Progression of Neuropsychiatric Symptoms over Time in an Incident Parkinson’s Disease Cohort (ICICLE-PD)

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
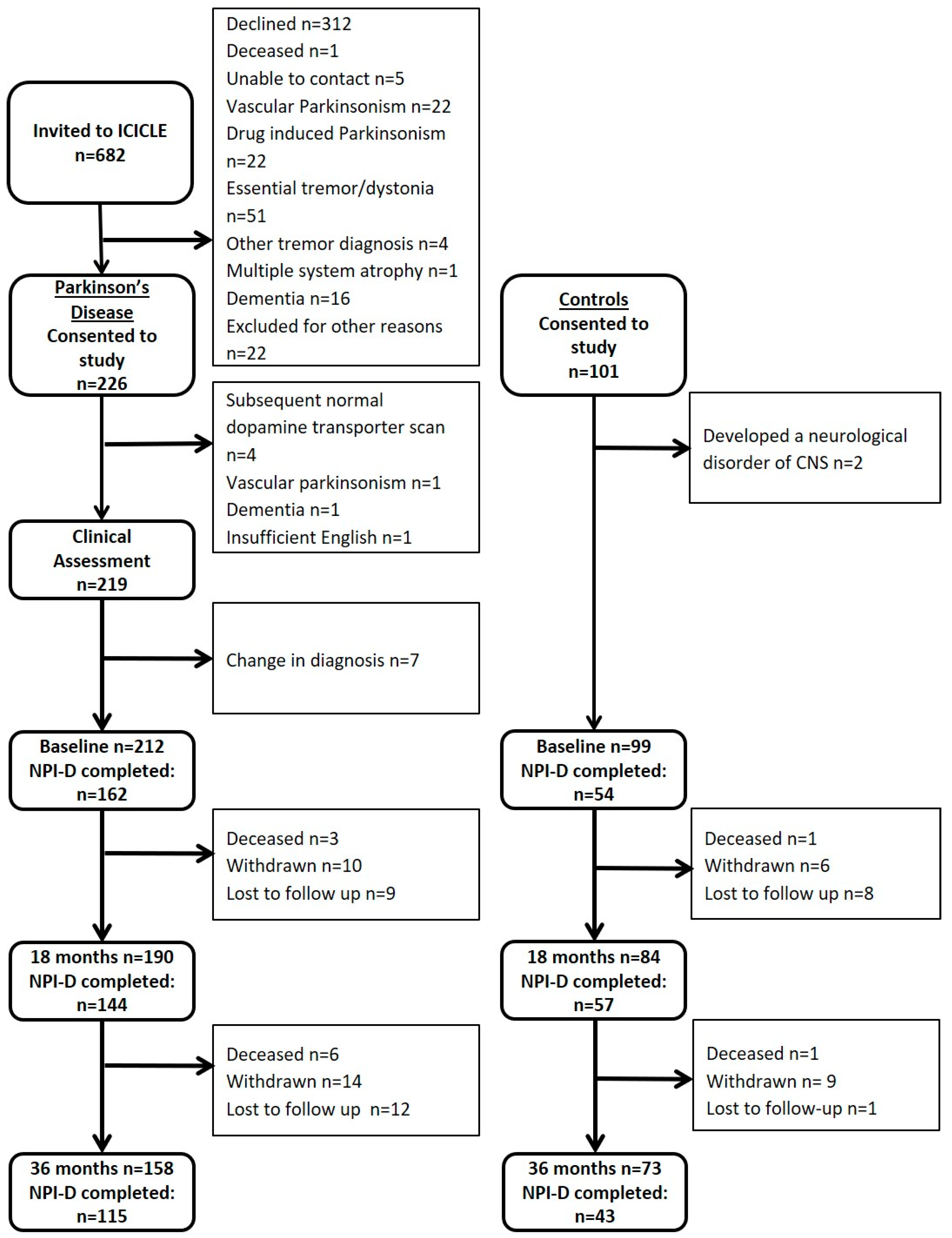
2.1. Participants
2.2. Assessments
2.3. Statistical Analyses
3. Results
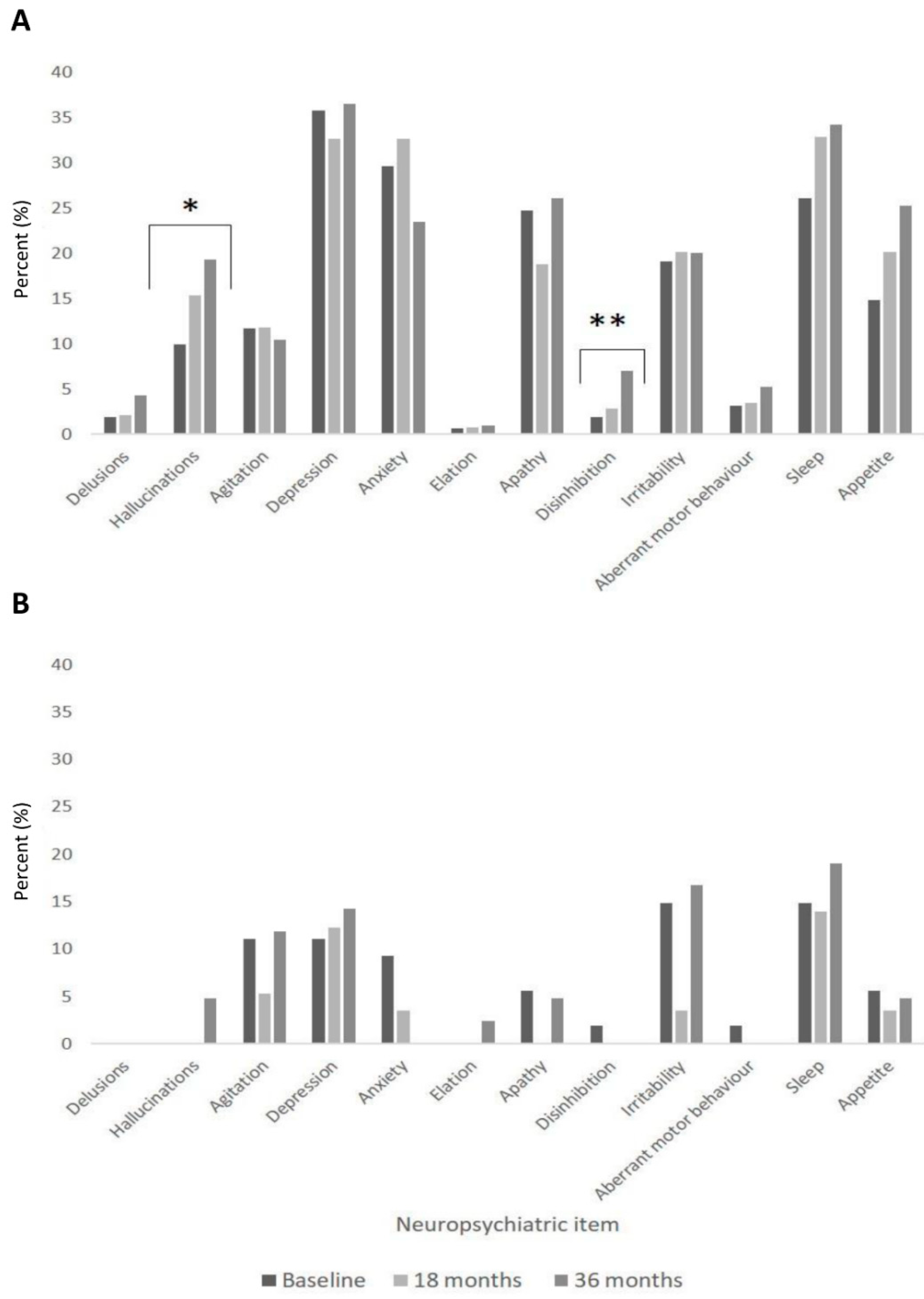
3.1. Comparisons of NPS in PD VS. Controls
3.2. Factors Associated with NPS
3.3. Factors Associated with QoL
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Aarsland, D.; Bronnick, K.; Ehrt, U.; De Deyn, P.P.; Tekin, S.; Emre, M.; Cummings, J.L. Neuropsychiatric symptoms in patients with Parkinson’s disease and dementia: Frequency, profile and associated care giver stress. J. Neurol. Neurosurg. Psychiatry 2007, 78, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Aarsland, D.; Larsen, J.P.; Lim, N.G.; Janvin, C.; Karlsen, K.; Tandberg, E.; Cummings, J.L. Range of neuropsychiatric disturbances in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1999, 67, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Kulisevsky, J.; Pagonabarraga, J.; Gironell, A.; Trapecio Group Study; Pascual-Sedano, B.; García-Sánchez, C. Prevalence and correlates of neuropsychiatric symptoms in Parkinson’s disease without dementia. Mov. Disord. 2008, 23, 1889–1896. [Google Scholar] [CrossRef] [PubMed]
- Thanvi, B.R.; Munshi, S.K.; Vijaykumar, N.; Lo, T.C.N. Neuropsychiatric non-motor aspects of Parkinson’s disease. Postgrad. Med J. 2003, 79, 561–565. [Google Scholar] [CrossRef] [Green Version]
- Todorova, A.; Jenner, P.; Chaudhuri, K.R. Non-motor Parkinson’s: Integral to motor Parkinson’s, yet often neglected. Pr. Neurol. 2014, 14, 310–322. [Google Scholar] [CrossRef]
- Leroi, I.; Harbishettar, V.; Andrews, M.; McDonald, K.; Byrne, E.J.; Burns, A. Carer burden in apathy and impulse control disorders in Parkinson’s disease. Int. J. Geriatr. Psychiatry 2012, 27, 160–166. [Google Scholar] [CrossRef]
- Kano, O.; Ikeda, K.; Cridebring, D.; Takazawa, T.; Yoshii, Y.; Iwasaki, Y. Neurobiology of Depression and Anxiety in Parkinson’s Disease. Park. Dis. 2011, 2011, 1–5. [Google Scholar] [CrossRef] [Green Version]
