palsy rehabilitation: An MRI based power analysis. Int. J. Dev. Neurosci. 2017, 58, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs, H.I.; Fasoli, S.E.; Dipietro, L.; Fragala-Pinkham, M.; Hughes, R.; Stein, J.; Hogan, N. Motor learning characterizes habilitation of children with hemiplegic cerebral palsy. Neurorehabilit. Neural Repair 2012, 26, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Ríos-Rincón, A.M.; Adams, K.; Magill-Evans, J.; Cook, A. Playfulness in children with limited motor abilities when using a robot. Phys. Occup. Ther. Pediatr. 2016, 36, 232–246. [Google Scholar] [CrossRef] [PubMed]
- Frascarelli, F.; Masia, L.; Di, G.R.; Cappa, P.; Petrarca, M.; Castelli, E.; Krebs, H. The impact of robotic rehabilitation in children with acquired or congenital movement disorders. Eur. J. Phys. Rehabil. Med. 2009, 45, 135–141. [Google Scholar] [PubMed]
- Ouellette, M.M.; LeBrasseur, N.K.; Bean, J.F.; Phillips, E.; Stein, J.; Frontera, W.R.; Fielding, R.A. High-intensity resistance training improves muscle strength, self-reported function, and disability in long-term stroke survivors. Stroke 2004, 35, 1404–1409. [Google Scholar] [CrossRef] [PubMed]
- Elsaeh, M.; Pudlo, P.; Djemai, M.; Bouri, M.; Thevenon, A.; Heymann, I. The effects of haptic-virtual reality game therapy on brain-motor coordination for children with hemiplegia: A pilot study. In Proceedings of the IEEE 2017 International Conference on Virtual Rehabilitation (ICVR), Montreal, QC, Canada, 19–22 June 2017; pp. 1–6. [Google Scholar]
- Marchal-Crespo, L.; Reinkensmeyer, D.J. Review of control strategies for robotic movement training after neurologic injury. J. Neuroeng. Rehabil. 2009, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Bayon, C.; Raya, R.; Lara, S.; Ramírez, O.; Serrano, J.; Rocon, E. Robotic therapies for children with cerebral palsy: A systematic review. Transl. Biomed. 2016, 7, 44. [Google Scholar] [CrossRef]
- Berdina, O.N.; Bairova, T.A.; Rychkova, L.V.; Sheptunov, S.A. The pediatric robotic-assisted rehabilitation complex for children and adolescents with cerebral palsy: Background and product design. In Proceedings of the IEEE 2017 International Conference on “Quality Management, Transport and Information Security, Information Technologies” (IT&QM&IS), St. Petersburg, Russia, 24–30 September 2017; pp. 360–363. [Google Scholar]
- Gilliaux, M.; Dierckx, F.; Berghe, L.V.; Lejeune, T.M.; Sapin, J.; Dehez, B.; Stoquart, G.; Detrembleur, C. Age effects on upper limb kinematics assessed by the REAplan robot in healthy school-aged children. Ann. Biomed. Eng. 2015, 43, 1123–1131. [Google Scholar] [CrossRef]
- Laut, J.; Porfiri, M.; Raghavan, P. The present and future of robotic technology in rehabilitation. Curr. Phys. Med. Rehabil. Rep. 2016, 4, 312–319. [Google Scholar] [CrossRef]
- DeMatteo, C.; Law, M.; Russell, D.; Pollock, N.; Rosenbaum, P.; Walter, S. The reliability and validity of the Quality of Upper Extremity Skills Test. Phys. Occup. Ther. Pediatr. 1993, 13, 1–18. [Google Scholar] [CrossRef]
- Charalambous, C.P. Interrater reliability of a modified Ashworth scale of muscle spasticity. In Classic Papers in Orthopaedics; Springer: Berlin, Germany, 2014; pp. 415–417. [Google Scholar]
