Behavioral and Electrophysiological Correlates of Performance Monitoring and Development in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Electrophysiological Methods
2.4. Analyses
3. Results
3.1. Behavioral Data in Patients with ADHD and Healthy Controls
3.2. ERP Data in Patients with ADHD and Healthy Controls
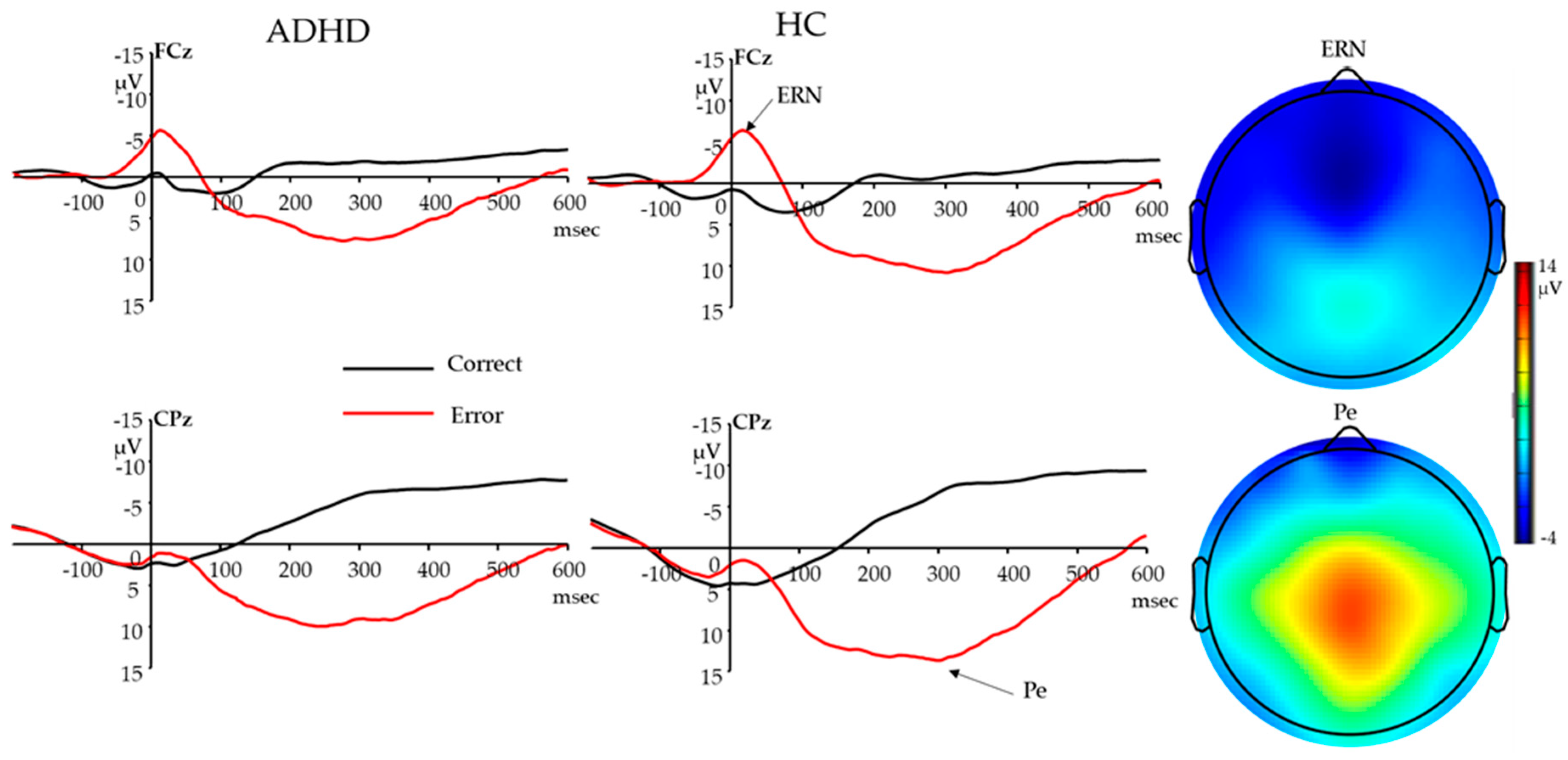
3.2.1. Response-Locked ERN
3.2.2. Response-Locked Pe
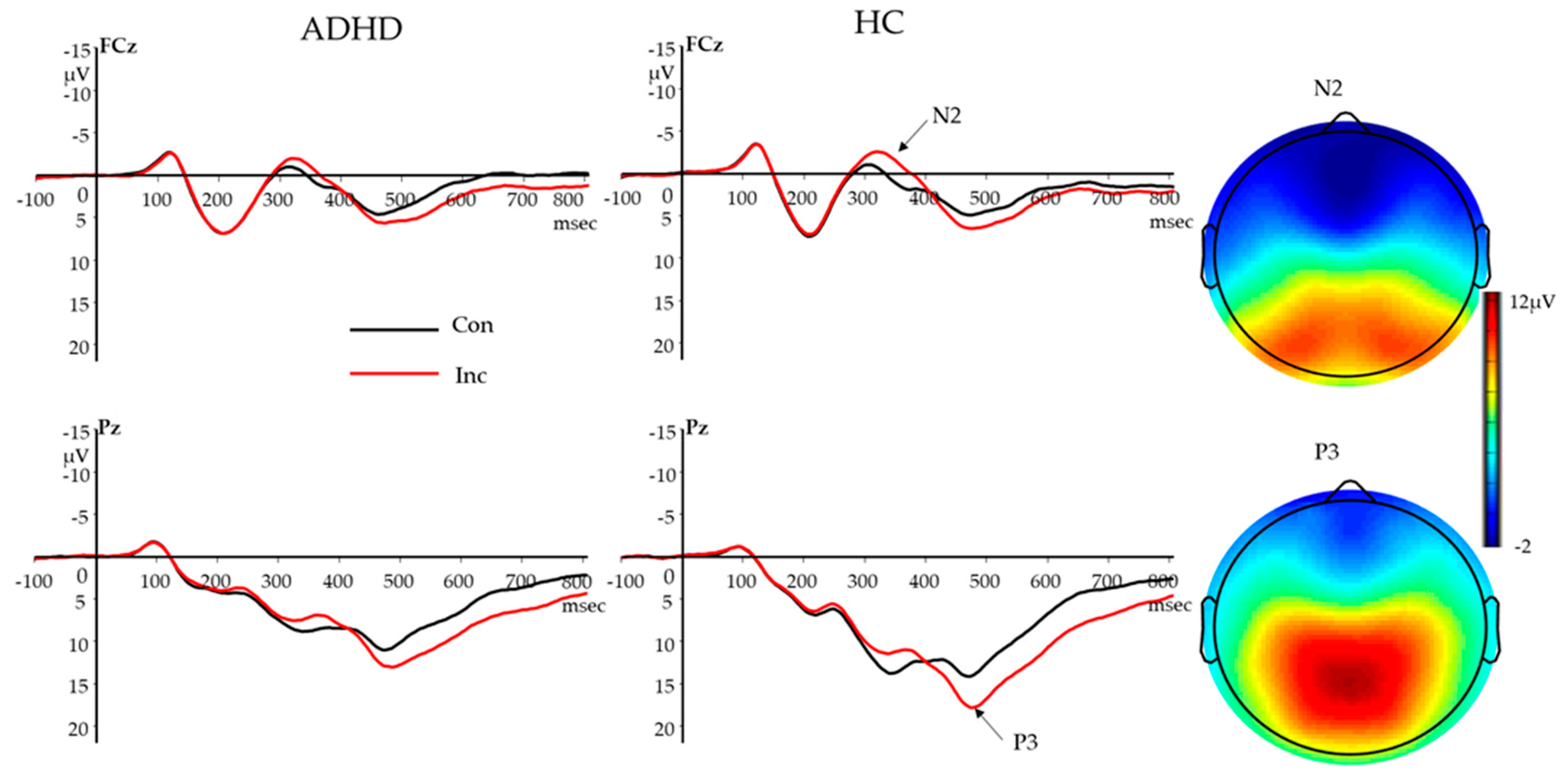
3.2.3. Stimulus-Locked N2
3.2.4. Stimulus-Locked P3
3.3. The Association of Behavioral and ERP Measures with ADHD Symptoms and ADHD Subtype
3.3.1. The Association of Behavioral and ERP Measures with K-SAD-PL ADHD Symptoms
3.3.2. The Association of Behavioral and ERP Measures with CBCL ADHD Problems Scale Scores
3.3.3. Behavioral and ERP Measures Among Different ADHD Subtypes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Willcutt, E.G. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Boil. Psychiatry 2005, 57, 1336–1346. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, F.X.; Tannock, R. Neuroscience of attention-deficit/hyperactivity disorder: the search for endophenotypes. Nat. Rev. Neurosci. 2002, 3, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Ehlis, A.-C.; Deppermann, S.; Fallgatter, A.J. Performance monitoring and post-error adjustments in adults with attention-deficit/hyperactivity disorder: an EEG analysis. J. Psychiatry Neurosci. 2018, 43, 396–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faraone, S.V.; Biederman, J.; Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychol. Med. 2006, 36, 159–165. [Google Scholar] [CrossRef]
- Shiels, K.; Hawk, L.W., Jr. Self-regulation in ADHD: The role of error processing. Clin. Psychol. Rev. 2010, 30, 951–961. [Google Scholar] [CrossRef] [Green Version]
- Klein, C.; Wendling, K.; Huettner, P.; Ruder, H.; Peper, M. Intra-subject variability in attention-deficit hyperactivity disorder. Boil. Psychiatry 2006, 60, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M.J.; Mader, K.; Schreppel, T.; Jacob, C.; Heine, M.; Boreatti-Hümmer, A.; Ehlis, A.-C.; Scheuerpflug, P.; Pauli, P.; Fallgatter, A.J. Neural correlates of performance monitoring in adult patients with attention deficit hyperactivity disorder (ADHD). World J. Boil. Psychiatry 2010, 11, 457–464. [Google Scholar] [CrossRef]