- DeMaagd, G.; Philip, A. Parkinson’s Disease and Its Management: Part 1: Disease Entity, Risk Factors, Pathophysiology, Clinical Presentation, and Diagnosis. Pharm. Ther. 2015, 40, 504–532. [Google Scholar]
- Brown, R.G.; Landau, S.; Hindle, J.V.; Playfer, J.; Samuel, M.; Wilson, K.C.; Hurt, C.S.; Anderson, R.J.; Carnell, J.; Dickinson, L.; et al. Depression and anxiety related subtypes in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2011, 82, 803–809. [Google Scholar] [CrossRef]
- Prakash, K.M.; Nadkarni, N.V.; Lye, W.; Yong, M.; Tan, E. The impact of non-motor symptoms on the quality of life of Parkinson’s disease patients: A longitudinal study. Eur. J. Neurol. 2016, 23, 854–860. [Google Scholar] [CrossRef]
- Weintraub, D.; Simuni, T.; Caspell-Garcia, C.; Coffey, C.; Lasch, S.; Siderowf, A.; Aarsland, D.; Barone, P.; Burn, D.; Chahine, L.M.; et al. Cognitive performance and neuropsychiatric symptoms in early, untreated Parkinson’s disease. Mov. Disord. 2015, 30, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Yarnall, A.J.; Breen, D.P.; Duncan, G.W.; Khoo, T.K.; Coleman, S.Y.; Firbank, M.J.; Nombela, C.; Winder-Rhodes, S.; Evans, J.R.; Rowe, J.B.; et al. Characterizing mild cognitive impairment in incident Parkinson disease: The ICICLE-PD study. Neurology 2014, 82, 308–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, A.J.; E Daniel, S.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical diagnostic criteria for dementia associated with Parkinson’s disease. Mov. Disord. 2007, 22, 1689–1707. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H.; Bédirian, V. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martínez-Martín, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427. [Google Scholar] [CrossRef] [Green Version]
- Peto, V.; Jenkinson, C.; Fitzpatrick, R.; Greenhall, R. The development and validation of a short measure of functioning and well being for individuals with Parkinson’s disease. Qual. Life Res. 1995, 4, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Clarke, C.E.; Gray, R. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The Neuropsychiatric Inventory: Comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeke, G.; Molenberghs, G.; Rizopoulos, D. Linear Mixed Models for Longitudinal Data; Springer Science & Business Media: Berlin, Germany, 2009. [Google Scholar]