- De Bode, S.; Firestine, A.; Mathern, G.W.; Dobkin, B. Residual motor control and cortical representations of function following hemispherectomy: Effects of etiology. J. Child Neurol. 2005, 20, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.M.; Randall, M.J.; Reddihough, D.S.; Byrt, T.; Oke, L.; Bach, T. Development of a clinical assessment of quality of movement for unilateral upper-limb function. Dev. Med. Child Neurol. 1994, 36, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Rosa-Rizzotto, M.; Visona Dalla Pozza, L.; Corlatti, A.; Luparia, A.; Marchi, A.; Molteni, F.; Fedrizzi, E.; Group, G.S.; et al. A new scale for the assessment of performance and capacity of hand function in children with hemiplegic cerebral palsy: Reliability and validity studies. Eur. J. Phys. Rehabil. Med. 2014, 50, 543–556. [Google Scholar] [PubMed]
- Krumlinde-Sundholm, L.; Holmefur, M.; Kottorp, A.; Eliasson, A.C. The Assisting Hand Assessment: Current evidence of validity, reliability, and responsiveness to change. Dev. Med. Child Neurol. 2007, 49, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Fasoli, S.E.; Fragala-Pinkham, M.; Hughes, R.; Hogan, N.; Stein, J.; Krebs, H.I. Upper limb robot-assisted therapy: A new option for children with hemiplegia. Technol. Disabil. 2010, 22, 193–198. [Google Scholar] [CrossRef]
- Chen, Y.P.; Howard, A.M. Effects of robotic therapy on upper-extremity function in children with cerebral palsy: A systematic review. Dev. Neurorehabilit. 2016, 19, 64–71. [Google Scholar] [CrossRef]
- Fasoli, S.E.; Ladenheim, B.; Mast, J.; Krebs, H.I. New horizons for robot-assisted therapy in pediatrics. Am. J. Phys. Med. Rehabil. 2012, 91, S280–S289. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, R.; Reinkensmeyer, D.; Shah, P.; Liu, J.; Rao, S.; Smith, R.; Cramer, S.; Rahman, T.; Bobrow, J. Monitoring functional arm movement for home-based therapy after stroke. In Proceedings of the IEEE 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; Volume 2, pp. 4787–4790. [Google Scholar]
- Krebs, H.I.; Hogan, N.; Aisen, M.L.; Volpe, B.T. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.H. Apparatus for measuring and perturbing shoulder and elbow joint positions and torques during reaching. J. Neurosci. Methods 1999, 89, 119–127. [Google Scholar] [CrossRef]
- Sukal, T.M.; Ellis, M.D.; Dewald, J.P. Shoulder abduction-induced reductions in reaching work area following hemiparetic stroke: Neuroscientific implications. Exp. Brain Res. 2007, 183, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Adamovich, S.V.; Fluet, G.G.; Merians, A.S.; Mathai, A.; Qiu, Q. Incorporating haptic effects into three-dimensional virtual environments to train the hemiparetic upper extremity. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.L.; Klein, J.; Dual, S.A.; Leong, T.C.; Burdet, E. reachMAN2: A compact rehabilitation robot to train reaching and manipulation. In Proceedings of the 2014 IEEE/RSJ International Conference on Intelligent Robots and Systems, Chicago, IL, USA, 14–18 September 2014; pp. 2107–2113. [Google Scholar]
- Gallagher, J.; Preston, N.; Holt, R.; Mon-Williams, M.; Levesley, M.; Weightman, A. Assessment of upper limb movement with an autonomous robotic device in a school environment for children with Cerebral Palsy. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, Singapore, 11–14 August 2015; pp. 770–774. [Google Scholar]