- Balogh, L.; Czobor, P. Post-error slowing in patients with ADHD: a meta-analysis. J. Atten. Disord. 2016, 20, 1004–1016. [Google Scholar] [CrossRef] [PubMed]
- Dutilh, G.; Vandekerckhove, J.; Forstmann, B.U.; Keuleers, E.; Brysbaert, M.; Wagenmakers, E.J. Testing theories of post-error slowing. Atten. Percept. Psychophys. 2012, 74, 454–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiersema, J.R.; Van Der Meere, J.J.; Roeyers, H. ERP correlates of impaired error monitoring in children with ADHD. J. Neural Transm. 2005, 112, 1417–1430. [Google Scholar] [CrossRef] [PubMed]
- Schachar, R.J.; Chen, S.; Logan, G.D.; Ornstein, T.J.; Crosbie, J.; Ickowicz, A.; Pakulak, A. Evidence for an error monitoring deficit in attention deficit hyperactivity disorder. J. Abnorm. Child Psychol. 2004, 32, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Jonkman, L.; Van Melis, J.J.; Kemner, C.; Markus, C.R. Methylphenidate improves deficient error evaluation in children with ADHD: An event-related brain potential study. Boil. Psychol. 2007, 76, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Van Meel, C.S.; Heslenfeld, D.J.; Oosterlaan, J.; Sergeant, J.A. Adaptive control deficits in attention-deficit/hyperactivity disorder (ADHD): The role of error processing. Psychiatry Res. 2007, 151, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Gehring, W.J.; Liu, Y.; Orr, J.M.; Carp, J. The error-related negativity (ERN/Ne); Luck, S.J., Kappenman, E.S., Eds.; The Oxford Handbook of Event-Related Potential Components; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Ullsperger, M.; Danielmeier, C.; Jocham, G. Neurophysiology of performance monitoring and adaptive behavior. Physiol. Rev. 2014, 94, 35–79. [Google Scholar] [CrossRef] [PubMed]
