The Development of Magnesium-Based Resorbable and Iron-Based Biocorrodible Metal Scaffold Technology and Biomedical Applications in Coronary Artery Disease Patients

 ,
,
Abstract
:1. Introduction
2. Transient Scaffolding of the Vessel Wall
3. Magnesium-Based Devices
3.1. Biological Effects of Magnesium
3.2. Magnesium Alloy Biocompatibility and Resorption
3.3. First Experience of a Magnesium Alloy Device
3.4. Lekton Magic Coronary Stent
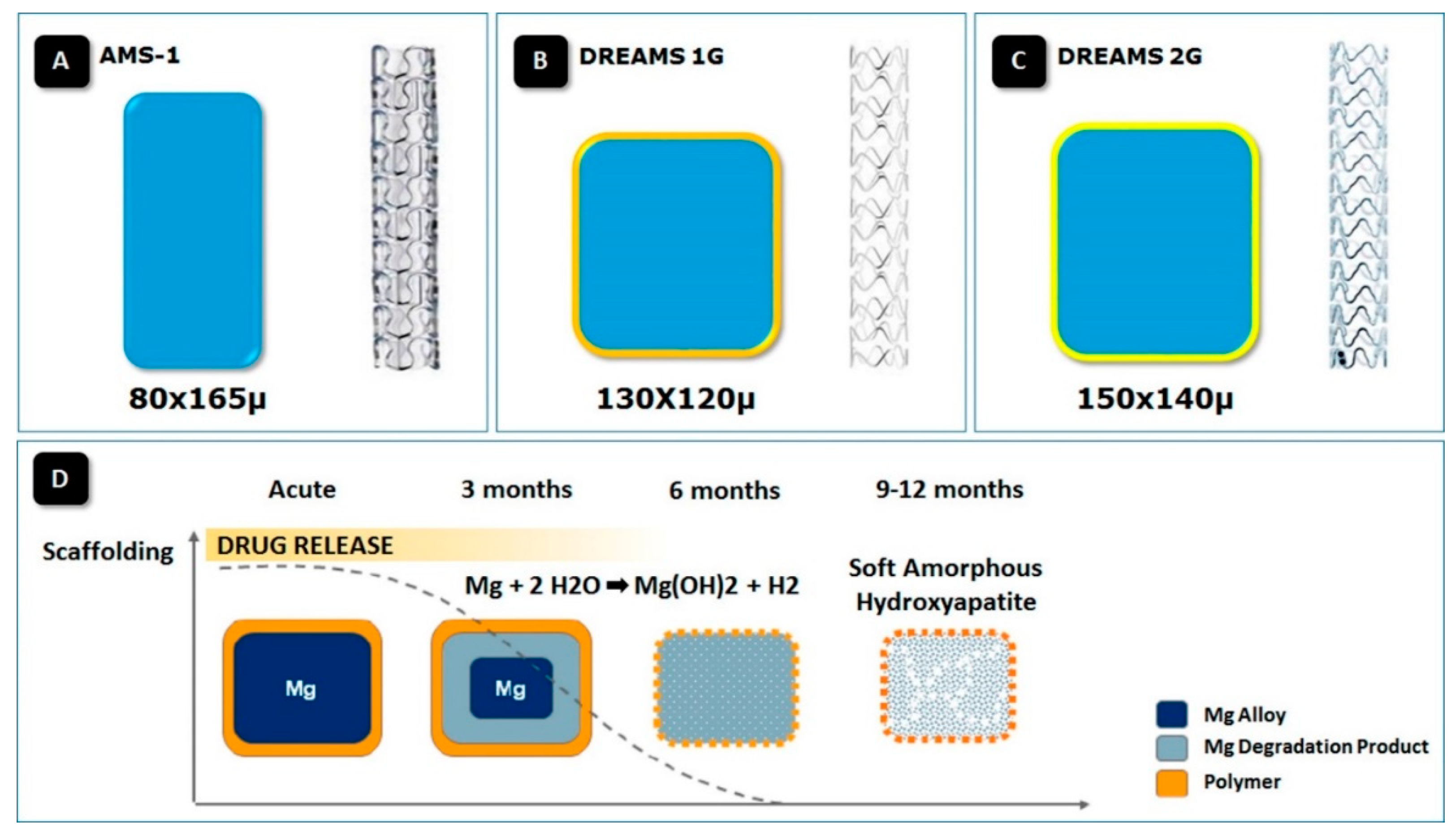
3.5. Absorbable Metal Stent First Generation (AMS-1)
3.6. DRug-Eluting Absorbable Metal Scaffold (DREAMS)
3.7. Sirolimus DRug-Eluting Absorbable Metal Scaffold (DREAMS 2nd Generation—2G)
3.8. Next Generation of Sirolimus-Eluting Resorbable Metal Scaffold (DREAMS 3rd Generation)
4. Iron-Based Devices
4.1. Iron Alloy Platform Degradation
4.2. Biocorrodible Pure Iron Devices
4.3. Sirolimus-Eluting Iron Bioresorbable Coronary Scaffold (IBS)
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mauri, L.; Hsieh, W.; Massaro, J.M.; Ho, K.K.L.; D’Agostino, R.; Cutlip, D.E. Stent thrombosis in randomized clinical trials of drug-eluting stents. N. Engl. J. Med. 2007, 356, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Byrne, R.A.; Joner, M.; Kastrati, A. Stent thrombosis and restenosis: What have we learned and where are we going? The Andreas Grüntzig Lecture ESC 2014. Eur. Heart J. 2015, 36, 3320–3331. [Google Scholar] [CrossRef] [PubMed]
- Witzenbichler, B.; Maehara, A.; Weisz, G.; Neumann, F.-J.; Rinaldi, M.J.; Metzger, D.C.; Henry, T.D.; Cox, D.A.; Duffy, P.L.; Brodie, B.R.; et al. Relationship between intravascular ultrasound guidance and clinical outcomes after drug-eluting stents: The assessment of dual antiplatelet therapy with drug-eluting stents (ADAPT-DES) study. Circulation 2014, 129, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Prati, F.; Kodama, T.; Romagnoli, E.; Gatto, L.; Di Vito, L.; Ramazzotti, V.; Chisari, A.; Marco, V.; Cremonesi, A.; Parodi, G.; et al. Suboptimal stent deployment is associated with subacute stent thrombosis: Optical coherence tomography insights from a multicenter matched study. From the CLI Foundation investigators: The CLITHRO study. Am. Heart J. 2015, 169, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Galper, B.Z.; Cohen, D.J.; Yeh, R.W.; Mauri, L. Balancing the risks of bleeding and stent thrombosis: A decision analytic model to compare durations of dual antiplatelet therapy after drug-eluting stents. Am. Heart J. 2015, 169, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Charpentier, E.; Barna, A.; Guillevin, L.; Juliard, J.M. Fully bioresorbable drug-eluting coronary scaffolds: A review. Arch. Cardiovasc. Dis. 2015, 108, 385–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishio, S.; Kosuga, K.; Igaki, K.; Okada, M.; Kyo, E.; Tsuji, T.; Takeuchi, E.; Inuzuka, Y.; Takeda, S.; Hata, T.; et al. Long-term (>10 years) clinical outcomes of first-in-human biodegradable poly-l-lactic acid coronary stents: Igaki-Tamai stents. Circulation 2012, 125, 2343–2353. [Google Scholar] [CrossRef] [PubMed]
- Heublein, B.; Rohde, R.; Kaese, V.; Niemeyer, N.; Hartung, W.; Haverich, A. Biocorrosion of magnesium alloys: A new principle in cardiovascular implant technology? Heart 2003, 89, 651–656. [Google Scholar] [CrossRef]
- Di Mario, C.; Griffiths, H.; Goktekin, O.; Peeters, N.; Verbist, J.; Bosiers, M.; Deloose, K.; Heublein, B.; Rohde, R.; Kasese, V.; et al. Drug eluting bioabsorbable magnesium stent. J. Interv. Cardiol. 2004, 17, 391–395. [Google Scholar] [CrossRef]
- Haude, M.; Erbel, R.; Erne, P.; Verheye, S.; Degen, H.; Böse, D.; Vermeersch, P.; Wijnbergen, I.; Weissman, N.; Prati, F.; et al. Safety and performance of the drug-eluting absorbable metal scaffold (DREAMS) in patients with de-novo coronary lesions: 12 months results of the prospective, multicentre, first-in-man BIOSOLVE-I trial. Lancet 2013, 381, 836–844. [Google Scholar] [CrossRef]
- Serruys, P.W.; Garcia-Garcia, H.M.; Onuma, Y. From metallic cages to transient bioresorbable scaffolds: Change in paradigm of coronary revascularization in the upcoming decade? Eur. Heart J. 2012, 33, 16b–25b. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.J.; Iqbal, J.; Nakatani, S.; Bourantas, C.V.; Campos, C.M.; Ishibashi, Y.; Cho, Y.K.; Veldhof, S.; Wang, J.; Onuma, Y.; et al. ABSORB Cohort B Study Investigators. Scaffold and edge vascular response following implantation of everolimus-eluting bioresorbable vascular scaffold: A 3-year serial optical coherence tomography study. JACC Cardiovasc. Interv. 2014, 7, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, H.M.; Haude, M.; Kuku, K.; Hideo-Kajita, A.; Ince, H.; Abizaid, A.; Tölg, R.; Lemos, P.A.; von Birgelen, C.; Christiansen, E.H.; et al. In vivo serial invasive imaging of the second-generation drug-eluting absorbable metal scaffold (Magmaris-DREAMS 2G) in de novo coronary lesions: Insights from the BIOSOLVE-II First-In-Man Trial. Int. J. Cardiol. 2018, 255, 22–28. [Google Scholar] [CrossRef] [PubMed]