- Keller, U.; Klamroth, V.; van Hedel, H.J.; Riener, R. ChARMin: A robot for pediatric arm rehabilitation. In Proceedings of the 2013 IEEE International Conference on Robotics and Automation, Karlsruhe, Germany, 6–10 May 2013; pp. 3908–3913. [Google Scholar]
- Keller, U.; Rauter, G.; Riener, R. Assist-as-needed path control for the PASCAL rehabilitation robot. In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; pp. 1–7. [Google Scholar]
- Stein, J.; Bishop, L.; Gillen, G.; Helbok, R. Robot-assisted exercise for hand weakness after stroke: A pilot study. Am. J. Phys. Med. Rehabil. 2011, 90, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Masia, L.; Casadio, M.; Giannoni, P.; Sandini, G.; Morasso, P. Performance adaptive training control strategy for recovering wrist movements in stroke patients: A preliminary, feasibility study. J. Neuroeng. Rehabil. 2009, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Aubin, P.M.; Sallum, H.; Walsh, C.; Stirling, L.; Correia, A. A pediatric robotic thumb exoskeleton for at-home rehabilitation: The Isolated Orthosis for Thumb Actuation (IOTA). In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; pp. 1–6. [Google Scholar]
- Martin, S.; Hillier, N. Characterisation of the Novint Falcon haptic device for application as a robot manipulator. In Proceedings of the Australasian Conference on Robotics and Automation (ACRA), Sydney, Australia, 2–4 December 2009; pp. 291–292. [Google Scholar]
- Hogan, N.; Krebs, H.I.; Charnnarong, J.; Srikrishna, P.; Sharon, A. MIT-MANUS: A workstation for manual therapy and training. I. In Proceedings of the IEEE International Workshop on Robot and Human Communication, Tokyo, Japan, 1992; pp. 161–165. [Google Scholar]
- Van der Linde, R.Q.; Lammertse, P.; Frederiksen, E.; Ruiter, B. The HapticMaster, a new high-performance haptic interface. In Proceedings of the Eurohaptics, Edinburgh, UK, 8–10 July 2002; pp. 1–5. [Google Scholar]
- Riener, R.; Lünenburger, L.; Maier, I.C.; Colombo, G.; Dietz, V. Locomotor training in subjects with sensori-motor deficits: An overview of the robotic gait orthosis lokomat. J. Healthc. Eng. 2010, 1, 197–216. [Google Scholar] [CrossRef]
- Koenig, A.; Keller, U.; Pfluger, K.; Meyer-Heim, A.; Riener, R. PASCAL: Pediatric arm support robot for combined arm and leg training. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1862–1868. [Google Scholar]
- Keller, U.; Riener, R. Design of the pediatric arm rehabilitation robot ChARMin. In Proceedings of the 5th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Sao Paulo, Brazil, 12–15 August 2014; pp. 530–535. [Google Scholar]
- Aggogeri, F.; Mikolajczyk, T.; O’Kane, J. Robotics for rehabilitation of hand movement in stroke survivors. Adv. Mech. Eng. 2019, 11, 1–14. [Google Scholar] [CrossRef]
- Keller, U.; van Hedel, H.J.; Klamroth-Marganska, V.; Riener, R. ChARMin: The first actuated exoskeleton robot for pediatric arm rehabilitation. IEEE/ASME Trans. Mechatron. 2016, 21, 2201–2213. [Google Scholar] [CrossRef]
- Frascarelli, F.; Masia, L.; Di Rosa, G.; Petrarca, M.; Cappa, P.; Castelli, E. Robot-mediated and clinical scales evaluation after upper limb botulinum toxin type a injection in children with hemiplegia. J. Rehabil. Med. 2009, 41, 988–994. [Google Scholar] [CrossRef]
