Feasibility of a 3D Surgical Guide Technique for Impacted Supernumerary Tooth Extraction: A Pilot Study with 3D Printed Simulation Models

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
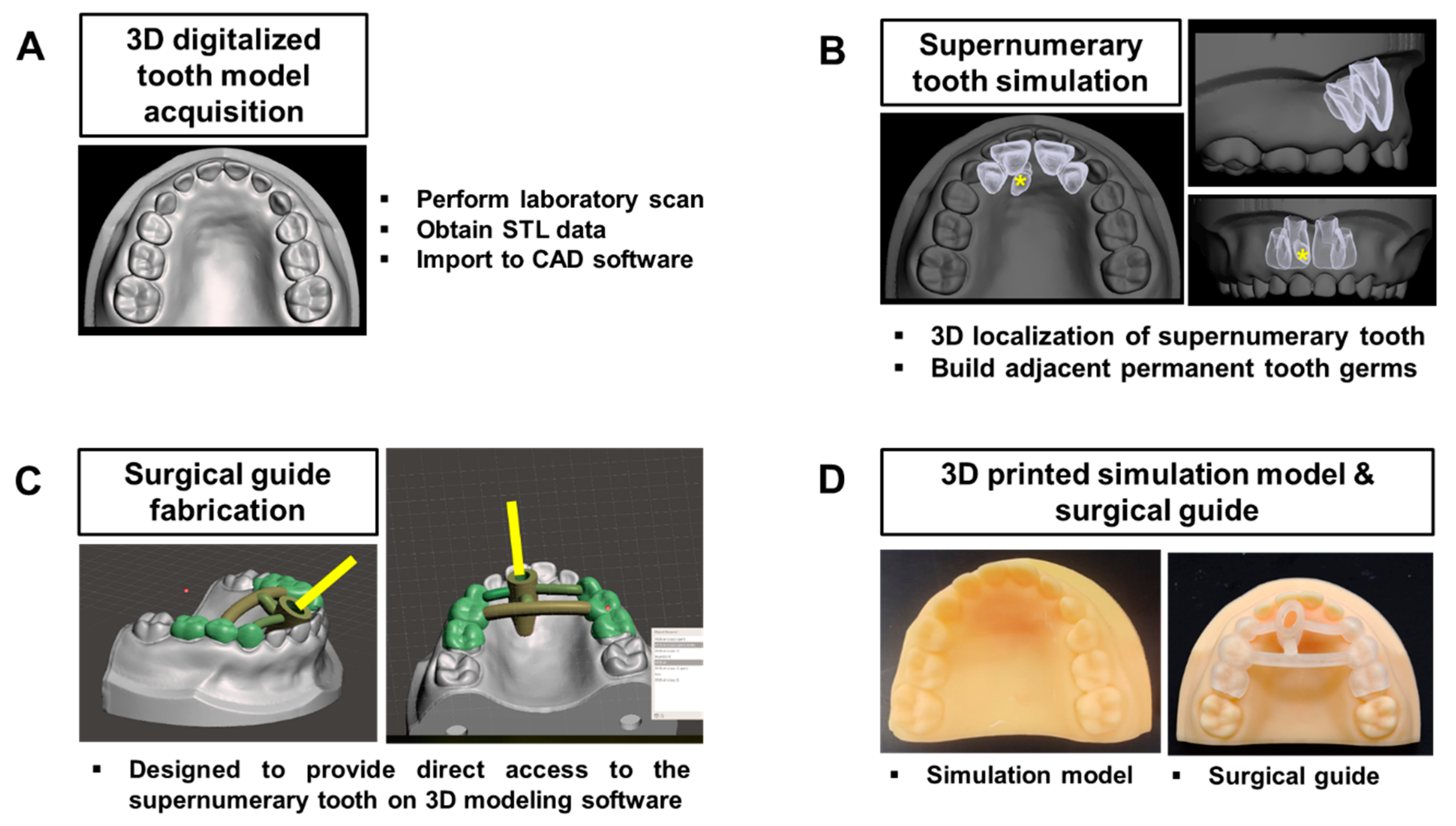
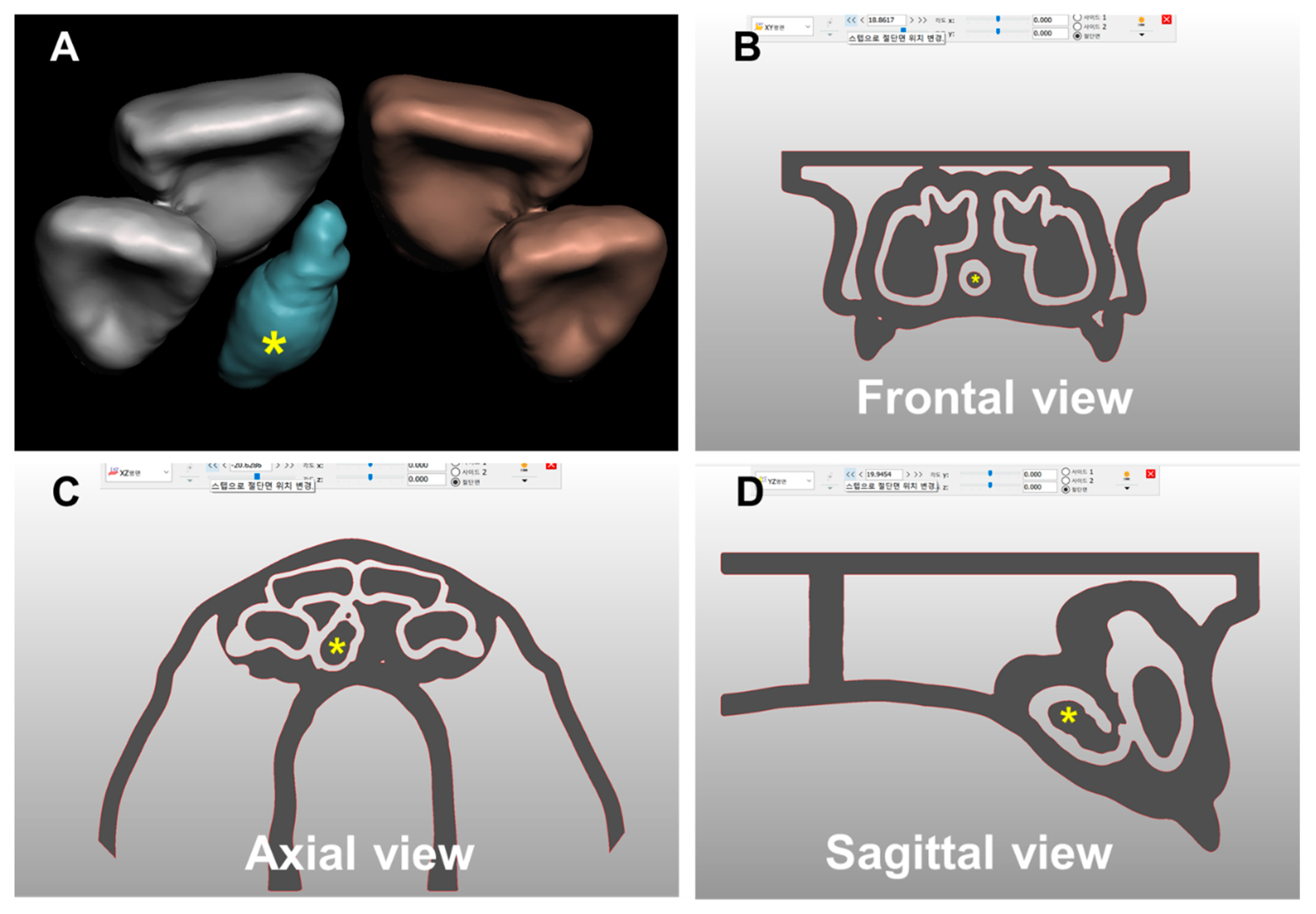
2.1. Development of the 3D Printed Simulation Model and Surgical Guide for ST
2.2. Participant Enrollment
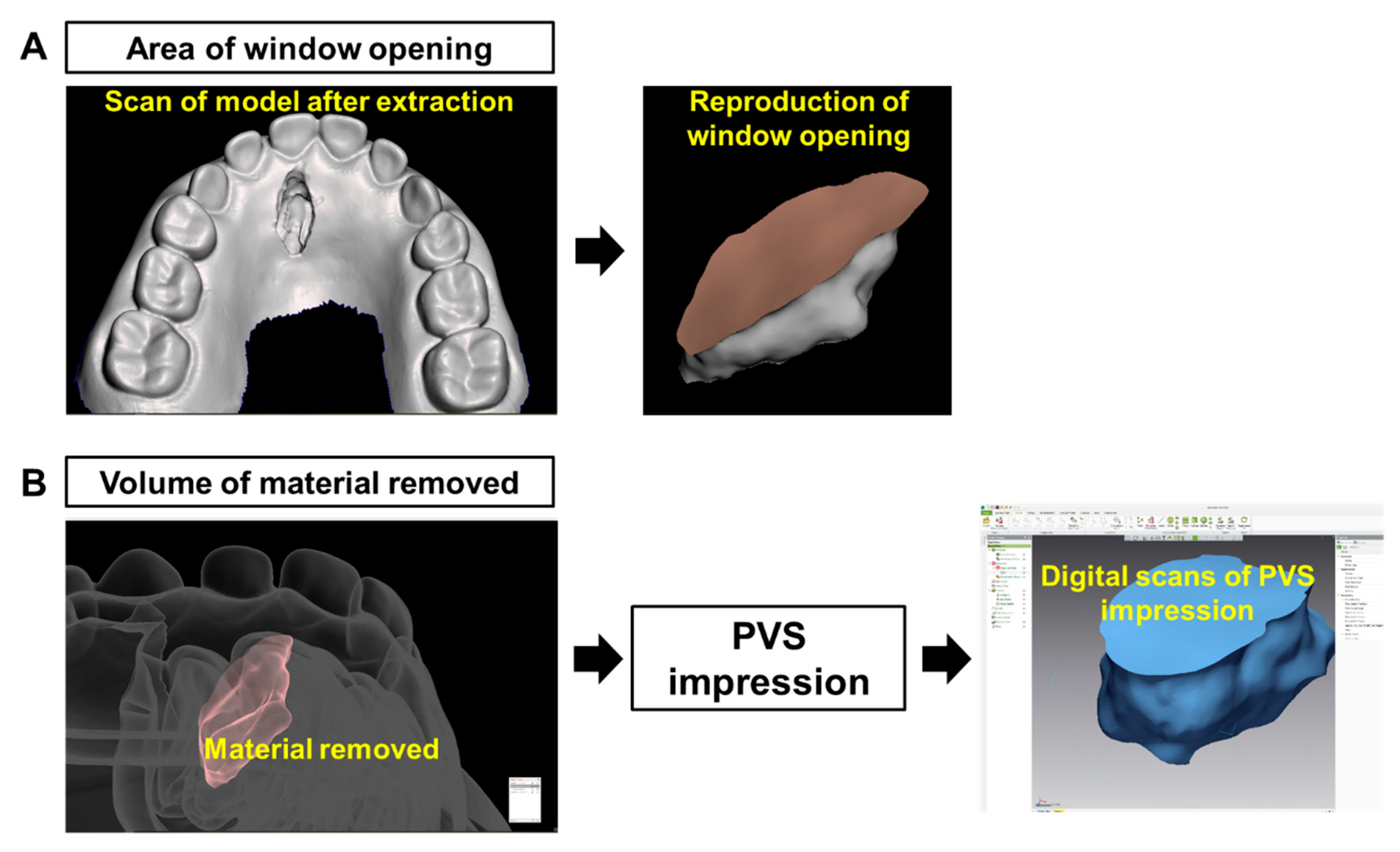
2.3. Evaluating Feasibility of Surgical Guide for Impacted ST Extraction
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rajab, L.D.; Hamdan, M.A. Supernumerary teeth: Review of the literature and a survey of 152 cases. Int. J. Paediatr. Dent. 2002, 12, 244–254. [Google Scholar] [CrossRef]
- Marya, C.M.; Kumar, B.R. Familial occurrence of mesiodentes with unusual findings: Case reports. Quintessence Int. 1998, 29, 49–51. [Google Scholar]
- Asaumi, J.I.; Shibata, Y.; Yanagi, Y.; Hisatomi, M.; Matsuzaki, H.; Konouchi, H.; Kishi, K. Radiographic examination of mesiodens and their associated complications. Dentomaxillofac. Radiol. 2004, 33, 125–127. [Google Scholar] [CrossRef]
- Nam, O.H.; Lee, H.S.; Kim, M.S.; Yun, K.H.; Bang, J.B.; Choi, S.C. Characteristics of mesiodens and its related complications. Pediatr. Dent. 2015, 37, E105–E109. [Google Scholar]