- Williams, D.R.; Lees, A.J. Visual hallucinations in the diagnosis of idiopathic Parkinson’s disease: A retrospective autopsy study. Lancet Neurol. 2005, 4, 605–610. [Google Scholar] [CrossRef]
- Holroyd, S.; Currie, L.; Wooten, G. Prospective study of hallucinations and delusions in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2001, 70, 734–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, J.; David, A.S. Visual hallucinations in Parkinson’s disease: A review and phenomenological survey. J. Neurol. Neurosurg. Psychiatry 2001, 70, 727–733. [Google Scholar] [CrossRef]
- Hobson, P.; Meara, J. Risk and incidence of dementia in a cohort of older subjects with Parkinson’s disease in the United Kingdom. Mov. Disord. 2004, 19, 1043–1049. [Google Scholar] [CrossRef]
- Aarsland, D.; Larsen, J.P.; Tandberg, E.; Laake, K. Predictors of nursing home placement in Parkinson’s disease: A population-based, prospective study. J. Am. Geriatr. Soc. 2000, 48, 938–942. [Google Scholar] [CrossRef]
- Leiknes, I.; Aarsland, D.; Larsen, J.P.; Tysnes, O.-B. Caregiver distress associated with neuropsychiatric problems in patients with early Parkinson’s disease: The Norwegian ParkWest study. Acta Neurol. Scand. 2010, 122, 418–424. [Google Scholar] [CrossRef]
- Tanji, H.; Anderson, K.E.; Gruber-Baldini, A.L.; Fishman, P.S.; Reich, S.G.; Weiner, W.J.; Shulman, L.M. Mutuality of the marital relationship in Parkinson’s disease. Mov. Disord. 2008, 23, 1843–1849. [Google Scholar] [CrossRef]
- Lyons, K.S.; Stewart, B.J.; Archbold, P.G.; Carter, J.H. Optimism, Pessimism, Mutuality, and Gender: Predicting 10-Year Role Strain in Parkinson’s Disease Spouses. Gerontologist 2009, 49, 378–387. [Google Scholar] [CrossRef] [Green Version]
- Leroi, I.; Pantula, H.; McDonald, K.; Harbishettar, V. Neuropsychiatric Symptoms in Parkinson’s Disease with Mild Cognitive Impairment and Dementia. Park. Dis. 2012, 2012, 1–10. [Google Scholar] [CrossRef]