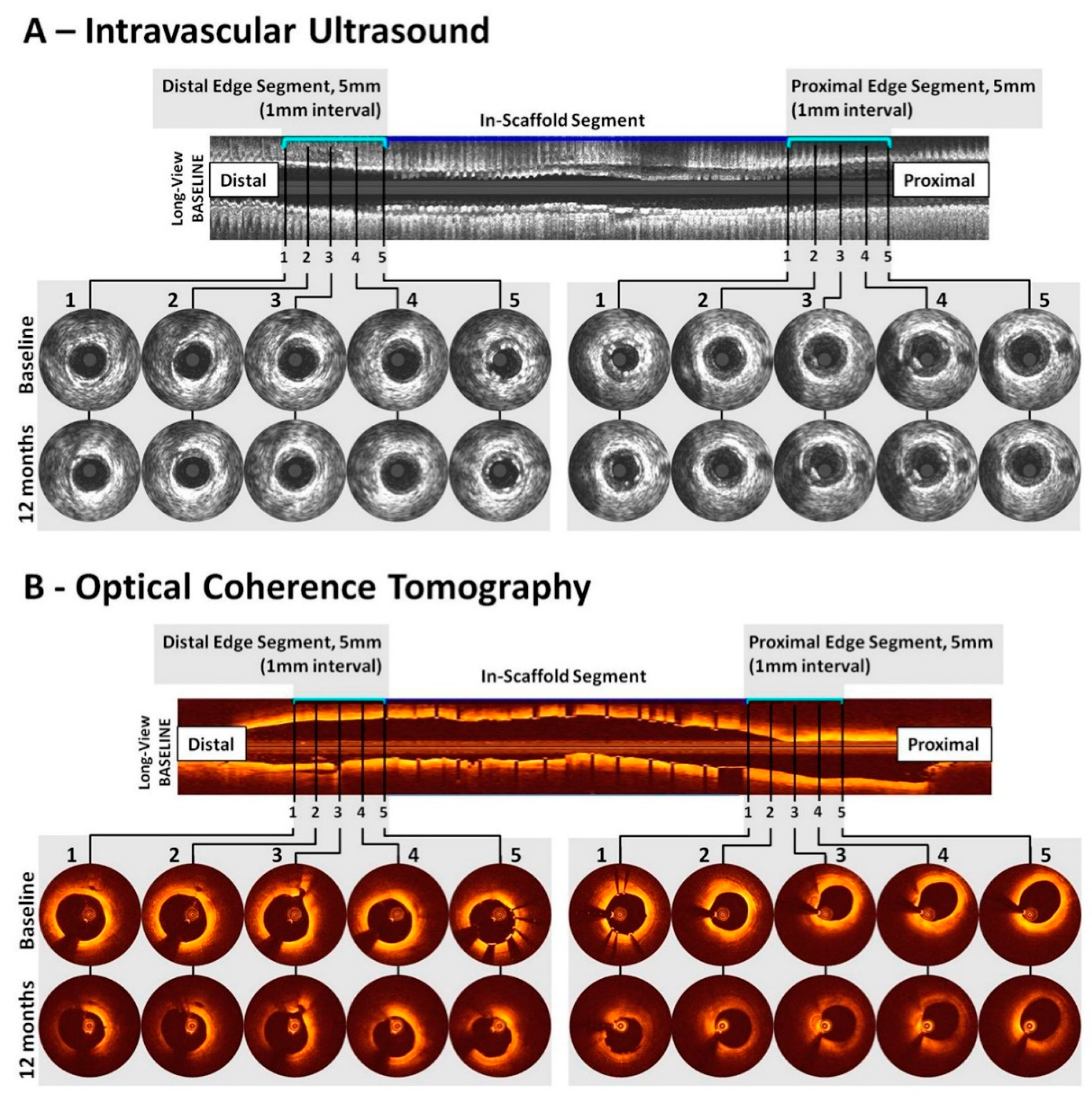
- Hideo-Kajita, A.; Garcia-Garcia, H.M.; Haude, M.; Joner, M.; Koolen, J.; Ince, H.; Abizaid, A.; Toelg, R.; Lemos, P.A.; von Birgelen, C.; et al. First Report of Edge Vascular Response at 12 Months of Magmaris, A Second-Generation Drug-Eluting Resorbable Magnesium Scaffold, Assessed by Grayscale Intravascular Ultrasound, Virtual Histology, and Optical Coherence Tomography. A Biosolve-II Trial Sub-Study. Cardiovasc. Revasc. Med. 2019, 20, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Jahnen-Dechent, W.; Ketteler, M. Magnesium basics. Clin. Kidney J. 2012, 5 (Suppl. 1), i3–i14. [Google Scholar] [CrossRef] [Green Version]
- Romani, A.M.P. Cellular Magnesium Homeostasis. Arch. Biochem. Biophys. 2011, 512, 1–23. [Google Scholar] [CrossRef]
- Vormann, J. Magnesium: Nutrition and metabolism. Mol. Aspects Med. 2003, 24, 27–37. [Google Scholar] [CrossRef]
- Vormann, J. Magnesium: Nutrition and Homoeostasis. AIMS Public Health 2016, 3, 329–340. [Google Scholar] [CrossRef]
- Severino, P.; Netti, L.; Mariani, M.V.; Maraone, A.; D’Amato, A.; Scarpati, R.; Infusino, F.; Pucci, M.; Lavalle, C.; Maestrini, V.; et al. Prevention of Cardiovascular Disease: Screening for Magnesium Deficiency. Cardiol. Res. Pract. 2019, 2019, 4874921. [Google Scholar] [CrossRef]
- Sawyer, P.N.; Srinivasan, S. The role of electrochemical surface properties in thrombosis at vascular interfaces: Cumulative experience of studies in animals and man. Bull. N. Y. Acad. Med. 1972, 48, 235–256. [Google Scholar]
- Joner, M.; Ruppelt, P.; Zumstein, P.; Lapointe-Corriveau, C.; Leclerc, G.; Bulin, A.; Castellanos, M.I.; Wittchow, E.; Haude, M.; Waksman, R. Precinical evaluation of degradation kinetics and elemental mapping of first- and second-generation bioresorbable magnesium scaffolds. EuroIntervention 2018, 14, e1040–e1048. [Google Scholar] [CrossRef]
- Rukshin, V.; Shah, P.K.; Cerck, B.; Finkelstein, A.; Tsang, V.; Kaul, S. Comparative antithrombotic effects of magnesium sulfate and the platelet glycoprotein IIb/IIIa inhibitors tirofiban and eptifibatide in a canine model of stent thrombosis. Circulation 2002, 105, 1970–1975. [Google Scholar] [CrossRef]
- Rukshin, V.; Azarbal, B.; Shah, P.K.; Tsang, V.T.; Shechter, M.; Finkelstein, A.; Cercek, B.; Kaul, S. Intravenous magnesium in experimental stent thrombosis in swine. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1544–1549. [Google Scholar] [CrossRef]