- Stokbro, K.; Aagaard, E.; Torkov, P.; Thygesen, T. Virtual planning in orthognathic surgery. Int. J. Oral Maxillofac. Surg. 2014, 43, 957–965. [Google Scholar] [CrossRef]
- Wang, W.; Somar, M.; Lv, K. Safer alternative for extraction of impacted supernumerary teeth of a patient in the mixed dentition stage with the aid of an image-guided operating system. Br. J. Oral Maxillofac. Surg. 2017, 55, 551–553. [Google Scholar] [CrossRef]
- Wang, J.; Cui, N.H.; Guo, Y.J.; Zhang, W. Navigation-Guided Extraction of Impacted Supernumerary Teeth: A Case Report. J. Oral Maxillofac. Surg. 2017, 75, 1136-e1. [Google Scholar] [CrossRef]
- Nam, O.H.; Lee, H.; Kim, M.S.; Lee, H.S.; Choi, S.C. Simplified technique for easy extraction of impacted supernumerary teeth using guided surgery. Quintessence Int. 2017, 48, 563–567. [Google Scholar]
- Becker, A.; Chaushu, S.; Casap-Caspi, N. Cone-beam computed tomography and the orthosurgical management of impacted teeth. J. Am. Dent. Assoc. 2010, 141 (Suppl. 3), S14–S18. [Google Scholar] [CrossRef]
- Lee, J.W.; Choi, B.J.; Nam, O.H.; Kwon, Y.D. Minimal invasive treatment using patient-specific template for mandibular fractures in children: “Wing-splint” by CAD/CAM technology. Br. J. Oral Maxillofac. Surg. 2016, 54, 1140–1141. [Google Scholar] [CrossRef]
- Seruya, M.; Borsuk, D.E.; Khalifian, S.; Carson, B.S.; Dalesio, N.M.; Dorafshar, A.H. Computer-aided design and manufacturing in craniosynostosis surgery. J. Craniofac. Surg. 2013, 24, 1100–1105. [Google Scholar] [CrossRef]