- Jones, A.J.; Kuijer, R.G.; Livingston, L.; Myall, D.; Horne, K.; Macaskill, M.; Pitcher, T.; Barrett, P.T.; Anderson, T.J.; Dalrymple-Alford, J.C. Caregiver burden is increased in Parkinson’s disease with mild cognitive impairment (PD-MCI). Transl. Neurodegener. 2017, 6, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrag, A.; Jahanshahi, M.; Quinn, N. What contributes to quality of life in patients with Parkinson’s disease? J. Neurol. Neurosurg. Psychiatry 2000, 69, 308–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balestrino, R.; Martinez-Martin, P. Reprint of “Neuropsychiatric symptoms, behavioural disorders, and quality of life in Parkinson’s disease”. J. Neurol. Sci. 2017, 374, 3–8. [Google Scholar] [CrossRef]
- McKinlay, A.; Grace, R.; Dalrymple-Alford, J.; Anderson, T.; Fink, J.; Roger, D. A profile of neuropsychiatric problems and their relationship to quality of life for Parkinson’s disease patients without dementia. Park. Relat. Disord. 2008, 14, 37–42. [Google Scholar] [CrossRef]
- Weintraub, D.; Moberg, P.J.; Duda, J.E.; Katz, I.R.; Stern, M.B. Recognition and treatment of depression in Parkinson’s disease. J. Geriatr. Psychiatry Neurol. 2003, 16, 178–183. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline | 18 Months | 36 Months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PD n = 162 | Control n = 54 | T/z/χ2 | p-value | PD n = 144 | Control n = 57 | T/z/χ2 | p-value | PD n = 115 | Control n = 42 | T/z/χ2 | p-value | |
| Age (years) | 66.2 (10.1) | 67.5 (7.5) | −1.0 | 0.335 † | 68.3 (9.4) | 68.6 (7.9) | −0.2 | 0.830 † | 69.3 (9.5) | 70.6 (6.4) | −1.0 | 0.313 † |
| Sex (Male) n (%) | 104 (64.2) | 30 (55.6) | 1.3 | 0.257 * | 97 (67.4) | 30 (52.6) | 3.8 | 0.051 * | 79 (68.7) | 23 (54.8) | 2.6 | 0.105 * |
| Education (years) | 12.5 (3.5) | 13.0 (3.3) | −1.1 | 0.261 | 12.8 (3.5) | 13.1 (3.2) | −0.9 | 0.373 | 12.7 (3.3) | 12.8 (3.2) | −0.3 | 0.801 |
| Disease duration (months) | 6.1 (5.4) | - | - | - | 24.1 (23.4) | - | - | - | 42.1 (41.4) | - | - | - |