- Bosecker, C.; Dipietro, L.; Volpe, B.; Igo Krebs, H. Kinematic robot-based evaluation scales and clinical counterparts to measure upper limb motor performance in patients with chronic stroke. Neurorehabilit. Neural Repair 2010, 24, 62–69. [Google Scholar] [CrossRef]
- Dukelow, S.P.; Herter, T.M.; Moore, K.D.; Demers, M.J.; Glasgow, J.I.; Bagg, S.D.; Norman, K.E.; Scott, S.H. Quantitative assessment of limb position sense following stroke. Neurorehabilit. Neural Repair 2010, 24, 178–187. [Google Scholar] [CrossRef]
- Qiu, Q.; Ramirez, D.A.; Saleh, S.; Fluet, G.G.; Parikh, H.D.; Kelly, D.; Adamovich, S.V. The New Jersey Institute of Technology Robot-Assisted Virtual Rehabilitation (NJIT-RAVR) system for children with cerebral palsy: A feasibility study. J. Neuroeng. Rehabil. 2009, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Fluet, G.G.; Qiu, Q.; Saleh, S.; Ramirez, D.; Adamovich, S.; Kelly, D.; Parikh, H. Robot-assisted virtual rehabilitation (NJIT-RAVR) system for children with upper extremity hemiplegia. In Proceedings of the 2009 Virtual Rehabilitation International Conference, Haifa, Israel, 29 June–2 July 2009; pp. 189–192. [Google Scholar]
- Fluet, G.G.; Qiu, Q.; Kelly, D.; Parikh, H.D.; Ramirez, D.; Saleh, S.; Adamovich, S.V. Interfacing a haptic robotic system with complex virtual environments to treat impaired upper extremity motor function in children with cerebral palsy. Dev. Neurorehabilit. 2010, 13, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Marini, F.; Squeri, V.; Cappello, L.; Morasso, P.; Riva, A.; Doglio, L.; Masia, L. Adaptive wrist robot training in pediatric rehabilitation. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, Singapore, 11–14 August 2015; pp. 175–180. [Google Scholar]
- Marini, F.; Hughes, C.M.; Squeri, V.; Doglio, L.; Moretti, P.; Morasso, P.; Masia, L. Robotic wrist training after stroke: Adaptive modulation of assistance in pediatric rehabilitation. Robot. Auton. Syst. 2017, 91, 169–178. [Google Scholar] [CrossRef]
- Taylor, J. Proprioception. In Encyclopedia of Neuroscience; Squire, L.R., Ed.; Academic Press: Oxford, UK, 2009; pp. 1143–1149. [Google Scholar]
- Kuczynski, A.M.; Semrau, J.A.; Kirton, A.; Dukelow, S.P. Kinesthetic deficits after perinatal stroke: Robotic measurement in hemiparetic children. J. Neuroeng. Rehabil. 2017, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Kuczynski, A.M.; Kirton, A.; Semrau, J.A.; Dukelow, S.P. Bilateral reaching deficits after unilateral perinatal ischemic stroke: A population-based case-control study. J. Neuroeng. Rehabil. 2018, 15, 77. [Google Scholar] [CrossRef] [PubMed]
- Krebs, H.I.; Palazzolo, J.J.; Dipietro, L.; Ferraro, M.; Krol, J.; Rannekleiv, K.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Performance-based progressive robot-assisted therapy. Auton. Robot. 2003, 15, 7–20. [Google Scholar] [CrossRef]
- Masia, L.; Frascarelli, F.; Morasso, P.; Di Rosa, G.; Petrarca, M.; Castelli, E.; Cappa, P. Abnormal adaptation in children affected by cerebral palsy to robot generated dynamic environment. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 3410–3413. [Google Scholar]