- Michelini, G.; Kitsune, G.L.; Cheung, C.H.; Brandeis, D.; Banaschewski, T.; Asherson, P.; McLoughlin, G.; Kuntsi, J. Attention-deficit/hyperactivity disorder remission is linked to better neurophysiological error detection and attention-vigilance processes. Boil. Psychiatry 2016, 80, 923–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquardt, L.; Eichele, H.; Lundervold, A.J.; Haavik, J.; Eichele, T. Event-related-potential (ERP) correlates of performance monitoring in adults with attention-deficit hyperactivity disorder (ADHD). Front. Psychol. 2018, 9, 485. [Google Scholar] [CrossRef]
- Groom, M.J.; Cahill, J.D.; Bates, A.T.; Jackson, G.M.; Calton, T.G.; Liddle, P.F.; Hollis, C. Electrophysiological indices of abnormal error-processing in adolescents with attention deficit hyperactivity disorder (ADHD). J. Child. Psychol. Psychiatry. 2010, 51, 66–76. [Google Scholar] [CrossRef]
- Wiersema, J.R.; van der Meere, J.J.; Roeyers, H. ERP correlates of error monitoring in adult ADHD. J. Neural. Transm. (Vienna) 2009, 116, 371–379. [Google Scholar] [CrossRef]
- Burgio-Murphy, A.; Klorman, R.; Shaywitz, S.E.; Fletcher, J.M.; Marchione, K.E.; Holahan, J.; Stuebing, K.K.; Thatcher, J.E.; Shaywitz, B.A. Error-related event-related potentials in children with attention-deficit hyperactivity disorder, oppositional defiant disorder, reading disorder, and math disorder. Biol. Psychol. 2007, 75, 75–86. [Google Scholar] [CrossRef] [Green Version]
- Meyer, A.; Hajcak, G. A review examining the relationship between individual differences in the error-related negativity and cognitive control. Int. J. Psychophysiol. 2019, 144, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Groen, Y.; Wijers, A.A.; Mulder, L.J.; Waggeveld, B.; Minderaa, R.B.; Althaus, M. Error and feedback processing in children with ADHD and children with Autistic Spectrum Disorder: An EEG event-related potential study. Clin. Neurophysiol. 2008, 119, 2476–2493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van De Voorde, S.; Roeyers, H.; Wiersema, J.R. Error monitoring in children with ADHD or reading disorder: An event-related potential study. Boil. Psychol. 