| GDS-15 | 3.1 (2.7) | 1.0 (1.6) | −6.0 | <0.001 | 2.9 (2.7) | 1.2 (2.0) | −5.2 | <0.001 | 3.1 (2.6) | 1.2 (2.0) | −5.0 | <0.001 |
| MoCA a | 25.3 (3.4) | 27.2 (2.2) | −3.6 | <0.001 | 26.1 (3.7) | 27.6 (2.7) | −2.9 | 0.004 | 25.6 (3.7) | 27.4 (3.0) | −3.0 | 0.002 |
| NPI total score | 6.7 (9.8) | 1.9 (4.3) | −4.5 | <0.001 | 6.4 (9.5) | 1.3 (3.3) | −5.4 | <0.001 | 7.2 (9.8) | 3.3 (8.3) | −4.3 | <0.001 |
| NPI-Caregiver distress score | 3.3 (4.8) | 0.9 (2.2) | −4.4 | <0.001 | 2.7 (4.0) | 0.6 (1.9) | −4.7 | <0.001 | 3.8 (5.3) | 1.5 (4.0) | −4.0 | <0.001 |
| PDQ-39 | 19.0 (14.3) | - | - | - | 21.1 (16.3) | - | - | - | 22.3 (17.2) | - | - | - |
| MDS-UPDRS-II | 10.2 (5.9) | - | - | - | 11.8 (6.0) | - | - | - | 14.5 (7.6) | - | - | - |
| MDS-UPDRS-III | 27.7 (12.3) | - | - | - | 33.3 (12.1) | - | - | - | 35.2 (15.0) | - | - | - |
| Hoehn and Yahr | 1.9 (0.7) | - | - | - | 2.2 (0.5) | - | - | - | 2.1 (0.6) | - | - | - |
| LEDD (mg/day) | 190.4 (159.9) | - | - | - | 413.8 (214.3) | - | - | - | 518.2 (273.5) | - | - | - |
| PDD n (%) | 0 (0) | - | - | - | 8 (5.6) | - | - | - | 14 (12.2) | - | - | - |
| PD | Control | |||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | t-value | p-value | β | SE | t-value | p-value | |
| NPI total | ||||||||
| Basic model | ||||||||
| Sex (Male) | 1.2 | 1.3 | 1.0 | 0.329 | −0.8 | 1.0 | −0.847 | 0.399 |
| Age | −0.1 | 0.1 | −1.6 | 0.105 | 0.1 | 0.1 | 0.940 | 0.350 |
| Time | 0.4 | 0.4 | 0.9 | 0.390 | 0.6 | 0.5 | 1.193 | 0.235 |
| Basic model + MDS-UPDRS III | ||||||||
| MDS-UPDRS III | 0.0 | 0.1 | 0.6 | 0.563 | ||||
| MDS-UPDRS III × Time | 0.1 | 0.0 | 2.0 | 0.044 | ||||
| Basic model + MoCA | ||||||||
| MoCA | −0.4 | 0.2 | −1.8 | 0.075 | 0.0 | 147.6 | 0.1 | 0.900 |
| MoCA × Time | −0.1 | 0.1 | −0.7 | 0.457 | −0.5 | 126.3 | −1.9 | 0.057 |
| NPI carer distress total | ||||||||
| Basic model | ||||||||
| Sex (Male) | 0.8 | 0.6 | 1.3 | 0.206 | 0.1 | 0.5 | 0.124 | 0.901 |
| Age | 0.0 | 0.0 | −0.3 | 0.791 | 0.0 | 0.0 | 0.525 | 0.601 |
| Time | 0.3 | 0.3 | 1.0 | 0.404 | 0.3 | 0.3 | 1.119 | 0.265 |
| Basic model + MDS-UPDRS III | ||||||||