- Masia, L.; Frascarelli, F.; Morasso, P.; Di Rosa, G.; Petrarca, M.; Castelli, E.; Cappa, P. Reduced short term adaptation to robot generated dynamic environment in children affected by Cerebral Palsy. J. Neuroeng. Rehabil. 2011, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- Fasoli, S.E.; Fragala-Pinkham, M.; Hughes, R.; Krebs, H.I.; Hogan, N.; Stein, J. Robotic therapy and botulinum toxin type A: A novel intervention approach for cerebral palsy. Am. J. Phys. Med. Rehabil. 2008, 87, 1022–1026. [Google Scholar] [CrossRef]
- Turner, D.L.; Winterbotham, W.; Kmetova, M. Using assistive robotic technology in motor neurorehabilitation after childhood stroke. J. Neurol. Res. 2012, 2, 65–68. [Google Scholar] [CrossRef]
- Aharonson, V.; Krebs, H.I. Prediction of response to robot-aided motor neuro-rehabilitation of children with cerebral palsy. Biomed. Signal Process. Control 2012, 7, 180–184. [Google Scholar] [CrossRef]
- Cimolin, V.; Vagnini, A.; Germiniasi, C.; Galli, M.; Pacifici, I.; Negri, L.; Beretta, E.; Piccinini, L. The Armeo spring as training tool to improve upper limb functionality in hemiplegic cerebral palsy: A pilot study. In Proceedings of the 2016 IEEE 2nd International Forum on Research and Technologies for Society and Industry Leveraging a better tomorrow (RTSI), Bologna, Italy, 7–9 September 2016; pp. 1–4. [Google Scholar]
- Biffi, E.; Maghini, C.; Cairo, B.; Beretta, E.; Peri, E.; Altomonte, D.; Mazzoli, D.; Giacobbi, M.; Prati, P.; Merlo, A.; et al. Movement Velocity and Fluidity Improve after Armeo® Spring Rehabilitation in Children Affected by Acquired and Congenital Brain Diseases: An Observational Study. BioMed Res. Int. 2018, 2018, 1537170. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Germiniasi, C.; Galli, M.; Condoluci, C.; Beretta, E.; Piccinini, L. Robot-Assisted Upper Limb Training for Hemiplegic Children with Cerebral Palsy. J. Dev. Phys. Disabil. 2019, 31, 89–101. [Google Scholar] [CrossRef]
- Turconi, A.C.; Biffi, E.; Maghini, C.; Peri, E.; Servodio, F.I.; Gagliardi, C. Can new technologies improve upper limb performance in grown-up diplegic children? Eur. J. Phys. Rehabil. Med. 2016, 52, 672–681. [Google Scholar] [PubMed]
- El-Shamy, S.M. Efficacy of Armeo® robotic therapy versus conventional therapy on upper limb function in children with hemiplegic cerebral palsy. Am. J. Phys. Med. Rehabil. 2018, 97, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Beretta, E.; Cesareo, A.; Biffi, E.; Schafer, C.; Galbiati, S.; Strazzer, S. Rehabilitation of Upper Limb in Children with Acquired Brain Injury: A Preliminary Comparative Study. J. Healthc. Eng. 2018, 3, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Peri, E.; Biffi, E.; Maghini, C.; Iammarrone, F.S.; Gagliardi, C.; Germiniasi, C.; Pedrocchi, A.; Turconi, A.C.; Reni, G. Quantitative evaluation of performance during robot-assisted treatment. Methods Inf. Med. 2016, 55, 84–88. [Google Scholar] [PubMed]
- Sukal, T.M.; Krosschell, K.J.; Dewald, J.P. Use of the ACT3D system to evaluate synergies in children with spastic hemiparetic cerebral palsy: A pilot study. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 964–967. [Google Scholar]
- Sukal, T.M.; Ellis, M.D.; Dewald, J.P. Dynamic characterization of upper limb discoordination following hemiparetic stroke. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 519–521. [Google Scholar]