2010, 84, 176–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albrecht, B.; Brandeis, D.; Uebel, H.; Heinrich, H.; Mueller, U.C.; Hasselhorn, M.; Steinhausen, H.C.; Rothenberger, A.; Banaschewski, T. Action monitoring in boys with attention-deficit/hyperactivity disorder, their nonaffected siblings, and normal control subjects: Evidence for an endophenotype. Biological Psychiatry 2008, 64, 615–625. [Google Scholar] [CrossRef] [Green Version]
- Kopp, B.; Rist, F.; Mattler, U. N200 in the flanker task as a neurobehavioral tool for investigating executive control. Psychophysiology 1996, 33, 282–294. [Google Scholar] [CrossRef]
- Nieuwenhuis, S.; Yeung, N.; Wildenberg, W.V.D.; Ridderinkhof, K.R. Electrophysiological correlates of anterior cingulate function in a go/no-go task: effects of response conflict and trial type frequency. Cogn. Affect. Behav. Neurosci. 2003, 3, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Van Veen, V.; Carter, C.S. The anterior cingulate as a conflict monitor: fMRI and ERP studies. Physiol. Behav. 2002, 77, 477–482. [Google Scholar] [CrossRef]
- Polich, J. Updating P300: An integrative theory of P3a and P3b. Clin. Neurophysiol. 2007, 118, 2128–2148. [Google Scholar] [CrossRef] [Green Version]
- Johnstone, S.J.; Barry, R.J.; Clarke, A.R. Behavioural and ERP indices of response inhibition during a Stop-signal task in children with two subtypes of Attention-Deficit Hyperactivity Disorder. Int. J. Psychophysiol. 2007, 66, 37–47. [Google Scholar] [CrossRef]
- Groom, M.J.; Bates, A.T.; Jackson, G.M.; Calton, T.G.; Liddle, P.F.; Hollis, C. Event-related potentials in adolescents with schizophrenia and their siblings: a comparison with attention-deficit/hyperactivity disorder. Boil. Psychiatry 2008, 63, 784–792. [Google Scholar] [CrossRef]
- Shen, I.-H.; Tsai, S.-Y.; Duann, J.-R. Inhibition control and error processing in children with attention deficit/hyperactivity disorder: An event-related potentials study. Int. J. Psychophysiol. 2011, 81, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.L.; Johnstone, S.J.; Barry, R.J. Inhibitory processing during the Go/NoGo task: an ERP analysis of children with attention-deficit/hyperactivity disorder. Clin. Neurophysiol. 