- Jo, C.; Bae, D.; Choi, B.; Kim, J. Removal of Supernumerary Teeth Utilizing a Computer-Aided Design/Computer-Aided Manufacturing Surgical Guide. J. Oral Maxillofac. Surg. 2017, 75, 924.e1. [Google Scholar] [CrossRef]
- Berman, B. 3-D printing: The new industrial revolution. Bus. Horiz. 2012, 55, 155–162. [Google Scholar] [CrossRef]
- Dawood, A.; Marti Marti, B.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29, 25–42. [Google Scholar] [CrossRef]
- Oberoi, G.; Nitsch, S.; Edelmayer, M.; Janjić, K.; Müller, A.S.; Agis, H. 3D Printing-Encompassing the Facets of Dentistry. Front. Bioeng. Biotechnol. 2018, 6, 172. [Google Scholar] [CrossRef]
- Hu, Y.K.; Xie, Q.Y.; Yang, C.; Xu, G.Z. Computer-designed surgical guide template compared with free-hand operation for mesiodens extraction in premaxilla using “trapdoor” method. Medicine 2017, 96, e7310. [Google Scholar]
- Farwell, D.G.; Reilly, D.F.; Weymuller, E.A., Jr.; Greenberg, D.L.; Staiger, T.O.; Futran, N.A. Predictors of perioperative complications in head and neck patients. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 505–511. [Google Scholar] [CrossRef]
- Davidovich, E.; Wated, A.; Shapira, J.; Ram, D. The influence of location of local anesthesia and complexity/duration of restorative treatment on children’s behavior during dental treatment. Pediatr. Dent. 2013, 35, 333–336. [Google Scholar]