- Marini, F.; Cappello, L.; Squeri, V.; Morasso, P.; Moretti, P.; Riva, A.; Doglio, L.; Masia, L. Online modulation of assistance in robot aided wrist rehabilitation a pilot study on a subject affected by dystonia. In Proceedings of the 2014 IEEE Haptics Symposium (HAPTICS), Houston, TX, USA, 23–26 February 2014; pp. 153–158. [Google Scholar]
- Jakob, I.; Kollreider, A.; Germanotta, M.; Benetti, F.; Cruciani, A.; Padua, L.; Aprile, I. Robotic and sensor technology for upper limb rehabilitation. PM&R 2018, 10, S189–S197. [Google Scholar]
- Bishop, L.; Gordon, A.M.; Kim, H. Hand Robotic Therapy in Children with Hemiparesis: A Pilot Study. Am. J. Phys. Med. Rehabil. 2017, 96, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.Z.; Ong, H.T.; Tan, J.X.; Lin, J.; Burdet, E.; Ge, S.; Teo, C.L. Pediatric rehabilitation with the reachMAN’s modular handle. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milano, Italy, 25–29 August 2015; pp. 3933–3936. [Google Scholar]
- Keller, J.W.; Van Hedel, H.J. Weight-supported training of the upper extremity in children with cerebral palsy: A motor learning study. J. Neuroeng. Rehabil. 2017, 14, 87. [Google Scholar] [CrossRef]
- Mehrholz, J.; Hädrich, A.; Platz, T.; Kugler, J.; Pohl, M. Electromechanical and robot-assisted arm training for improving generic activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2012, 6, CD006876. [Google Scholar] [CrossRef]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2017, 5, CD006185. [Google Scholar] [CrossRef] [PubMed]
- Prechtl, H.F. General movement assessment as a method of developmental neurology: New paradigms and their consequences The 1999 Ronnie MacKeith Lecture. Dev. Med. Child Neurol. 2001, 43, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Adde, L.; Helbostad, J.L.; Jensenius, A.R.; Taraldsen, G.; Grunewaldt, K.H.; Støen, R. Early prediction of cerebral palsy by computer-based video analysis of general movements: A feasibility study. Dev. Med. Child Neurol. 2010, 52, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.; Orton, J.; Anderson, P.; Boyd, R.; Doyle, L.W. Early developmental intervention programmes post-hospital discharge to prevent motor and cognitive impairments in preterm infants. Cochrane Database Syst. Rev. 2012, 12, CD005495. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Robot | DOFs | Rehab Joint | Type | Output Measurements | Modality | Feedback | Market Available |
|---|---|---|---|---|---|---|---|
| KINARM (1999) [46] | 2 + 2 | Shoulder elbow | End-effector | Kinesthesia, position sense, kinematics | Active; passive | Visual | ✓ |
| InMotion2 (2003) [45] | 2 | Shoulder elbow | End-effector | Kinematics | Active; passive; assistive; weight support | Visual haptic auditory | ✓ |
| Armeo Spring (2004) [44] | 5 | Shoulder elbow forearm wrist fingers | Exoskeleton | Kinematics | Active; weight support | Visual auditory | ✓ |
| ACT3D (2007) [47] | 3 | Shoulder elbow | End-effector | Kinematics, Forces | Active; passive; weight support | Visual haptic auditory | |
| NJIT-RAVR (2009) [48] | 6 | Shoulder elbow forearm | End-effector | Kinematics, RoM | Active; assistive; resistive; weight support | Visual haptic auditory | |
| WristBot (2009) [54] | 3 | Forearm wrist | End-effector | Kinematics, wrist RoM | Active; passive; assistive; weight support | Visual hapitc auditory | |
| Novint Falcon (2009) [56] | 3 | Shoulder elbow forearm | End-effector | Kinematics | Active; assistive | Visual auditory haptic | ✓ |