2004, 115, 1320–1331. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, S.J.; Barry, R.J.; Clarke, A.R. Ten years on: A follow-up review of ERP research in attention-deficit/hyperactivity disorder. Clin. Neurophysiol. 2013, 124, 644–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szuromi, B.; Czobor, P.; Komlosi, S.; Bitter, I. P300 deficits in adults with attention deficit hyperactivity disorder: A meta-analysis. Psychol. Med. 2011, 41, 1529–1538. [Google Scholar] [CrossRef]
- Johnstone, S.J.; Barry, R.J.; Markovska, V.; Dimoska, A.; Clarke, A.R. Response inhibition and interference control in children with AD/HD: A visual ERP investigation. Int. J. Psychophysiol. 2009, 72, 145–153. [Google Scholar] [CrossRef]
- Kratz, O.; Studer, P.; Malcherek, S.; Erbe, K.; Moll, G.H.; Heinrich, H. Attentional processes in children with ADHD: An event-related potential study using the attention network test. Int. J. Psychophysiol. 2011, 81, 82–90. [Google Scholar] [CrossRef]
- Barry, R.J.; Johnstone, S.J.; Clarke, A.R. A review of electrophysiology in attention-deficit/hyperactivity disorder: II. Event-related potentials. Clin. Neurophysiol. 2003, 114, 184–198. [Google Scholar] [CrossRef]
- A Friedman, L.; Rapoport, J.L. Brain development in ADHD. Curr. Opin. Neurobiol. 2015, 30, 106–111. [Google Scholar] [CrossRef]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial Reliability and Validity Data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef]
- Hanna, G.L. Schedule for obsessive-compulsive and other behavioral syndromes (SOCOBS); University of Michigan: Ann Abor, MI, USA, 2013. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA school-age forms & profiles; University of Vermont, Research Center for Children, Youth, and Families: Burlington, VT, USA, 2001. [Google Scholar]
- Berument, S.K.; Rutter, M.; Lord, C.; Pickles, A.; Bailey, A. Autism screening questionnaire: diagnostic validity. Br. J. Psychiatry 1999, 175, 444–451. [Google Scholar] [CrossRef]
- American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders. Diagn. Stat. Man. Ment. Disord. 2013.