- Waksman, R.; Lipinski, M.J.; Acampado, E.; Cheng, Q.; Adams, L.; Torii, S.; Gai, J.; Torguson, R.; Hellinga, D.M.; Westman, P.C.; et al. Comparison of Acute Thrombogenicity for Metallic and Polymeric Bioabsorbable Scaffolds: Magmaris Versus Absorb in a Porcine Arteriovenous Shunt Model. Circ. Cardiovasc. Interv. 2017, 10, e004762. [Google Scholar] [CrossRef]
- Lipinski, M.J.; Acampado, E.; Cheng, Q.; Adams, L.; Torii, S.; Gai, J.; Torguson, R.; Hellinga, D.G.; Joner, M.; Harder, C.; et al. Comparison of Acute Thrombogenicity for Magnesium versus Stainless Steel Stents in a Porcine Arteriovenous Shunt Model. EuroIntervention 2018, 14, 1420–1427. [Google Scholar] [CrossRef]
- Kemp, P.A.; Gardiner, S.M.; March, J.E.; Rubin, P.C.; Bennett, T. Assessment of the effects of endothelin-1 and magnesium sulphate on regional blood flows in conscious rats, by the coloured microsphere reference technique. Br. J. Pharmacol. 1999, 126, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Berthon, N.; Laurant, P.; Fellmann, D.; Berthelot, A. Effect of magnesium on mRNA expression and production of endothelin-1 in DOCA-salt hypertensive rats. J. Cardiovasc. Pharmacol. 2003, 42, 24–31. [Google Scholar] [CrossRef]
- Basoli, A.; Cametti, C.; Satriani, F.G.; Mariani, P.; Severino, P. Hemocompatibility of stent materials: Alterations in electrical parameters of erythrocyte membranes. Vasc. Health Risk Manag. 2012, 8, 197–204. [Google Scholar] [CrossRef]
- Song, G.L. Control of biodegradation of biocompatible magnesium alloy. Corros. Sci. 2007, 49, 1696–1701. [Google Scholar] [CrossRef]
- Sillekens, W.H.; Bormann, D. Advances in Wrought Magnesium Alloys; Woodhead Publishing Series: Metals and Surface Engineering; Elsevier: Sawston, UK, 2012; pp. 427–454. [Google Scholar]
- Chawla, S.L.; Gupta, R.K. Materials Selection for Corrosion Control; ASM International: Materials Park, OH, USA, 1993. [Google Scholar]
- Waksman, R.; Pakala, R.; Kuchulakanti, P.K.; Baffour, R.; Hellinga, D.; Seabron, R.; Tio, F.O.; Wittchow, E.; Hartwig, S.; Harder, C.; et al. Safety and efficacy of bioabsorbable magnesium alloy stents in porcine coronary arteries. Catheter. Cardiovasc. Interv. 2006, 68, 607–617; discussion 618–619. [Google Scholar] [CrossRef]
- Böse, D.; Eggebrecht, H.; Haude, M.; Schmermund, A.; Erbel, R. First absorbable metal stent implantation in human coronary arteries. Am. Heart Hosp. J. 2006, 4, 128–130. [Google Scholar] [CrossRef]