| AMADEO (2011) [53] | 5 | Fingers | End-effector | Magnitude and directionality of the forces | Active; passive; assistive | Visual haptic | ✓ |
| IOTA (2013) [55] | 2 | Thumb | Exoskeleton | Wrist RoM, angular rotation of the thumb | Active; passive; assistive | Visual haptic | |
| PASCAL (2013) [52] | 3 + 2 | Shoulder elbow | End-effector | End-effector kinematics | Active; passive; assistive; weight support | Visual haptic | |
| CHARMin (2013) [51] | 6 | Shoulder forearm wrist | Exoskeleton | Arm kinematics | Active; passive; assistive; weight support | Visual haptic auditory | |
| ReHaptic Handle (2014) [49] | 2 | Forearm wrist | End-effector | Grip forces, kinematics, wrist RoM | Active; passive assistive; resistive weight support | Visual haptic | |
| REAPlan (2015) [15] | 2 | Shoulder elbow | End-effector | End-effector kinematics | Active, passive, assistive | Visual haptic auditory | ✓ |
| MyPam (2015) [50] | 2 | Shoulder elbow | End-effector | Kinematics | Active; assistive | Visual haptic |
| Robot, Study | nP, Mean Age (±SD) | Diagnosis, Mean Age at Injury (±SD) | nCG, Mean Age (±SD) | Duration [Weeks] | n Sessions for Day | Intensity [min/ses] | Clinical Assessment | Robotic Assessment | Results |
|---|---|---|---|---|---|---|---|---|---|
| InMotion2 [14] | 12, 9.2 (2.1) | CP ABI | No | 8 2 days/week | 1 | 60 | QUEST MAS FMA | Kinematics | - Strong improvement of QUEST and FMA - Moderate effect in MAS |
| InMotion2 [26] | 12, 11.7 (3.1) | CP Stroke ABI, 2.9 (2.7) | No | 6 3 days/week | 1 | 60 | MAS FMA MAAULF | Kinematics Smoothness | - Higher smoothness - Better shoulder-elbow connection |
| InMotion2 [24] | 12, [5,12] a | CP ABI | No | 8 2 days/week | 1 | 60 | QUEST MAS FMA | Kinematics | - Higher smoothness - Improvement of kinematics |
| InMotion2 [21] | 31, 8.2 (0.0) | CP ABI, 6 | No | 8 2 days/week | 1 | 60 | MAS FMA | \ | - Significant improvement of FMA in both the random and sequential groups - No differences between groups |
| InMotion2 [79] | 1, 17.0 (0.0) | ABI, 17.0 (0.0) | No | 36 2 days/week | 1 | 60 | FMA | \ | - FMA score is greatest over the first 3 months - the increase of FMA is slower in the child patient than in an adult stroke patient |
| Armeo Spring [84] | 10, 10.9 (2.3) | CP ABI | No | 4 2 days/week | 1 | 45 | QUEST MAS MAUULF | RoM | - Significant improvement of MAUULF - QUEST remained the same - No improvement for hand and fingers dexterity |
| Armeo Spring [81] | 8, [6,14] a | CP | 10 healthy [7,14] a | 4 5 days/week | 2 | 45 | QUEST MAUULF | \ | - Improvement of clinical scales - Improvement of kinematic evaluation |
| Armeo Spring [85] | 15, 6.9 (0.8) | CP | 15 CP, 6.8 (0.8) | 12 3 days/week | 1 | 45 | QUEST MAS | \ | - Significant improvement of MAS and QUEST in the group of robotic rehabilitation |
| Armeo Spring [86] | 18, 12.3 (5.1) | Stroke ABI, 10.9 (4.9) | No | 4 5 days/week | 1 | 45 | QUEST MAAULF | \ | - Improvement of MAUULF - Improvement of the shoulder abd/add and reduction of the shoulder flex/ext |
| Armeo Spring [82] | 43, 11.1 (5.8) | CP ABI, 10.0 (8.9) | No | 4 5 days/week | 1 | 45 | QUEST MAUULF | Kinematics Smoothness | - Improvement of MAUULF and QUEST for both CP and ABI children - Improvement of the kinematic values - More improvements in ABI than in CP |