- Getz, T.; Weinstein, P. The effect of structural variables on child behavior in the operatory. Pediatr. Dent. 1981, 3, 262–266. [Google Scholar]
- Bello, S.A.; Adeyemo, W.L.; Bamgbose, B.O.; Obi, E.V.; Adeyinka, A.A. Effect of age, impaction types and operative time on inflammatory tissue reactions following lower third molar surgery. Head Face Med. 2011, 7, 8. [Google Scholar] [CrossRef]
- Muhonen, A.; Ventä, I.; Ylipaavalniemi, P. Factors predisposing to postoperative complications related to wisdom tooth surgery among university students. J. Am. Coll. Health 1997, 46, 39–42. [Google Scholar] [CrossRef]
- Park, S.J.; Leesungbok, R.; Cui, T.; Lee, S.W.; Ahn, S.J. Reliability of a CAD/CAM Surgical Guide for Implant Placement: An In Vitro Comparison of Surgeons’ Experience Levels and Implant Sites. Int. J. Prosthodont. 2017, 30, 367–369. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mean (sec) | SD (sec) | Z | p | |
|---|---|---|---|---|
| Conventional technique | 213.65 | 167.45 | ||
| −2.201 | 0.028 1 | |||
| Surgical guide technique | 114.76 | 42.87 |
| Mean (sec) | SD (sec) | Z | p | |
|---|---|---|---|---|
| Area of window opening (mm2) | ||||
| Conventional technique | 48.10 | 9.44 | ||
| −0.876 | 0.381 | |||
| Surgical guide technique | 45.90 | 8.17 | ||