- Ozaki, Y.; Garcia-Garcia, H.M.; Hideo-Kajita, A.; Kuku, K.O.; Haude, M.; Ince, H.; Abizaid, A.; Tölg, R.; Lemos, P.A.; von Birgelen, C.; et al. Impact of procedural characteristics on coronary vessel wall healing following implantation of second-generation drug-eluting absorbable metal scaffold in patients with de novo coronary artery lesions: An optical coherence tomography analysis. Eur. Heart J. Cardiovasc. Imaging 2018, 20, 916–924. [Google Scholar] [CrossRef]
- Campos, C.M.; Muramatsu, T.; Iqbal, J.; Zhang, Y.J.; Onuma, Y.; Garcia-Garcia, H.M.; Haude, M.; Lemos, P.A.; Warnack, B.; Serruys, P.W. Bioresorbable drug-eluting magnesium-alloy scaffold for treatment of coronary artery disease. Int. J. Mol. Sci. 2013, 14, 24492–24500. [Google Scholar] [CrossRef]
- Erbel, R.; Di Mario, C.; Bartunek, J.; Bonnier, J.; de Bruyne, B.; Eberli, F.R.; Erne, P.; Haude, M.; Heublein, B.; Horrigan, M.; et al. Temporary scaffolding of coronary arteries with bioabsorbable magnesium stents: A prospective, non-randomised multicentre trial. Lancet 2007, 369, 1869–1875. [Google Scholar] [CrossRef]
- Wittchow, E.; Adden, N.; Riedmüller, J.; Savard, C.; Waksman, R.; Braune, M. Bioresorbable drug-eluting magnesium-alloy scaffold: Design and feasibility in a porcine coronary model. EuroIntervention 2013, 8, 1441–1450. [Google Scholar] [CrossRef]
- Haude, M.; Ince, H.; Abizaid, A.; Toelg, R.; Lemos, P.A.; von Birgelen, C.; Christiansen, E.H.; Wijns, W.; Neumann, F.J.; Kaiser, C.; et al. Safety and performance of the second-generation drug-eluting absorbable metal scaffold in patients with de-novo coronary artery lesions (BIOSOLVE-II): 6 month results of a prospective, multicentre, non-randomised, first-in-man trial. Lancet 2016, 387, 31–39. [Google Scholar] [CrossRef]
- Haude, M.; Ince, H.; Abizaid, A.; Toelg, R.; Lemos, P.A.; von Birgelen, C.; Christiansen, E.H.; Wijns, W.; Neumann, F.J.; Kaiser, C.; et al. Sustained safety and performance of the second-generation drug-eluting absorbable metal scaffold in patients with de novo coronary lesions: 12-month clinical results and angiographic findings of the BIOSOLVE-II first-in-man trial. Eur. Heart J. 2016, 37, 2701–2709. [Google Scholar] [CrossRef]
- Haude, M.; Ince, H.; Kische, S.; Abizaid, A.; Tölg, R.; Alves Lemos, P.; Van Mieghem, N.M.; Verheye, S.; von Birgelen, C.; Christiansen, E.H.; et al. Sustained safety and clinical performance of a drug-eluting absorbable metal scaffold up to 24 months: Pooled outcomes of BIOSOLVE-II and BIOSOLVE-III. EuroIntervention 2017, 13, 432–439. [Google Scholar] [CrossRef]