| Armeo Spring [83] | 21, [7,14] a | CP | 15 healthy [7,14] a | 4 5 days/week | 2 | 45 | QUEST MAUULF | \ | - Improvement of MAAULF and QUEST - Improvement of the kinematics - No improvement for upper limb RoMs |
| Armeo Spring [94] | 11, 12.8 (3.3) | CP | No | 1 3 days/week | 1 | 70 | BBT MAAULF | Kinematics | - Improvement of the BBT - Evidence of retention - No improvements of kinematics and MAAULF |
| NJIT-RAVR [68] | 4, 10.5 (3.3) | CP | 4 CP 8.5 (3.1) | 3 3 days/week | 1 | 60 | MAAULF | Kinematics Smoothness | - Both groups improved kinematics and MAUULF - Feasibility of combining robotic therapy with that conventional without adverse effects |
| NJIT-RAVR [67] | 2, 8.5 (1.5) | CP | No | 3 3 days/week | 1 | 60 | MAAULF | Kinematics RoM Forces | - Improvements of motor performance and kinematics |
| NJIT-RAVR [69] | 9, 9.4 (3.5) | CP | No | 3 3 days/week | 1 | 60 | MAAULF | Kinematics RoM | - Better active supination RoM - Greater arm elevation |
| WristBot [90] | 1, 14.0 (0.0) | ABI | No | 1 3 days/week | 1 | 60 | \ | Kinematics Smoothenss RoM | - Improvement of smoothness - Better accuracy and better control of the affected limb |
| WristBot [70] | 2, 8.0 (1.0) | ABI 5.0 (1.0) | No | 6 2 days/week | 1 | 30 | QUEST MAS BBT | Kinematics Smoothenss RoM | - Improvement of rad\uln RoM - Better accuracy - Significant reduction in the amount of assistive force |
| WristBot [71] | 1, 14.0 (0.0) | Stroke 13.0 (0.0) | No | 12 2 days/week | 1 | 60 | MAAULF MAS AHA | Kinematics Smoothenss RoM | - Higher smoothness - Significant reduction in robot intervention - Improvement of both distal and proximal segments of upper limbs |
| Novint Falcon [28] | 2, 8.5 (1.5) | CP | No | 1 3 days/week | 1 | 120 | \ | Kinematics | - Improvement of kinematics - No pain during the training |
| Amadeo [92] | 12, 9.0 (3.6) | ABI | No | 6 3 days/week | 1 | 60 | QUEST FMA AHA | Grip forces Kinematics | - Improvements of clinical scales - Improvement focused on the distal part of upper limbs |
| ReHaptic Handle [93] | 1, 8.0 (0.0) | CP | No | 2 3 days/week | 1 | 60 | \ | Kinematics Smoothness | - Improvement of kinematics and smoothness |
| REAPlan [15] | 8, 10.8 (4.6) | CP | 8 CP 11.0 (3.5) | 8 5 days/week | 1 | 45 | QUEST MAS BBT | Kinematics Forces Spasticity | - Kinematics and manual dexterity improved more in the group undergoing robotic therapy |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falzarano, V.; Marini, F.; Morasso, P.; Zenzeri, J. Devices and Protocols for Upper Limb Robot-Assisted Rehabilitation of Children with Neuromotor Disorders. Appl. Sci. 2019, 9, 2689. https://doi.org/10.3390/app9132689
Falzarano V, Marini F, Morasso P, Zenzeri J. Devices and Protocols for Upper Limb Robot-Assisted Rehabilitation of Children with Neuromotor Disorders. Applied Sciences. 2019; 9(13):2689. https://doi.org/10.3390/app9132689
Chicago/Turabian StyleFalzarano, Valeria, Francesca Marini, Pietro Morasso, and Jacopo Zenzeri. 2019. "Devices and Protocols for Upper Limb Robot-Assisted Rehabilitation of Children with Neuromotor Disorders" Applied Sciences 9, no. 13: 2689. https://doi.org/10.3390/app9132689
APA StyleFalzarano, V., Marini, F., Morasso, P., & Zenzeri, J. (2019). Devices and Protocols for Upper Limb Robot-Assisted Rehabilitation of Children with Neuromotor Disorders. Applied Sciences, 9(13), 2689. https://doi.org/10.3390/app9132689