| MDS-UPDRS III | 0.0 | 0.0 | 0.1 | 0.957 | ||||
| MDS-UPDRS III × Time | 0.1 | 0.0 | 3.1 | 0.002 | ||||
| Basic model + MoCA | ||||||||
| MoCA | −0.3 | 0.1 | −2.7 | 0.007 | 0.0 | 147.8 | −0.2 | 0.865 |
| MoCA × Time | 0.0 | 0.1 | −0.8 | 0.432 | −0.2 | 127.2 | −1.9 | 0.065 |
| Basic Model | β | SE | t Value | p-Value |
|---|---|---|---|---|
| Basic model | ||||
| Sex (Female) | −3.4 | 1.7 | −2.1 | 0.041 |
| Education (Years) | −0.6 | 0.2 | −2.5 | 0.012 |
| Age | −0.3 | 0.1 | −3.9 | <0.001 |
| LEDD | 0.0 | 0.0 | 3.1 | 0.002 |
| MDS-UPDRS III | 0.4 | 0.0 | 8.3 | <0.001 |
| Time (Assessment) | 12.5 | 3.4 | 3.7 | <0.001 |
| MoCA | −0.1 | 0.2 | −0.4 | 0.654 |
| MoCA × Time | −0.5 | 0.1 | −3.8 | <0.001 |
| Basic model + NPI Total | ||||
| NPI Total | 0.3 | 0.1 | 3.9 | <0.001 |
| NPI Total × Time | 0.0 | 0.1 | 0.6 | 0.551 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dlay, J.K.; Duncan, G.W.; Khoo, T.K.; Williams-Gray, C.H.; Breen, D.P.; Barker, R.A.; Burn, D.J.; Lawson, R.A.; Yarnall, A.J. Progression of Neuropsychiatric Symptoms over Time in an Incident Parkinson’s Disease Cohort (ICICLE-PD). Brain Sci. 2020, 10, 78. https://doi.org/10.3390/brainsci10020078
Dlay JK, Duncan GW, Khoo TK, Williams-Gray CH, Breen DP, Barker RA, Burn DJ, Lawson RA, Yarnall AJ. Progression of Neuropsychiatric Symptoms over Time in an Incident Parkinson’s Disease Cohort (ICICLE-PD). Brain Sciences. 2020; 10(2):78. https://doi.org/10.3390/brainsci10020078
Chicago/Turabian StyleDlay, J. K., G. W. Duncan, T. K. Khoo, C. H. Williams-Gray, D. P. Breen, R. A. Barker, D. J. Burn, R. A. Lawson, and A. J. Yarnall. 2020. "Progression of Neuropsychiatric Symptoms over Time in an Incident Parkinson’s Disease Cohort (ICICLE-PD)" Brain Sciences 10, no. 2: 78. https://doi.org/10.3390/brainsci10020078
APA StyleDlay, J. K., Duncan, G. W., Khoo, T. K., Williams-Gray, C. H., Breen, D. P., Barker, R. A., Burn, D. J., Lawson, R. A., & Yarnall, A. J. (2020). Progression of Neuropsychiatric Symptoms over Time in an Incident Parkinson’s Disease Cohort (ICICLE-PD). Brain Sciences, 10(2), 78. https://doi.org/10.3390/brainsci10020078