| Volume of material removed (mm3) | ||||
| Conventional technique | 121.65 | 43.69 | ||
| −2.154 | 0.031 1 | |||
| Surgical guide technique | 99.12 | 17.88 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Chae, Y.K.; Choi, S.; Jih, M.K.; Lee, J.-W.; Choi, S.C.; Nam, O.H. Feasibility of a 3D Surgical Guide Technique for Impacted Supernumerary Tooth Extraction: A Pilot Study with 3D Printed Simulation Models. Appl. Sci. 2019, 9, 3905. https://doi.org/10.3390/app9183905
Lee H, Chae YK, Choi S, Jih MK, Lee J-W, Choi SC, Nam OH. Feasibility of a 3D Surgical Guide Technique for Impacted Supernumerary Tooth Extraction: A Pilot Study with 3D Printed Simulation Models. Applied Sciences. 2019; 9(18):3905. https://doi.org/10.3390/app9183905
Chicago/Turabian StyleLee, Hyeonjong, Yong Kwon Chae, Seulki Choi, Myeong Kwan Jih, Jung-Woo Lee, Sung Chul Choi, and Ok Hyung Nam. 2019. "Feasibility of a 3D Surgical Guide Technique for Impacted Supernumerary Tooth Extraction: A Pilot Study with 3D Printed Simulation Models" Applied Sciences 9, no. 18: 3905. https://doi.org/10.3390/app9183905
APA StyleLee, H., Chae, Y. K., Choi, S., Jih, M. K., Lee, J. -W., Choi, S. C., & Nam, O. H. (2019). Feasibility of a 3D Surgical Guide Technique for Impacted Supernumerary Tooth Extraction: A Pilot Study with 3D Printed Simulation Models. Applied Sciences, 9(18), 3905. https://doi.org/10.3390/app9183905