- Hideo-Kajita, A.; Garcia, H.G.; Azizi, V.; Ince, H.; Kische, S.; Abizaid, A.; Töelg, R.; Lemos, P.; Van Mieghem, N.; Verheye, S.; et al. Comparison of Clinical Outcomes Between Magmaris (DREAMS 2G) and Orsiro Drug-Eluting Stents: Pooled Patient Level Analysis from BIOSOLVE II-III and BIOFLOW II trials. J. Am. Coll. Cardiol. 2018, 71, A1109. [Google Scholar] [CrossRef]
- Hideo-Kajita, A.; Garcia-Garcia, H.; Azizi, V.; Ince, H.; Kische, S.; Abizaid, A.; Töelg, R.; Lemos, P.A.; Van Mieghem, N.M.; Verheye, S.; et al. CRT-600.07 Comparison of Clinical Outcomes Between Magmaris (dreams 2g) and Orsiro Drug Eluting Stents: Pooled Patient Level Analysis from Biosolve II-III and Bioflow II Trials. JACC Cardiovasc. Interv. 2018, 11, S43. [Google Scholar] [CrossRef]
- Haude, M. Future developments: Next gen Magmaris. In Proceedings of the EuroPCR, Paris, France, 21 May 2019. [Google Scholar]
- Peuster, M. A novel approach to temporary stenting: Degradable cardiovascular stents produced from corrodible metal—Results 6–18 months after implantation into New Zealand white rabbits. Heart 2001, 86, 563–569. [Google Scholar] [CrossRef]
- Zheng, J.-F.; Qiu, H.; Tian, Y.; Hu, X.-Y.; Luo, T.; Wu, C.; Tian, Y.; Tang, Y.; Song, L.F.; Li, L.; et al. Preclinical Evaluation of a Novel Sirolimus-Eluting Iron Bioresorbable Coronary Scaffold in Porcine Coronary Artery at 6 Months. JACC Cardiovasc. Interv. 2019, 12, 245–255. [Google Scholar] [CrossRef]
- Lin, W.-J.; Zhang, D.-Y.; Zhang, G.; Sun, H.-T.; Qi, H.-P.; Chen, L.-P.; Liu, Z.; Gao, R.; Zheng, W. Design and characterization of a novel biocorrodible iron-based drug-eluting coronary scaffold. Mater. Des. 2016, 91, 72–79. [Google Scholar] [CrossRef]
- Waksman, R.; Pakala, R.; Baffour, R.; Seabron, R.; Hellinga, D.; Tio, F.O. Short-Term Effects of Biocorrodible Iron Stents in Porcine Coronary Arteries. J. Interv. Cardiol. 2008, 21, 15–20. [Google Scholar] [CrossRef]
- Lin, W.; Qin, L.; Qi, H.; Zhang, D.; Zhang, G.; Gao, R.; Qiu, H.; Xia, Y.; Cao, P.; Wang, X.; et al. Long-term in vivo corrosion behavior, biocompatibility and bioresorption mechanism of a bioresorbable nitrided iron scaffold. Acta Biomater. 2017, 54, 454–468. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Device | Mg Alloy | Scaffolding Time | Resorption Time, Months | Coating (Thickness) | Eluting-Drug (Drug Density) | Radiopaque Marker | Platform | Struts, µm | Device Sizes, mm | Elastic Recoil, % | Collapse Pressure, Atm | Crossing Profile, mm | Longitudinal Shortening, % | Ref. | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Crowns | Links | Thickness | Width | Diameter | Length | ||||||||||||