- Leckman, J.F.; Sholomskas, D.; Thompson, W.D.; Belanger, A.; Weissman, M.M. Best estimate of lifetime psychiatric diagnosis: a methodological study. Arch. Gen. Psychiatry 1982, 39, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Abbreviated Scale of Intelligence (WASI-II); Psychological Corporation: San Antonio, TX, USA, 2011. [Google Scholar]
- Eriksen, B.A.; Eriksen, C.W. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percep. Psychophysics 1974, 16, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Hanna, G.L.; Liu, Y.; Isaacs, Y.E.; Ayoub, A.M.; Torres, J.J.; O’Hara, N.B.; Gehring, W.J. Withdrawn/depressed behaviors and error-Related brain activity in youth With Obsessive-Compulsive Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 906–913.e2. [Google Scholar] [CrossRef] [Green Version]
- Gratton, G.; Coles, M.G.; Donchin, E. A new method for off-line removal of ocular artifact. Electroencephalogr. Clin. Neurophysiol. 1983, 55, 468–484. [Google Scholar] [CrossRef]
- Simons, R.F. The way of our errors: theme and variations. Psychophysiology 2010, 47, 1–14. [Google Scholar] [CrossRef]
- Best, J.R.; Miller, P.H. A developmental perspective on executive function. Child Dev. 2010, 81, 1641–1660. [Google Scholar] [CrossRef] [Green Version]
- Davidson, M.C.; Amso, D.; Anderson, L.C.; Diamond, A. Development of cognitive control and executive functions from 4 to 13 years: evidence from manipulations of memory, inhibition, and task switching. Neuropsychologia 2006, 44, 2037–2078. [Google Scholar] [CrossRef] [Green Version]
- Doehnert, M.; Brandeis, D.; Imhof, K.; Drechsler, R.; Steinhausen, H.-C. Mapping attention-deficit/hyperactivity disorder from childhood to adolescence—no neurophysiologic evidence for a developmental lag of attention but some for Inhibition. Boil. Psychiatry 2010, 67, 608–616. [Google Scholar] [CrossRef] [Green Version]
- Tamnes, C.K.; Walhovd, K.B.; Torstveit, M.; Sells, V.T.; Fjell, A.M. Performance monitoring in children and adolescents: a review of developmental changes in the error-related negativity and brain maturation. Dev. Cogn. Neurosci. 2013, 6, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Wiersema, J.R.; Van Der Meere, J.J.; Roeyers, H. Developmental changes in error monitoring: an event-related potential study. Neuropsychologia 2007, 45, 1649–1657. [Google Scholar] [CrossRef] [PubMed]
- Geburek, A.; Rist, F.; Gediga, G.; Stroux, D.; Pedersen, A. Electrophysiological indices of error monitoring in juvenile and adult attention deficit hyperactivity disorder (ADHD)—a meta-analytic appraisal. Int. J. Psychophysiol. 2013, 87, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Moser, J.S.; Moran, T.P.; Schroder, H.S.; Donnellan, M.B.; Yeung, N. On the relationship between anxiety and error monitoring: a meta-analysis and conceptual framework. Front. Hum. Neurosci. 2013, 7, 466. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Mean | Group Difference | Age Correlation (r) | CBCL ADHD Problems Scale Correlation (r), Covarying Age | ||||
|---|---|---|---|---|---|---|---|
| ADHD | HC | F | p | ADHD | HC | ||
| Demographic and Clinical Data | |||||||
| Age | 13.6 ± 3.2 | 13.6 ± 3.1 | 0.00 | 0.982 | |||
| IQ | 106.3 ± 13.4 | 110.6 ± 10.2 | 4.38 | 0.038 | |||
| SCQ | 4.0 ± 3.5 | 1.8 ± 1.8 | 22.76 | 0.000 | |||
| CBCL_ADHD | 65.3 ± 8.3 | 51.3 ± 3.2 | 191.71 | 0.000 | |||
| ADHD Symptom Counts from K-SAD-PL | |||||||
| Hyperactive/Impulsive | 3.8 ± 2.8 | ||||||
| Inattentive | 7.1 ± 1.6 | ||||||
| Total | 10.9 ± 3.1 | ||||||
| Behavioral Data | |||||||
| Overall RT (msec) | 580.2 ± 176.0 | 503.0 ± 142.6 | 8.92 | 0.003 | −0.668 ** | −0.668 ** | 0.330 ** |
| Overall RTV (msec) | 185.6 ± 114.4 | 135.6 ± 101.7 | 8.20 | 0.005 | −0.677 ** | −0.591 ** | 0.329 ** |
| Overall Accuracy | 90.7% ± 5.9% | 90.4% ± 5.6% | 0.09 | 0.769 | 0.208 @ | 0.325 ** | 0.041 |
| Post-error Slowing (msec) | 14.5 ± 119.4 | 57.5 ± 62.9 | 7.80 | 0.006 | 0.338 ** | 0.034 | −0.218 ** |
| Conflict RT (msec) | 86.3 ± 62.1 | 69.5 ± 42.9 | 3.81 | 0.075 | −0.160 | −0.321 * | 0.161 * |
| Conflict Accuracy | 10.6% ± 8.0% | 10.8% ± 7.6% | 0.88 | 0.350 | 0.102 | −0.056 | −0.063 |
| ERP Data | |||||||
| ERN at FCz | −3.20 ± 5.11 | −3.78 ± 4.88 | 0.42 | 0.474 | −0.346 ** | −0.223 | 0.025 |
| CRN at FCz | 0.93 ± 4.77 | 2.41 ± 3.69 | 4.53 | 0.035 | 0.108 | 0.248 * | −0.205 * |
| dERN at FCz | −4.13 ± 6.20 | −6.19 ± 5.44 | 4.72 | 0.031 | −0.369 ** | −0.368 ** | 0.179 * |
| Pe at CPz | 8.99 ± 8.82 | 12.57 ± 9.66 | 5.62 | 0.019 | 0.014 | 0.047 | −0.208 * |
| Pc at CPz | −5.40 ± 6.50 | −6.10 ± 6.19 | 0.45 | 0.506 | 0.268 * | 0.095 | −0.052 |
| dPe at CPz | 14.40 ± 9.37 | 18.66 ± 8.75 | 8.37 | 0.004 | −0.173 | −0.017 | −0.176 * |
| N2 con at FCz(µV) | 0.36 ± 5.57 | 0.80 ± 5.25 | 0.23 | 0.630 | 0.242 * | 0.563 ** | −0.003 |
| N2 inc at FCz(µV) | −0.49 ± 5.14 | −0.92 ± 4.81 | 0.30 | 0.583 | 0.229 * | 0.458 ** | 0.073 |
| dN2 at FCz(µV) | −0.84 ± 2.17 | −1.72 ± 2.55 | 5.00 | 0.027 | −0.084 | −0.297 ** | 0.148 @ |
| P3 con at Pz(µV) | 8.85 ± 5.47 | 11.58 ± 6.06 | 8.63 | 0.004 | −0.086 | −0.220 @ | −0.266 ** |
| P3 inc at Pz(µV) | 10.56 ± 6.16 | 14.57 ± 6.25 | 16.10 | 0.000 | 0.091 | 0.010 | −0.291 ** |
| dP3 at Pz(µV) | 1.71 ± 3.20 | 3.00 ± 3.16 | 6.27 | 0.013 | 0.323 ** | 0.443 ** | −0.113 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Hanna, G.L.; Hanna, B.S.; Rough, H.E.; Arnold, P.D.; Gehring, W.J. Behavioral and Electrophysiological Correlates of Performance Monitoring and Development in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder. Brain Sci. 2020, 10, 79. https://doi.org/10.3390/brainsci10020079
Liu Y, Hanna GL, Hanna BS, Rough HE, Arnold PD, Gehring WJ. Behavioral and Electrophysiological Correlates of Performance Monitoring and Development in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder. Brain Sciences. 2020; 10(2):79. https://doi.org/10.3390/brainsci10020079
Chicago/Turabian StyleLiu, Yanni, Gregory L. Hanna, Barbara S. Hanna, Haley E. Rough, Paul D. Arnold, and William J. Gehring. 2020. "Behavioral and Electrophysiological Correlates of Performance Monitoring and Development in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder" Brain Sciences 10, no. 2: 79. https://doi.org/10.3390/brainsci10020079
APA StyleLiu, Y., Hanna, G. L., Hanna, B. S., Rough, H. E., Arnold, P. D., & Gehring, W. J. (2020). Behavioral and Electrophysiological Correlates of Performance Monitoring and Development in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder. Brain Sciences, 10(2), 79. https://doi.org/10.3390/brainsci10020079