| Heublein et al. prototype | AE21 | NA | NA | No | No | No | NA | NA | 150–200 * | NA | 2.0 | 10 | NA | NA | NA | NA | [8] |
| Lekton Magic Coronary Stent | WE43 | NA | <2 | No | No | No | 4 | 4 | 165 | 80 | NA | NA | 5% | 0.8 | 1.2 | NA | [9] |
| AMS-1 | WE43 | NA | ~1 | No | No | No | 4 | 4 | 165 | 80 | 3.0 3.5 | 10 15 | 6 to 7% | 0.8 | 1.4 | <5% | [33,37] |
| AMS-3.0 (DREAMS) | WE43 | NA | ~3 | PLGA (1–3 μm) | Paclitaxel (0.07 μg/mm2) | No | 6 | 3 | 120 | 130 | 3.25 3.5 | 16 | 9% | 1.5 | 1.2 | NA | [10,37] |
| Magmaris (DREAMS 2G) | WE43 | up to 3 months | ~12 | PLLA (7 μm) | Sirolimus (1.4 μg/mm2) | 2× tantalum | 6 | 2 | 150 | 150 | 3.0 3.5 | 15 20 25 | <8% | 0.8 | 1.75 | NA | [38] |
| DREAMS 3G | WE43 | ≥3 months | ~12 | PLLA (NA) | Sirolimus (1.4 μg/mm2) | Yes (New Concept) | NA | NA | 99 117 147 | 150 | 2.5 3.0 3.5 4.0 | 13 18 22 30 | NA | NA | NA | NA | [43] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hideo-Kajita, A.; Wopperer, S.; Seleme, V.B.; Ribeiro, M.H.; Campos, C.M. The Development of Magnesium-Based Resorbable and Iron-Based Biocorrodible Metal Scaffold Technology and Biomedical Applications in Coronary Artery Disease Patients. Appl. Sci. 2019, 9, 3527. https://doi.org/10.3390/app9173527
Hideo-Kajita A, Wopperer S, Seleme VB, Ribeiro MH, Campos CM. The Development of Magnesium-Based Resorbable and Iron-Based Biocorrodible Metal Scaffold Technology and Biomedical Applications in Coronary Artery Disease Patients. Applied Sciences. 2019; 9(17):3527. https://doi.org/10.3390/app9173527
Chicago/Turabian StyleHideo-Kajita, Alexandre, Samuel Wopperer, Vinícius Bocchino Seleme, Marcelo Harada Ribeiro, and Carlos M. Campos. 2019. "The Development of Magnesium-Based Resorbable and Iron-Based Biocorrodible Metal Scaffold Technology and Biomedical Applications in Coronary Artery Disease Patients" Applied Sciences 9, no. 17: 3527. https://doi.org/10.3390/app9173527
APA StyleHideo-Kajita, A., Wopperer, S., Seleme, V. B., Ribeiro, M. H., & Campos, C. M. (2019). The Development of Magnesium-Based Resorbable and Iron-Based Biocorrodible Metal Scaffold Technology and Biomedical Applications in Coronary Artery Disease Patients. Applied Sciences, 9(17), 3527. https://doi.org/10.3390/app9173527